
Abstract
Highlights
Our simulation optimization framework was used to design weekly schedules for random screening tests and masking within K-12 schools to mitigate COVID-19 infections.
We considered multiple objectives and applied the NSGA-II algorithm to find a Pareto solution set.
Based on local context and preferences, decision makers can trade off testing and masking to achieve a similar number of end-of-semester infections.
When a few weeks of masks are mandated, it is best to use them at the beginning of a semester.
COVID-19 has posed great challenges to the global health system since 2020. This airborne, highly transmissive disease was responsible for causing more than 103 million cases and more than 1 million deaths as of December 2023. 1
It is well documented that hospitalization rates for individuals infected with COVID-19 vary by age, with significantly higher rates for people who are 65 y and older (511.9 per 100,000) compared with 5- to 17-y-olds (21.4 per 100,000) based on data from the beginning of January 2022. 2 Because of this, many studies regarding the effectiveness and design of nonpharmaceutical interventions (NPIs) focused on the general population or older adults.3,4 However, children contribute significantly to infections. 5 It was estimated that about 9.8% of infections originated from children aged 0 to 19 y when schools reopened in October 2020, which is much higher than the proportion of infections originating from those 65 y and older (about 2.8%) due to the different social dynamics among different age groups. Thus, analyzing disease transmission among younger age groups within the school environment is important, not only for disease control among school-aged children but also for protecting the entire community. 6
During 2020 to 2023, many different interventions were implemented in K-12 schools (the term “K-12 schools” is commonly used in the United States to represent primary and secondary education from kindergarten to 12th grade). In previous work, 7 we demonstrated the effectiveness of NPIs, such as universal masking, random screening tests, and school closures. However, there may be some negative consequences associated with implementing NPIs, such as school closures. For example, it is estimated that more than 370 million children lost access to their primary source of balanced and nutritious meals when schools were shut down during the pandemic. 8 Furthermore, children experienced significant learning loss due to school closures during the pandemic. 9 Parents were also worried about their children’s lack of social and physical activities, which may affect their social and emotional well-being and lead to mental health issues such as anxiety and depression.10,11 Data show that from April to October 2020, among all pediatric ED visits, the proportion of mental health–related ED visits increased by more than 20% for children from 5 to 17 y old. 12 Thus, in this article, we excluded school closures as a potential NPI and examined how we can keep children in school and at the same time keep them safe through the use of other NPIs.
In 2022, pandemic fatigue rose, and opposition to wearing masks grew. 13 In early 2022, mask mandates were lifted in most K-12 schools that had implemented them. 14 Most schools also stopped requiring negative test results after illness, removed partitions between seats, and brought back regular school events and activities. However, the highly contagious subvariant of Omicron brought new challenges to K-12 schools in late 2022 and early 2023, which resulted in some school districts reimplementing mask mandates and other preventive measures after winter break. 15 During that time, state-funded testing programs were proposed by the North Carolina Department of Health and Human Services, which allowed schools in North Carolina to determine their preferred testing/quarantine and isolation plan. 16 Montgomery County Public Schools (MCPS) in Maryland stated that they would implement COVID-19 mitigation strategies in their Spring 2023 Reopening Guide. Some of the strategies included strategically timed screening tests, testing following school-based outbreaks, and using face coverings to maintain safe in-person learning. 17 These events suggested that interventions were still necessary in schools but needed to be implemented in a way that considered the local context and preferences.
Policy planning and resource allocation are essential for improved preventive health. In uncertain and complex environments, the integration of simulation and optimization techniques can be an effective approach to aid decision makers. The results from these tools can provide guidance for stakeholders to reduce the burden of disease when resources are limited. In this work, we focused on helping K-12 schools find the best way to utilize and allocate the NPIs, such as tests and masks, which schools can easily access. Therefore, we designed and solved a multiobjective simulation optimization problem within a school setting, with the goal of finding an optimal solution for K-12 schools to plan their random screening tests and universal masking schedules while minimizing end-of-semester infections. While the results provided are based on the COVID-19 pandemic, this framework can easily be extended to future pandemics.
Methods
In this section, we briefly discuss the design of the multigrouped susceptible-exposed-infected-recovered (SEIR) model we built in a previous study. 7 Due to the rapid mutation of the Omicron subvariants, we made the necessary modifications and parameterizations to the previous model. The full list of parameters is provided in the appendix. We also describe in detail the design of the optimization problem as well as the assumptions we made.
Simulation Model Structure and Parameters
In 2022, we built a multigrouped SEIR model to simulate the disease transmission within US K-12 schools using R programming language. For the model structure, we considered 9 different health states, as shown in Figure 1. In the model, we broke down the “infected” states into asymptomatic (“Infected(A)”), presymptomatic (“Infected(pre-S)”), and symptomatic (“Infected(S)”). We also distinguished the posttesting states based on the testing results and isolation status. Because COVID-19 tests can be inaccurate under certain circumstances, we considered the possibility of false negatives, followed by the “recovered unknown” state. All the individuals exclusively belonged to one of the health states at any point during the simulation.

Flowchart of the updated COVID-19 disease model.
To keep up with the newest subvariant of COVID-19 and to find the optimal schedule, we made several modifications to the original model. First, the subvariant BA.5 was highly contiguous and responsible for a high reinfection rate. We assumed the reinfection rate was 13%, 18 and the time between “recovered” and “susceptible” had a mean of 100 d. 19 Thus, in addition to the general flow of susceptible-exposed-infected-recovered, we included the transition from “recovered” to “susceptible,” as shown by the green dotted line in Figure 1. In the simulation, we assumed the isolation compliance rate after a school-based positive test to be 100%. Then, infected individuals who received tests would be either positive and isolated or false negative. The differential equations associated with the model are described in the appendix, and the R code is shared in a GitHub repository (https://github.com/yz-ncsu/Optimizing-Masks-and-Random-Screening-Test-Usage-within-K-12-Schools).
With regard to the multigrouped model setting, we split the students and teachers within the school into subgroups and parameterized 3 distinct contact matrices to represent different social patterns within elementary schools (K-5), middle schools, and high schools. For K-5, we assumed the total population of students and teachers was 500, with a total of 18 student subgroups and a teacher subgroup. The 3 contact patterns were “well-mixed,”“cohort,” and “isolated.”“Cohort” represented the social-distancing strategy during the pandemic, in which students had close to a prepandemic-level interaction within their own classrooms but fewer interactions outside of their subgroups. The contact matrices for the different contact patterns are included in the appendix. In this study, we assumed students and teachers were “well-mixed,” representing the schools returning to prepandemic classroom spacing. In addition, although the model was capable of simulating K-12 schools, we limited our analysis to K-5 in this study. In addition, we assumed 1 of the 500 individuals was exposed on the first day of the semester. For the rest of the individuals, 30% of the K-5 school students and 50% of the teachers were in the “recovered” state due to vaccination or previous infection.
We also introduced the concept of weekdays and weekends in the simulation. We assumed the transmission rate within schools was zero during the weekends, as there was no interaction between individuals in schools. The overall simulation period was 107 d, which was about the length of a semester, and the first day of school was assumed to be Monday.
We considered the disease burden from the community by simulating a dynamic disease prevalence during the semester. We generated a random variable
Design of the Optimization Problem
Layered on top of the simulation model, we designed a multiobjective optimization problem. We treated the number of the end-of-semester infections (this includes infections acquired in and outside of the school), the number of random screening tests, and weeks of masks as our 3 objectives. We aim to solve the problem by minimizing all 3 of the objectives together.
There were 2 sets of decision variables in this problem: the testing ratio and the mask usage each week. We considered the testing ratio in each week
The formulation of the 3-objective optimization problem is shown below. In the formulation,




We also considered the dynamic changes in disease transmission during the semester. When the disease starts to spread quickly in a school, many students or teachers may be absent either because they isolate following positive test results or because they develop symptoms and decided to self-quarantine at home. This results in missed school time during the semester. To reduce daily absences, we added the intervention of additional random screening tests, which are triggered by the number of students and teachers who were absent at the beginning of each week. Specifically, if 10 students or 2 teachers are absent on Monday, an additional set of random screening tests at the level of 40% will be scheduled the next day. Because the school population is 500, 10 students correspond to 2% of the school population. We call this absence-triggered (AT) testing; this was designed to simulate the screening tests following school-based outbreaks that the MCPS schools reopen guide suggested. 17
In this study, we assumed the testing kits used in K-12 schools could either be polymerase chain reaction (PCR) tests or rapid antigen tests. The 2 types of testing kits have distinctive characteristics. For instance, rapid antigen tests do not require lab work to retrieve results; thus, results are returned very quickly. PCR tests are much more expensive than rapid antigen tests but more accurate, especially for asymptomatic individuals. The sensitivity rate and specificity rate for PCR tests and rapid antigen tests (symptomatic or asymptomatic) are shown in Table 1.22–24 The results for the rapid antigen tests and PCR tests are shown separately in the Results section.
Sensitivity and Specificity Rate of Polymerase Chain Reaction (PCR) Tests and Rapid Antigen Tests among Symptomatic and Asymptomatic People

From equation (1), we can see that the 2 sets of decision variables have 5 and 2 possible values, respectively, forming a total number of
We modified the function “nsga2R” in the R package called “nsga2R” to solve our multiobjective optimization problem.25,26 There are 4 main parameters of NSGA-II with some conventional choices. Based on the parameter tuning process we conducted in another study, we chose the number of generations = 100, population size = 50, probability of crossover (
In each iteration (generation), the algorithm sorts the parent and offspring populations, retaining the best solutions from the nondominated set for the subsequent iteration until all iterations are complete. Note that good solutions are sometimes discarded to ensure diversity among the solutions. To ensure this, those with the largest crowding distance are also selected for the next iteration. As a result, within a single simulation run, the algorithm identifies multiple diverse Pareto-optimal solutions. In the appendix (Figure D-2), we provide an example of how the solutions change over iterations to yield a Pareto-optimal solution.
Results
Optimal Solutions: PCR Tests
First, we ran the simulation and solved the problem assuming PCR tests were used as the measure of screening tests in school. Planned testing, if used, was scheduled once per week on Wednesday. By leveraging 3 cost functions in the process of optimization at the same time, we found 47 optimal solutions within the Pareto front, all of which are not dominated by each other. In Figure 2, each dot represents the cost function values

The 47 optimal values of the objective in the Pareto front. The y-axis represents the end-of-semester infections (C1); the x-axis represents the number of random screening tests (C2); the color of the dots represents the number of weeks of masks during the entire semester (C3). Same number of weeks of masks are connected with lines. The 7 Pareto solutions marked with red squares are picked as representative solutions for further analysis.
We picked 7 of the Pareto-optimal solutions with end-of-semester values scattered over the limits within the Pareto front to explore further; they are marked with squares in Figure 2 and listed in Table 2. For each of the Pareto-optimal solutions, the columns show the following information: the total end-of-semester infections, the total number of PCR tests performed during the semester, the total number of days when tests occurred (note that this equals the total number of days when the planned testing occurred plus the total number of days when AT testing occurred, as shown in the fifth and sixth columns), and the total number of weeks masks were scheduled. From Table 2, we observe (from the sixth row) that 1 week of masks and 880 screening tests together result in 278 end-of-semester infections. From the fifth row, we see that under a similar level of infections, those 880 screening tests can be saved if 3 more weeks of masks are carried out. In addition, we notice that we can achieve as few as 192 end-of-semester infections if we implement planned testing and masks every week. In addition, we notice that for result 3 and result 6, AT testing occurred twice. This occurred because the daily number of absent students exceeded 10 two times. Although it cannot be observed from Table 2, we point out that AT was not triggered by teacher absences in any of the results shown. We believe this was because of the higher proportion of teachers who were “recovered” prior to the beginning of the semester due to vaccination or prior infection.
The 7 Representative Optimal Schedules Picked from the Pareto Front by Ascending Order of Total Infection

AT, absence triggered.
We designed 4 extreme scenarios: “Result_No_Test_No_Mask” means no screening tests or masks are implemented during the entire semester; “Result_Test_All” represents the scenario where the planned testing is scheduled each week with a ratio equal to the maximum value of 80% and assumes AT testing occurs every week as well, but no mask usage is required; “Result_Mask_All” means masks are put in effect every week during the semester but no screening tests, neither planned testing nor AT testing are used; “Result_All_Test_All_Mask” is the scenario of fully implementing both interventions, 80% planned testing, AT testing and mask usage every week. The percentage choice of testing was designed to reflect the highest level of testing in the simulation.
Figures 3 and 4 show the cumulative number of infections and the daily number of infections of the 4 extreme scenarios as well as the 7 representative optimal solutions, respectively. Clearly, “Result_All_Test_All_Mask” returns the lowest number of cumulative infections, but many screening tests and masks are used, which require additional funds and time. On the other hand, no interventions at all “Result_No_Test_No_Mask” resulted in 301 infections in the school by the end of the semester. The cumulative infections of the representative optimal solutions fall strictly between “Result_No_Test_No_Mask” and “Result_All_Test_All_Mask.”

The cumulative number of infections under the 7 representative optimal schedules as well as the 4 extreme scenarios.

The daily number of infections under the 7 representative optimal schedules as well as the 4 extreme scenarios.
In Figure 2, we can see the 3 optimal solutions where universal masking is never implemented (0 wk, as seen by the gray dots). By comparing these 3 solutions in Table 3, we conclude that no matter how many routine screening tests are scheduled, additional screening tests are always triggered during the semester when no masks are used. This shows that if a universal mask policy is never implemented, the number of absent students will always reach the threshold and require more tests. This reflects the high infectivity and the relatively low protection in the community.
Optimal Schedules in the Pareto Front where Masks Were Never Used

AT, absence-triggered.
Recall that we included the AT testing and mask usage in our 3-objective problem simulation. The existence of AT testing affected the number of planned tests needed. Thus, by checking the specific schedules of the 47 optimal solutions, we noticed that the schedule and ratio of planned testing did not show a clear pattern, as shown in Figure 5. When we narrowed the scope of our observation and took a closer look at the optimal schedules of planned testing when 3 wk of masks are used, Figure 6 suggested a trend: higher testing ratio and frequency corresponded to lower end-of-semester infections. Moreover, Figure 7 shows that the schedule of masks suggested that more weeks of masks resulted in fewer end-of-semester infections. In addition, if schools determine masks should be implemented for only 3 or 4 wk, it is optimal to schedule them during the first half of the semester.

The 47 test schedules of the optimal solutions. Each column of squares represents a Pareto solution with the corresponding number of end-of-semester infections shown on the top. The color of the 16 squares in each column represents the testing ratio performed in those weeks. Black square means no tests are performed in that week.
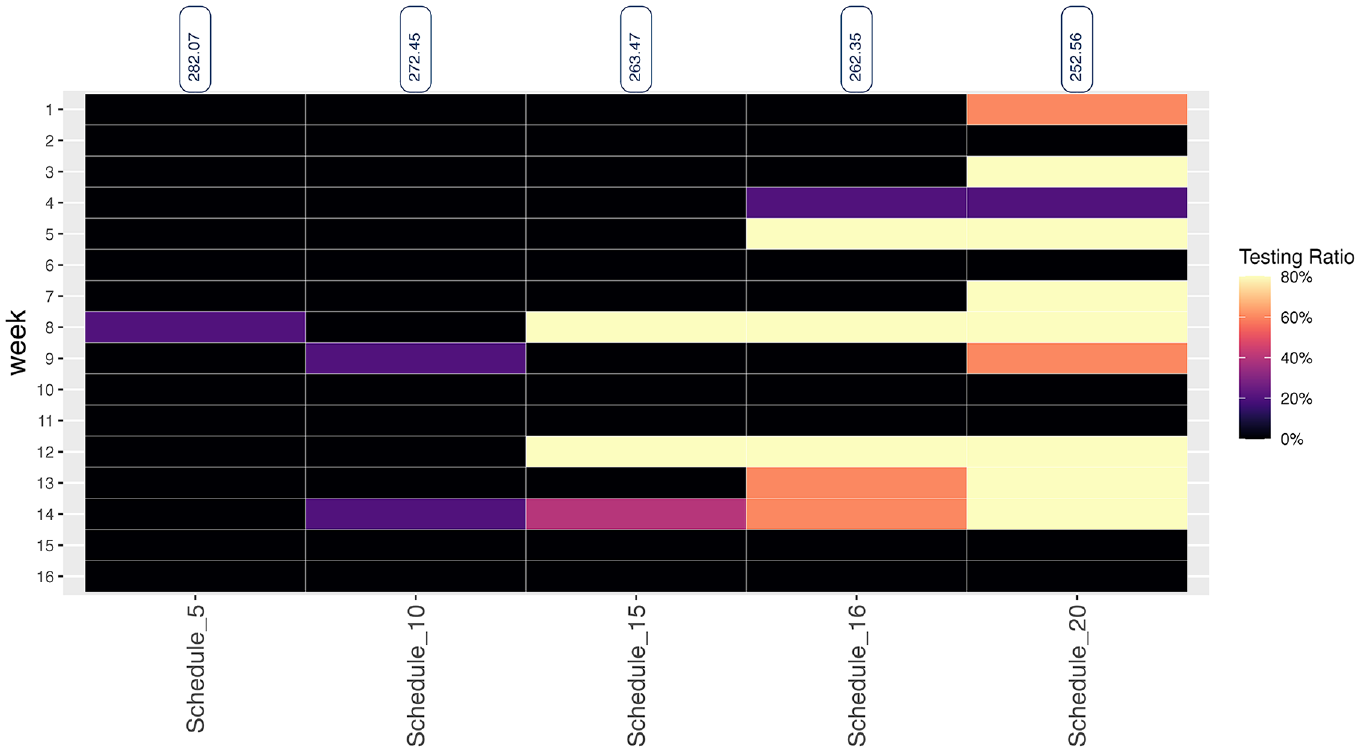
The 5 optimal test schedules with 3 wk of masks. The heatmap shows the subset of the Pareto solutions when 3 wk of masks are used.
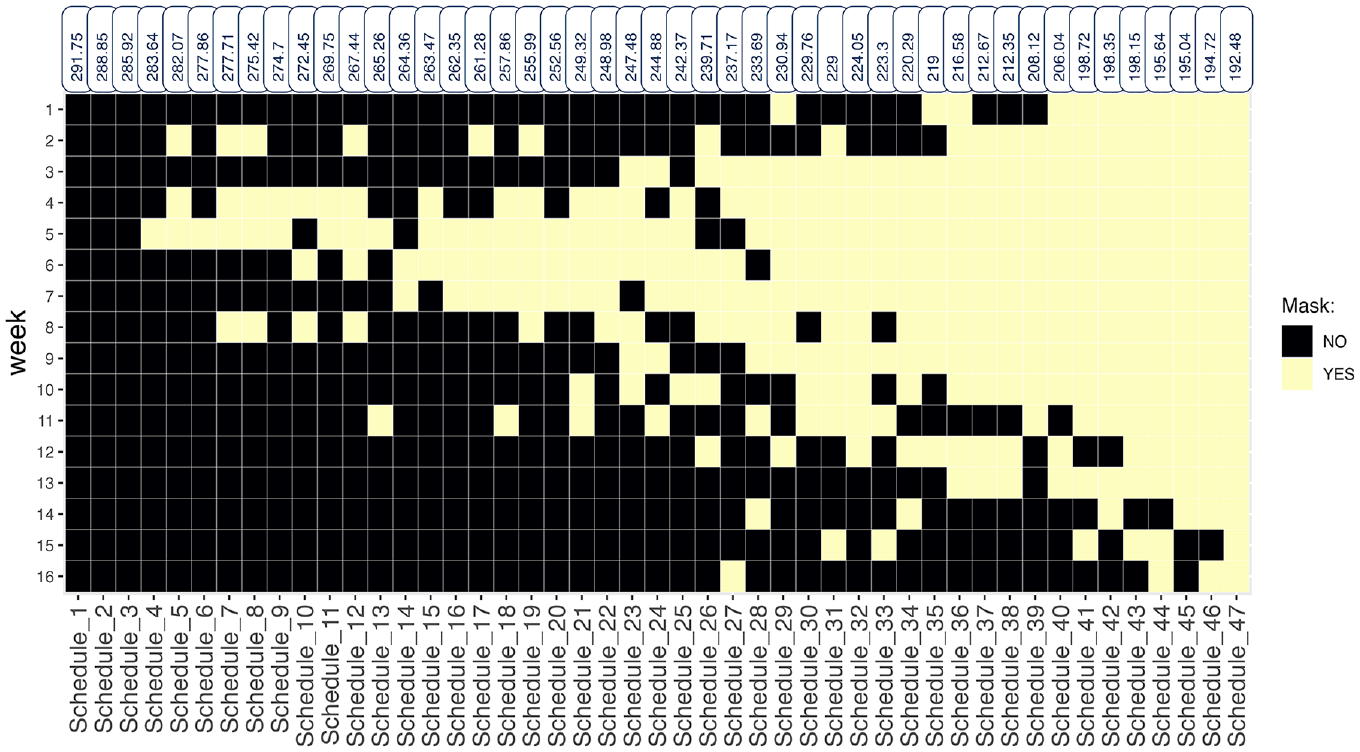
The universal masking schedules of the 47 Pareto optimal solutions. Each column of squares represents a Pareto solution with the corresponding number of end-of-semester infections shown on the top. The color of the 16 squares in each column represents whether universal masking is implemented in those weeks. Black square means no masks are used in that week.
Optimal Solutions: Rapid Antigen Tests
We performed similar analysis with rapid antigen tests for screening. We modified the simulation to reflect the change, which allows individuals to receive test results the same day and transfer to isolation immediately if needed.
By comparing Figures 2 and 8, we see the overall range of the end-of-semester infections was similar between PCR tests and rapid antigen tests. In addition, the effect of tests and masks on end-of-semester infections was consistent between the 2 types of tests. For instance, the highest gray points in Figures 2 and 8 suggested that 584 PCR tests were able to reduce the end-of-semester infections to 292, whereas 8 fewer tests of the rapid antigen type resulted in 1 more infection by the end of the semester. Additional results for the rapid antigen test are shown in Appendix Section E.

The 48 optimal values of the objective in the Pareto front using rapid antigen tests.
Discussion
In this study, we designed and solved a multiobjective simulation optimization problem using NSGA-II. The problem was used to help K-12 schools plan their random screening test and universal masking schedules.
There are some limitations to the study. Certain assumptions were made, such as the number of exposed individuals. This number is uncertain and may differ between schools. In addition, as the virus evolves, some of the parameters we referenced from previous studies—such as the effectiveness of masks, the proportion of asymptomatic infections, and the sensitivity and specificity of PCR and rapid antigen tests—may change. To address these uncertainties, we conducted a sensitivity analysis focusing on 3 key parameters: 1) the effectiveness of masks, 2) the proportion of asymptomatic infections, and 3) the number of exposed individuals on the first day of the semester. The results are provided in Appendix Section F. From the sensitivity analysis, we observed that a higher effectiveness of masks and a greater proportion of asymptomatic infections corresponds to lower end-of-semester infections. In addition, the marginal benefit of 1 additional week of masking is much larger with higher mask effectiveness. While certain parameter values may change as conditions evolve, the method we developed can be easily executed for changes to any parameters and can be tailored to any school.
By solving the 3-objective optimization problem, we successfully verified the negative relationship between the cumulative number of infections and the number of weeks masks are used as well as the negative relationship between the cumulative number of infections and the number of random screening tests, regardless of which type of test we chose. We found that screening tests and masks can be surrogates for each other when prioritizing the value of infections. Thus, if schools prefer one intervention over another, by choosing the aspects they are most concerned about, they can find an optimal policy schedule to implement based on the simulation results. For instance, if schools have a limited supply of tests to distribute during the semester, the Pareto front results can show the lowest number of cumulative infections they can achieve at different levels of mask usage.
Together with masks, we saw that the effect of reducing the end-of-semester infections can be quite similar between rapid antigen and PCR tests. Future work can be done around the cost-effectiveness of the 2 types of tests, as PCR tests are more expensive. In the current framework, we designed AT testing to resemble the schools’ mitigation strategy of screening testing following school-based outbreaks; similarly, masking mandates can be designed to be triggered by the number of infections. Infection-triggered masking would be driven by the disease and not controlled by decision makers directly. Thus, the decision maker could decide the preplanned mask weeks, but the total number of mask weeks would depend on the spread of the disease. This is a possible extension to the model.
Overall, the analysis in this study can offer valuable insights for policy makers in K-12 schools. The conclusions derived from this research can serve as a foundation for making informative decisions regarding random screening tests and universal masking policies. The policies resulting from this model are the most efficient in the sense that they provide the minimum combination of testing and masking to achieve desired infection reduction targets. They also provide the best implementation schedules when the decision maker wants to limit either testing, masking, or both. This benefits students, teachers, and parents by creating a safe learning environment during the pandemic that avoids school closures. In addition, our simulation optimization approach can be generalized to other diseases and be used to make other resource allocation or preventive policy decisions.
Supplemental Material
sj-docx-1-mpp-10.1177_23814683241312225 – Supplemental material for Optimizing Masks and Random Screening Test Usage within K-12 Schools
Supplemental material, sj-docx-1-mpp-10.1177_23814683241312225 for Optimizing Masks and Random Screening Test Usage within K-12 Schools by Yiwei Zhang, Maria E. Mayorga, Julie S. Ivy and Julie L. Swann in MDM Policy & Practice
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided in part by a grant from UL1TR002489 from the NCATS/NIH and Cooperative Agreement NU38OT000297 from the CSTE and the CDC. The research also received partial support from NC State University. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
Ethical Considerations
Not applicable: The study did not use any animal or human subjects. It is a modeling study using with parameters informed by previously published literature.
Consent to participate
Not applicable: The study did not use any animal or human subjects. It is a modeling study using with parameters informed by previously published literature.
Consent for publication
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.