
Abstract
Highlights
Shared decision making in DART is influenced by various barriers and facilitators present at the patient, provider, organizational, and health system levels.
Patients need education, and health care staff need regular training to improve SDM in DART service provision.
Patient access to decision support tools that aid in the selection of the preferred DART model in health facilities is critical.
Policy makers and program managers shall consider the availability of adequate and trained human resources as well as provide adequate space and private rooms for SDM in the implementation of DART.
Keywords
Introduction
During the early stage of antiretroviral therapy (ART) expansion, most countries used clinic-based model largely undifferentiated for individual needs.1,2 Since 2015, the World Health Organization (WHO) 2 has recommended ART through differentiated service delivery (DSD). DSD is a person-centered approach that streamlines and adapts human immunodeficiency virus (HIV) services across the cascade in ways that satisfy the needs of individuals living with and vulnerable to HIV while also optimizing the available resources in health systems. 3 The principles of DSD can be applied to prevention, testing, linkage to care, ART initiation, and follow-up and integration of HIV care and coinfections and comorbidities. DSD for ART has focused primarily on clinically stable people (established on ART). 2 The WHO has developed criteria for determining whether a person has been successfully established on ART. The criteria include receiving ART for at least 6 mo; no current illness, which does not include well-controlled chronic health conditions; good understanding of lifelong adherence: adequate adherence counseling provided; and evidence of treatment success: at least 1 suppressed viral load result within the past 6 mo (if viral load is not available: CD4 cell count >200 cells/mm3 or weight gain, absence of symptoms and concurrent infections). For children 3 to 5 y, the criterion is CD4 cell count >350 cells/mm3. 2
Since 2016, several Sub-Saharan African (SSA) nations have implemented differentiated antiretroviral therapy (DART) as part of DSD.2,4,5 Effective DART model implementation reduces the burdens for clients and health systems and improves patient outcomes (treatment adherence, retention in care, and viral suppression).3,6–8 Ethiopia adopted the appointment spacing model (ASM) at the end of 2016 9 and now is implementing 5 less-intensive (LI) models, namely, ASM, 3 multimonth dispensing (3MMD), fast-track antiretroviral refill (FTAR), health extension professional managed community ART refill group (HEP_CAG), and peer-led community-based ART distribution (PCAD). 10
Shared decision making (SDM) is considered one of the integral building blocks of patient-centered care. 11 It has been defined as “an approach where clinicians and patients make decisions together using the best available clinical evidence and the patient’s informed preferences.” 12 The SDM process includes several important components: 1) creating a context in which patients’ views on treatment options are valued and considered essential, 2) transferring technical information and ensuring that patients understand it, 3) helping patients make informed decisions based on the best evidence available, 4) eliciting patients’ preferences and sharing treatment recommendations, and 5) making the component of uncertainty in the clinical decision-making process clear.13,14 In the context of implementing LI DART models, SDM means that patients on ART are encouraged to weigh the risks and benefits of available models and select the best model for themselves. The Ethiopian HIV Care and Treatment Guideline 10 recommends the use of the patient’s willingness to provide informed consent to receive ART service based on his or her preferred LI DART model as one of the criteria to declare the client’s eligibility for LI DART models. The guideline states that “after appropriate classifications based on the criteria, clients should be informed and give verbal consent on type of the service delivery model they prefer.” The implementation guide for community-based DART service delivery models in Ethiopia also recommends ART service providers shall educate and counsel all clients on ART and obtain consent from patients for community-based drug refilling. 15
As with other illnesses, optimal ART is thought to depend on substantial patient engagement in their care.16–18 According to a US survey, roughly 23% of HIV patients wanted their doctor to make the decision to start ART, 63% wanted to discuss decisions with their doctor, and 13% wanted to make all final decisions on their own. 19 Nearly similar findings were reported in another study in the United States, where 72% of HIV patients chose to share decisions with their physician, 23% wanted their doctor to make decisions, and 5% wanted to make treatment decisions alone. 20 A qualitative study of HIV patients who were established in ART but did not select their DART model in Ethiopia revealed that most participants preferred to make their own decisions about what DART model to use next, whereas others wanted the provider to decide for them. Some valued reaching a consensus and having SDM. 21
A US study on the relationship between HIV patients’ preferred involvement in the decision to start ART and medication adherence found that HIV patients who preferred SDM were more likely to adhere to ART than those who preferred that their providers make decisions. 19 Salient and viable differences between options, comorbidities or current health status, trust in the provider, perceptions of agency, and attitudes about decision-making roles were among the factors that could facilitate or impede SDM in routine HIV care including initiating ART revealed by a study in the United States. 22 A study in 25 countries indicated that the perception that nothing could be done, providers never bringing up the issue, and not wanting to appear difficult were major reasons for people living with HIV (PLHIV) on ART not discussing their concerns with their providers. 23
SDM has not yet been extensively used in practice in Africa compared with other parts of the world. Health care professionals have limited decision-making tools available to them, and most are not designed to support their decision making with patients. Other than specific health care programs (COVID-19, HIV/AIDS, and maternal/neonatal care), there are no SDM trainings available for health care workers. Implementing SDM faces many barriers, such as a dearth of options, inadequate health resources, and low educational attainment.24,25 There are no studies indicating the previous use of SDM for LI DART in Africa including Ethiopia. The current study aimed to explore the barriers and facilitators in implementing SDM during the choice of care models from the perspectives of patients and providers in Awi, East Gojjam, and West Gojjam zones and Bahir Dar City Administration in Northwest Ethiopia, which aids both decision and policy makers and service providers to improve the implementation of patient-centered DART service delivery in Ethiopia.
Methods
Study Setting and Period
The study setting included 15 health facilities including 9 health centers (Abay, Bahir Dar, Bichena, Dangila, Debre Markos, Finote Selam, Han, Shimbt and Tis Abay), 3 primary hospitals (Addis Alem, Bichena and Dangila), 1 general hospital (Finote Selam), and 2 comprehensive specialized hospitals (Debre Markos and Felege Hiwot) in Awi, East Gojjam, and West Gojjam zones and Bahir City Administration located in the northern part of Ethiopia. Data were collected between June 3 and June 27, 2023.
Study Design
A qualitative descriptive study was conducted. This study design is useful for a comprehensive summary of a subject and provides a direct description of a phenomenon. 26
Study Population
The study population included ART service providers and stable PLHIV aged 18 y and older enrolled in 1 of the 5 LI DART models at the ART clinics mentioned in the study setting. As per the Ethiopian HIV care and treatment guideline, the criteria for being eligible for LI DART models include 1) patients on ART for at least 6 mo; 2) no current illness, which does not include well-controlled chronic health conditions such as hypertension or diabetes mellitus; 3) good understanding of lifelong adherence, with adequate adherence counseling provided (a patient with an adherence level of 95% for the last 6 mo); 4) evidence of treatment success (at least 1 suppressed viral load result [i.e., <50 c/mL] and if no viral load result, a patient with rising CD4 cell count or CD4 cell count >200 cells/mm3); 5) age >5 y; 6) no current opportunistic infections; 7) no adverse drug reactions and does not need careful clinical monitoring; and 8) willing to provide consent to get the ART service based on his or her preferred LI DART model. 10 Providers were eligible if they were physicians, nurses, or health officers directly prescribing antiretroviral drugs and had worked in the ART clinic for at least 6 mo.
There are practical recommendations for using a SDM process in DART service delivery sites in the study settings. However, there are no decision aids that support formal SDM processes in the practice sites.
Sampling
Previous recommendations suggest a minimum sample size of 12 for qualitative studies to achieve data saturation.27–29 We initially conducted interviews with 12 patients and 12 providers. An additional 5 patients and 3 providers were invited and recruited until thematic saturation was attained. In total, 17 in-depth interviews with patients and 15 key informant interviews with providers were conducted. A purposive sampling technique was used to identify and select participants with knowledge or experience in LI DART model decision making. Participants were recruited from different facilities (tertiary hospital, general hospital, primary hospital, health center) and enrolled in the 5 LI DART models, and a mix of providers was included (physicians, nurses, and health officers) to gain information from many perspectives.
Development of the Data Collection Tool and Data Collection Procedure
Data were collected using independently developed, translated, and pretested semi-structured interview guides for patients and providers (Supplementary File 1 and Supplementary File 2). The interview guide for patients consists of 6 sections, including 1) awareness of DART model options, 2) perceptions of SDM, 3) familiarity with SDM, 4) a description of SDM, 5) barriers and facilitators to SDM, and 6) strategies to improve the execution of SDM. The provider interview guide consists of 7 sections, including 1) awareness of DART model options; 2) awareness, perception, and experience with SDM; 3) a description of SDM; 4) use of decision aids; 5) training about SDM; 6) barriers and facilitators to SDM; and 7) strategies to improve the execution of SDM. In this article, we present the analysis for the barriers and facilitators to implementing SDM during DART model selection.
While developing the interview guides, the researchers conducted a literature review on similar topics to determine the constructs of interest. The interview guides were prepared in English by the researchers themselves. Then the translation of the tools into Amharic (a local language) was done by 2 experts (1 subject matter and 1 language) who were fluent in both languages. One physician and 1 public health professional, both with master’s degrees in public health and having extensive experience in the HIV/AIDS program, reviewed the guides. The interview guides were pretested on 4 participants, 2 from each group, at Debre Markos health center and Felege Hiwot comprehensive specialized hospital (2 interviews per health facility).
Two trained bilingual health professionals (1 male, 1 female) who have master’s degrees in health promotion, taught at universities, and have extensive experience in conducting qualitative interviews participated in the data collection. They received 1-d training on interview guides, DART, SDM, ethics, and interview conduct. All interviews were tape recorded. The length of the interviews ranged from 30 to 80 min. Field notes were written during and after the interviews. The principal investigator (Y.A.B.) supervised the data collection process. The principal investigator (Y.A.B.) possessed significant expertise in clinical care (including HIV/AIDS), public health practice, academics, conducting interviews, analyzing data, and publishing qualitative research.
Data Management and Analysis
Before data analysis began, participants’ responses from audio recordings were transcribed verbatim and then translated into English by bilingual researchers. The translated data were imported to the MAXQDA version 20 software for coding. A thematic analysis was done. A 4-step process adapted from Bingham 30 was followed during the data analysis. In the first phase, data organization was done by detailed file labeling when importing data into MAXQDA software. In the second phase, inductive coding was done independently by the 2 researchers. There was no major conflict with the codes, and minor differences were resolved by 1 researcher. The third phase involved identifying, verifying, and reaching a consensus on themes among the research staff. In the final phase, reporting of the findings was done following the consolidated criteria for reporting qualitative studies (COREQ) 31 (Supplementary File 3).
Trustworthiness of the Study
To ensure the credibility of the study, data triangulation by interviewing multiple participants at different health facilities and methodological triangulation through in-depth and key informant interviews were done. Spending long periods in the field to build trust with the study participants was done. Moreover, 3 transcripts (1 for the patient and 2 for the provider) were sent to selected participants and helped us to obtain additional clarification of information. A thick description of the findings, verbatim quotations, and purposive selection of study locations and informants was made to ensure the transferability of the findings to similar contexts. Records of the raw data, field notes, transcripts, translations, and reports were kept in well-organized archives for future use, and participants were given the researchers’ personal and academic information for contact or explanation at any time to enhance dependability. Moreover, confirmability was ensured through expert review and a pretest of guides. The findings from the pretest were not included in the final report.
Results
Participant Characteristics
A total of 19 patients and 16 providers were approached. Two patients and 1 provider were unable to participate in an interview because they were too busy. Overall, 17 PLHIV enrolled in 1 of the 5 LI DART models, and 15 providers were interviewed. Eleven patients and 9 providers, respectively, were females. The majority of both types of participants were from 1 of the 9 health centers. Six patients were enrolled in the ASM, 1 in FTAR, 5 in PCAD, and 5 in the HEP_CAG model. Nine of the provider participants were nurses in their profession (Table 1).
Sociodemographic Characteristics of Participants in Northwest Ethiopia, 2023

ART, antiretroviral therapy; DART, differentiated antiretroviral therapy.
Barriers to and Facilitators of SDM during DART Model Selection
Ten themes emerged at 4 levels related to SDM in the provision of DART: patient, provider, organizational, and health system. Below we discuss each theme grouped by level and with illustrative quotations to support each theme. More barriers than facilitators were reported by patients and providers to SDM during DART model selection (Table 2).
Barriers to and Facilitators of Implementation of Shared Decision Making in Differentiated Antiretroviral Therapy Service in Northwest Ethiopia, 2023
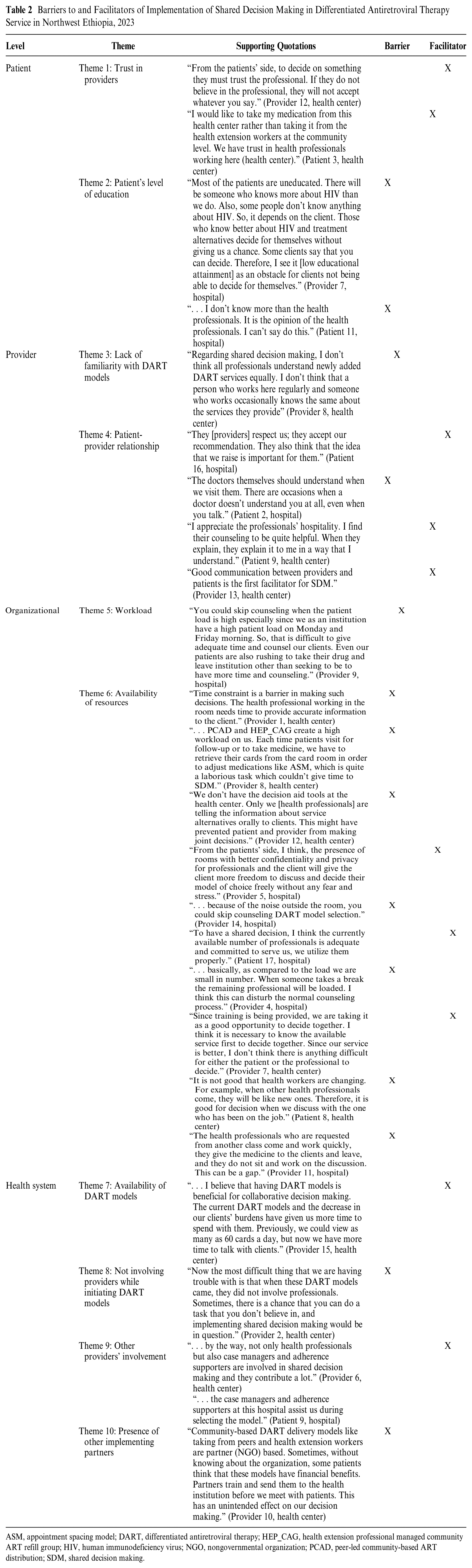
ASM, appointment spacing model; DART, differentiated antiretroviral therapy; HEP_CAG, health extension professional managed community ART refill group; HIV, human immunodeficiency virus; NGO, nongovernmental organization; PCAD, peer-led community-based ART distribution; SDM, shared decision making.
Patient Level
Trust in providers and patient’s education status were the 2 themes that emerged at the patient level.
Theme 1: Trust in providers
Providers and patients reported that trust in health care workers was a facilitator for SDM. The providers emphasized that patients’ trust in their providers is a must before deciding on treatment option.
From the patients’ side, to decide on the DART model they must trust the professional. If they do not believe in the professional, they will not accept whatever you say. (Provider 12, health center)
Patients also mentioned a trust in the providers led them to continue taking medication from the same health facility rather than considering other options.
I would like to take my medication from this health center rather than taking from the health extension workers at the community level. We have trust in health professionals working here. (Patient 3, health center)
Theme 2: Patient’s level of education
Providers stated that one of the barriers to involving patients in the SDM process was their inability to comprehend information provided on the risks and benefits of available DART models. They explained that patients’ involvement in decision making is based on their educational attainment; those with greater knowledge of HIV and available models make decisions more readily, whereas most patients lack education and defer to their providers.
Most of the patients are uneducated. There will be someone who knows more about HIV than we do. Also, some people don’t know anything about HIV. So, it depends on the client. Those who know better about HIV and treatment alternatives decide for themselves without giving us a chance. Some clients say that you can decide. Therefore, I see it [low educational attainment] as an obstacle for clients not being able to decide for themselves. (Provider 7, hospital)
Professional Level
Lack of familiarity with the existing DART models and the patient-provider relationship were the 2 themes that emerged from the health care professional level.
Theme 3: Lack of familiarity with DART models
Providers’ lack of familiarity with available DART models was mentioned as the barrier to implementation of SDM during DART model selection from the providers’ perspective. The providers fail to present and inform the pros and cons of DART models. Some providers have a concern that different professionals (who work regularly versus infrequently in the room) have different understandings of newly introduced DART models, which brings a challenge to deciding with a patient.
Regarding SDM, I don’t think all professionals understand newly added DART models equally. I don’t think that a person who works here regularly and someone who works occasionally knows the same about the model they provide. (Provider 8, health center)
Theme 4: Patient-provider relationship
The patient-provider relationship was reported as a barrier and facilitator of SDM. Listening to and respecting the concerns or opinions of patients was found as both a barrier and facilitator of SDM from the patients’ perspective. Health professionals who make an effort to understand each patient’s needs and preferences encourage participation in SDM.
They [providers] respect us; they accept our recommendation. They also think that the idea that we raise is important for them. (Patient 16, hospital)
On the other hand, other patients mentioned that a lack of listening and respecting patients’ concerns was a barrier to SDM.
The doctors themselves should understand us when we visit them. There are occasions when a doctor doesn’t understand you at all, even when you talk. (Patient 2, hospital)
From the viewpoints of both patients and providers, strong interpersonal skills among providers were perceived as a facilitator of SDM
I appreciate the providers’ hospitality. I find their counseling to be quite helpful. When they explain, they explain it to me in a way that I understand. (Patient 9, health center) Good communication between providers and patients is the first facilitator for SDM. (Provider 13, health center)
Organizational Level
Two themes emerged from the organizational level. These were workload and the availability of resources.
Theme 5: Workload
From the providers’ perspective, the workload at the health facility was reported as a barrier to engaging providers and patients in SDM.
You could skip counseling when the patient load is high especially since we as an institution have a high patient load on Monday and Friday morning. So, that is difficult to give adequate time and counsel our clients. Even our patients are also rushing to take their drugs and leave institution other than seeking to be to have more time and counseling. (Provider 9, hospital)
Theme 6: Availability of resources
The availability of resources theme had 4 subthemes: time, decision support tool, service delivery room, and human resource situation. We have presented these subthemes below.
Time
Providers expressed concerns about the heavy workload caused by the newly introduced PCAD and HEP-CAG models. They felt that this increased their workload thereby limited their time for SDM with patients.
PCAD and HEP_CAG create a high workload on us. Each time patients visit for follow-up, we have to retrieve their cards from the card room in order to adjust medications, which is quite a laborious task that couldn’t give time to SDM. (Provider 8, health center) Time constraint is a barrier during DART model selection decision. The provider working in the room needs time to provide accurate information to the client. (Provider 1, health center)
Decision support tool
Providers reported a lack of patient decision aids at health facilities that explain the benefits and risks of DART models as a barrier to meaningful conversations between provider and patient.
We don’t have the decision aid tools at the health center. Only we [providers] are telling the information about models orally to clients. This might have prevented patient and provider from SDM during model selection. (Provider 12, health center)
Service delivery room
Providers expressed varying opinions on the role of the ART service delivery room for SDM practice. Some providers highlighted the availability of a convenient ART room in the ART clinic as a facilitator to undertake SDM during model selection.
From the patients’ side I think, the presence of rooms with better privacy will give the client more freedom to discuss and decide their model of choice freely without any fear and stress. (Provider 5, hospital)
Some providers, on the other hand, cited noisy environments where the ART service was close to other non-HIV service delivery rooms as a barrier to SDM.
. . . because of the noise outside the room, you could skip counseling during model selection. (Provider 14, hospital)
Human resource situation
Staff adequacy, training, change of providers, and working by coming from other rooms were further subthemes that emerged under the human resource subtheme. Participants perceived the staff adequacy as both a barrier and a facilitator to SDM. For example, a patient at the hospital stated, “To have a shared decision, I think the currently available number of providers is adequate and committed to serving us, we utilize them properly” (patient 17, hospital).
On the other hand, a provider at the hospital mentioned the shortage of staff as a barrier to having SDM. He stated, “basically, as compared to the load we are small in number. When someone takes a break the remaining provider will be loaded. I think this can disturb the normal counseling process” (provider 4, hospital).
The availability of trained staff was perceived as a facilitator for SDM from the providers’ perspective. From the patients’ view, patients mentioned not having the same provider (change of provider) in every visit as a barrier for SDM.
It is not good that providers are changing. For example, when other providers come, they will be like new ones. Therefore, it is good for decision when we discuss with the one who has been on the job. (Patient 8, health center)
Working by rotating from other rooms was also cited as a barrier to implementing SDM reported by providers.
The providers who are requested from another class come and work quickly, they give the drug to the clients and leave, they do not sit and work on the discussion. This can be a gap. (Provider 11, hospital)
Health System Level
The 4 themes that emerged in the health system level were the availability of the DART model, not involving providers while initiating DART models, other providers’ involvement, and the presence of other implementing partners.
Theme 7: Availability of DART models
According to the providers’ view, the DART model program made it easier for patients to participate in SDM.
I believe that having DART models is beneficial for SDM. The current DART models and the decrease in our clients’ burdens have given us more time to spend with them. Previously, we could view as many as 60 cards a day, but now we have more time to talk with clients. (Provider 15, health center)
Theme 8: Not involving providers while initiating DART models
Providers mentioned that not engaging providers during the initiation of DART models as a barrier to implementing SDM during care model selection.
Now the most difficult thing that we are having trouble with is that when these DART models are coming through either the ministry of health or health office, they did not involve providers at the design stage. Sometimes, there is a chance that you can do a task that you don’t believe in and implementing SDM would be in question. (Provider 2, health center)
Theme 9: Other providers’ involvement
It has been noted by providers and patients that the involvement of trained nonclinical staffs (PLHIV volunteers) such as adherence case managers and adherence supporters facilitates SDM. In Ethiopia, adherence case managers engage in adherence counseling, supporting index case family testing, screening for mental illness, and linking to treatment, facilitating referral linkage with community resources, patient tracking, and education and support. Adherence supporters facilitate intra- and interfacility referral linkage, track patient appointments, and conduct tracing for lost patients. 32
. . . by the way, not only providers but also case managers and adherence supporters are involved in SDM and they contribute a lot. (Provider 6, health center) . . . the case managers and adherence supporters at this hospital assist us during model selection. (Patient 9, hospital)
Theme 10: Presence of other implementing partners
Some providers have expressed their perceptions that the practice of some nongovernmental organizations (NGOs) in community-based DART models hinders patients’ ability to collaborate with providers on decisions, as the NGOs are generating needless demands by organizing patients at the community level.
Community-based DART models like taking from peers and health extension workers are NGO based. Sometimes, without knowing about the organization, some patients think that these models have financial benefits. Partners train and send them to the health institution before we meet with patients. This has an unintended effect on our decision making. (Provider 10, health center)
Discussion
To the best of our knowledge, this is the first study that explored the barriers and facilitators to implementing SDM focused on DART model selection from the perspective of providers and patients in Ethiopia. This could add insights to the existing body of literature. This study identified themes that emerged across 4 levels relevant to SDM in DART: patient, provider, organizational, and health system.
Patient Level
In the current study, patients’ trust in their providers was reported as a facilitator by both patients and providers. Patients who trust their doctors are more likely to feel safe discussing treatment options openly. A previous study in the United States 22 found that trust in the provider could work in favor or against SDM (patients may accept or defer to their provider for decisions if they have a high degree of trust in them). We also found that the patient’s low educational attainment was a barrier to SDM. When involved in SDM, patients with low education levels may fail to absorb and understand the benefits and risks of all DART models informed by providers. This finding is supported by a systematic review of the barriers and facilitators of SDM in hospitals 33 and umbrella review. 34
Provider Level
The patient-provider relation was found as enabling and hindering for successful implementation of SDM. Patients fully engage in model decisions when there is a trusting patient-provider relationship. Patients need providers to respect, listen, and understand their concerns or opinions. On the contrary, a lack of a good patient-provider relationship was a barrier to SDM. Previous HIV-based studies in the United States, 22 Kenya, 35 Austria, 36 and the United States, Puerto Rico, and Botswana 37 ; a survey of PLHIV from 25 countries 23 ; and an umbrella review of SDM-based studies in health care 34 similarly found that the patient’s trust in the provider could work for or against SDM.
Providers’ lack of familiarity with available DART models was reported to be a barrier to implementing SDM. Providers had varying understandings of available DART models, especially newly introduced ones, which are perceived to create hurdles to SDM in clinical practice. Inadequate information provision from providers makes it difficult for patients to consider available treatment options. A systematic review and meta-analysis of randomized controlled trials in SSA also revealed that there was a lack of knowledge about DART models among providers, resulting in barriers to their adoption. 38 Another study in Uganda 39 similarly found that provider competence in DART was a bottleneck to delivering ART service in health facilities. This suggests that providers shall be the focus of continued training initiatives regarding the available DART options to successfully practice SDM in model selection.
Organization Level
A lack of patient support tools that explain the pros and cons of each DART model was reported as a barrier to implementing SDM in this study. Meaningful conversations between the provider and patient could be challenged in the absence of decision aids. An earlier umbrella review of the factors affecting SDM found that using decision aids was a facilitator. 34 According to a Cochrane systematic review, patients who have used decision aids report less decisional conflict associated with apathy in decision making, feeling misinformed, and uncertainty about personal values. 40 Decision support systems offer physicians summarized data about the risks and benefits of various options in the same way that they do for patients. 41 This has important implications for the need for policy support for the use of decision aids in DART service.
Time constraints due to the heavy workload for providers associated with the introduction of new community-based DART models (PCAD and HEP-CAG) have been identified as a barrier to SDM implementation. Time is required for consultations, and without providing additional time, SDM would be difficult to implement in practice. A study in the United Kingdom also revealed that time constraints, such as short consultation time or complex patients who require more time than usual, hindered effective participation in SDM in HIV care. 42 A scoping review into the explanations for differences in the degrees of SDM experienced by patients cited constraints on the time available to make an informed decision. 43 The finding of the current study contradicts the established belief that implementing DART models significantly increases providers’ capacity to spend more time communicating with patients as a result of the decongestion of health facilities. 2 PCAD and HEP_CAG in the study health facilities were in the pilot stage, which may have led to the difference by requiring providers to be occupied with preparation, demand creation, and social mobilization.
Regarding the clinical environment, the service delivery room was reported to affect both positively and negatively SDM mainly related to privacy protection. A convenient service delivery room in ART clinics was found to be a facilitator for SDM. On the other hand, the noisy setting with the ART service adjacent to other service delivery rooms was reported as a barrier to SDM. The umbrella review 34 also found that insufficient environmental conditions were a barrier to implementing SDM. This has policy implications in availing the convenient service delivery room for providing DART service and hence implementing SDM effectively.
Lack of trained and adequate human resources was found to be barrier to implementing SDM. A study in Zambia similarly concluded that limited human resources were a barrier to accommodating individual patient needs in HIV care. 44 Human resources for HIV/AIDS shortages are a major impediment to obtaining universal ART coverage in underdeveloped countries, and implementation of SDM could be in question. 45 This has relevant implications for policy makers and program planners to strengthen their investments in optimizing the health workforce for DART service delivery, thereby bringing better implementation of SDM.
Health System Level
The availability of the DART models was found to be facilitator for implementing SDM. The DART models decongest the health facilities, thereby giving the providers adequate time for discussion with their patients. This is in line with a qualitative study in Ethiopia 46 that reported decreased workload and therefore the ability for providers to have longer discussions with patients after the implementation of ASM in Ethiopia. This also has the policy support of WHO guidelines on DART service, which aimed to improve the efficiency of service delivery and bring client empowerment in addition to better adherence and client satisfaction outcomes. 47 In addition, this has relevant programmatic implications for the continued implementation of the DART models for better SDM practice.
The inclusion of trained nonclinical staff (PLHIV volunteers) such as adherence supporters and adherence case managers in HIV care emerged as a facilitator for SDM. They could help patients prepare for the SDM process. This is supported by an earlier study in which assistance from case managers improved SDM outcomes in a medication clinic. 48 Ethiopia included trained PLHIV in the workforce to provide social support and counseling to other HIV patients for rapid scale up of ART service. 49 This has relevant programmatic implications on the continued involvement of both case managers and adherence supporters in routine decisions during DART model selection.
The presence of other implementing partners was perceived as a barrier to SDM. The practice of some NGOs working with community-based DART models created a challenge in exercising the SDM activity since patients were mobilized to join these models. A study in Mozambique 50 similarly revealed that implementing partners were found to favor certain models over others, leading to a limited variety of models being implemented in the health facilities they supported. This has programmatic implications for reconsidering the demand creation and social mobilization activities of partners involved in the community-based DART model and the consequent practice of the SDM.
Limitations
This study has the following limitations. First, this study considered the perspectives of only patients and providers. It did not include interviews with policy makers, HIV/AIDS program managers, health care administrators, or experts working with development partners. Their perspectives would allow for further triangulation of the data. Second, the qualitative observation method, which allows us to better understand the process of SDM, was not undertaken due to ethical and feasibility concerns.
Conclusions
SDM implementation in DART is influenced by barriers and facilitators at patient, provider, organizational, and health system levels. Based on these findings, the following steps are recommended. To improve SDM in DART, health care staff needs regular training and patients’ levels of educational attainment should be raised. Health facilities should make patient decision aids available and work on using the support tools to assist patients in choosing their care models. To ensure proper SDM implementation in clinical practice, policy makers and program managers need to assess resources (training and size of human resources and convenience of rooms). Future research including policy makers, HIV/AIDS program managers, health care administrators, and experts working in NGOs shall be conducted to understand multilevel factors that influence SDM.
Supplemental Material
sj-doc-3-mpp-10.1177_23814683241281385 – Supplemental material for Barriers and Facilitators for Implementing Shared Decision Making in Differentiated Antiretroviral Therapy Service in Northwest Ethiopia: Implications for Policy and Practice
Supplemental material, sj-doc-3-mpp-10.1177_23814683241281385 for Barriers and Facilitators for Implementing Shared Decision Making in Differentiated Antiretroviral Therapy Service in Northwest Ethiopia: Implications for Policy and Practice by Yihalem Abebe Belay, Mezgebu Yitayal, Asmamaw Atnafu and Fitalew Agimass Taye in MDM Policy & Practice
Supplemental Material
sj-docx-1-mpp-10.1177_23814683241281385 – Supplemental material for Barriers and Facilitators for Implementing Shared Decision Making in Differentiated Antiretroviral Therapy Service in Northwest Ethiopia: Implications for Policy and Practice
Supplemental material, sj-docx-1-mpp-10.1177_23814683241281385 for Barriers and Facilitators for Implementing Shared Decision Making in Differentiated Antiretroviral Therapy Service in Northwest Ethiopia: Implications for Policy and Practice by Yihalem Abebe Belay, Mezgebu Yitayal, Asmamaw Atnafu and Fitalew Agimass Taye in MDM Policy & Practice
Supplemental Material
sj-docx-2-mpp-10.1177_23814683241281385 – Supplemental material for Barriers and Facilitators for Implementing Shared Decision Making in Differentiated Antiretroviral Therapy Service in Northwest Ethiopia: Implications for Policy and Practice
Supplemental material, sj-docx-2-mpp-10.1177_23814683241281385 for Barriers and Facilitators for Implementing Shared Decision Making in Differentiated Antiretroviral Therapy Service in Northwest Ethiopia: Implications for Policy and Practice by Yihalem Abebe Belay, Mezgebu Yitayal, Asmamaw Atnafu and Fitalew Agimass Taye in MDM Policy & Practice
Footnotes
Acknowledgements
We acknowledge the University of Gondar for funding this study. The authors wish to acknowledge the study participants and data collectors.
Authors’ Contributions
All authors participated in the conception and design of this study including data collection tool development. Y.A.B. transcribed, translated, coded, and analyzed the data. Y.A.B. drafted the manuscript. Feedback and editing were provided by M.Y., A.A., and F.A.T. All authors read and approved the final manuscript.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided by the University of Gondar. The fund was given to the corresponding author for data collection purpose. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
Ethics Approval and Consent to Participate
The Institutional Review Board of the University of Gondar granted ethical approval for this study(approval No. V/P/RCS/05/762/2021), and the Amhara Public Health Institute provided a formal permission letter. Participants provided written informed consent documenting willingness to participate in interviews.
Availability of Data and Materials
The datasets used during the current study are available from the corresponding author upon reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.