
Abstract
Highlights
What is known:
Fecal microbial transplantation (FMT) is the transfer of microbiome from healthy donors to patients.
Fecal donors undergo multiple strict screening tests to exclude any transmissible disease.
Screening tests of potential fecal donors is expensive and time consuming.
FMT is the most efficient treatment for recurrent C difficile infection.
What is new here:
An algorithm to optimize the order of donors’ screening tests in terms of cost was defined.
Optimizing the order tests can save nearly 50% in costs of screening a potential donor.
Fecal microbial transplant (FMT) is a method in which microbiota, isolated from the feces of a healthy donor, is administered into a patient’s gastrointestinal tract. FMT has a success rate of up to 90% for the treatment of recurrent Clostridioides difficile infection1,2 and has been approved by multiple health regulatory authorities worldwide for this indication. The greatest challenge in performing FMT is in its safety, trying to avoid the transfer of pathogenic or opportunistic microbes from the donor to the recipient. Thus, meticulous screening for disease conditions is important. This is a multistage and relatively costly process, involving constant screening of potential stool donors.3,4
The more meticulous the screening process is, the higher the economic burden. Currently, there is no international standardized protocol for donor screening for FMT.5,6 Although there are no official universal guidelines, there are consensus reports aimed to create clear and well-founded instructions regarding stool bank management and donor screening. These reports provide recommendations including topics for the initial questionnaire, detailing what blood and stool tests should be performed.7,8 Thus, there is currently a great deal of similarity between the screening processes of different stool banks.9–11 However, neither the consensus reports nor other articles that describe the screening tests for a stool donor refer to the order of the tests to be performed.
The aim of the current study is to optimize the order of the multistep process of screening and authorizing stool donors in terms of cost and time, based on the cost and probability of failing each screening test.
We hypothesized that through analysis of the screening steps and respective costs, we would be able to reduce the costs and improve the process for stool donor selection. Thus, we tested the process of screening stool donors using a mathematical algorithm that optimizes the order of performing each test and minimizes the effort and costs of screening donors.
Methods
Assumptions for Disqualification Probabilities of Donors
To optimize the timing of laboratory screening, we aggregated lab tests, which can be performed simultaneously from the same sample. We generated 14 groups of lab tests and calculated the cost of each group, based on the Israeli Ministry of Heath pricing list (Table 1).
Groups of Screening Tests, Their Cost, and Probability of Disqualifying a Potential Stool Donor according to the Published Literature and according to Real-Life Data (Research Group)

Ab, antibody; Ag, antigen; ANCA, anti-neutrophil cytoplasmic antibodies; ASCA, anti–Saccharomyces cerevisiae antibodies; CBC, complete blood count; CMV, cytomegalovirus; CRE, carbapenem-resistant enterobacteriaceae; ESBL, extended-spectrum beta-lactamases; F, female; FANA, fluorescent antinuclear antibody; gamma-GT, gamma glutamyl transpeptidase; GOT (AST)-glutamate oxaloacetate transaminase (aspartate aminotransferase); GPT (ALT), pirovate transaminase (alanine aminotransferase); HIV, human immunodeficiency virus; HTLV, human T-lymphotropic virus; LDH, lactate dehydrogenase; M, male; MRSA, Methicillin-resistant Staphylococcus aureus; NAT, nucleic acid test; PCR, polymerase chain reaction; TPHA, Treponema pallidum hemagglutination assay; TSH, thyroid-stimulating hormone; TTG, tissue transglutaminase; VDRL, Venereal Disease Research Laboratory; VRE, vancomycin-resistant enterococcus; WBC, white blood cell.
To estimate the probability of disqualification of donors according to the literature, we relied on published data on potential abnormalities of the lab tests in the apparently healthy general population.12–15 If these data were not available, such as in the case of biochemical tests, we used a previously reported large cohort of healthy Israeli adults, 18 to 60 y old, with a normal body mass index (BMI) and no use of medication, undergoing routine annual checkups at the Tel Aviv Medical Center (TLVMC) between 2000 and 2018. 16 For tests in which the rates of abnormalities in the healthy population were not available, the probability of disqualification was determined based on the experts’ opinion.
Algorithm
The algorithm to optimize (cost minimization) or the optimal order of performing each test is based on the following mathematical theorem:
Given n group of tests,

Proof
The logic behind the algorithm is that, intuitively, a test with a lower cost should be done earlier, and in addition, a test with lower probability of disqualification should be done later to minimize the average cost. Thus, the ratio of the cost to the probability of disqualification may be the best way to order the tests to minimize the average cost. Although, intuitively, this seems quite trivial, the analytic mathematical proof of the algorithm is more complex and is presented in the supplementary methods. Consequently, the optimal algorithm to find the optimal order of performing the tests is by sorting the group of tests by
Assessment of the Algorithm in a Real-Life Cohort
The real-life cohort consisted of potential healthy subjects who volunteered to become fecal donors and were screened at the TLVMC between 2014 and 2019. The eligibility of volunteers for screening was 18 to 50 y of age, BMI of 18.5 to 25 kg/m2, and no apparent illness. Eligible volunteers completed a health questionnaire and underwent an interview and physical examination by a single physician (N.M.). Blood and fecal tests were performed in a standardized multiphase process (Figure 1). All lab tests were performed concurrently in each phase. If the patient failed on a test from phase 1, the expenses on all phase 1 tests were already included, and the patient did not undergo the stool polymerase chain reaction (PCR) tests of phase 2. The current screening process at the TLVMC includes several blood and stool tests, chosen according to the recommendations and guidelines of the Food and Drug Administration and Israeli Ministry of Health regulations. 17 A total of 87 volunteers were screened as potential stool donors at our bacteriotherapy clinic (Figure 2). Thirty-four volunteers were ineligible according to their questionnaire, 13 withdrew due to an inability to complete the donation process, and 6 were disqualified after the interview and physical examination.
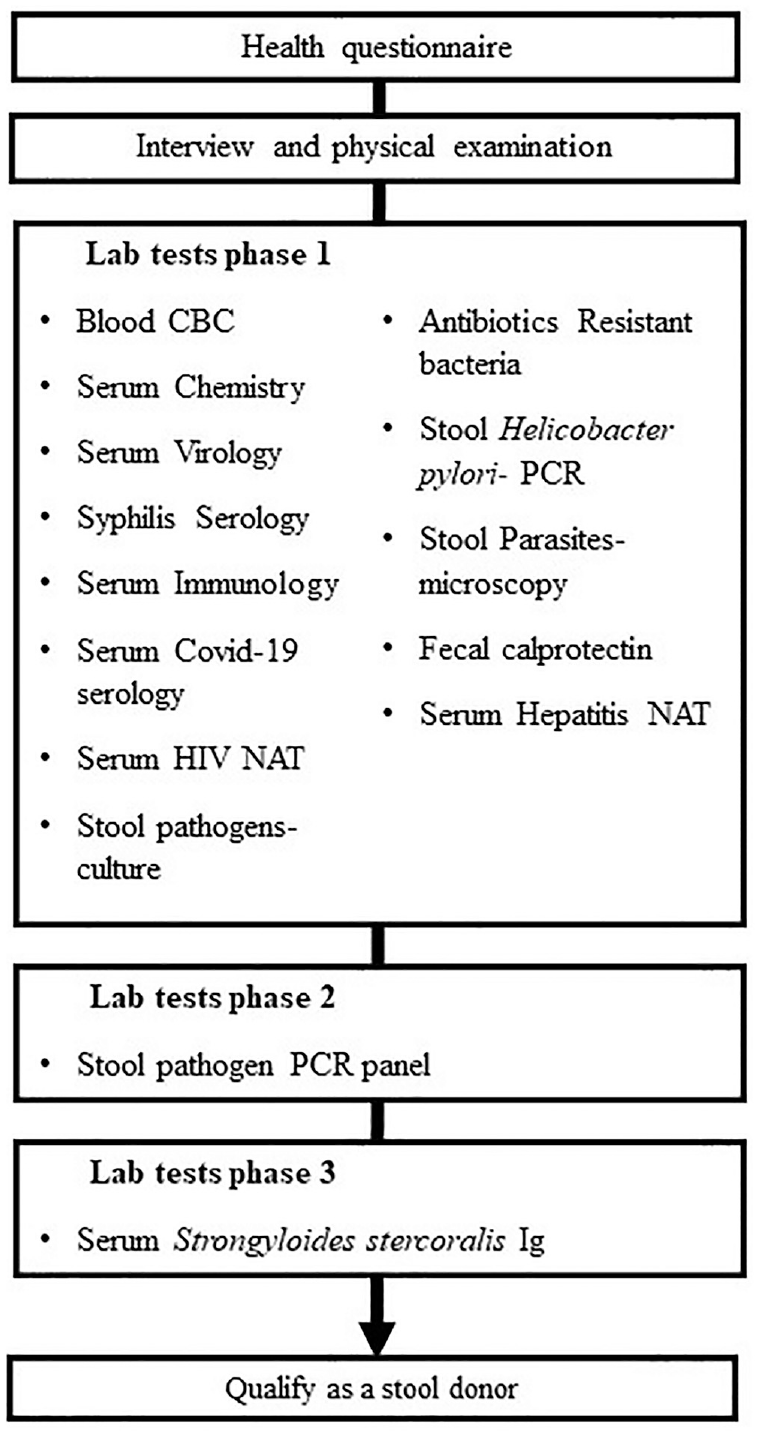
Multiphase process of stool donors screening at the Tel Aviv Medical Center stool bank. Each phase was performed only after the donor was qualified in the former phase.

Flowchart of the study population screened for stool donation.
Time to donor disqualification was defined as the time from the beginning of lab screening until receiving a disqualifying test. At the TLVMC bacteriotherapy clinic, the BioFire PCR was the last exam (besides Strongyloides stercoralis) in the multiphase process, as it was the most expensive test (Figure 1). The time calculations did not take into account the test for S. stercoralis, as it is performed at a central lab, resulting in an inherent delay in screening time. The number of potential donors who had to be screened to find 1 qualified donor was the number of potential donors who started the screening process divided by the number of approved donors.
The average cost for finding a single qualified donor was the sum of money spent on laboratory tests for all potential donors divided by the number of approved donors. All data regarding participants and their screening process were documented retrospectively. This included reason and stage of disqualification, cost of each stage and the tests included therein, as well as the order of the tests and the length of screening (days from screening initiation).
For the real-life cohort, the probability of disqualification of a donor was calculated by dividing the number of disqualified subjects in each lab test by the number of subjects screened. For tests that were normal for all screened volunteers (did not disqualify any potential donor), we assumed the probability to disqualify a donor was 1 divided by (the number of screened volunteers + 1), assuming that the next potential donor is disqualified for that test. Alternatively, if the probability for disqualifying from these tests was available only from the literature, we used the probability described in the literature (Table 1). We calculated the cost of screening each potential donor, even if the candidate failed, and the cost of finding a validated healthy donor in our cohort. It is noteworthy that when a test result disqualifies a potential donor, that donor does not undergo any further tests and is not assumed to pass all tests. The study was approved by the ethics committee of TLVMC. All participants signed an informed consent form as part of the process and allowed use of the collected data for research.
Statistical Analysis
Descriptive statistics were used to describe characteristics of potential stool donors and of the chronologic and financial costs of the donor-screening process. Continuous variables were evaluated for normal distribution using the Kolmogorov-Smirnov test and were reported as means ± standard deviations or medians accordingly. Categorical variables were reported as percentages. The mean cost and time to rejection of a donor and the proportion of each criteria for rejection fulfilled are presented. The analysis was performed using IBM SPSS Statistics for Windows, version 22.0 (IBM Corp., Armonk, NY, USA). For further validation, we also conducted our calculations on the real-life and literature cohorts using Excel (Supplementary Methods 2).
Results
Initially, we examined the probability for disqualifying a potential donor due to an abnormal lab test result, according to the data from the published literature, in each of the 14 test groups (Table 1). Although most of the tests had similar probability for disqualification, several tests, such as GPT and alkaline phosphatase, had different chances for disqualification when comparing the published data with our real-life data.
We then used our algorithm to examine the optimal order of tests for the data from the published literature (Table 2). The average cost for screening a potential donor until disqualification or approval was $132.70 ± $487.40, and the average cost to qualify a single donor was $3,014.40. Thus, there was a potential saving of 94.2% of the cost of screening a potential donor when comparing the optimal algorithm to the worst algorithm.
Optimal Order of Performing the 14 Groups of Tests, with the Probabilities of Disqualification, Based on the Published Literature
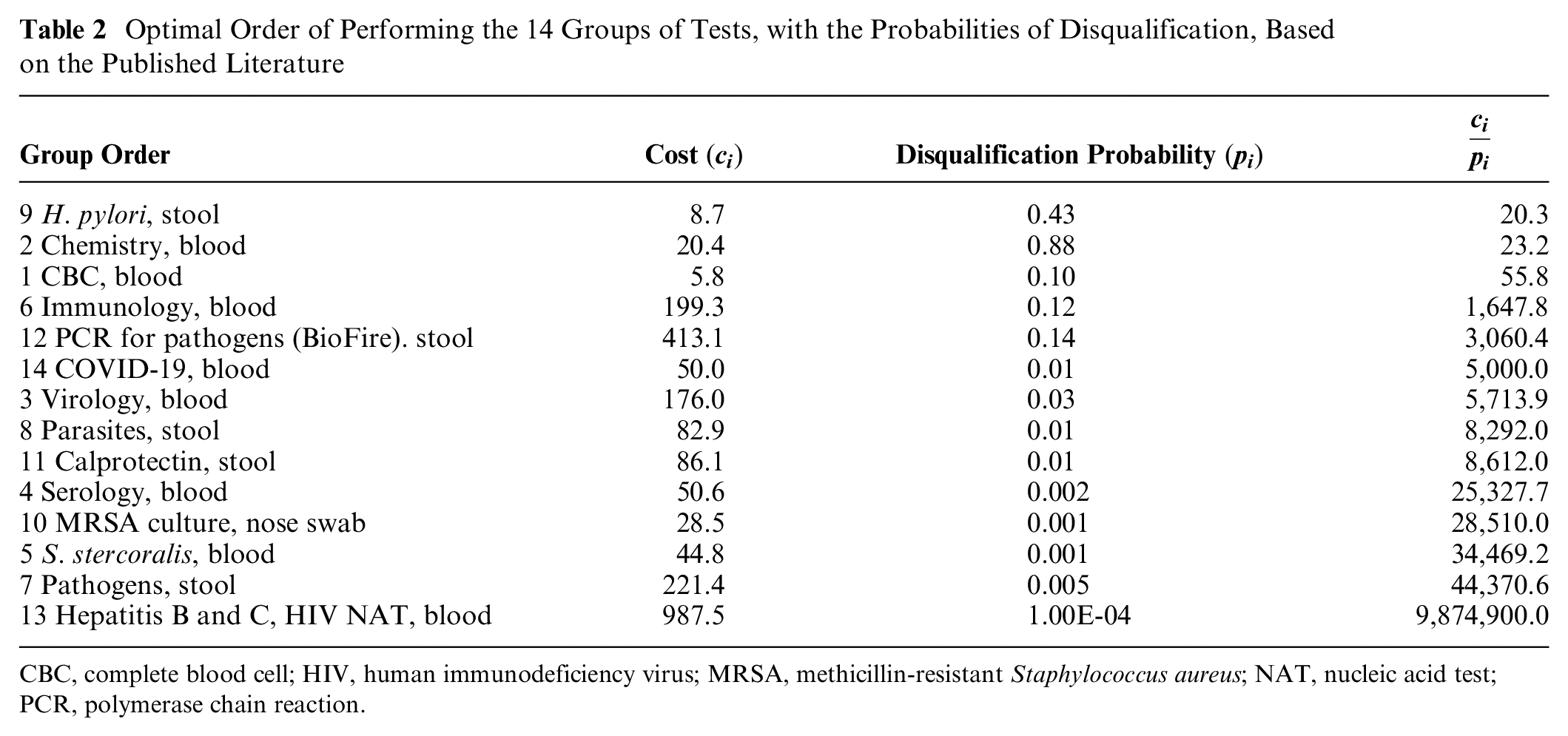
CBC, complete blood cell; HIV, human immunodeficiency virus; MRSA, methicillin-resistant Staphylococcus aureus; NAT, nucleic acid test; PCR, polymerase chain reaction.
To confirm the algorithm, we also examined other screening rules that can be applied. Thus, besides the optimal strategy our algorithm elucidated, we also examined other strategies such as rating the group tests by the probability of disqualification or by their costs (from the higher to the lower or opposite). Supplementary Table 1 summarizes the results of these algorithms and confirms the cost-effectiveness of our algorithm.
Similarly, we used the algorithm on disqualification probabilities on our real-life data (Table 3). Thirty-four potential donors (age 31.0 ± 6.6 y, 59% male, mean BMI: 21.9 ± 1.9 kg/m2), were screened by laboratory tests. Ten volunteers were disqualified due to abnormal lab tests: positive fluorescent antinuclear antibody + anti–Saccharomyces cerevisiae antibodies (n = 3), elevated fecal calprotectin level (n = 3), and detection of a fecal pathogen through pan-PCR testing (n = 4). Finally, 24 potential donors were qualified as stool donors (age 31.2 ± 7.3 y, 50% male, BMI 21.6 ± 1.8 kg/m2). The average time to qualify a stool donor was 38.8 ± 27.9 d, while the average time to disqualify potential volunteers was 27.3 ± 23.8 d. The number of potential donors who were screened (including by questionnaires) to find 1 qualified donor was 3.6. We found that in the real-life data set, the average cost for optimal screening of a potential donor was $1,147.50 ± 1,032.20, and the average cost to qualify a single donor was $2,551.20. Thus, using this algorithm in our real-life setting would have saved potentially nearly 50% in the cost of screening a potential donor.
Optimal Order of Performing the 14 Groups of Tests with the Probabilities of Disqualification, Based on the Real-Life TLVMC Cohort

CBC, complete blood cell; HIV, human immunodeficiency virus; MRSA, methicillin-resistant Staphylococcus aureus; NAT, nucleic acid test; PCR, polymerase chain reaction; TLVMC, Tel Aviv Medical Center.
It is noteworthy that in both the real-life data and literature cohorts, the relatively high standard deviation (variance) in the costs of the optimal order was mainly due to an outlier that is manifested when all tests must be conducted to approve the subject for donation. Importantly, the probability of performing all the tests is not negligible and the cost is relatively high; therefore, the contribution to the variance is high. Although the variance does not affect the proposed order of tests, further clarification of the calculations for mean and variance are included in Supplementary Methods 2.
The disqualification probabilities on our real-life cohort were lower than the disqualification probabilities based on the literature, and thus, the average cost of screening a person was higher, but the average cost to find a suitable donor was lower.
Because several tests, in different groups, are associated in terms of probabilities of disqualification, we ran our algorithm again while taking that assumption into account. For example, the liver tests in group 2 (GOT, GPT, alkaline phosphatase, and gamma-GT) are associated with one another. In many cases, when one is abnormal, other tests of this group are similarly abnormal. Therefore, instead of using the accumulative probability for group 1 and group 2, we estimated a disqualification probability of 0.029 for either group. Under these assumptions, the average cost for optimal screening a potential donor is $1,734.60 ± $800.50, and the average cost to qualify a single donor is $2,534.20. Thus, the potential savings in the cost of screening a potential donor is 24.2%, with 21.3% savings in cost to qualify a single donor. The optimal order of tests is shown in Table 4. In either case, the order of test performance was quite similar and more cost-effective than the original order.
Optimal Order of Performing Stool Donors’ Screening Tests, Assuming an Association of Abnormalities among the Various Subgroup Tests of CBC (Group 1) or of the Tests Included in Chemistry (Group 2) with the Probabilities of Failure Obtained from the Real-Life Data of Rate of Volunteers’ Disqualification
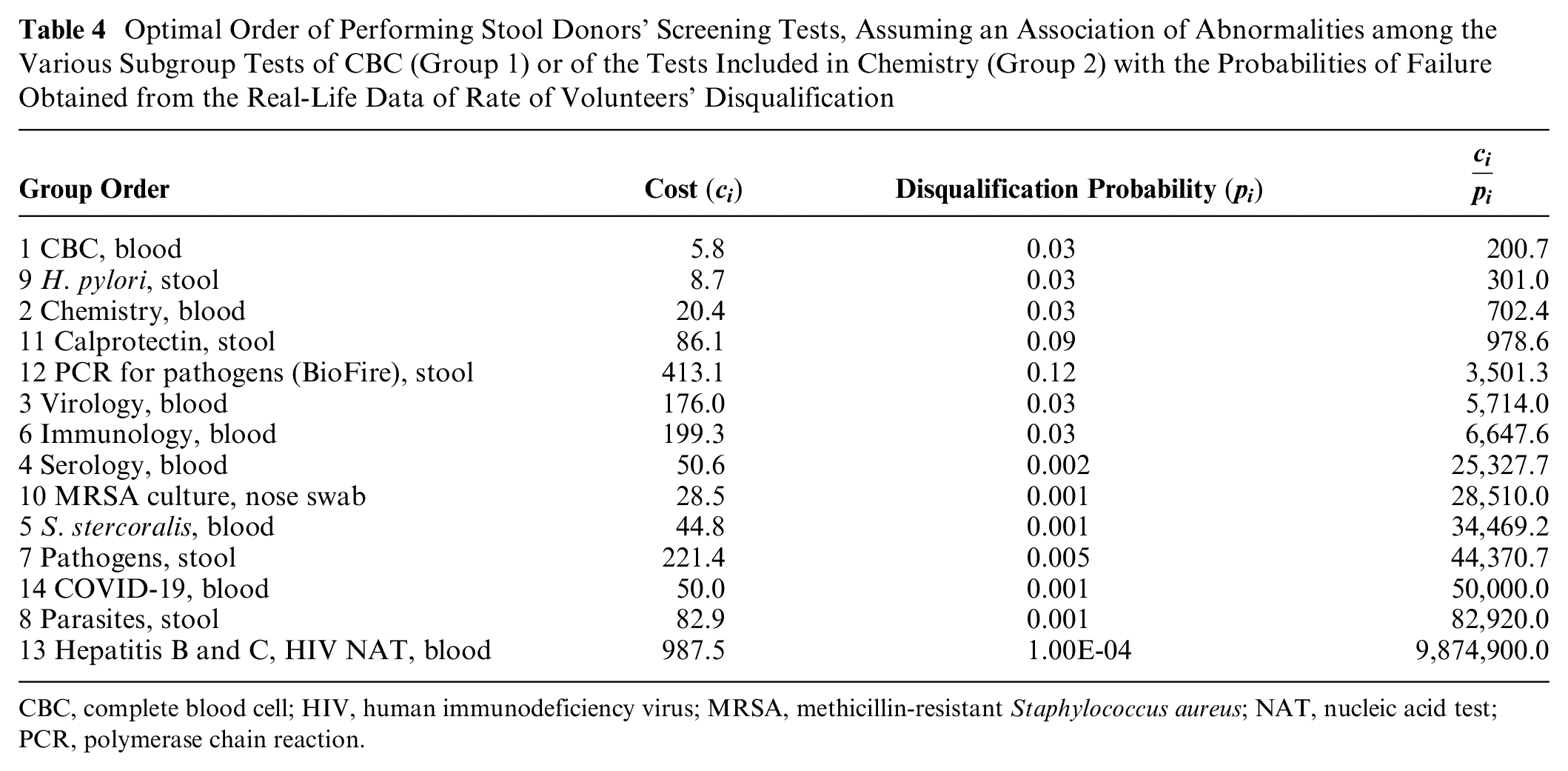
CBC, complete blood cell; HIV, human immunodeficiency virus; MRSA, methicillin-resistant Staphylococcus aureus; NAT, nucleic acid test; PCR, polymerase chain reaction.
Discussion
The screening process of healthy volunteers to allocate healthy stool donors is a multistep and relatively expensive process. During screening, many volunteers are disqualified, adding to the costs of the process. Currently, there is no international standardized protocol that dictates the order of stool donor–screening tests. Thus, performing the tests is quite random, probably leading to a nonefficient process in terms of costs. In the current study, we used a specifically developed algorithm, enabling optimization of the order of lab tests, taking into account the cost of each lab test and its probability of disqualifying the donor.
Using the algorithm for analysis of the data gathered in our center in the past 5 y, combined with the data from the literature, revealed a more beneficial order of tests. Thus, the cost for screening a potential stool donor can be decreased by up to 50%, and the cost to qualify a single donor can be decreased by about 21%.
Previous reports provide guidance on general recommendations for screening of donors and review the economic impact of FMT-related costs.18,19 However, there is no reference to the order of the tests to be performed. For example, blood and stool tests performed at the Netherlands Donor Feces Bank (NDFB) differ slightly from the tests performed at the TLVMC, and the order of the screening tests is different as well: NDFB starts with a stool test before the blood test, whereas the TLVMC starts with the serum screenings.6,7,9
After optimization, the first 3 test groups in both the real-life and literature cohorts were 1, 2, and 9, but the order of these groups was altered. Furthermore, the last test group to be performed in both analyses was group 13 (hepatitis B and C and HIV NAT). The differences between the optimized orders generated from our data and the published data might be related to the small sample size in our research group or due to a prior selection bias in this group due to the primary screening with a health questionnaire and physical examination.
We further tried to optimize the order of tests by assuming that several tests can be clustered, as they are biologically associated and thus have similar chances to fail a lab test (Table 4). Interestingly, both analyses resulted in a similar order of tests, differing only in the order of the first 3 lab test groups. Thus, the analysis should start with groups 2, 1, and 9—chemistry, CBC, and Helicobacter pylori. Indeed, these 3 group tests are among the cheapest of the screening tests with a high probability of being positive. Our study also includes COVID-19 serology tests, as there was a continued need for FMT treatments during the COVID-19 pandemic. 20 Since SARS-CoV-2 has become endemic, prevention measures can be implemented in existing protocols without increasing the burden for donors or increasing the costs of tests.
It is noteworthy that the change in the order of the tests, according to the optimized order, does not increase the number of times potential donors are required to come to the clinic, as serum and stool samples are stored for future tests.
The optimal order of the screening tests is relevant to other stool banks, which use similar disqualification terms to us. Indeed, in an Italian study, of 36 candidates who reached the lab tests phase, 7 were disqualified. All 7 volunteers were disqualified due to a positive result for fecal pathogens in a 1-step reverse transcription PCR assay test. 10 In our study, 10 of the 34 volunteers who reached the lab tests phase were disqualified. Of these 10, 4 potential donors were disqualified due to detection of a fecal pathogen through pan-PCR testing, whereas the others were disqualified for other reasons. The optimal order of tests we presented in Tables 2 and 3 is based on the disqualification data that were gathered in our study, applied to our algorithm. However, since in both papers several potential donors were disqualified for the same reason—the PCR test—our optimal order of tests may help optimize the Italian screening process as well.
The main limitation of this study is the relatively small sample group in the research. To address this limitation, we used an additional published large cohort that examined the probabilities of test failures in an apparently healthy population. 17 However, it is also limited, given that our potential stool donors undergo an additional screening stage by a health questionnaire and a physical examination. It is noteworthy that our findings and recommendations for the order of the screening tests are based on Israeli test prices and local disqualification etiologies, which may not be compatible with those of other stool banks.
To our knowledge, this is the first study to offer a recommendation for an optimal order of the screening tests to evaluate a potential stool donor and minimize screening costs and make the procedure more efficient. The unique algorithm that was designed especially for this research enabled the determination of the optimized order of tests that will make stool donor screening a more cost-effective process.
Supplemental Material
sj-docx-1-mpp-10.1177_23814683241254809 – Supplemental material for Economic and Chronologic Optimization of Fecal Donors Screening Process
Supplemental material, sj-docx-1-mpp-10.1177_23814683241254809 for Economic and Chronologic Optimization of Fecal Donors Screening Process by Bar Levy, Naomi Fliss Isakov, Tomer Ziv-Baran, Moshe Leshno, Nitsan Maharshak and Lael Werner in MDM Policy & Practice
Supplemental Material
sj-xlsx-2-mpp-10.1177_23814683241254809 – Supplemental material for Economic and Chronologic Optimization of Fecal Donors Screening Process
Supplemental material, sj-xlsx-2-mpp-10.1177_23814683241254809 for Economic and Chronologic Optimization of Fecal Donors Screening Process by Bar Levy, Naomi Fliss Isakov, Tomer Ziv-Baran, Moshe Leshno, Nitsan Maharshak and Lael Werner in MDM Policy & Practice
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.