
Abstract
Highlights
This study is the first to explore parents’ perspectives of triadic SDM involving an adolescent with a chronic condition.
We identify situations (e.g., non–life-threatening treatment decisions, before an impending transition to adult medicine) in which parents may be more amenable to including their adolescent in the decision process.
Understanding parents’ perspectives on decision making can help providers establish strong relationships with the families, which may improve care for adolescents with chronic conditions.
Keywords
Shared decision making (SDM) is a collaborative process for making health care decisions wherein information is exchanged between the health care provider and patient so they can work together to make a decision based on evidence and the patient’s goals, values, and preferences. 1 In the United States, medical decisions for chronic care are typically triadic (patient–health care provider–parent) because adolescents have limited legal ability to consent for treatment. 2 Families with children entering adolescence may be unfamiliar with triadic SDM and need to be taught to participate collaboratively in these interactions. 3 However, SDM with adolescents can also be a difficult task because consideration must be given to what is important to both the adolescent and their parents, how to engage each in decision making, 4 and an adolescent’s ability to be involved in the decision process.5,6
Parents play an important role in adolescent triadic SDM due to their legal authority and long-term perspective on the effect of decisions. Parents may assume different roles in triadic SDM with an adolescent based on multiple factors, including parenting styles, 4 their adolescent’s drive for autonomy, 6 the parents’ emotional states, 7 and the nature of the adolescent’s illness. 8 These roles may, in turn, affect the decision-making process.
Understanding parents’ perspectives about SDM with their adolescent is essential for developing interventions to improve triadic SDM. However, there is a critical gap in our understanding of parent perspectives. Existing research has primarily examined parents’ or caregivers’ roles in dyadic (parent–health care provider) SDM.9–12 A recent study 13 described parent, adolescent, and clinician perspectives of adolescent decision involvement, a related but distinct concept,14,15 in adolescents with chronic conditions. 16 To our knowledge, no research has specifically focused on parent perspectives about their role in triadic SDM with an adolescent. The focus of this article is to understand parents’ perspectives on triadic SDM with their adolescent with a chronic condition and their adolescent’s health care provider. These data will then be used as part of a larger research program aimed at developing a measure of triadic SDM.
Materials and Methods
We interviewed parents of adolescents (aged 12–17 y) with a chronic condition receiving care at a large, urban children’s hospital in the Midwestern United States from November 2022 to July 2023. The hospital’s Institutional Review Board approved all study procedures and granted a waiver of written informed consent. Study staff documented verbal informed consent.
Eligible parents and legal guardians, henceforth referred to as parents, were identified using adolescents’ electronic health records from participating clinics, including primary care, gastroenterology, rheumatology, pulmonology, and endocrinology. We chose clinics to ensure diversity of perspectives, specifically by including both primary care and specialty clinics. Eligible parents were 1) English speaking, 2) at least 18 y old, and 3) the primary caregiver of an adolescent, age 12 to 17 y, receiving care for a chronic condition and who made a treatment decision at a recent clinic visit (<3 wk prior to the interview). We contacted parents using phone calls, text messages, or e-mails. Study staff scheduled interested parents for a 60-min video conference or telephone interview. Interviewers were trained study staff with prior experience in qualitative interviewing. All interviewers (E.A.L., I.K.P., C.A.) identified as female and White. We recruited participants until we achieved thematic saturation, the point at which there were no new conceptual insights in 3 sequential interviews. 17
We developed a semi-structured interview guide (Supplemental Material). Interview questions were based on SDM literature,18,19 prior research,20,21 and clinical experience. Interviewers asked parents open-ended questions about recent and past decision interactions regarding their child’s chronic disease treatment. In addition, parents provided feedback on a proposed conceptual model of triadic SDM (Figure 1) and their experience with specific components of the model. After the first 2 interviews, and every subsequent 4 to 5 interviews, we modified interview guides as necessary (e.g., adding more specific language) to improve participant understanding of the questions. The interviewer obtained demographic information at the end of each interview.

Proposed model of triadic shared decision making.
A third-party Health Insurance Portability and Accountability Act–compliant transcription service transcribed the interviews, and study staff checked the transcripts for accuracy, deidentified the transcripts, and uploaded the transcripts into Dedoose 22 for analysis. We used both inductive and deductive coding approaches. The investigators open coded the first 2 interviews as a team, to establish a preliminary codebook.23,24 Preliminary codes were drawn from the conceptual model and new codes were established through discussion. Coders (E.A.L., I.K.P., C.A.) then independently coded 6 more interviews and met in pairs to achieve consensus so that each of the 6 interviews were coded by 2 coders. The 3 coders resolved discrepancies and added to and refined the codebook, as needed, through discussion. Subsequently, the coders independently coded the remaining interviews using the established codebook. The coders met regularly to discuss modifications to the codebook, uncertainties in coding, and emerging themes.
Data analysis used a thematic content analysis approach.17,25,26 We first clustered potentially connected codes into candidate themes. 26 Then, we examined the data to explore how candidate themes fit across the data rather than within 1 specific code. 26 Next, we created a thematic map to chart patterns across the dataset. 26 We iteratively added, deleted, or refined candidate themes throughout this process. 26 We calculated descriptive statistics for demographic variables. Deidentified data are available from the corresponding author upon request.
Coder Reflexivity
All 6 coders were White, cis-identifying women with experience in health care settings. The coders included a physician–scientist, a rehabilitation scientist, and a psychology graduate student. All had clinical and research experience working with adolescents with chronic conditions and their families.
Results
Twenty-one parents of adolescents with chronic conditions participated (Table 1). Most parents self-reported as White (57%), female (91%), and had at least some college education (52%). The most common chronic conditions among parents’ adolescents were asthma (24%), attention-deficit/hyperactivity disorder (24%), and inflammatory bowel disease (24%). We identified 4 major themes from the data, as described below.
Parent and Adolescent Demographic Characteristics
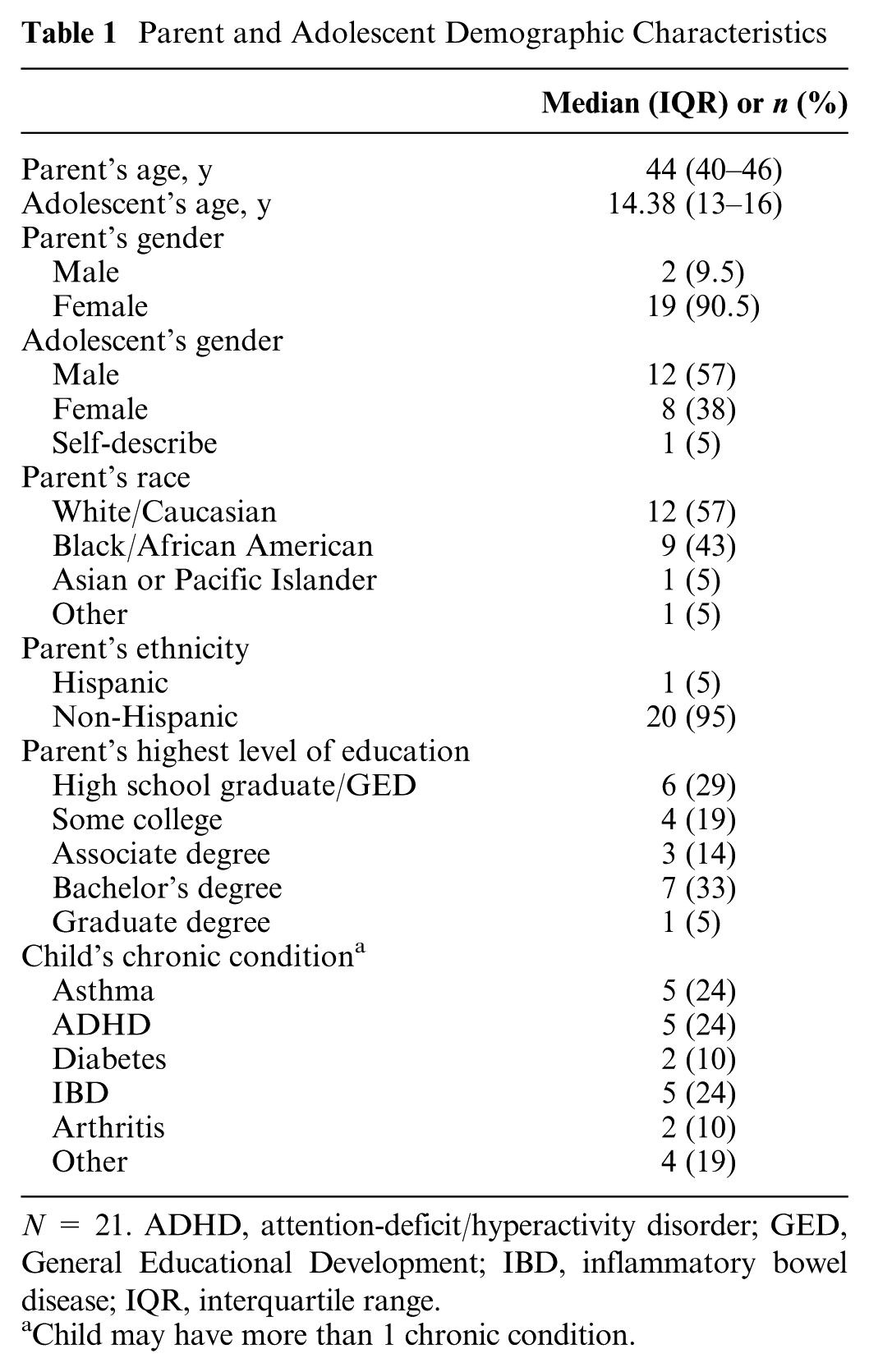
N = 21. ADHD, attention-deficit/hyperactivity disorder; GED, General Educational Development; IBD, inflammatory bowel disease; IQR, interquartile range.
Child may have more than 1 chronic condition.
Parents Want an Executive Role
Parents described seeking to ensure that their adolescent’s involvement in SDM is appropriate for their developmental level, maturity, competence, and experience. To accomplish this, parents sought to control the power that the parent, health care provider, and adolescent had in SDM, a concept we define as the parent’s “executive role.” Some parents, especially of younger adolescents, want to fill this executive role because they feel that their adolescent is not competent to play a large role in SDM. For these parents, SDM is a dyadic interaction between the parent and health care provider. A mother of a 17-y-old boy (ID09) shared, “The younger the child the more the parent has to step up and say, hey, like this is what we think is a good thing to do.” Other parents, particularly of older adolescents, use SDM to build their adolescent’s independence, preparing them to manage their own care. As one mother of a 17-y-old boy (ID11) said, “. . . because he’s 17 now, I also like [the discussion] to be more of, like, a collaborative thing and where he’s making those decisions too and not just being told.” A father of a 15-y-old girl (ID05) said,
It’s her life. And at some point, she will be an adult that has to manage this herself alongside of the doctor as well. So, it’s almost like a way for her to grow through the situation and learn the skills and the right questions to ask.
Although parents reported wanting their adolescents involved in SDM, only a few parents thought that their adolescent should be the final decision maker for all decisions. Several parents said they would be comfortable letting their adolescent be the final decision maker in at least some circumstances. One parent of a 17-y-old girl (ID12) shared, “. . . ultimately, because [my child] is not an adult, it has to be up to the doctor and the parent, you know.” While parents typically see themselves as the final decision maker, some parents defer to the health care provider. One mother of a 14-y-old girl (ID07) said, “. . . I can’t picture a time when I won’t just revert to whatever the doctor thinks is best.” Several parents described deferring to the health care provider, rather than engaging in triadic SDM, when their child was acutely ill: “. . . if [the doctors] felt that [my child] was in an unstable [condition] . . . then I would say, leave it up to the doctors as far as making a decision” (ID12).
Parents described feeling comfortable taking an executive role because they see themselves as the conduit between their adolescent and the health care provider. They described their life experience as enabling them to understand what is being communicated to the family and comprehend “what the decision means, not just for the short term, but the long term” (father of a 14-y-old girl; ID05). In addition, parents feel they know their child’s values, goals, and preferences as well as how they are coping with treatment so far. One father of a 14-y-old girl (ID05) expressed this belief, saying, “you know your kid really, really well as a parent.” Parents’ ability to synthesize information from the other 2 parties in the triad gives parents the confidence to step into this executive role, even when their preference differs from that of their adolescent. One mother of a 14-y-old boy (ID08) noted that she tries to “explain [to my son] that other side of things and why things may need to be the way that they are, as opposed to what [my son] really wants.”
Parents as Experts
Parents believe that one of their SDM responsibilities is to understand all information communicated to the family by the health care provider and ensure that their adolescent also understands it. One father of a 14-y-old girl (ID05) stated, “it’s really important as a parent to educate yourself . . . so that you can ask the best questions.” This understanding includes knowing the options, potential outcomes, and the related medical evidence. One mother of a 14-y-old boy (ID01) shared, “my role would be, of course, communicating with the physician and communicating with my child everything that I understand. And the things that my child does not understand, I could clarify those.” Although parents seem eager to take on this responsibility in their adolescent’s care, they also feel pressure to make the “right” decision for their adolescent. One mother of a 13-y-old boy (ID14) voiced, “[My child] puts a lot of trust in us, and that puts a lot of pressure on us to do him right.”
As part of their expert role, parents seek to make sure they are informed, including gathering information from multiple sources. One mother of a 13-y-old girl (ID02) stated, “if I have questions, I’ll either send one on MyChart, or . . . I Google quite a bit.” Many parents bring options to their child’s health care provider because of a feeling of responsibility to explore all options and advocate for their child. One mother of a 17-y-old (ID03) shared, “[the doctor] had not brought up the, you know, herbal stuff or homeopathic stuff, and we brought it up.” However, more typically, parents focus on the options presented by their health care provider during their visit. A mother of a 13-y-old girl (ID02) shared, “we just kind of hope for the best I think and trust what the doctors have to say.”
In addition to being an expert on information related to the decision, parents also saw themselves as an expert on their child. One mother of a 13-y-old boy (ID14) shared that “the doctor knows what he knows, but I know what I know.” Parents expressed that this expertise allows them to understand if their child has the skills and maturity to participate in SDM. One mother of a 16-y-old boy (ID16) stated, “why don’t [the doctors] all stop asking him questions because now he’s giving you the wrong information because he don’t understand the words you all are saying.” Parents spend much more time around their child than the doctor does and are able to communicate information about their adolescent’s condition back to the doctor. One mother of a 13-y-old boy (ID14) shared,
[I ask] my son, you know, what number of pain he’s at daily . . . me basically getting all the information, him sharing it with me. . . . If we think that something needs to change because something’s not going right, then we reach out to the doctor.
This expertise sometimes prompts parents to initiate decision making. A mother of a 12-y-old girl (ID06) stated,
the only way a doctor would know there’s a problem to begin with is if the problem was told by the parent. . . how is the doctor going to know what a child is doing when the doctor is not around the child 24/7?
Parents’ Perceptions of Others’ Roles
Adolescents’ role
From the parent’s perspective, the adolescent’s role is to communicate information about their preferences and values, begin to learn how to make decisions independently, and trust that their parents have their best interests in mind. Some parents discussed that adolescents had a responsibility to fulfill these roles because the adolescent is the one with the chronic condition. These attitudes were exemplified by one (ID15) who shared, “it’s [my child’s] body . . . I figure she got a role to play in that because it’s her. She got to live with this.” Parents also stated that as their adolescent starts to age out of the pediatric health care system, they should start to take more responsibility.
Many parents mentioned getting information about their adolescent’s preferences and values by directly asking their adolescent or through interpreting their adolescent protesting particular options. However, parents also reported that adolescents struggled to identify their values. Parents described using their knowledge of their child to lay out how a decision would affect the adolescent’s life. One mother of a 14-y-old boy (ID10) shared,
I just pan out the things that could happen, and [my son] makes the decision of whether or not he wants to continue or not. And he’s, “oh, no, I’ll take it.” Because now, it’s affecting something you want. And I had to let him know those are the risks and benefits if you don’t take it.
Providers’ role
Parents saw health care providers’ roles as providing information about the decision, supporting the family in the process, and guiding the family’s decision making. Regarding information about a decision, many parents shared that “the doctor is really good at explaining things to where I understand” (ID18) and that health care providers are skilled at “[giving] us our options and [telling] us the pros and cons and [discussing] with us their opinion of what they think is best” (0029P). Some parents described appreciating when health care providers engage their adolescent in decision making. One mother of a 13-y-old boy (ID04) said that
[My child’s] doctor, you know, kind of talks to him and doesn’t just like talk to me and just, he tries to, he engages [my child] in the conversation too. And I think that really helps [my child] open up if he does have a problem.
Overall, parents feel that the health care provider can support the family by including both the parents and the adolescent in the decision. One parent (ID02) said, “I think that ultimately falls on, you know, [my child’s] care team, just to make sure that everybody’s in the loop.”
Parents’ necessities for SDM
Parents discussed how trusting relationships between the health care provider and parent as well as between the parent and adolescent are essential for SDM. When parents trust their adolescent’s health care provider, they assume that the provider knows what is important to the family. One mother of a 12-y-old girl (ID15) shared, “[the doctor’s] going to [know what’s important to us], if he don't know, he would ask.” Another mother, of a 14-y-old boy (ID10), said, “100% of the time, [the doctors] totally understand where I’m coming from. They get it.” Parents also voiced that there needs to be a trusting relationship with their adolescent. This looks different from parent to parent. For some parents, a trusting relationship with their adolescent means that their child trusts them to make the right decision. A mother of a 13-y-old boy (ID04) shared that, “I would hope he values my opinion and, you know, what I feel is right for him.” For other parents, it may look like the parent giving their adolescent more control over the decision.
Parents appreciate when health care providers make clear that some decisions are not permanent and explicitly invite families to reevaluate the decision or select another option at future visits. One mother of a 13-y-old boy (ID18) expressed that health care providers should “[make] us understand that it’s our decision, but also [make] us understand that if we change our mind, the options, you know, will always be there.” Even though parents appreciate knowing the options for a decision, some may want the doctor to guide decision making because they feel that it is the best way to get their adolescent good care. One mother of a 16-y-old boy (ID13) shared, “Any decision that they come with to me, I feel like it’s the best decision, because . . . they pick out the best [option].”
Discussion
In this study, we explored parents’ perspectives on sharing decisions with their adolescent and their adolescent’s health care provider. We identified 4 main themes from the data: parents want an executive role, parents as experts, parents’ perspectives of others’ roles, and parents’ necessities for SDM. Parents in this study desired control over key aspects of SDM interactions, including how much and to what extent their adolescent is encouraged to participate. Our results contribute to this emerging area of SDM by describing parents’ perspectives on SDM as well as their perspectives on their own role and those filled by their adolescent and health care provider.
Similar to previous studies, we found that parents and health care providers, rather than the adolescent, tend to be the primary decision makers.8,12,27,28 Our study expands on this by demonstrating that at least some parents believe that they should get to determine who the final decision maker is, even if they relinquish that role to the health care provider or their adolescent.
Prior qualitative studies of triadic decisions in pediatric oncology found that parents shared few decisions with their children due to the life-threatening course of their illness and regimented treatment.8,12 Conversely, our study showed that parents share many aspects of the decision with their adolescent. A potential reason for this difference may be because we interviewed parents of adolescents whose chronic condition is currently managed primarily as an outpatient. Parents in our study discussed instances in which they give their adolescents more autonomy in SDM. These instances were when they knew their child was developmentally capable or when they were trying to prepare their adolescent to take more control over their care. Parents justified their role in determining the final decision maker because of their knowledge of their adolescent and previous experience in medical decision making for either themselves or their child. Previous research indicates that parents may have misconceptions about what is most important to their child in making treatment decisions and that there is a discrepancy between when parents consider their adolescent to be developmentally ready to make decisions and when the adolescent considers themselves ready.4,5,8,29 Failing to accurately judge an adolescent’s capacity to choose particular treatment options may result in health consequences (e.g., reduced adherence to medications). It is unclear how to best determine an adolescent’s readiness to participate in decisions, but health care providers may be able to bridge this gap by facilitating conversations between the parent and the adolescent about the adolescent’s readiness for decision making. In chronic conditions, these conversations need not occur at a discrete moment in time but rather can be revisited as the adolescent’s health changes and they developmentally mature.
Parents in our study also identified trust between health care providers and the family as an important contributor to triadic SDM. Previous research shows that trust in the physician is an important facilitator of SDM.30–32 The relationship between trust in the physician and SDM appears to be bidirectional, 32 and greater trust in the physician has been shown to predict SDM. 30 Parents in our study reported that trust is built when the health care provider actively listens to the perspective of the family with empathy and when they provide tailored treatment options. Others have commented that providing options in SDM is important to patients because it gives them a role in their care 33 ; our study suggests that health care providers can build trust with parents by including adolescents and their parents in decisions about the adolescent’s care.
A strength of our study is that we recruited parents within a few weeks of a treatment change; however, these changes may not have used SDM. Results are limited by all parents being recruited from a single children’s hospital. In addition, all interviewers were affiliated with the hospital where the interviewee’s adolescent was receiving care. This may have led to social desirability bias and limited statements that might appear critical of the health care provider or the care received. 34
Conclusion
Findings from this study contribute to knowledge about triadic SDM by elucidating perspectives of parents of adolescents with chronic medical conditions about SDM interactions involving a parent, an adolescent, and a health care provider. These insights can be used by health care providers to promote SDM when making decisions with adolescents. Future research should determine how best to incorporate parents in triadic SDM to optimize adolescent health outcomes and prepare adolescents to take a larger role in their care. However, there is currently no measure that evaluates the process of triadic SDM from the viewpoint of parents, their adolescent, and their adolescent’s health care provider. This work will inform our work developing such a measure so that clinic visits can be evaluated to improve triadic SDM and, consequently, care for adolescents with chronic conditions.
Supplemental Material
sj-docx-1-mpp-10.1177_23814683251409819 – Supplemental material for “The Doctor Only Knows What He Knows, but I Know What I Know:”: Parent Perspectives on Shared Decision Making with Adolescents
Supplemental material, sj-docx-1-mpp-10.1177_23814683251409819 for “The Doctor Only Knows What He Knows, but I Know What I Know:”: Parent Perspectives on Shared Decision Making with Adolescents by Isabella K. Pallotto, Adam C. Carle, Chelsey B. Anderson, Naana Ennin, Mary Anne Ammon and Ellen A. Lipstein in MDM Policy & Practice
Footnotes
Acknowledgements
Dr. Lipstein affirms that everyone who has made significant contributions to this work is included. Generative AI, AI-assisted technologies, or writing assistance were not used in the preparation of this manuscript.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided entirely by an Agency for Healthcare Research and Quality Grant (#1R01 HS028976-01) to Drs. Carle and Lipstein. Dr. Anderson’s effort on this project was supported by the National Research Service Award in Primary Medical Care, T32HP10027, through the Health Resources and Services Administration. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
Meeting Presentations
This work was presented in an earlier form as a poster at the 45th Annual North American Meeting of the Society for Medical Decision Making (SMDM 2023) Conference in Philadelphia, Pennsylvania.
Ethical Considerations
Ethical approval for this study was granted by the Cincinnati Children’s Institutional Review Board (#2022-0329).
Consent to Participate
A waiver of written consent was granted for this study. All participants provided verbal consent before the interview.
Consent for Publication
During the verbal consent process, participants were informed that all interviews would be deidentified and that no identifying information would be included in any study-related papers or presentations. All participants gave verbal consent to participate in the interview.
Data Availability
Deidentified data are available upon request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.