
Abstract
Background:
We evaluated the patient-partner experience in a longitudinal program called Integrated Population Medicine in the Sydney Medical School to assess its acceptability. The program exposed senior medical students to the lived experience of chronic disease.
Methods:
We surveyed 267 people with chronic conditions recruited as patient-partners by the 2012 student cohort in a mixed-methods longitudinal cohort study. Surveys were administered ‘over’ 18 months: before, during, and after the program.
Results:
A total of 155 (58%) patient-partners completed the baseline survey; 52 patients returned all 3 surveys. Patient-partners remained very positive about the program across all surveys. More than 95% of respondents enjoyed interacting with the student, and most were very positive about their role in teaching the student. Three major themes emerged: willingness to help, a sense of gratitude and enjoyment, and a chance to teach and learn. Participants were willing to discuss their illness experiences and were keen to spend more time with students.
Conclusions:
Patients are willing participants in longitudinal patient-partner programs. They perceive benefits for themselves and others, for the health system, and for students and would like to become more actively involved in medical education.
Keywords
Background
Patients are integral to medical education. 1 Increasingly, they are becoming more actively involved in roles from curriculum development to teaching and assessment,2,3 and new ways of structuring student-patient learning programs are emerging.4,5
In 2012, the Sydney Medical School introduced a Longitudinal Patient Partnership Program (LPtPP) called Integrated Population Medicine (IPM). IPM aimed to expose senior medical students to the intersection of population medicine principles, clinical practice, and professional skills through exposure to the lived experience of chronic disease and disability. We aimed to create an engaging, patient-centered learning experience that would inspire student inquiry and be manageable for students and patients. The details of the IPM curriculum are reported elsewhere. 6
Longitudinal partnering with students is a relatively new role for patients in medical education. As in longitudinal integrated clerkships, LPtPPs are aimed at increasing patient-centered care and learner-centered education. In addition, LPtPPs place the patient in the role of teacher and provide an immersive educational experience in which students develop clinical knowledge through sequential conversations with patients over time.7,8 Studies suggest patients value longitudinal relationships with students and feel the involvement of students enhances their care in a range of ways and increases their well-being.9,10
In developing the program, we looked to the Bleakley and Bligh 11 construct of a patient-centered model of learning being a knowledge-generating dialogue between patient and student, with educators acting as a resource to support rather than determine student learning.
Understanding the effects of culture and marginalization on health outcomes was another important aim of the program, so students were encouraged to choose culturally diverse patients. Students attended a 2-hour diversity workshop, based on the cultural humility model of Tervalon and Murray-García 12 and Augusto Boal’s 13 “forum theater” techniques. 14
Cultural humility requires students to first consider their own identity and become aware of some of the barriers that identity may create in communicating effectively with others. It also requires a lifelong commitment to self-evaluation, reflection, and critique and acknowledges and aims to equalize the power imbalances in the physician-patient dynamic to develop mutually beneficial therapeutic partnerships. 12
The pedagogical basis for forum theater as an agent of change is Paulo Freire’s model of problem-posing dialogue in which a continual exchange occurs between teacher (who also learns) and learners (who also teaches). 15 It has been used elsewhere in medical education with good effect.16,17
Students in IPM were given topics to discuss with their patients, focusing on the patient experience of managing a chronic illness and navigating the health system within the broader context of their day-to-day lives and communities. Each student was responsible for recruiting and arranging to meet the patient approximately every 2 months to cover the topics required in the program and to develop and build a relationship. Students were encouraged to allow the conversation to unfold using a semistructured interview approach, with an emphasis on hearing the patient’s story.18,19 Students were asked to reflect on and report to an expert tutor in a confidential format what they learned from each encounter.
This is the kind of relationship Towle and Godolphin 20 were unable to find when looking for programs “in which patients have been given the power to educate students without the mediation or control of faculty.” Patient-partners in IPM were free to discuss any relevant aspects of their care, and students were challenged to think what this might mean to their future practice and what aspects of patient management might need to change at both individual and systemic levels to address the issues raised.
The use of patient-partners in IPM raised faculty and student concerns that chronically ill people would be unwilling to commit to multiple visits or to share the details of their lives with students. It was felt this may be an imposition on patients’ time and privacy. This evaluation also aimed to see whether patient-partners shared these concerns. We describe aspects of their experiences here.
Methods
We conducted a longitudinal cohort study using 3 surveys designed to evaluate the patient-partner experience. Quantitative and qualitative analyses were undertaken in a mixed-methods study. The evaluation was approved by The University of Sydney Human Research Ethics Committee (protocol ID 11-2011/14276).
Participants were all people living with chronic conditions or disabilities recruited as patient-partners by the 2012 IPM student cohort. Students were responsible for recruiting, informing, and gaining the written consent of a patient to follow for the program. We prepared students and patients with written guides, participant information in community languages, simple consent documents, face-to-face training for students, faculty support, and tutorial discussions. The informed consent process was clearly outlined in the student guide, and patient participation documents described the roles of patient and student. Students were expected to discuss this information and address any questions before consent was sought. Patient-partners could contact the program manager at any time to discuss concerns or provide feedback.
The program manager sent the first survey and participant information statement about the evaluation by mail to every patient-partner recruited by an IPM student, once their written consent was received. Only those patient-partners who returned survey 1, after one reminder letter, were sent surveys 2 and 3. Table 1 shows survey response rates. Participants could choose either paper surveys returned by mail or online responses using LimeSurvey. No incentives were offered. Participants were de-identified, but a numerical code linked the participant and their recruiting student, and their responses over time.
Survey response rates.

Surveys were sent to participating patient-partners in March 2012 (S1) just after recruitment (baseline), October 2012 (S2) midway through the program, and June 2013 (S3) at the end of the student contact period. Questions from each survey are listed in Table 2. Surveys were developed by the evaluation subgroup of the program working party to evaluate the program in terms of the following categories:
Program structure,
Provision of information,
Time commitment required of participants,
Behavior of the student,
Professionalism,
Communication,
Cultural respect,
Satisfaction with different aspects of the program,
Question content,
Participant’s perceived role in teaching,
Interaction with the student,
Overall satisfaction of the patient-partner,
Whether they would enroll in IPM again,
Whether they would recommend the program to others.
Questions from each survey.
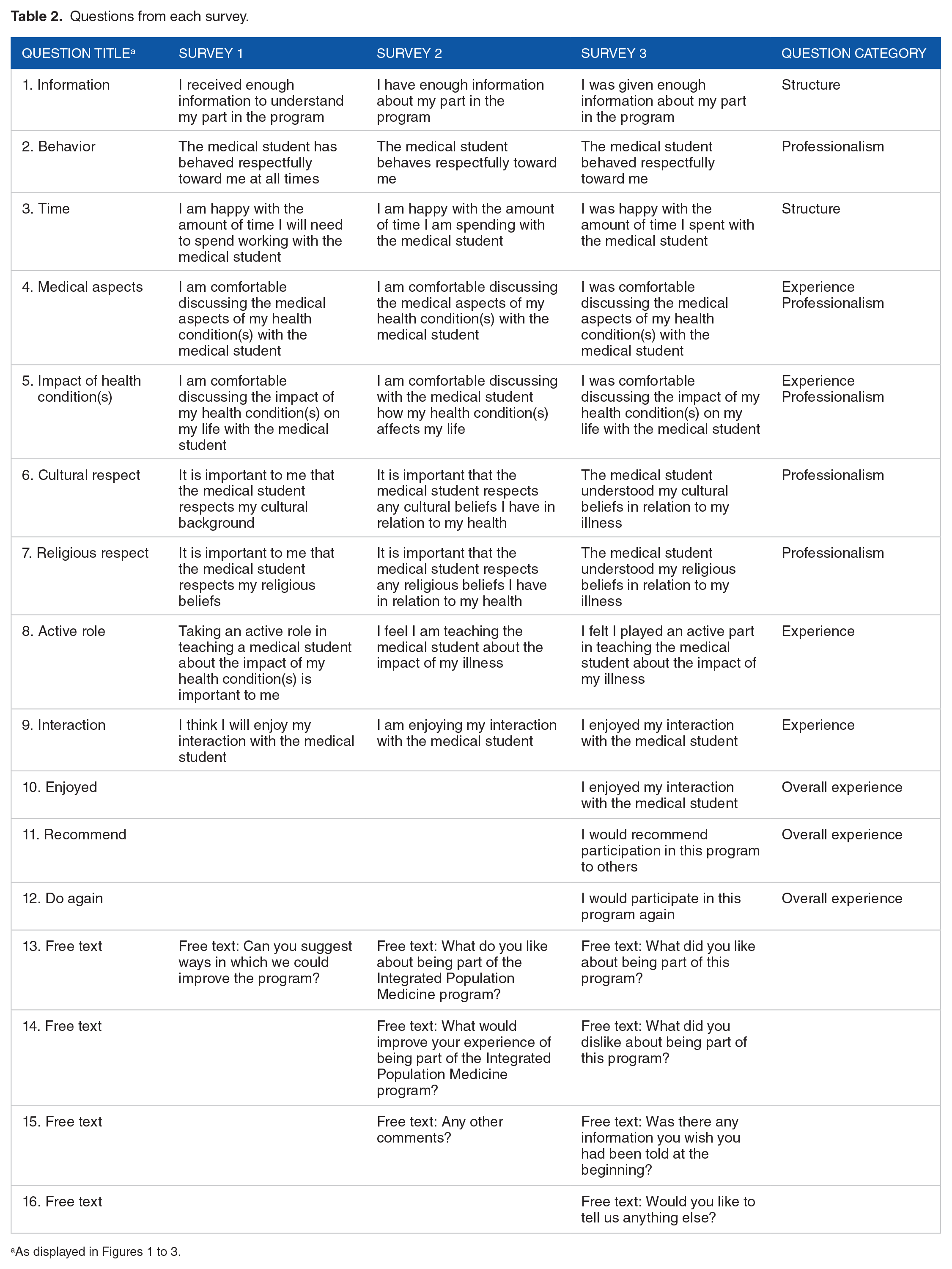
Responses consisted of 5-point Likert scales and free text boxes.
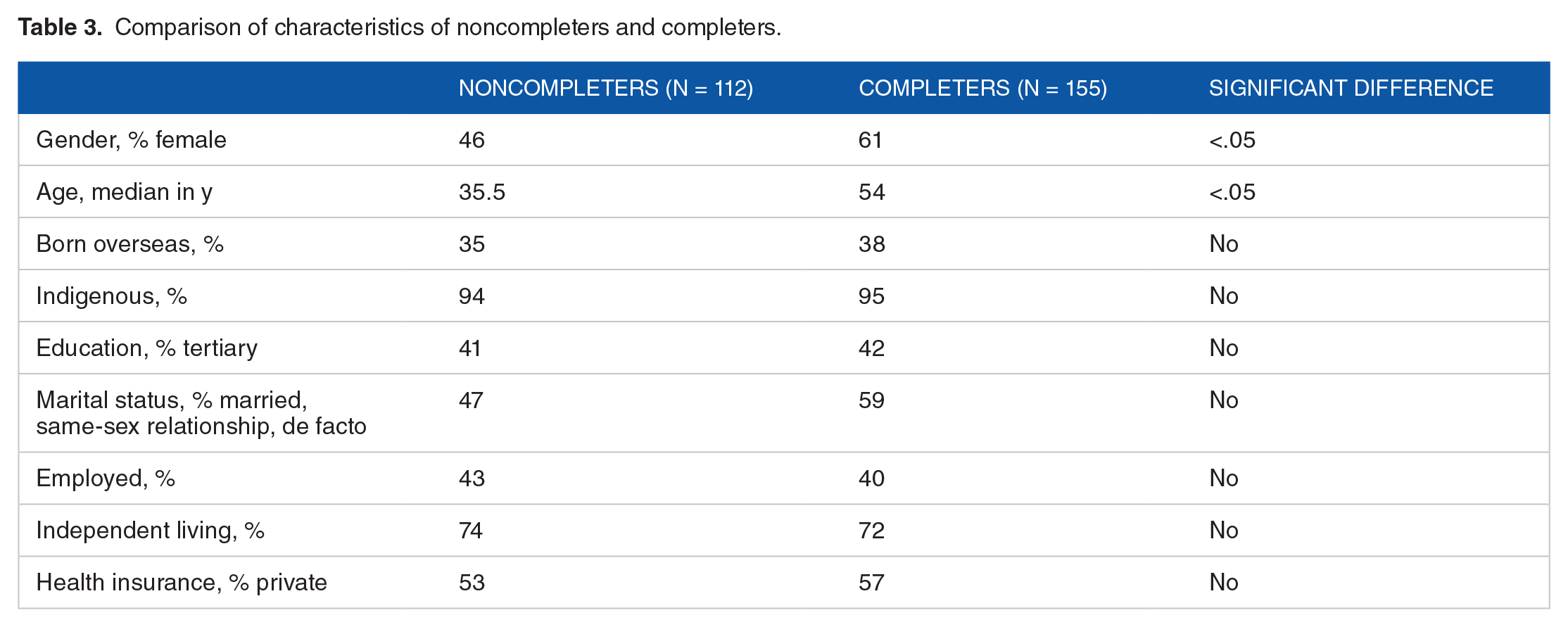
All quantitative analyses were conducted using IBM SPSS v21, and P values less than .05 were considered statistically significant. The demographics of people who returned survey 1 were compared with those who did not return it (see Table 3). For categorical data such as gender, chi-square analyses were conducted. The distribution of age was assessed for skew using a 1-sample Kolmogorov-Smirnov test. The distribution deviated significantly from normal, so completers and noncompleters of the initial survey were compared on age using the Mann-Whitney U test. Changes in the ordinal survey responses (strongly agree to strongly disagree) over time were analyzed using the Wilcoxon signed rank tests to compare survey 1 vs survey 2 and survey 2 vs survey 3. In addition, the Friedman test was used to compare responses across all 3 surveys.
Comparison of characteristics of noncompleters and completers.
Free text comments from each survey were transcribed into Excel spreadsheets. A simple framework analysis was used to group participants’ responses into major topic headings. These brief statements were coded manually by author K.D.I. over several readings. Coding focused on participants’ reasons for participation and their experience of participation.
Results
Students recruited 267 eligible patients into the program. All patients were sent survey 1 and 155 (58.1%) returned it. Subsequent response rates were 90 of 149 (60.4%) and 64 of 146 (43.8%) (Table 1). A total of 64 patients returned survey 3; however, 12 of these had not returned survey 2. Therefore, 52 patients returned all 3 surveys. Fifteen (15) patients withdrew or died over the period of the program (January 2012 to September 2013). Of these, 8 had completed survey 1, 3 completed survey 2, and only 2 completed all 3 surveys. How these withdrawals/deaths affected survey distribution numbers is also shown in Table 1.
Patients who completed survey 1 were significantly more likely to be older (median: 54 years) and women (61%) than nonrespondents (35.5 years and 46% women; P < .05 for both) but did not differ significantly in any other demographic criteria (Table 3).
The health problem of more than 80% of participating patient-partners fell into 1 of 9 disease categories shown in Table 4. The most common were endocrine (14.2%, mostly type 2 diabetes mellitus), rheumatology, and arthritis (11.6%). The top 9 aligned well with the Australian national health priority areas and included cardiovascular and respiratory diseases and psychiatric illnesses.
Top 9 disease categories of patient-partners.

National health priority areas (http://www.aihw.gov.au/national-health-priority-areas/).
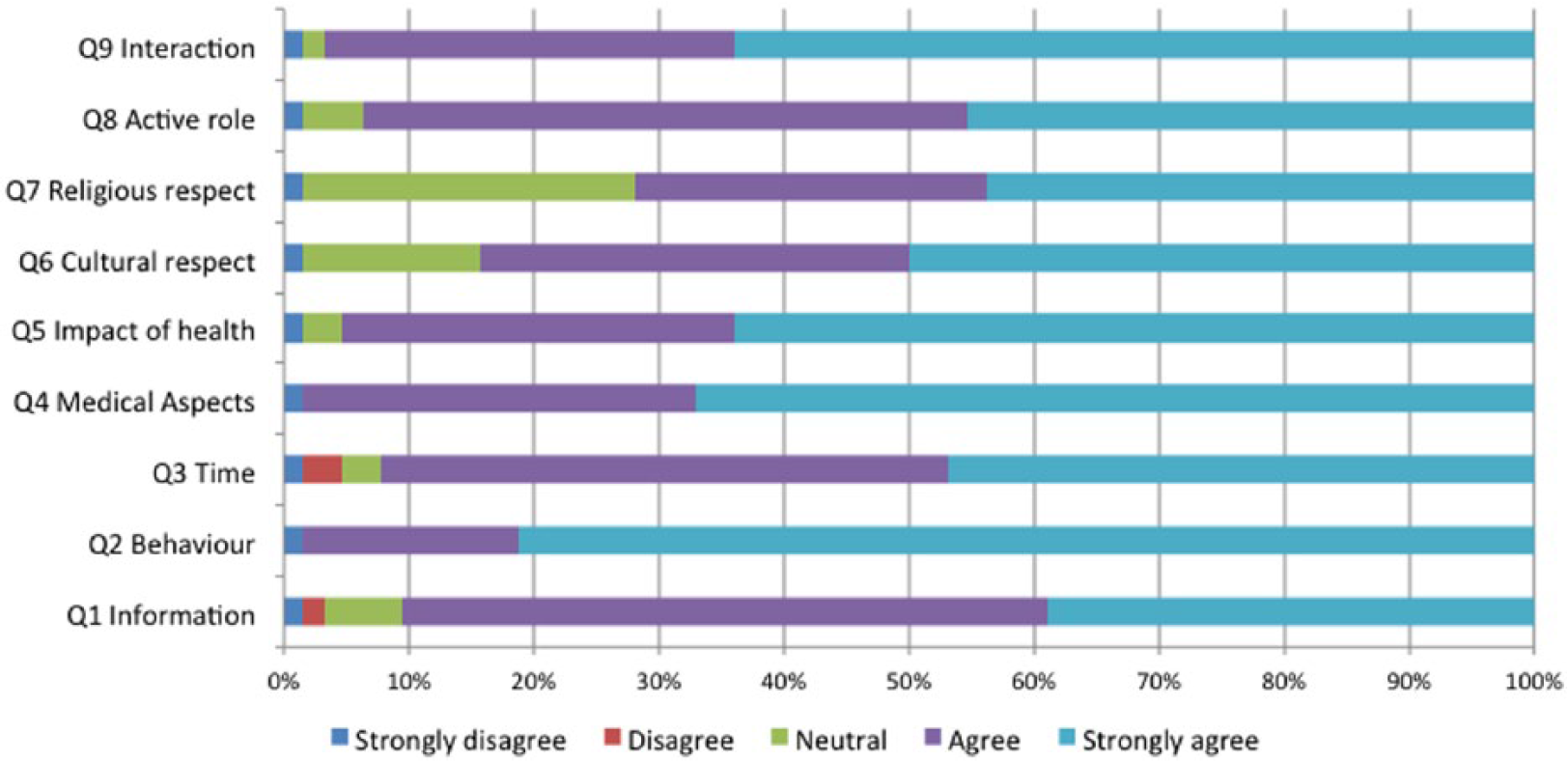
Quantitative results for each survey are shown in Figures 1 to 3.

Participant quantitative responses Q1 to Q9, survey 1: percentage responses based on 5-point Likert scales from strongly disagree to agree, demonstrating largely positive responses in all parameters except Q6 and Q7.

Participant quantitative responses Q1 to Q9, survey 2: percentage responses based on 5-point Likert scales from strongly disagree to agree, demonstrating largely positive responses in all parameters except Q6 and Q7 and starting to show time-related concerns in Q3.
Participant quantitative responses Q1 to Q9, survey 3: percentage responses based on 5-point Likert scales from strongly disagree to agree, demonstrating largely positive responses in all parameters except Q6 and Q7 and starting to show increasing time- and information-related concerns in Q1 and Q3.
Structure and content
Most participants (96.8%) agreed or strongly agreed they had sufficient information about the program in survey 1, and this remained greater than 90% throughout.
In survey 1, participants (98.7%) were happy regarding time spent with the student. This dropped to 88.8% in S2 but rose to 92.2% in S3. This was a significant change over the 3 time points (Friedman’s χ2 = 6.83, df = 2, P < .05; n = 52) and between S1 and S2 (z = −3.1, P < .01, n = 89), but not between S2 and S3 (P = .86, n = 52).
The free text comments confirmed that overall participants were very happy with the structure and content of the program and included constructive suggestions.
When asked what would improve IPM, the 2 most compelling issues were a desire for more time with the student and for feedback about the progress of the program, including the opportunity to meet with other participants and discuss their experiences:
Maybe seeing how the student puts into action some if any of the things they have picked up on throughout this program. (S3) Perhaps an update on how the project is progressing? It would be interesting to hear about other participants and their issues. (S3)
Mirroring the quantitative drop in survey 2, participants were concerned they spent too little time with their student, rather than too much, and some were less than pleased with the time their student dedicated to meetings:
The student is very busy and has seen me once only since my discharge from hospital in March. (S2) Bit more interaction. But not sure if it is meant to be more interaction? (S2) Having more regular and organised meetings e.g. set every 2-3 months. (S2)
Participant experience
Participants’ enjoyment of their interaction with the student remained greater than 95% positive throughout the program (S1 = 97.4%; S2 = 95.5%; S3 = 96.9%). Participants were also very positive about their active role in teaching the student (S1 = 91.6%; S2 = 85.4%; S3 = 93.8%). Although overall there was a significant change in ratings of their role across the 3 surveys (Friedman’s χ2 = 6.82, df = 2, P < .05; n = 52), neither was the drop in the proportion of participants who gave a positive response between surveys 1 and 2 significant (P = .07, n = 89) nor was the increase from S2 to S3 (P = .08, n = 52). In survey 3, most (90.6%) participants agreed or strongly agreed they would recommend participation in the program to others, and 84.4% agreed or strongly agreed that they would participate again.
These results were reinforced by participant’s comments, from which 3 main themes emerged:
A willingness to help,
A sense of gratitude and enjoyment,
A chance to teach and learn.
Willingness to help
Participants most commonly expressed a sense of excitement at having been asked to participate and a desire to help:
. . . I will say that I am excited about being part of this study, which I find to be innovative, and an extremely important resource tool for medical students—the human factor. (S1) Good to see medicine back to the patient! (S1)
The desire to help manifested as either helping the student understand the impact of chronic disease on the person’s life or helping improve knowledge about chronic disease that would benefit future doctors or future patients:
I’m hoping it is helping to make a better doctor of my student, for her to understand from my point of view and assist the whole in learning about health or illness and the impact on everyone—student, doctor, patient and family. (S2) Knowing that my input will help the student in his studies in the hope that in the future someone else will benefit also from my information. (S3)
A chance to teach and learn
Participants also commented on how they saw themselves specifically affecting the student’s education. They particularly highlighted the importance of learning from experience over theoretical learning. They wanted students to understand their conditions and their experiences as patients and to stress the importance of holistic, patient-centered care:
I know that the information I share . . . will provide . . . a better understanding [of] complexities experienced by someone surviving the HIV virus (30 years) and the sort of information that cannot be accessed through books but rather through personal, life experience. (S2) It’s good that this program is giving practical knowledge to medical graduates—about the impacts of medical condition on their personal, family and professional life. I am sure real life learnings will prepare graduates better to handle medical conditions of their patients. (S2)
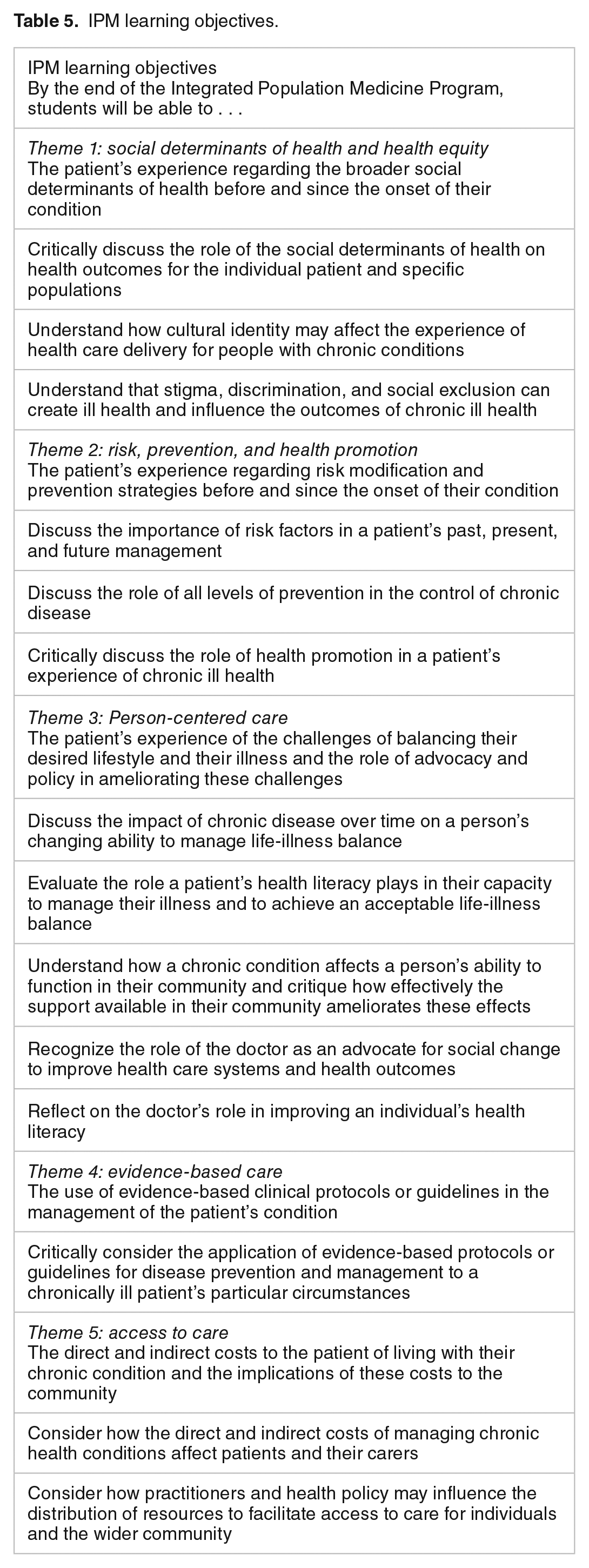
Many comments also demonstrated that participants were learning about their own health care through interaction with the student. This outcome aligned with the IPM learning objective around the doctor’s role in improving patients’ health literacy:
I liked that this gave me the opportunity to find out more about my illness. (S3) It helped me reflect on how I handle my condition. (S3)
Gratitude and enjoyment
Several participants expressed gratitude at being given an opportunity to “give back” to medicine for care they had received:
I am grateful what medical science has done for me and I always help when I can. (S3)
Enjoyment, interaction with the student, and chance to be heard were also strong positives of the program:
I have made a good friend through it. I have been able to share my experience, which is helpful. (S2) Thank you for giving me a voice! (S2) It was also enjoyable to talk and interact with the student. (S3)
Learning outcomes
There was evidence that student-patient interactions helped address some of the key learning objectives of IPM (see Table 5), in particular.
IPM learning objectives.
The role of the social determinants of health:
I hoped it would show medical students that coming from a regional area presents more problems than in a city. (S3)
The impact of chronic conditions on a person’s ability to function in their community:
I thought it was an important contribution to the student’s understanding of the ‘non-medical’ aspects of a chronic illness. The negative impact on work/ family/ financial/ social etc.—which can also loop back to perhaps needing more medical intervention. (S3)
The role of the doctor as an advocate:
Hopefully that my input leads to change for the better in the health system. (S3) Encourage students to . . . gain insights into medical problems and difficulties faced by rural patients . . . information with which they could lobby governments for improvements in rural health facilities. (S1)
The impact of the direct and indirect costs of health care:
I was particularly happy in making the student aware of what it costs (money wise) to have this illness or whatever incapacities the patients have. (S2)
Student behavior
Overall, participants were very positive about the behavior of the students. Greater than 98% agreed or strongly agreed the student behaved respectfully toward them.
Patients generally reported feeling comfortable discussing the impact of their medical condition on the lives. At all 3 time points, 95% or more of the patients agreed or strongly agreed that they felt comfortable in these discussions:
I have to compliment my Medical Student on the way he engages me in conversation . . . with respect and gentle approach. I doubt if I would have been so open had he taken a more clinical approach. Excellent! (S2) Praise for “my” student—who heard through the “grapevine” that I was in hospital, and took the time to pay me a visit. . . . It seems that he will make a caring and dedicated doctor in whichever field he chooses. (S2) My student behaved in an exemplary manner at all times—her care and sense of humour making the experience pleasant. [Student] has a care and understanding which make her “bedside manner” ideal for a future medic. (S2)
Glossary of terms.

The frequent references to “my student” also suggest a sense of ownership by patient-partners of their participation in the program and the positive relationships they felt with the student.
Before IPM started, we ran a workshop on working with diversity for the students, so we wanted to know how students behaved regarding the patient-partners’ cultural and religious values and beliefs. There was a significant improvement over time to the question on respect for cultural background and beliefs. Specifically, responses were stable between S1 and S2 (63%-67% agreed or strongly agreed the student respected their cultural background or beliefs) and improved in S3 (84% agreed or strongly agreed). This change was significant according to the Friedman test (χ2 = 7.65, df = 2, P = .022):
[The program] gives me an insight into the standards of privacy, respect for patients and requirements of care and understanding asked for in our future medics. (S2)
Some comments hinted, however, that not all students had complied with program requirements about informing and consenting patients. It appears some participants may not have seen the preconsent information sheet, only the participant information sheet sent with the first survey:
A letter/some info about the program before signing up, not after. (S3) I would have liked an info sheet in the beginning saying how long the study would go for, what the student will gain from it etc. (S3)
The less time some students spent and their poor communication with the patient were mentioned in the free text by 11 patient-partners and also reflected negatively on students’ professionalism toward the participant:
. . . I would like to be more involved with my student, but only received a few emails, that’s all, no contact. (S2) I haven’t seen my medical student for months. (S2)
Discussion
This study provides further evidence that people living with chronic illness are willing participants in longitudinal patient-partner programs and would be willing to spend more time and become more actively involved in medical education. They perceive benefits for themselves, for others with their conditions in the future, for the health system, and for medical students. The time commitment of such a program is not a deterrent. In fact, participants were keen to spend more time with students.
A strength of this study was the opportunity to obtain participant perspectives of the program as it was evolving. Every participant was invited to complete the evaluation. Data are informative as patient-partners provided extensive free text comments, over 3 time points, with relatively high completion rates, given the duration of the follow-up period.
Our patient-partner group was living with conditions that echoed the common chronic conditions in Australia and included several of the national priority health areas, suggesting that their experiences of the health system would be reflective of experiences of many people in the wider community. Our data align with other studies that show people living with chronic illnesses often feel that doctors ignore aspects of their condition outside their immediate clinical needs 21 and are keen to redress this by improving the knowledge of future doctors. Consequently, they welcomed a medical education initiative that brought “medicine back to the patient.”
The surveys were designed for the purpose and were based on participants’ self-report. Such surveys are susceptible to self-report and social-desirability biases where participants attempt to “look better” to researchers or to be overly positive.22,23 Participants may try to “guess” the purpose of the study, choose an answer that they feel casts them in a more positive light, or try to “please” the researcher. Or they may simply feel more or less strongly about a statement from one day to the next. 23
Using a mail survey may also have affected response rates. International data show response rates to mail surveys are decreasing. 24 Also, Likert scales are subject to user variance that is amplified in a study with small numbers. 23
Our respondents were more likely to be older and women. In all other respects, however, completers and noncompleters were similar. However, it is possible younger, male participants may have been less enthusiastic about the program or less willing to commit their time to the survey. It is also possible participants who were negative about the program either did not say so or did not complete the surveys. The overall similarity between completers and noncompleters, however, suggests that the impact of this on our results is likely to be limited.
The complexity of the Sydney Medical Program (SMP) stage 3 curriculum, which covers 2 academic years and includes an 8- to 13-week elective placement in which most students travel abroad, meant there were potentially lengthy periods of noncontact between patient and student when students undertook electives or rural placements. Poor communication by students at these times may have caused the drop in patient satisfaction with the time spent with students between S1 and S2 and the subsequent recovery in S3.
Despite concerns about patients’ privacy and rights and the time imposition, our findings indicate patient-partners were not concerned. In line with previous strong evidence of Australian patients’ willingness to be involved in medical education and LPtPPs,10,25 our patient-partners’ responses to the program were almost universally positive. Our data suggest that patients would prefer to spend more time with students, would be keen to participate again, and become more involved. The patients saw value in sharing their experience of chronic disease outside the hospital and in allowing students to see the evolution of disease and management. This suggests time taken in LPtPPs is time well invested from the patients’ perspective. However, the data suggest a few students did not respect the gift of the patients’ time and expertise.
This evaluation provided useful insights into the patient experience of our new curriculum. These insights allowed us to subsequently modify the program structure, student preparation and documentation, and patient communication strategies.
Conclusions
This evaluation demonstrates that people living with chronic conditions are likely to be willing and enthusiastic participants in longitudinal programs and in medical education generally. They perceive benefits for themselves, for others, for the health system, and for medical students. The time commitment is not a deterrent, but students and faculty must ensure effective communication and respect for patients’ contributions to their learning. Effective evaluation is key to maximizing the benefits of the experience for all.
Footnotes
Peer Review:
Five peer reviewers contributed to the peer review report. Reviewers’ reports totaled 1661 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Kimberley Dale Ivory received funding from the University of Sydney Divisional Strategic Teaching Enhancement Project Scheme (STEPS) in 2011 to support the development and evaluation of the IPM program.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
KI: evaluation design, data analysis, preparation and editing of draft.
GL: data analysis, draft preparation and editing.
LK: evaluation design, data analysis, draft preparation and editing.
AB: draft editing and review.