
Abstract
Highlights
Two prior studies examined the cost-effectiveness of screening followed by treatment for PTSD among individuals exposed to other disaster-type events (i.e., terrorist attack and Hurricane Sandy) and found screening followed by treatment (i.e., cognitive behavioral therapy [CBT]) to be highly cost-effective.
Among wildfire evacuees, screening followed by treatment with paroxetine or trauma-focused (TF)–CBT provides additional quality-adjusted life-years (QALYs) and is cost-saving from a societal perspective. TF-CBT was the treatment option found most likely to be cost-effective.
Neither treatment option was cost-effective at a willingness-to-pay threshold of $50,000 per QALY from a health care perspective.
Screening programs for PTSD should be considered for wildfire evacuees, and individuals diagnosed with PTSD could be prescribed either TF-CBT or paroxetine depending on their preference and resources availability.
Global climate change is resulting in devastating wildfires globally and in Canada, which are predicted to get worse as global temperatures continue to rise. 1 In 2016, the city of Fort McMurray, Alberta, was evacuated due to the Horse River Wildfire, 2 while nearly the entire town of Lytton, British Columbia, was destroyed by a devastating wildfire in 2021. 3 The year 2023 was the worst on record with an estimated 196,000 individuals evacuated due to forest fires as of mid-August. 4 Being evacuated from a wildfire results in a high risk of developing posttraumatic stress disorder (PTSD), 5 with a 3-month prevalence of PTSD of 29.1% among Fort McMurray evacuees, 6 a substantially greater prevalence than the general population’s lifetime prevalence (9.2%). 7 Although there are limitations to the sampling of this study (i.e., small sample and convenience sampling), the prevalence estimated from this study is very similar to the prevalence of PTSD estimated from a systematic review among individuals experiencing nonintentional trauma. 8 Postwildfire PTSD is a chronic issue with a 10-y prevalence of 7.6%, 5 which is more than 3 times the prevalence of the general population (2.4%). 7 Despite significant distress, reduced health-related quality of life (HRQoL), 9 and increased health care burden, 10 PTSD often goes undetected and untreated in primary care. 11
Trauma-focused cognitive behavioral therapy (TF-CBT) or treatment by selective serotonin reuptake inhibitors (SSRIs; e.g., paroxetine) 12 are typically recommended as first-line treatments for PTSD.12,13 Although TF-CBT is more effective (i.e., higher remission rate)14,15 and has negligible adverse effects, it costs more than 10 times as much as paroxetine. Moreover, it is not as easily implemented or accessible given it is usually administered by psychotherapists, who are a limited in number and whose services are often not covered by government-run health care plans.
Given there are tradeoffs between paroxetine and TF-CBT and that PTSD is highly elevated for a long period post wildfire, 5 modeling studies are needed to consider the dynamics of condition over time to appropriately estimate the impacts of treatment. Although there have been studies on the cost-effectiveness of different treatment options for PTSD15,16 and for screening for PTSD after other types of disasters (i.e., terrorist attacks, hurricanes),11,17 no studies have been conducted that examine the cost-effectiveness of different screening and treatment options in wildfire evacuees. Therefore, the objective of this study was to examine the incremental cost-utility ratio (ICUR) and incremental net monetary benefit (INMB; i.e., net monetary value of the health benefits) of screening followed by treatment with paroxetine or TF-CBT versus no screening in Canadian adult wildfire evacuees.
Methods
Study Design
An economic evaluation was conducted to evaluate screening followed by treatment with paroxetine or TF-CBT, both of which were compared with no screening for wildfire evacuees. Combining paroxetine and TF-CBT is not recommended as it is not more effective than individual treatments. 12 It was assumed that in the no-screening option, individuals would be treated with paroxetine as they seek care or are diagnosed over time. In the base case, it was assumed that all individuals who are offered treatment accept it. The target population was adults (≥18 y) evacuated from a region experiencing wildfires, regardless of whether their home or family members/friends were directly affected, given that there is a lack of evidence to suggest that the prevalence of PTSD meaningfully differs across other wildfire-specific exposures, such as property damage or injury. 5 Children were not examined since there were several school-based mental health–related programs implemented after the Fort McMurray wildfires. 18 Outcomes included quality-adjusted life-years (QALYs), costs, net monetary benefit (NMB), ICUR, and INMB. A QALY is a function of quality of life and length of life (e.g., 1 QALY is equivalent to a year spent in perfect health).
Screening
Individuals underwent a screening protocol similar to that of Hogan et al., 11 which mimicked the protocol implemented after the 2005 and 2017 London bombings. Individuals were first screened with the Trauma Screening Questionnaire at 3 mo, and those who screened positive completed a Structured Clinical Interview for DSM-5 (SCID-5). 11 We similarly assumed that the SCID-5 is 100% accurate, and false positives are screened out by this tool, but the tool has a false-negative rate, which we applied. 11 Screening occurred at month 3 and month 9 after the wildfire. 11
Model
The base case for the model was chosen to be a 30-y-old Canadian wildfire evacuee. A Markov model approach was used to simulate transitions between different health states of PTSD over time. The base-case time horizon was 5 y, given we modeled only the initial course of treatment, which lasted for 3 to 6 mo and aids comparison with other studies.11,17 A within-cycle correction was applied, and the Markov model cycle length was 1 quarter (3 mo).
Model States
The Markov model enabled individuals to transition between the following health states as shown in Figure 1: never PTSD, remitted PTSD, undiagnosed active PTSD, diagnosed active PTSD, diagnosed active PTSD with treatment, and a death-absorbing state (i.e., a state from which individuals cannot transition out). The effect of screening was modeled by shifting all individuals with PTSD initially (prevalence = 18.8% 8 ) from the undiagnosed active PTSD state to the diagnosed active PTSD with treatment state. Both undiagnosed active PTSD and diagnosed active PTSD with treatment were considered tunnel states, which enabled time-in-state specific remission rates for untreated PTSD.

Simplified state transition diagram of a wildfire evacuees.
Based on discussion with a psychiatrist (S.S.), the decision to not include mild-moderate-severe PTSD states was determined to be reasonable given this is not considered in treatment decisions.
Data
The data incorporated in the model were derived from the available literature (Table 1). The probabilities of diagnosis of PTSD over time without screening were specific to wildfire victims. 19 It was assumed that wildfire-induced PTSD had similar values for other parameters compared with PTSD induced by other forms of trauma given a lack of parameters specific to this population. This was considered reasonable based on conversations with a psychiatrist (S.S.) who mentioned that the effect of type of trauma is not a significant factor in PTSD clinical decision making. Where not quarterly, all original parameter values were converted to the quarterly values as shown in Table 1.
Parameters Used in the Markov Model to Estimate Costs and Quality-Adjusted Life-Years for Canadian Wildfire Evacuees
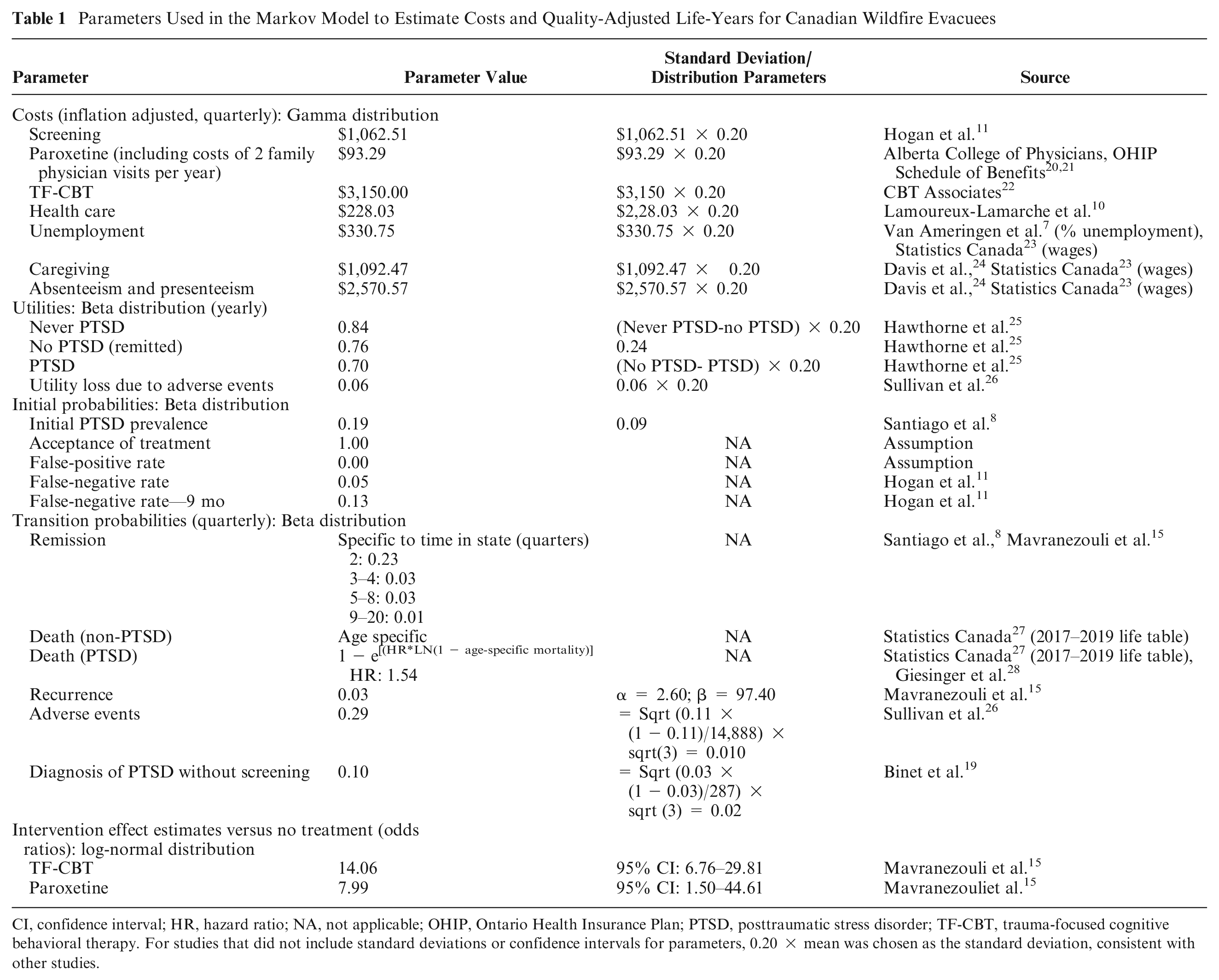
CI, confidence interval; HR, hazard ratio; NA, not applicable; OHIP, Ontario Health Insurance Plan; PTSD, posttraumatic stress disorder; TF-CBT, trauma-focused cognitive behavioral therapy. For studies that did not include standard deviations or confidence intervals for parameters, 0.20 × mean was chosen as the standard deviation, consistent with other studies.
Probabilities
Time-in-state specific probabilities of remission for untreated PTSD were used. From a systematic review of untreated PTSD among patients with nonintentional trauma, the study prevalence at 3 mo is 18.8% and at 6 mo is 14.4%. Therefore, we assumed 23.4% remission ([18.8–14.8]/18.8)) from quarter 1 to 2. 8 After this period, from quarters 3 to 20, we used the time-in-state specific remission probabilities from Mavranezouli et al. 15 (Table 1). We used standard formulas to convert probabilities to rates and then rates to probabilities to estimate quarterly values from annual or monthly values. Given that some time is required to set up a screening program postwildfire and given spontaneous remission of PTSD is common after nonintentional trauma, a prevalence of 18.8% was chosen as the initial prevalence, which is the 3-mo prevalence of PTSD among individuals who have experienced nonintentional trauma and have not yet received intervention. 8
Death rates were age specific and calculated based on published life tables, 27 and the hazard ratio of death due to PTSD was applied to this population to estimate the death rates for individuals with PTSD. 28 Given the prevalence of treatment was 33% at 1 y without a screening program postwildfire among Fort McMurray, Alberta, evacuees in 2016, the diagnosis of PTSD over time, without screening, was assumed to occur at the level found in Fort McMurray. 19 A 1-quarter incidence was calculated from this yearly value, and this value was assumed to be constant over time within the first year and beyond.
Utilities
Given the unavailability of utilities for the Canadian general population for individuals with active and remitted PTSD, we relied on values from the Australian general population from the Australian Survey of Mental Health and Wellbeing study. 25 The utilities for active (i.e., past-year PTSD; n = 533), remitted PTSD (i.e., lifetime PTSD; n = 1,026), and never PTSD (n = 7,280) were derived using the Assessment of Quality of Life (AqoL-4D) instrument, which consists of 4 domains (i.e., independent living, physical senses, psychological well-being, and social relationships). 25 To estimate the utility value from the AqoL-4D questionnaire, a multiattribute utility function was generated from a representative sample of the general population of Victoria, Australia, using the time-tradeoff method. 25 A reduction in utility from adverse events due to paroxetine was estimated using the EuroQol-5D.15,26 Since no adverse effects were expected from the use of TF-CBT (discussed with S.S.), a probability and disutility of adverse effects of 0 were used.
Costs
All costs from a societal perspective were inflated to 2020 values using the Consumer Price Index for health and personal care. 29 The cost of screening was £588 in 2018, 11 which, after adjustment, equated to $1,092.47. These costs included the costs of program start-up, management, screening, and referral management. 11 It was assumed that individuals would receive paroxetine 20 for 3 mo at a dose of 20 mg/d, and during this period they would have 1 visit to a family physician to prescribe and oversee medication (cost: $36.85, K081 remote primary mental health care). 21 The cost of paroxetine for 1 quarter would be $56.44 for a total cost of $93.29 per quarter. 20 Each individual with PTSD received 12, 1.5-h-long sessions of TF-CBT over a period of 3 mo. This is in agreement with Hogan et al. 11 and slightly more than Mavranezouli et al., 15 who included 9 sessions over 12 wk. The unit cost was $175 per hour 22 for a psychologist salary, which results in a total cost of $3,150 per quarter (12 sessions × 1.5 h × $175). Based on discussions with a psychiatrist (S.S.), it was assumed that individuals stopped treatment once they achieved remission, given limited resources to treat PTSD in the community and the high remission rate without treatment. To reduce the impact of this assumption, the base-case assumption was an additional 3 mo of treatment costs accumulated post-remission for individuals receiving paroxetine, which would similarly cost $93.29 (i.e., cost of drug with 1 physician visit). Given TF-CBT is a nonpharmacologic treatment, we assumed no maintenance treatment was required during remission. The total excess health care costs due to PTSD were based on a prior study that included outpatient, emergency department, hospitalization, and medication costs (except antidepressants) among individuals ≥65 y old. 10 The excess health care costs of PTSD were assumed to be the same for adults <65 and ≥65 y old given a lack of data and given prior studies show a large amount of variation across countries. 30 Indirect costs included the cost of unemployment, caregiving, and productivity losses. The health care and indirect costs are excess costs of PTSD compared with no PTSD. The cost of unemployment was calculated based on a prevalence of excess unemployment of 2.7% 7 and median wage for Canadians of $49,000. 31 We calculated caregiving costs and productivity losses per quarter as follows24,31,32:


Intervention Effects
The effects of treatment were modeled through changes in remission rates, which means transitioning from the PTSD state to the no PTSD state. 15 In the case of paroxetine and TF-CBT, the effect of intervention versus no treatment was applied as an odds ratio taken from a network meta-analysis, which made direct comparisons between TF-CBT and SSRIs. 14 We have used the estimates for the effects of treatment for TF-CBT (odds ratio: 14.06) and for SSRI (7.99) from this study, which are for remission at “treatment endpoint” and refer to a 1-quarter time period for receiving the intervention.14,15
Given a small proportion of patients would have a response but not achieve remission, treatment effects would be underestimated; however, it is not clear from the literature what the change in utility would be for those on treatment who do not achieve remission. It was assumed that there is no effect of intervention on the hazard ratio of death for PTSD (discussed with S.S.).
Analysis
Calibration and validation
The calculated prevalence of PTSD over time without screening was compared with previous estimates,5,8 and life expectancy from the model was compared with Statistics Canada life tables. 27
The face validity of the model was discussed with S.S., a psychiatrist who has experience in building cost-effectiveness models.
Base case, sensitivity, and scenario analyses
Model estimates of costs and QALYs were used to calculate the ICUR of both interventions compared with no screening: ICUR = ΔCosts/ΔQALYs. According to Canadian Agency for Drugs and Technologies in Health (i.e., central agency for health technology assessments) guidelines, 33 INMB was calculated using a willingness-to-pay (WTP) threshold (λ) of $50,000, which is frequently used in Canada 34 : INMB=(λ∗ΔQALYs)−ΔCosts and costs and utilities were discounted at a 1.5% rate in the base case. NMB was also calculated using a WTP threshold ( λ ) of $50,000: NMB = (λ∗QALYS) − Costs. We have used the 1.5% discount rate as recommended by Canadian Agency for Drugs and Technologies in Health. 33 However, we have adjusted our sensitivity analysis to vary the discount rate from 0% to 7%. The base-case results are derived from the probabilistic sensitivity analysis.
Deterministic 1-way sensitivity analyses were presented as tornado diagrams highlighting how varying parameter inputs across a range of values influences the results. Most parameters were varied 50% above and below the base-case values. 35 The false-negative rate was varied from 0 to 0.5, while the probability of accepting treatment was varied between 0.5 and 1. The number of months of additional treatment after remission was varied between 0 and 6 mo.
To further examine the impact of uncertainty in model parameters on model conclusions, probabilistic sensitivity analyses were conducted by running the model 10,000 times with model parameters randomly selected from predefined distributions. Beta distributions were used for probabilities and utilities, log-normal distributions for intervention effects, and gamma distributions for costs. Parameters defining these distributions (i.e., alpha, beta, lambda) or the standard deviation were used based on prior studies where available (Table 1), and where not, standard deviations were set to 0.2 times the mean, consistent with other studies. 36 Results from probabilistic sensitivity analyses were presented as incremental cost-effectiveness scatterplots, which present each simulation as 1 point on a Cartesian plane of incremental costs and incremental effects, and as cost-effectiveness acceptability curves, which present the results as the percentage of iterations that are below varying WTP thresholds. Scenario analyses also included calculations of INMB at 2 y from a societal perspective and 5 y without indirect costs (i.e., health care perspective) to compare results to studies that examined screening and treatment among populations exposed to other traumatic events including a hurricane 17 and terrorist attack. 11 All analyses were completed in TreeAge Health Care Pro 2022.
Results
Validation
The calculated prevalence of PTSD over time without screening was in line with previously published estimates.
Base Case (5-y Time Horizon, Societal Perspective)
The results from the base-case (probabilistic) analysis are shown in Table 2, in Figure 2 as incremental cost-effectiveness scatterplots, and in Figure 3 as a cost-effectiveness acceptability curve. Compared with no screening, screening followed by treatment with paroxetine or TF-CBT showed cost-savings and higher benefits (Table 2). Meanwhile, the TF-CBT option provided greater incremental QALYs (0.006) compared with the paroxetine option, and TF-CBT saved more money from a societal perspective; therefore, it was found to be the option most likely to be cost-effective (probability = 0.649) at a WTP threshold of $50,000 per QALY in the cost-effectiveness acceptability curve (i.e., most simulations with highest NMB; Figure 3).
Comparison of the Costs, QALYs, and INMBs across Different Intervention Groups and between Analysis of the Base Case for 5 y (Societal Perspective), 2 y (Societal Perspective), and 5 y (Health Care Perspective), Ranked by Cost
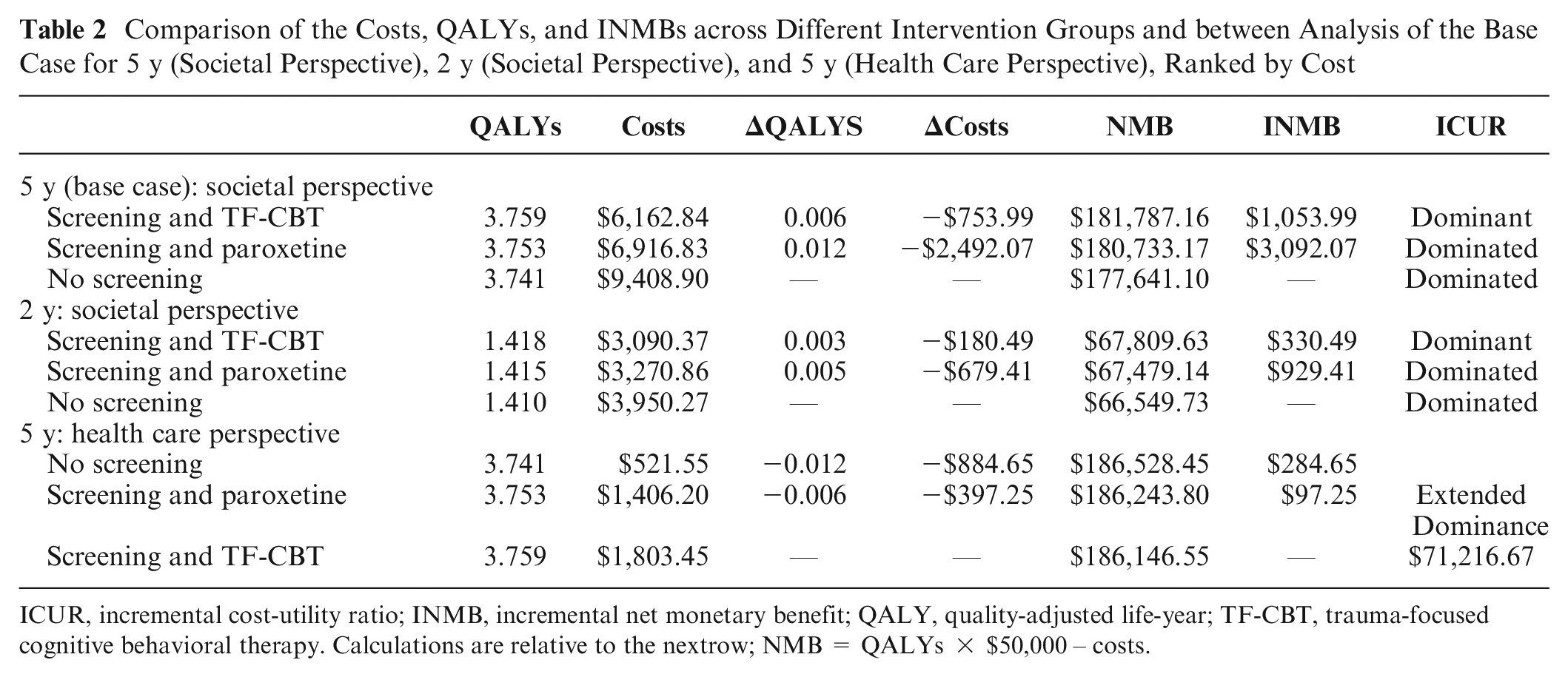
ICUR, incremental cost-utility ratio; INMB, incremental net monetary benefit; QALY, quality-adjusted life-year; TF-CBT, trauma-focused cognitive behavioral therapy. Calculations are relative to the nextrow; NMB = QALYs × $50,000 – costs.

Probabilistic sensitivity analysis from a societal perspective, incremental cost-effectiveness scatterplot, 5-y horizon: (A) screening and trauma-focused cognitive behavioral therapy versus no screening and (B) screening and paroxetine versus no screening.
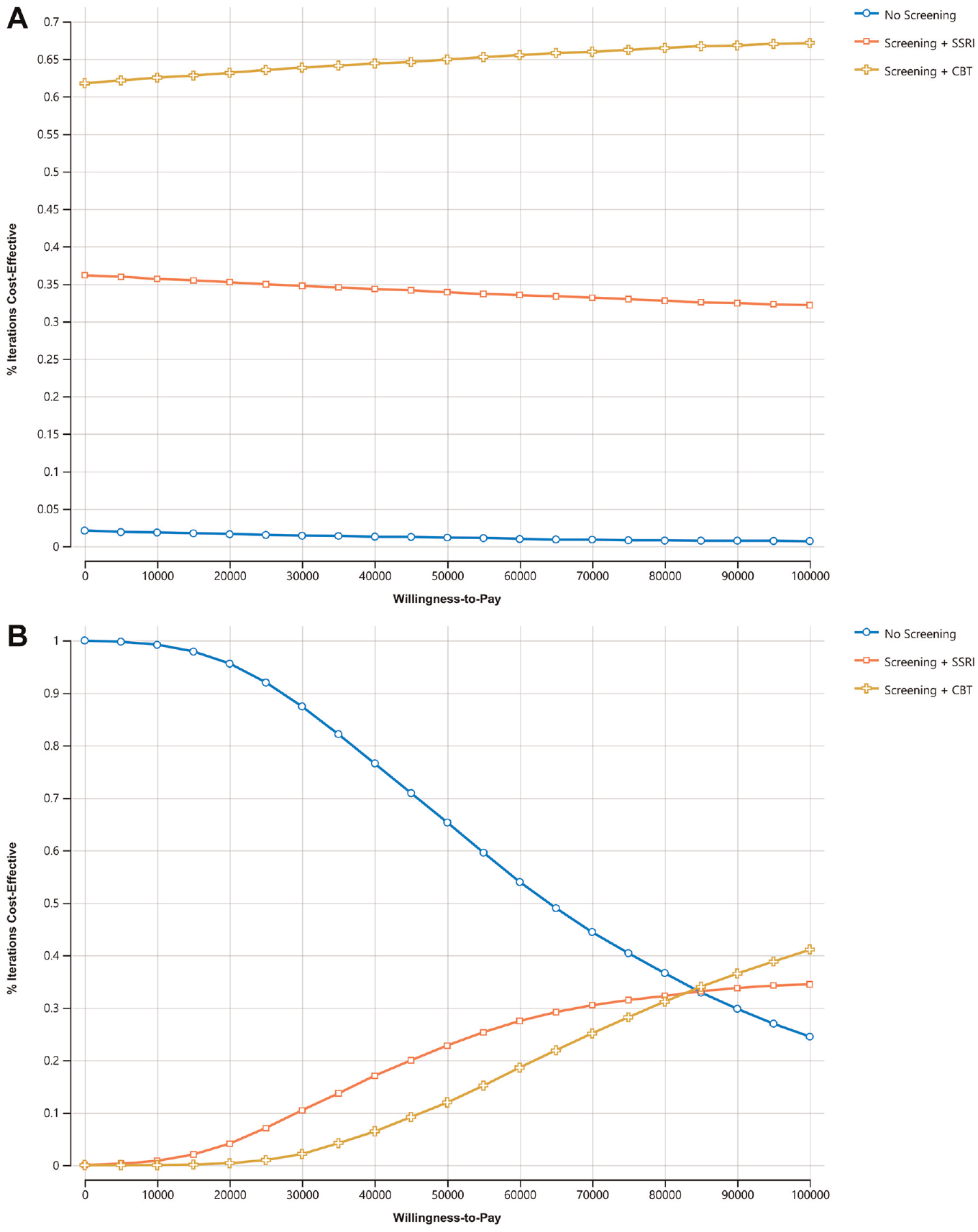
Probabilistic sensitivity analysis, cost-effectiveness acceptability curve, 5-y time horizon. (A) Societal perspective. (B) Health care perspective.
Sensitivity and Scenario Analyses
Scenario analysis with a 2-y time horizon from a societal perspective indicated cost-savings with both strategies (screening with paroxetine or TF-CBT), with savings and NMB being higher for screening followed by treatment with TF-CBT. Screening followed by TF-CBT yielded 0.003 more incremental QALYs compared with screening followed by paroxetine.
Sensitivity analysis (5-y time horizon) from a health care perspective suggested that neither of the strategies are cost-effective at a WTP threshold of $50,000 and no screening had the highest NMB.
Tornado diagrams examined the INMBs rather than ICURs since the ICURs for paroxetine and TF-CBT were negative (Appendix Figure 1A–C). Comparing both paroxetine and TF-CBT treatment to no screening suggested that the parameters with the greatest effects on the INMB were initial prevalence of PTSD (higher = higher INMB), probability of accepting treatment (lower = lower INMB), cost of absenteeism/presenteeism (higher = higher INMB), and treatment effects of paroxetine and TF-CBT (higher = higher INMB). The INMB for both paroxetine and TF-CBT remained positive across all parameters that were varied. Comparing paroxetine to TF-CBT, the parameters that changed the relative ranking between the 2 treatments was the effectiveness of paroxetine, effectiveness of TF-CBT, cost of TF-CBT, and probability of remission over time. Tornado diagrams from a health care perspective (Appendix Figure 2A–C) highlighted that the initial prevalence of PTSD and cost of screening were the most important factors.
Discussion
Key Findings
The cost-effectiveness of screening followed by treatment with paroxetine and screening followed by treatment with TF-CBT treatment were evaluated in comparison with no screening, and to each other, using a Markov model to address the high prevalence of PTSD among wildfire evacuees. Screening followed by treatment with paroxetine and TF-CBT were cost-saving, and both interventions provided additional QALYs, with TF-CBT being the most cost-effective option (Table 2). Deterministic sensitivity analyses highlighted that the initial prevalence of PTSD, initial acceptance of treatment, productivity costs, and treatment effects had the greatest impact on INMB of both treatment arms versus no screening. This suggests that the high indirect costs of PTSD are among the most important drivers of the results. From a health care perspective, neither intervention was cost-effective at a threshold of $50,000 per QALY. Meanwhile, the initial prevalence of PTSD and the cost of screening were the most important factors affecting the INMB from a health care perspective.
Comparison to Prior Studies
Mavranezouli et al. 15 found the same pattern of results as the current study, in which individuals with PTSD treated with TF-CBT versus SSRIs had slightly higher levels of QALYs, higher costs, and consequently lower NMB from the perspectives of the National Health Service and personal social services in England. Similarly, using a health care perspective, Mihalopoulos et al. 16 showed the same pattern of results (slightly higher QALYs gained and higher incremental costs) for TF-CBT than treatment with SSRI. In contrast to both of these studies where all individuals were treated,15,16 we did not find these interventions to be cost-effective relative to no treatment from a health care perspective. This difference is likely due to the fact that all individuals needed to be screened and only a fraction of those individuals are treated. Screening of those who do not subsequently need treatment increases total costs without offering any benefits. This is highlighted by the results showing that the cost of screening and initial prevalence of PTSD were the 2 most important factors in 1-way sensitivity analyses. Thus, if the fraction of screened individuals who required treatment (i.e., were positive for PTSD) was higher or if the cost of screening was lower, then screening followed by treatment (paroxetine) wouldalso be cost-effective under a health care perspective.
Treatment options in prior disaster-related cost-effectiveness studies included screening followed by TF-CBT versus treatment as usual (assessment and identification of PTSD by a general practitioner) after a terrorist attack 11 and stepped care (i.e., TF-CBT) intervention versus usual care (i.e., skills for psychological recovery, a skill-building intervention) in the treatment of PTSD after Hurricane Sandy. 17 Both studies found screening and treatment to be highly cost-effective (terrorist attack: £7,931 per QALY 11 ; hurricane [range]: $3,428.71–$6,857.68 per disability-adjusted life-year avoided 17 ). Paroxetine and TF-CBT were cost-effective and cost-saving estimated over a 2-y and 5-y time horizon from a societal perspective but not cost-effective from a health care perspective. Although the model time horizon was different across studies along with other modeling differences (e.g., allowable state transitions 11 ), it appears the most important factor was the type of treatment (i.e., pharmaceutical or psychological therapy) examined and the associated costs (i.e., 14-fold difference in the cost of treatment). Altogether, the results from our and these other 2 studies11,17 generally suggest that screening programs for PTSD after population-wide traumatic events are cost-effective.
Implications
Given that the main parameters (i.e., prevalence of PTSD, treatment effects) were derived from sytematic reviews and meta-analyses,8,14 utilities were derived from the general population of individuals with PTSD, 25 and the screening and treatment program was the same as that implemented in another developed country (i.e., the United Kingdom), 11 we believe that the main finding that both interventions are cost-saving from a societal perspective is important, and the study findings may be transferable to other contexts with similar health care costs and ability to implement these type of screening programs. This is also supported by 2 other studies examining the cost-effectiveness of screening after other disasters that found similar results.11,17 However, the results from the health care perspective were above the threshold of $50,000 per QALY, which needs to be considered given that the health care sector would bear the costs for this policy’s implementation. It suggests that much of the value of the program lies in reducing indirect costs such as costs of productivity losses and caregiving time. It is important to note that this threshold is not official or consistently applied in Canada, has been in use for many years without adjustment for inflation, and treatments greater than $50,000 are frequently funded 34 (i.e., Canadian Agency for Drugs and Technologies in Health uses 50,000 and 100,000 per QALY thresholds). More research from other countries is needed to evaluate the cost-effectiveness with local costs and WTP thresholds and to determine the feasibility of its implementation.
In addition, costs and other parameters were varied considerably in the sensitivity analysis, which we expect to account for some of these cross-country differences, thereby increasing the generalizability of the results.
Given the growing scale of wildfires, with close to 200,000 Canadian evacuees in 2023 across many towns, cities, and provinces, many of which were rural locations, 4 the requirements on the health care labor force to implement this intervention would be demanding. Given that 18 h of therapy is recommended, with tens of thousands of individuals with PTSD (at a prevalence of 18.8%), the number of hours of required therapy could easily expand beyond the available supply, especially in rural jurisdictions. This would likely require TF-CBT to be provided by a psychotherapist working remotely. In addition, this intervention would likely require tens of thousands of visits to family practitioners to prescribe paroxetine, putting a significant strain on these resources, which may be alleviated if nurse practitioners could be involved in prescribing paroxetine in addition to screening. Therefore, despite the interventions being cost-saving, the initial resource implications need to be considered when designing the final screening program. The eventual screening program may need to include a mix of these 2 interventions to accommodate system resources and patient preferences.
Strengths and Limitations
This is the first study to examine the cost-effectiveness of screening and treating PTSD among wildfire evacuees and one of the few cost-effectiveness analyses focused on PTSD in Canada. The analysis was modeled over a 5-y time horizon using a Markov modeling approach, similar to other studies, such as those on terrorist events (5 y) 11 and hurricanes (2 y) 17 This enabled measurement of the changes in costs and outcomes over the course of this chronic, relapsing condition.
This study is not without limitations. First, the model did not address the existence of comorbidities such as depression, which are common in patients with PTSD and elevated among wildfire evacuees and have the potential to influence costs and HRQoL. Future research is recommended that incorporates depression in the model and screening interventions could consider screening and treatment for both PTSD and depression. Second, due to a lack of wildfire-specific PTSD data, most parameters are from studies with a mix of patients with different types of traumatic exposures. In addition, there were several assumptions made for model parameters due to a lack of data. However, we attempted to address potential biases from assumptions using probabilistic sensitivity analyses and incorporating large variations (±50%) into deterministic sensitivity analyses. Moreover, several assumptions were confirmed with a psychiatrist (S.S.) and were generally made to result in more conservative results. Future research should collect data specific to wildfire evacuees with PTSD. Third, due to data availability, we did not consider discontinuation in the model; however, this is indirectly included given that the effect estimates from the meta-analysis used to inform treatment effects were from studies conducted in an intention-to-treat fashion. Lastly, we did not include opportunity costs of seeking therapy, as it is not commonly reported in the literature.
Conclusions
Screening followed by treatment with paroxetine or TF-CBT for wildfire evacuees results in additional QALYs gained and cost-savings relative to no screening from a societal perspective, but neither intervention was cost-effective from a health care perspective. Both interventions were found to have favorable INMB in most sensitivity analyses conducted. Therefore, screening programs for PTSD should be considered for wildfire evacuees, and individuals diagnosed with PTSD could be prescribed either paroxetine or TF-CBT depending on patient preference, availability of physicians and psychotherapists, and resource constraints.
Supplemental Material
sj-docx-1-mpp-10.1177_23814683241260423 – Supplemental material for Screening and Treatment of Posttraumatic Stress Disorder in Wildfire Evacuees: A Cost-Utility Analysis
Supplemental material, sj-docx-1-mpp-10.1177_23814683241260423 for Screening and Treatment of Posttraumatic Stress Disorder in Wildfire Evacuees: A Cost-Utility Analysis by Michael Lebenbaum and S. Ahmed Hassan in MDM Policy & Practice
Footnotes
Acknowledgements
We would like to thank Dr. Saadia Sediqzadah for reviewing the model and model assumptions and Dr. Ahmed Bayoumi for comments on an earlier draft of the manuscript.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors received no financial support for the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Michael Lebenbaum was supported by postdoctoral fellowship award from the Canadian Social Sciences and Humanities Research Council (SSHRC). The funder played no role in the conceptualization, design, data collection, analysis, decision to publish, or preparation of the manuscript.
Author Contributions
ML/AH, conception, data curation, methodology, formal analysis, writing–original draft; writing–review and editing.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.