
Abstract
Highlights
Direct and indirect costs have a wide-ranging impact on the material, behavioral, and psychosocial aspects of financial well-being of Black prostate cancer survivors and their caregivers.
These results emphasize the need for sharing cost information to support medical decision making.
Future research should focus on the design of cost-sharing interventions that target the complexities of direct and indirect costs collectively, rather than separately.
This is a visual representation of the abstract.
Introduction
In the United States, the prevalence and mortality of prostate cancer (PCa) is higher in Black men than in other racial/ethnic groups. 1 Undergoing PCa treatment can create substantial financial burden for patients and their caregivers. 2 Financial hardships are the financial problems associated with costs of cancer care that contribute to financial distress. 3 Financial hardship is prevalent among Black PCa patients and survivors and exacerbates health disparities. 4
Black individuals report facing a variety of financial burdens related to direct and indirect costs of medical care, including greater stress over paying medical bills, difficulty living on their income, and reduction in living standards when compared with other racial/ethnic groups.5,6 Caregivers of Black cancer patients also experience financial hardship.7,8 Many caregivers have reported changes in their work schedule, required time off work while caregiving, going unpaid while caregiving, and feeling that they had inadequate financial resources to fulfill the patient and their needs.7,8
Cancer-related cost conversations are often difficult to initiate for providers, patients, and their caregivers. 9 Cost conversations occur in fewer than a quarter of observed oncology visits and are typically very brief, lasting a median of 33 s. 10 Health care staff report that medical cost conversations are difficult to initiate due to a lack of available cost data and information, unawareness of patients’ financial stressors, inadequate time in clinic, and uncertainty around their role in discussing costs. 11 Despite existing barriers, characterizing and sharing cost information can help individuals with cancer make informed decisions about their treatment pathway and seek financial assistance earlier in their care continuum.12–15
When examining patient and caregiver experiences with financial hardship, the impact of direct and indirect costs should be considered.12,13,16 While direct costs mostly refer to insurance-related fees (i.e., co-pays, co-insurance),17,18 indirect costs can include the unforeseen costs of care, including patient-time costs, caregiver-time costs, lost wages, and transportation costs.18–20 Literature on the impact of financial hardship on caregivers of PCa patients is limited, thus emphasizing the importance of including caregiver perspectives on cost burden associated with cancer care. We aim to characterize the direct and indirect costs associated with PCa treatment among Black men and their caregivers to inform shared decision-making materials.
Methods
Study Recruitment
Participants were recruited between October 2022 and May 2023. Eligible PCa survivors (1) were English speaking, (2) self-identified as Black men, (3) were diagnosed with PCa within the past 10 y, (4) were treated with radiation, surgery, and/or active surveillance, and (5) received at least 1 bill for PCa treatment. For this study, we defined survivors as “those living with cancer and those free of cancer.” 21 Caregivers of eligible PCa survivors were also eligible to participate. We recruited participants through our partnership with The Empowerment Network, the Washington University Research Participant Registry, and the community (e.g., e-mail, social media). Eligible individuals were contacted by research staff (H.E.R.) by e-mail or telephone to confirm eligibility. Recruitment continued until we reached data saturation, meaning no new data points were being identified and there was no need for further sampling. 22
Study Design
The multidisciplinary research team collaborated to develop separate semi-structured interview guides for PCa survivors and caregivers. The interview guides (Appendices I–II) were designed to elicit participant perspectives on their general experiences with PCa treatment, the direct and indirect costs of care, and how costs affected them and their families. Team members designed the guides to gain a better understanding of the material, behavioral, and psychosocial aspects of participants’ care-related costs, as guided by the Measures of Financial Wellbeing framework. 23 This financial hardship framework emphasizes the importance of considering these domains (Figure 1) alongside the more traditional aspects of financial well-being (e.g., income), without specifying the correlational or directional relationship among them. 23

Definitions of material, behavioral, and psychosocial domains of financial well-being as defined by Tucker-Seeley et al.
Interview, Data Collection, and Analysis
Once informed consent was obtained, a research staff member (H.E.R.) conducted all interviews, and additional research team members were present to observe and take notes (A.J.H., A.J.L.). Each interview was conducted and recorded via virtual video; audio recordings were transcribed verbatim. Interviews lasted between 45 min to 1 h.
Members of the research team followed a qualitative descriptive approach 24 to analyze interview transcripts. Several team members collaborated to iteratively design and refine a codebook to capture the domains of financial well-being discussed by participants as well as direct and indirect costs. With the finalized codebook, 2 team members (H.E.R., A.S.) independently coded the transcripts following a deductive and inductive approach. Throughout this process, research team members met frequently to review procedures and discuss insights from the analysis. We identified and grouped themes into the 3 domains of financial well-being and along their intersections.
Results
We interviewed 11 PCa survivors with a median age of 68 y (interquartile range [IQR] 62–71.5 y) and 11 caregivers with a median age of 64 y (IQR 58.5–70.5; Table 1). Guided by the Measures of Financial Wellbeing framework, 23 we grouped themes into the 3 domains of financial well-being and described their intersections. These themes included 1) work and insurance status, 2) rearranging and adaptability, 3) the weight of indirect costs, 4) “I just paid it off,” 5) “It didn’t cross my mind at all,” and 6) “We know we can handle that” (Figure 2 and Table 2). Throughout our analysis, we observed significant co-occurrence between the domains, rather than distinct, mutually exclusive categories. Figure 2 and Table 2 illustrate the blending of these domains and their relationship with the themes we identified. Their co-occurrence is an important finding of our analysis and was critical in understanding participant experiences with financial hardship. The breadth of perspectives from survivors and caregivers reenforced similar themes; therefore, we present data from both participant groups together.
Survivor and Caregiver Sociodemographics
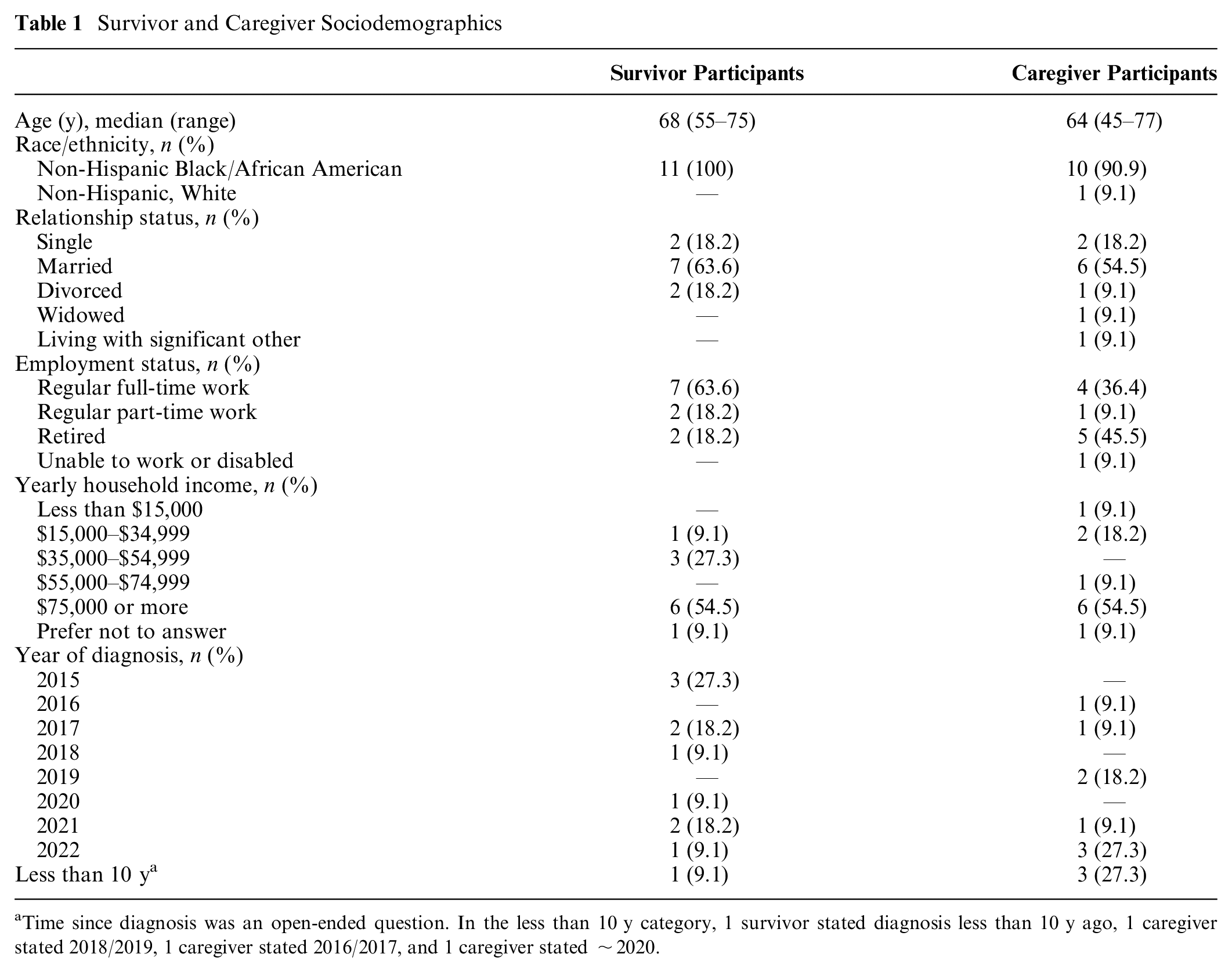
Time since diagnosis was an open-ended question. In the less than 10 y category, 1 survivor stated diagnosis less than 10 y ago, 1 caregiver stated 2018/2019, 1 caregiver stated 2016/2017, and 1 caregiver stated ∼2020.

Identified themes and corresponding domains of well-being.
Themes, Sample Quotes from Participants, and Identified Domains.

FMLA, Family and Medical Leave Act.
Work and Insurance Status
Participants consistently reported that their work and insurance status affected the availability of their financial resources and overall financial stress. For example, participants who were veterans or retirees noted minimal cost-related stress due to their comprehensive insurance coverage (i.e., insurance through the military, Medicare, etc.). A survivor participant noted, “As far as the financing part, between [military insurance type] and [insurance type], I knew I was covered. So, I never really had any concerns about how I would pay” (survivor participant 9). In addition, because retirees and their caregivers did not rely on full-time income, they did not experience any loss of income during treatment, thus reducing overall financial stress.
Financing PCa treatment was more of a challenge for participants who were nonveterans, Medicare beneficiaries, or individuals with low levels of insurance coverage. In some cases, caregivers considered bringing survivors onto their own health care plans because theirs offered more coverage. One caregiver shared, “If things got to the point that they was real bad . . . I was gonna claim him as a dependent and get him on my insurance through the military” (caregiver participant 8). These participants also spent more time negotiating with hospital systems and insurance companies.
Rearranging and Adaptability
Survivor and caregiver participants reported the need to be adaptable throughout their treatment journey to meet the changing circumstances. For some, this meant reorganizing their day-to-day spending to leave enough for making treatment-related payments. Participants noted that it was significantly time-consuming and difficult to manage these adjustments, especially without previous experience reorganizing budgets. One caregiver shared, “So all of that stuff was new, you know, on trying to make sure we managed everything ’cause I done got this bill. Well right now we don’t have no money because he’s not working” (caregiver participant 6). This same participant noted that covering treatment costs required them to stop paying all their regularly scheduled payments for a period, including their mortgage, electric, gas, water, internet, and cell phone bills. Another caregiver participant reported,
It’s not that we have money because we’re definitely, you know, neither one of us are rolling in dough . . . but he knows he has insurance. But I know that a lot of times insurance doesn’t cover everything. And so if cost was a factor, I told him if it means me having to sell my home, if it means you having to sell your home—a house is nothing but bricks with dirt, okay? (caregiver participant 5)
Despite potentially limited insurance coverage, this participant was willing to adapt to the circumstances even with extreme measures, such as selling their home.
Some survivors relied on family members to help cover their household payments during their treatment until they were able to return to work. For example, a survivor participant noted, “For my mortgage and everything, my father and my sons, they took care of all that. So, they took care of all the normal bills until I was able to get back to work” (survivor participant 8). In the case of caregivers, some contributed from their personal finances to financially support their care recipients during treatment. One caregiver shared, “My sister and my other brother . . . was able to help, but you know, a lot of it still fell on me” (caregiver participant 8).
The Weight of Indirect Costs
Survivor and caregiver participants encountered a wide variety of indirect costs, which had different effects on their financial behaviors. Many participants reported indirect costs related to transportation, such as time and gas required to travel to and from appointments or the money required to pay for parking at treatment facilities. Others needed to order ride-share services to and from treatment. One survivor shared, “I live alone. I don’t have my own personal transportation, so, I Uber [to my appointments]. I use Uber a lot” (survivor participant 7). Some caregivers noted the cost of gas or transportation between their home and that of their care recipient as well as to appointments. For some, these were major unforeseen costs that added to their routine spending.
In addition, participants experienced indirect costs associated with time off work. One caregiver noted, “[Caregiving] just affected the need to rearrange the budget to be able to get back up [to him] when I needed to and to do the things I needed to do for him” (caregiver participant 11). For survivor and caregiver participants, time off meant anywhere between a few weeks and a few months without regular pay. Even for participants who were retired from full-time work, this meant pausing part-time jobs that they relied on for extra income. One survivor explained,
I was retired, but I still had little jobs on the side to make extra money, and all of that stopped. So, the little extra money that I was able to help pay my obligations, I wasn’t able to do that during that period. (Survivor participant 4)
“I Just Paid It Off”
This theme describes how participants felt about financing PCa treatment. When we asked participants how they managed their treatment payments, several noted that they conceptualized these payments the same way they do other regular payments in their life. For example, one participant said, “it feels like paying a regular utility bill. Just a bill” (survivor participant 8). Survivor and caregiver participants shared that they quickly accepted the reality around their treatment costs and focused on paying them off. They knew the bills would come and that they would need to be paid and seemed to cope with this through acceptance and paying what they could, when they could. For example, a caregiver participant shared, “I was like, ‘Okay. It’s just gonna be another bill.’ You know? We’re just gonna pay ‘em whatever we can each month” (caregiver participant 6).
“It Didn’t Cross My Mind at All”
When confronted with their PCa diagnosis, participants did not immediately consider their treatment costs. Even for participants who knew that financing PCa treatment would be a challenge, worrying about costs was not the primary concern when facing a serious disease. For example, a survivor participant reported, “money was not an object. I just wanted to get rid of [the cancer]” (survivor participant 2). Many participants noted that despite potential financial barriers, pursuing successful treatment was the priority. Another survivor participant shared, “I really was more concerned about my health. And whatever it took to do this, I woulda made it work for myself” (survivor participant 5). Even as costs began to accumulate, participants reported that they remained focused on their or their care recipient’s healing and not on finances. A caregiver participant noted, “[The costs] became a lot. But we wanted his life to continue, so we just didn’t worry about it” (caregiver participant 7). When comparing treatment costs to loss of life, financial concerns seemed small, regardless of whether making payments was challenging.
“We Know We Can Handle That”
Both survivor and caregiver participants commented on their experiences with weighing their treatment costs and finding confidence in their ability to pay them. For some, the knowledge that they had some level of insurance coverage was enough to help them feel at ease. A survivor participant shared, “I talked with my wife, but most of the time it was always talkin’ about my illness, the treatments, things of that nature . . . ’cause we already knew that we had insurance” (survivor participant 1). Others noted that reviewing available cost information, such as explanation of benefit statements, allowed them to conceptualize and become comfortable with the amounts they might owe. For example, a caregiver participant noted, “we have gotten the benefit statements saying, ‘This is what you might owe,’ you know. And so we have a comfort level, and we know we can handle that” (caregiver participant 1). Some survivor and caregiver participants reported having the perception that treatment costs would not and did not cause them complete financial desolation and were therefore manageable.
Discussion
This study contributes to the understanding of the direct and indirect costs incurred by survivors and caregivers during PCa treatment and furthers the complex effort to define and measure these costs. Survivors and caregiver participants reinforced the identified themes from their perspectives. Specifically, participants emphasized how work and insurance status affected the availability of their financial resources and the need to adjust their financial behaviors accordingly. Participants encountered indirect costs encompassing many categories but seemingly coped by quickly accepting them and paying them off as they could. For many, costs did not come to mind in the face of a cancer diagnosis, and when they did, participants worked to develop a plan for affording them. Overall, survivors and caregiver participants highlighted the need to adapt to the financial circumstances that PCa treatment required.
Our findings contribute to this body of research by advancing our understanding of the lived experiences of Black PCa survivors and caregivers when navigating direct and indirect costs. Many of the themes identified in this analysis highlight the growing need for cost transparency to support medical decision making,4,12,25 identifying opportunities to screen early for financial hardship, and allowing patients and caregivers to prepare and plan for the financial burden associated with treatment-related costs, 26 specifically, advancing opportunities to support patient-centered communication and information exchange between clinicians and patients.27,28 Affording both the direct and indirect costs associated with treatment required survivor and caregiver participants to make significant adjustments to their financial, professional, familial, and personal behaviors. Participants reported a wide variety of these rearrangements, including halting contributions or withdrawing from personal savings, taking unpaid time off work, or foregoing activities and opportunities, such as continuing education. For those who had not previously needed to make such drastic adjustments, especially in response to indirect costs, reorganizing their financial behaviors came with a learning curve. In current practice, PCa patients and their caregivers are often expected to wait for bills to arrive and then independently navigate the insurance systems to clarify, potentially negotiate, and pay their treatment costs. This system places much of this burden on patients and caregivers. Survivor and caregiver participants alike spent significant time and energy discerning how to manage medical bills and unforeseen costs. Providing cost information early in the treatment journey, both on direct and indirect costs, could allow patients and their caregivers not only to make increasingly informed decisions about their care but also to proactively plan for financial adjustments. It is important to note that while many participants described prioritizing their medical care over financial well-being, the weight of the required adjustments was significant and had lasting impacts past their treatment and into survivorship. Both participant groups expressed a lack of agency over their financial situations, noting that there was nothing they could do to control their costs, and so they had to focus on treatment instead. Although they did work to adapt to their circumstances, this does not justify the level of financial burden placed on survivors and their caregivers. Therefore, the impetus for initiating cost conversations should be undertaken by clinical staff rather than placing the burden on the patient who is already navigating a highly stressful and complex diagnosis and care pathway.
The co-occurrence of the domains of financial well-being among identified themes introduces an opportunity for consolidating cost-sharing intervention efforts. Our analysis demonstrates that neither survivors nor caregivers experienced the domains of financial well-being in isolation of one another but rather across a spectrum. These findings advance the extant literature describing the multiple subjective and objective factors associated with these domains. 29 Interventions and policies designed to deliver cost information to cancer patients and their caregivers should therefore target these domains collectively, rather than separately. While components of the material domain, such as work and insurance status, affected the availability of financial resources, they also required significant rearranging of individual and household budgets (aspects of the behavioral domain) and influenced perceptions of financial stability and security (aspects of the psychosocial domain). Financing PCa treatment required survivor and caregiver participants to navigate each of these domains simultaneously, highlighting the importance of delivering interventions and policies that holistically target all domains of financial well-being. This also involves considering multiple levels of influence across the domains, including individual patient, social, and policy levels. In addition, it is noteworthy that participants reported the impacts of direct and indirect costs across stage at diagnosis. Financial burden was described by survivors and caregivers of those with advanced PCa and those with localized disease.
This research is not without limitations. While we used purposive sampling to recruit survivor and caregiver participants with a range of experiences with PCa treatment, none of our participants were uninsured, and more than half reported an average annual income of $75,000 or more. However, even among this sample, participants shared their substantial financial hardships and we were able to use purposive sampling to recruit Black PCa survivors and many Black caregivers to center their voice and experience in this research. In addition, while we recruited participants within the first 10 y of survivorship to characterize costs near diagnosis, future work should explore how perceptions and experiences across the domains of financial well-being evolve over time for Black PCa survivors and caregivers. Our recruitment occurred in a Midwestern city in the United States and may not be generalizable to all US regions. Future qualitative research may explore lived experiences among various sociodemographic groups to further our understanding of costs related to PCa survivorship.
We aim to apply these findings to support higher-quality decision making with the use of a patient decision aid. Future work will be to incorporate these qualitative data in combination with the quantitative data we have collected on estimated health care costs associated with localized PCa. 30 We plan to pilot test the patient decision aid containing these data in a larger implementation trial. In addition, there are opportunities to expand this work beyond PCa for other cancer types.
Supplemental Material
sj-docx-1-mpp-10.1177_23814683241282413 – Supplemental material for “I Just Had to Do What I Had to Do”: Characterizing Direct and Indirect Prostate Cancer Treatment Costs for Black Survivors and Their Caregivers
Supplemental material, sj-docx-1-mpp-10.1177_23814683241282413 for “I Just Had to Do What I Had to Do”: Characterizing Direct and Indirect Prostate Cancer Treatment Costs for Black Survivors and Their Caregivers by Hannah E. Rice, Allison J. L’Hotta, Amela Siječić, Bettina F. Drake, Su-Hsin Chang, Eric H. Kim, Robin Wright-Jones, Mellve Shahid, Camille Neal and Ashley J. Housten in MDM Policy & Practice
Footnotes
Acknowledgements
We would like to acknowledge and thank all study participants for sharing their experiences with our team.
Authors’ Note
The results of this research were presented at the Society for Medical Decision Making Annual North American Meeting in Philadelphia, Pennsylvania (October 2023).
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RW-J and MS were employed by The Empowerment Inc., United States. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided, in part, by The Implementation Science Centers in Cancer Control (ISC3; Beau Biden Cancer Moonshot Initiative; NCI P50 CA244431) and Washington University and Siteman Cancer Center Institutional matching funds, CTSA grant UL1 TR002345. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
Study Approval
This research project was approved by the Washington University in St. Louis School of Medicine Institutional Review Board, protocol No. 202202157.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.