
Abstract
Highlights
Shared decision making (SDM) in chronic hepatitis B (CHB) patients is at an above-average level, with significant individual differences.
Gender and cirrhosis status are key independent factors influencing SDM levels.
Higher SDM levels positively affect both medication self-efficacy and adherence, with self-efficacy serving as a mediator.
In recent years, the doctor–patient relationship has evolved from a traditional “active-recipient” model to a more collaborative “guidance-cooperation” approach. Shared decision making (SDM) 1 refers to the process in which medical staff members help patients understand treatment options based on the best available evidence, reaching a mutual agreement on the treatment plan. SDM has been shown to enhance patient involvement and satisfaction, reduce decision-making regret and conflict, improve treatment adherence, and, ultimately, contribute to better health outcomes. 2 Hepatitis B virus (HBV) infection is a global issue, affecting approximately 296 million people worldwide, with a prevalence rate of 3.8%. 3 It is a major cause of cirrhosis and hepatocellular carcinoma, and 84% of liver cancer cases in China are attributed to HBV infection. 4 Currently, antiviral treatment remains the most crucial and effective approach for managing chronic hepatitis B (CHB). The primary strategy involves the use of potent, low-resistance nucleos(t)ide analogues (NAs), with interferon therapy serving as an adjunct for optimization. 5 By 2022, the detection and treatment rates for CHB were 22% and 15%, respectively, 6 falling short of the WHO’s 2030 targets of 90% and 80%. The choice of treatment and patient adherence are influenced by a variety of factors, including individual characteristics, disease-related factors, treatment-related issues, economic and social conditions, and health care systems. It is essential to encourage active patient cooperation and improve treatment adherence to ensure the successful implementation of antiviral therapy. In recent years, the doctor–patient relationship has evolved from a traditional “active recipient” model to a more collaborative “guidance-cooperation” approach. This study aims to evaluate the current state of SDM in CHB patients undergoing antiviral therapy and explore how the level of SDM affects medication adherence.
Methods
Study Population
Convenience sampling was used to select CHB patients who were admitted to or visited the infectious disease department of a tertiary hospital in Shanghai between April and June 2024. The patients met the diagnostic criteria outlined in the “Guidelines for the Prevention and Treatment of Chronic Hepatitis B (Version 2022),” 5 and were undergoing oral NA treatment for more than 3 mo, and had not received any antiviral treatment other than oral NA. The study was approved by the hospital’s ethics committee (approval No. [2020] Lin Lun Shen No. [331]). Inclusion criteria for the study were as follows: 1) age ≥18 y and 2) the patient provided informed consent and voluntarily participated in the study. Exclusion criteria for the study were as follows: 1) patients with cognitive, visual, auditory, or psychiatric disorders who were unable to complete the survey independently; 2) patients with co-infections of hepatitis A, C, D, or E; 3) pregnant or lactating women; and 4) patients with other severe physical or psychological conditions. The sample size was estimated at 5 to 10 times the number of variables, and an additional 20% was added to the initial estimate considering noncooperation and invalid questionnaires. This study involved 15 variables, thus requiring 90 to 180 samples. Based on the requirements of constructing a structural equation model, the sample size was set at ≥200 cases. A previous study showed that the standard deviations (SDs) ranged from 1.37 to 2.92 among individual SDM-Q-9 scores. 7 In the case of a sample size of 200, under the assumption of normal distribution, the range of the confidence interval (CI) of the SDM-Q-9 score was calculated to be ±0.19 to ±0.40, which was expected to be within 1 point of the SDM-Q-9 score. Therefore, we considered the sample size set at 200 to be adequate.
Survey Instruments
General information questionnaire, including age, gender, long-term residence, educational level, marital status, occupation, per capita monthly household income, and medical payment method.
Disease-related information questionnaire, including duration of hepatitis B, presence of cirrhosis or liver cancer, co-occurrence of other chronic diseases, family history of hepatitis B, and regular medical follow-up (e.g., regular doctor visits).
The 9-item Shared Decision Making Questionnaire (SDM-Q-9), developed by Doherr et al. 2 in 2010, is widely used to assess patients’ perceived level of SDM. The scale consists of 9 items, forming a unidimensional structure, with a 5-point Likert scale (0–5): completely disagree = 0, strongly disagree = 1, somewhat disagree = 2, somewhat agree = 3, strongly agree = 4, completely agree = 5. The total score ranges from 0 to 45, which is then converted to a 0-to-100 scale by multiplying the raw score by 20/9 for easier comparison. The Chinese version of the SDM-Q-9 7 has a Cronbach’s α of 0.945.
The Self-Efficacy for Appropriate Medication Use Scale (SEAMS) 8 is used to measure patients’ self-efficacy in medication adherence. It consists of 13 items, with a 3-point Likert scale ranging from 1 to 3 for each item. The total score ranges from 1 to 39, with higher scores indicating better medication self-efficacy. The Chinese version 9 has a Cronbach’s α of 0.934.
The Morisky Medication Adherence Scale-8 (MMAS-8) was developed by Morisky et al. 10 The scale consists of 8 items, with items 1 to 7 scored as follows: “Yes” = 0 points, “No” = 1 point, with item 5 being reversely scored. Item 8 is scored on a 5-point scale: “Never” = 1 point, “Once in a while” = 0.75 points, “Sometimes” = 0.5 points, “Usually” = 0.25 points, and “All the time” = 0 points. The total score ranges from 0 to 8, with scores <6 indicating low adherence, 8 indicating high adherence, and scores in between (6 and 7) indicating moderate adherence. The Chinese version 11 has a Cronbach’s α of 0.810.
Data Collection
The research team consisted of 5 nurses and 1 physician. Before the investigation, a unified instruction was given to explain the purpose of the survey and the method of filling out the questionnaire. After obtaining informed consent, the respondents filled out the electronic questionnaire on the spot in a quiet and relatively independent space. The questionnaire was set up in such a way that it could be submitted only after all items were completed. The research nurses were present throughout the process to provide unified answers to the respondents’ questions, and the research doctor confirmed the answers. When the respondents were unable to fill out the questionnaire independently, the research nurses or the patients’ family members assisted them through a question-and-answer format. The participants did not receive any form of compensation for completing the survey. The lead words of the doctor–patient SDM questionnaire, self-efficacy Scale for Appropriate Medication Taking, and Morisky Medication Adherence Scale indicated that all the questions were related to oral hepatitis B antiviral drugs (i.e., NAs).
Statistical Analyses
Statistical analyses were performed using SPSS Statistics 22.0 and AMOS 21.0, including descriptive analysis, chi-square test, logistic regression analysis, Pearson correlation analysis, K-means clustering analysis, and structural equation modeling. The significance level was set at α = 0.05.
Results
Current Status of SDM in Patients with CHB
A total of 239 patients were included in this study, with ages ranging from 25 to 77 y (mean age: 52.3 ± 12.5 y). Among the participants, 157 were male (65.7%) and 82 were female (34.3%). The types of oral NAs currently being used were as follows: 115 patients (48.1%) were taking entecavir (ETV), 21 (8.8%) were taking tenofovir disoproxil fumarate (TDF), 108 (45.2%) were taking tenofovir alafenamide fumarate (TAF), and 5 (2.1%) were taking telbivudine (TMF). In addition, 10 patients (4.2%) were using a combination of 2 NAs (ETV + TDF or TAF). Among the 67 patients (28.0%) who had previously changed their NA types, 65 (97.0%) were aware of the reason for the change.
The SDM score for CHB patients, standardized to a 100-point scale, was 71.99 ± 9.22. Among the 9 items, the highest score was for item 3: “My doctor told me that there are different options for treating my medical condition,” while the lowest score was for item 4: “My doctor precisely explained the advantages and disadvantages of the treatment options.”
The 239 patients were divided into 2 groups by k-means cluster analysis: 142 (59.4%) in group A and 97 (40.5%) in group B. The total SDM score in group A (78.18 ± 3.78) was significantly higher than that in group B (62.93 ± 7.08; P < 0.001), and the scores for all 9 individual items in group A were also higher than those in group B (P < 0.001). Therefore, group A was named the “high decision-making level group,” and group B was the “low decision-making level group.”
Influencing Factors of SDM Level in CHB Patients
A comparison of demographic and disease-related information between the 2 groups revealed significant differences in SDM levels based on gender, long-term residence, history of cirrhosis, history of liver cancer, and family history of hepatitis B, as shown in Table 1. In the high-level group, the proportion of males and urban residents was higher than that of females and rural residents. Most of the patients with cirrhosis or liver cancer were in the high-level group, which may be related to the progress of the disease and the need for more medical consultation. Patients with a known family history of hepatitis B were more likely to be in the low-level group, they may have more knowledge about hepatitis B treatment, or they thought they have, thus reducing their interest in communicating with doctors and participating in decision making.
Univariate Analysis of the Level of Shared Decision Making in Patients with Chronic Hepatitis B

Using these 5 factors as independent variables and SDM level as the dependent variable, logistic regression analysis was performed. The regression analysis was conducted using the “Forward: Conditional” method for variable selection. The results indicated that male gender (odds ratio [OR] = 2.047, 95% confidence interval [CI]: 1.177–3.560, P = 0.011) and a history of cirrhosis (OR = 2.163, 95% CI: 1.245–3.759, P = 0.006) were independent factors influencing the SDM level in CHB patients.
Correlation Analysis of SDM, Self-Efficacy for Appropriate Medication Use, and Medication Adherence in CHB Patients
The score of self-efficacy for appropriate medication use in CHB patients was 32.36 ± 3.46 (scoring rate 82.97%). Among all the dimensions, the score of the “difficult situations” dimension was 14.60 ± 1.70 (scoring rate 81.11%), while that of the “uncertain situations” dimension was 17.80 ± 1.99 (scoring rate 84.76%). Besides, the score of medication adherence was 7.13 ± 1.17, which was at a medium level. Figure 1 shows the correlation analysis of SDM, self-efficacy for appropriate medication use, and medication adherence.

Correlation matrix of shared decision making, self-efficacy, and medication adherence. Significant positive correlations were observed among shared decision making (SDM), self-efficacy for appropriate medication use, and medication adherence in chronic hepatitis B patients (P < 0.01).
Path Analysis of the Impact of SDM Level on Medication Adherence in CHB Patients
Based on the correlation analysis results of SDM, self-efficacy for appropriate medication use, and medication adherence, taking medication adherence as the dependent variable, it was assumed that self-efficacy for appropriate medication use and SDM levels directly affect medication adherence. Meanwhile, the level of doctor–patient SDM indirectly affects medication compliance by influencing the self-efficacy of rational drug use. A structural equation model was constructed based on these hypotheses (see Figure 2). The model fit indices were as follows: X2/df = 2.121, goodness-of-fit index = 0.929, adjusted goodness-of-fit index = 0.893, normed fit index =0.925, incremental fit index = 0.959, comparative fit index = 0.958, Tucker–Lewis index = 0.947, and root mean square error of approximation = 0.069, indicating a good model fit. In this model, self-efficacy for appropriate medication use and SDM level accounted for 50.00% of the total variance in medication adherence among CHB patients (R2 = 0.500).

Structural equation model of the effect of shared decision making on medication adherence. Shared decision making and self-efficacy directly influence medication adherence in CHB patients, with shared decision making also exerting an indirect effect via self-efficacy. The model showed good fit (X2/df = 2.121, goodness-of-fit index = 0.929, adjusted goodness-of-fit index = 0.893, normed fit index = 0.925, incremental fit index = 0.959, comparative fit index = 0.958, Tucker–Lewis index = 0.947, and root mean square error of approximation = 0.069), and self-efficacy and shared decision making together explained 50% of the variance in medication adherence (R2 = 0.500).
The path analysis of the model showed that the level of SDM had a significant positive effect on both self-efficacy for appropriate medication use (β = 0.568, P < 0.001) and medication adherence (β = 0.413, P < 0.001). In addition, self-efficacy for appropriate medication use positively affected medication adherence (β = 0.386, P < 0.001).
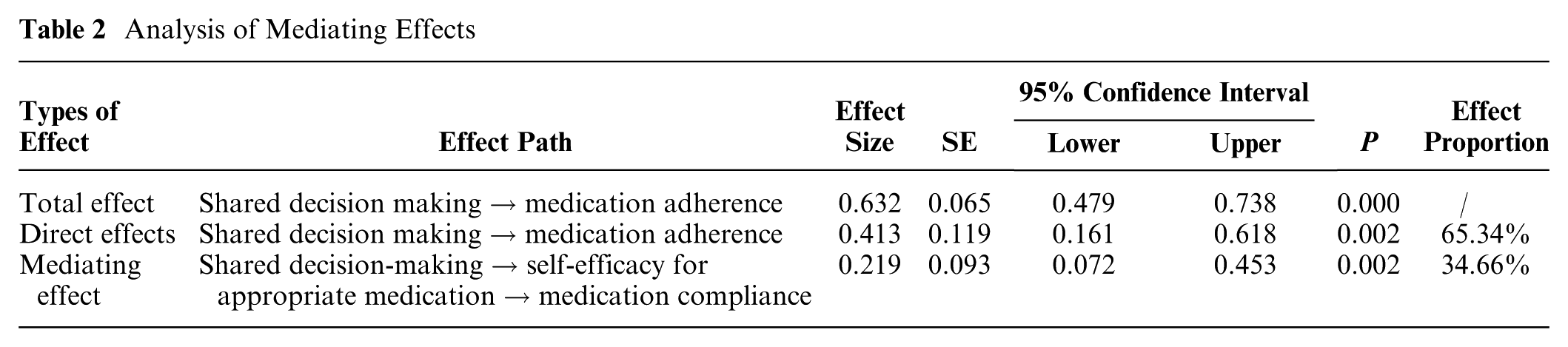
Bootstrap sampling estimation (5,000 iterations) was used to test the mediating effect of the model, with the results shown in Table 2. The total effect size of SDM on medication adherence was 0.632, of which the direct effect size was 0.413, accounting for 65.34%. The mediating effect size of self-efficacy for appropriate medication taking was 0.219, accounting for 34.66%. It was thereby concluded that self-efficacy for appropriate medication use had a significant mediating effect between SDM and medication adherence. In addition, SDM could not only directly affect medication adherence but also indirectly affect medication adherence through self-efficacy for appropriate medication use.
Analysis of Mediating Effects
Discussion
SDM of Antiviral Therapy in CHB Patients at an Upper-Middle Level
The essence of SDM is achieving a consensus between doctors and patients, based on the patient’s full understanding and approval of the treatment plan. With the continuous improvement of the affordability and accessibility of antiviral drugs in recent years, the major economic barrier to HBV antiviral treatment in China has been largely removed. 12 However, patient understanding and recognition may become key factors influencing population screening rates and treatment coverage. “Guidelines for the Prevention and Treatment of Chronic Hepatitis B (Version 2022)” further relaxed the treatment indications, and the standards for starting antiviral therapy have been gradually simplified. 5 Clinical cure (functional cure) has become the ideal treatment goal recommended by both domestic and international guidelines. 13 The development of individualized treatment plans, including combinations or sequential therapies of NAs and interferon, is expected to help CHB patients break free from the long-term, or even lifelong, need for antiviral treatment.
In this study, the antiviral therapy of CHB patients was well standardized, with all patients receiving first-line antiviral drugs. Most of those who had switched their drugs were aware of the reasons for the change (e.g., viral breakthrough, drug resistance). The level of SDM in antiviral treatment for CHB patients was at an upper-middle level, basically the same as that in common chronic diseases such as diabetes, 14 which was slightly lower than that in patients with coronary heart disease and cataract15,16 and significantly higher than that in patients with CKD, rheumatoid arthritis, and cancer.17–19
On the other hand, patients believed that while they were informed of different treatment options, the specific advantages and disadvantages of different options were not fully explained. This phenomenon was attributed to the traditional communication model between doctors and patients and the asymmetry of knowledge and ability between the 2 sides. 20 It also highlights the growing need for patients’ involvement in medical decision making and access to health information, yet the practice of SDM remains limited. Limited health care resources may be the main factors leading to patients’ failure to obtain sufficient communication time and decision-making information. 21 Both doctors and patients commonly feel that “doctors have heavy workloads, and there are many patients” and “there is not enough time to explain.” 22 In response, sufficient evidence has shown that the construction and application of patient decision aids can effectively address this issue and improve the communication efficiency and quality between patients and health care providers. 23 In addition, some studies suggest that courses such as SDM training and medical humanities quality should be introduced to improve the ability, attitude, and behavior of SDM. 24
Differences in the SDM Level among CHB Patients with Different Characteristics
This study showed that gender and the presence of cirrhosis were the influencing factors of SDM level in CHB patients. Male patients had a higher level of SDM, consistent with findings from both domestic and international studies.25,26 Influenced by traditional social gender roles, men are often granted more authority and voice, making them more likely to express their opinions and make decisions. 27 Psychologists suggest that, in uncertain situations, men tend to exhibit “high self-evaluation,” leading to overconfidence in their decisions compared with women. 28 The research on doctor–patient communication in China mainly focuses on the discussion of medical factors, such as the characteristics of doctors and medical institutions, training methods, and effect of evaluation of humanistic and communication skills but less on the mining of patient factors. In recent years, a number of studies involving medical treatment methods have shown29,30 that men have higher acceptance and satisfaction with online diagnosis and treatment than women do. Compared with offline clinics, men can obtain more emotional communication and trust relationships, and men may be more inclined to solve problems and obtain clear suggestions. It is suggested that health care providers should not only take full advantage of patients’ enthusiasm to participate in decision making but also develop a healthy trust relationship with patients. It is also necessary to objectively describe the choices and outcomes in decision aids, 31 including the indications to start antiviral therapy, the pros and cons of different antiviral drugs and the expected effect, the cost of drugs, and whether to be included in medical insurance, so as to guide patients to correctly express their values and intentions.
Liver cirrhosis is a special stage in the course of CHB. Relevant studies have shown that even in patients with HBV DNA-negative compensated cirrhosis, those who do not receive antiviral treatment have a significantly higher cumulative incidence of hepatocellular carcinoma than those who receive antiviral therapy. 32 In the new guideline of China in 2022, liver cirrhosis has been regarded as an indication for antiviral therapy independent of HBV DNA and HBsAg. This study suggests that liver cirrhosis is an important catalyst for SDM, possibly due to the presence of physical symptoms that increase patients’ awareness of health issues as well as more opportunities for communication with health care providers and gaining knowledge about disease treatment. 33 Because CHB is a chronic infectious disease, most patients with the disease gradually acknowledge and accept their illness as the disease advances. In this study, patients with different courses of disease did not show differences in the level of SDM, but the extension of the course of disease was reported as a protective factor in the self-management ability.34–36 Therefore, to improve the level of SDM, efforts should be concentrated on newly diagnosed CHB patients and those who have not yet reached advanced stages such as cirrhosis or liver cancer. This can be achieved by providing basic knowledge of HBV and self-health management, along with addressing negative psychological factors such as stigma, fear, anxiety, and negative coping behaviors. It is also important to emphasize the timely initiation of antiviral treatment, present successful cases of clinical cure for hepatitis B, and help patients make treatment decisions together.
SDM Level Positively Affecting the Medication Adherence of Antiviral Drugs
Existing studies report that the medication adherence rate in CHB patients ranges from 50% to 80%, with no significant differences between domestic and international findings. Low adherence is closely associated with viral breakthrough and increased drug resistance, and unauthorized drug withdrawal can lead to severe consequences, including acute liver injury or even liver failure. Compared with the optimal treatment adherence rate of 95%, a low adherence rate (65%) is estimated to result in an additional 2.6 million CHB patients’ deaths within 15 y. 37 Therefore, achieving high levels of antiviral treatment adherence is a critical issue that must be addressed in the current management of CHB patients in China. 38 Self-efficacy for appropriate medication use refers to patients’ belief in their ability to follow treatment plans and use medications correctly. 39 This study shows that self-efficacy for appropriate medication use has a direct positive effect on medication adherence. In addition, it is positively correlated with the level of SDM and mediates the effect of shared decision making on medication adherence. A survey of patients with hepatitis B cirrhosis in Taiwan province showed that poor adherence was mainly related to patients’ low awareness of the treatment benefits and their reluctance to take medication without obvious symptoms. 40 Australian researchers followed 1,026 hepatitis B patients for 3 y and found that young age (<35 y) and irregular medical visits (consulting multiple doctors in a short period) were major factors contributing to poor adherence. 41 Health is determined not only by the doctor but also by the patient’s knowledge, experience, lifestyle, mental condition, and self-management skills in daily life. A survey of 13,966 outpatients in public hospitals in Hong Kong showed that those participants who had been more involved in decision making and wanted to continue being more involved had greater levels of satisfaction and a better health status. 42 In line with this study’s findings, high levels of SDM can enhance patients’ understanding of both the disease and treatment, improve doctor–patient communication and trust, and thus promote medication adherence through both belief and behavioral changes.
Conclusions
The level of SDM among CHB patients is on par with that of common chronic diseases and is influenced by various factors, including gender and the presence of liver cirrhosis. Therefore, the socioeconomic background of different patients, including education level, income level, and family support, as well as the degree of participation in decision making and medical resources available to them, should be fully considered, with a focus on newly diagnosed patients and those with disease progression (e.g., cirrhosis) to promote the application and popularization of SDM in CHB treatment and further to strive to achieve the purpose of improving medication self-efficacy and treatment compliance. However, the subjects of this study were limited to patients in a tertiary hospital in Shanghai who had started to receive standardized antiviral therapy, which could not represent the overall situation of CHB patients, especially for special groups such as those who met the indications of antiviral therapy but did not start treatment and those who discontinued treatment without authorization. In lower-level hospitals, such as those in rural areas, patients may have greater concerns about treatment options due to limited access to specialized care and resources, potentially leading to lower trust in health care providers and reduced SDM. However, physicians in these settings may have more time to engage in detailed discussions with patients, fostering a better understanding of the disease and potentially enhancing SDM. For untreated CHB patients, the lack of treatment experience and possible skepticism about therapeutic benefits may further reduce their engagement in SDM compared with those already receiving antiviral therapy.
Future studies should include diverse populations, from which subgroup analyses could be conducted to identify specific factors influencing SDM across different populations. These efforts will help clarify the determinants of SDM and inform tailored interventions to promote SDM in varied clinical contexts.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided entirely by a grant of Shanghai Jiao Tong University School of Medicine: Nursing Development Program (SJTUHLXK2024). The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
Ethical Considerations
The study was approved by the ethics committee of Ruijin Hospital (approval No. [2020] Lin Lun Shen No. [331]). All participants provided written informed consent prior to their inclusion in the study. The study was conducted in accordance with the principles of the Declaration of Helsinki (1975, revised in Hong Kong 1989).
Consent to Participate
All participants provided written informed consent prior to their inclusion in the study.
Consent for Publication
This study does not contain any identifiable patient data, and informed consent for publication was not required.
Data Availability
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.