
Abstract
Highlights
This is the first study in Canada to assess the decisional needs of older adults receiving care at home and to identify their most common difficult decisions.
Difficult decisions most frequently made were about housing and safety. The most significant decisional conflict was experienced by people making decisions about palliative care.
When their quality-of-life score was low, older adults experienced clinically significant decision conflict.
This is a visual representation of the abstract.
Keywords
Background
The proportion of older adults in almost every country in the world is growing, and Canada is no exception 1 Living longer has multiple age-related consequences, 2 and due to declining health and autonomy, many older adults need additional care but wish to receive it at home,3,4 especially since the COVID-19 epidemic, which has caused more deaths in residential care than anywhere else. 5
In Canada, home care services are a range of services provided in the home by trained staff, including nurses, physiotherapists, occupational therapists, nutritionists, social workers and personal support workers. 6 Home care is not covered by the Canada Health Act, which ensures federal funding transfers to provinces and territories for health care, funds that are administered by Canada’s provinces and territories according to their own priorities. Thus, home care across Canada varies widely in scope of services, eligibility requirements, and funding arrangements (i.e., public/private, not-for-profit/for profit). 7
Older adults have complex health care needs and face many health-related decisions, some more difficult than others. 8 A difficult decision is a situation in which there is a priori no evident best option among the choices. Older adults may also be overwhelmed or insecure about their ability to make decisions.
Decisional needs are defined as “deficits that can adversely affect the quality of a decision and require tailored decision support.” 9 When decisional needs are unmet, uncertainty and distress escalate, decision quality is reduced, and decision regret may follow. 10 These hamper effective decision making and timely follow through. Manifestations of decisional needs are lack of knowledge, unrealistic expectations, unclear values, inadequate support, complexity of decisions (including difficult decision types), personal and clinical needs, and, foremost of all, decisional conflict. 9 Decisional conflict is defined as ambiguity or oscillation between options, causing stress and difficulty in deciding. 11 Decisional conflict can be measured to identify factors associated with a person’s most difficult decisions and to indicate other decisional needs.
An effective approach to reducing decisional conflict and meeting other decisional needs is shared decision making (SDM),12–17 a collaborative process whereby health care teams support clients in making decisions informed by best evidence and by what matters most to them.18–20 Key to patient-centered care,21–23 SDM also respects patients through asking them about their goals and the role they desire to play in the decision-making process.24–27 Although SDM has been promoted by several provincial governments,28–31 it is still not widely practiced by health care professionals in Canada. Little is known about the extent to which SDM has been adopted specifically with older adults in home care, and indeed, troubling evidence shows that older Canadians receiving home care services have the least experience of SDM. 32
While SDM is challenging with older adults, and their complex care needs,27,33–37 it has been shown to improve their decision-making experiences.36,38 During the SDM process, decision aids or coaching can be used to improve decision quality by addressing unresolved decisional needs.39,40 To prepare the way for these SDM tools and custom design them to this population, a detailed portrait of their most difficult decisions and the variables that affect them is needed. However, no decisional needs assessment has yet been published regarding older adults or those receiving home care services specifically. 39
Consequently, to provide SDM tailored to the context of older adults receiving home care services, we sought to assess the decisional needs of this population in Canada, including identifying the most difficult decisions they faced, and to measure clinically significant decisional conflict (CSDC) and factors associated with it.
Methods
Study Design
We conducted a cross-sectional survey across the 10 Canadian provinces and used the Checklist for Reporting Results of Internet E-Surveys to guide reporting of results. 41 This project is embedded in a 7y Canadian Institutes for Health Research–funded research program whose overarching goal is ensuring that more older Canadians and caregivers in home care become fully engaged as partners in their care. 42
Study Participants and Recruitment
Eligible participants were Canadians aged 65 y or older from the 10 provinces (excluding the territories) who were receiving home care services or had received such services in the past year and who were enrolled in Leger Marketing’s pan-Canadian Web panel of a total of 400,000 individuals. Leger uses traditional and mobile telephone methodologies to recruit participants using the Leger call center (61%), partner programs (25%), recommendations from other panel members (5%), registration on the panel website and social media (5%), and offline recruitment (4%). Panelists fill out a detailed profiling questionnaire at registration to decrease multiple entries and fraudulent panelists. A quality control of the panel is also carried out continuously. Each time panelists complete a new survey, their answers to the sociodemographic questions are re-recorded and their profile is renewed. Thus, the panelists, already profiled by demographics, occupation, and chronic conditions, could be directly recruited based on our eligibility criteria. A nonprobability sampling method was used to invite 29,628 panelist adults aged 65 or older to participate. Using the Leger random sampling software, the sample was balanced across age, sex, and region. A query was then entered into the panel software based on the screening criteria to locate all eligible respondents, who were asked how old they were, whether they had received home care services during the last 12 mo, and to indicate if possible the exact date. Participants were not aware that they would be asked about decision-making needs or related issues before signing consent, which appeared after the eligibility filter questions.
Data Collection
To our knowledge, no other study has reported on decisional needs for this population and context. We were inspired by the populational decisional needs assessment by O’Connor et al. 43 and by another decisional needs assessment in focus groups by Légaré et al. 44 Because of the lack of a standardized questionnaire, we developed our own using the Ottawa Decision Support Framework (a guide to the development of interventions to prepare patients and health care professionals for SDM), 9 the Decisional Needs Assessment in Populations Workbook (which includes outlines for establishing questions to assess decisional needs), 45 and the informed decision model, which refines the understanding of the decision node in SDM. 46 The questions were designed in February 2020 (before the COVID-19 outbreak reached Canada).
The survey first asked questions about the sociodemographic characteristics, including household size, and to indicate which of 15 potential decisions made in the home care setting in the past year the participant found the most difficult. In phase 1 of this research program, interviews with older adults and caregivers in a Canadian home and community care organization identified difficult decisions they had made. 47 We triangulated these results with decisions found in other published studies with older adults and caregivers48–50 as well as with expert opinion (Table 1) to arrive at the 15 difficult decisions presented to our participants. If participants were unable to find 1 in the 15 that matched their personal experience, they were invited to add a new difficult decision in their own words. For the identified difficult decision, we measured decisional conflict using the validated 16-item Decisional Conflict Scale (DCS) with responses on a 5-point Likert-type scale. 51 We also measured components of their decision-making process using the validated 5-item Control Preferences Scale, 52 the validated 5-item Decision Regret Scale (DRS), 53 and the Kemp Quality of Life Scale. 54
In total, the survey asked 25 questions including 3 open (age, options considered, and decision made) and 8 semi-open questions (decision points, ethnicity, first language learned, people involved in decision making, information desired for future decisions, preferred format of information, information sources considered reliable, and professional home-care help received). The full questionnaire in both French and English was pilot tested for navigability and comprehensibility by a random sample of 30 eligible panelists before data collection. Questionnaire completion time was about 20 min.
Leger Marketing created a Web-based closed survey for our questionnaire. A unique URL link to the survey was emailed to participants. This allowed respondents who had interrupted the completion of the questionnaire to pick up again where they had stopped. Participants completed the survey in English or French. Respondents logged in using their panel member account, which allowed only 1 questionnaire validation per member to avoid duplicate entries. Questions appeared in the same order for all participants. Participants had to answer all questions on 1 page to move to the next and clicked on the Finish button on the last page to submit their responses. The survey was voluntary; as is Leger’s practice, $1.60 was offered to participants for completing the survey.
Sample Size and Data Analysis
Our sample size was informed by previous work, 26 a cross-sectional study with a quantitative approach supplemented by a qualitative data arm reporting on older adults’ and caregivers’ experiences of housing decisions. We extracted the proportion of older adults who had CSDC associated with a housing decision at the threshold of 37.5 for sample size calculation. The computed sample size a priori was 460 participants, which ensured at least 80% power for the study. A nonprobability sample of this size would guarantee that if we estimated at least 26% of respondents would have CSDC at the threshold of 37.5, the 95% confidence interval would be ±4% or narrower. First, after discussion, we chose to organize43,55 the 15 difficult decisions into 3 categories for statistical analysis with CSDC: 1) decisions about housing and safety, which were grouped together because housing decisions are often provoked by safety concerns, such as falls, and are not necessarily medical decisions 56 ; 2) decisions about management of health conditions; and 3) decisions about end-of-life care. To ease interpretation of decisional conflict scores, following the user manual, we calculated the average value of DCS items, subtracted 1, and multiplied it by 25 to standardize the total score from 0 (low decisional conflict) to 100 (high decisional conflict). 51 We defined older adults with CSDC as those with DCS scores greater than 37.5, 57 a threshold associated with delayed decision making and uncertainty about following through with the decision. 58 We also converted decision regret scores by reverse-coding statements 2 and 4 of the DRS and subtracting 1 from each item, as mentioned in the DRS manual. We then multiplied the sum by 25 and divided it by 5 to obtain a score out of 100.
To identify the category of decisions for which the CSDC was most frequent, we calculated the proportion of respondents with DCS scores greater than 37.5 in each decision category in relation to the total for that decision category.
Third, we performed descriptive, bivariable analysis and multivariable analysis of CSDC for 46 independent variables (Supplemental material) using generalized linear models regression to determine factors associated with CSDC. To achieve the underlying assumption of multivariable analyses, the variables were checked for linearity and multicollinearity. We found no multicollinearity problem, and the linearity assumption was not violated. The 18 variables with P values of <0.20 in the bivariate analysis were eligible for exploratory multivariable analysis. For the latter, we used the stepwise selection method to examine models with different combinations of variables that otherwise might be overlooked. The entry and exit significance levels were 0.15 and 0.20, respectively. An entry significance level of 0.15 indicated that a variable must have a P value <0.15 to enter the model during stepwise selection. An exit significance level of 0.20 indicated that a variable must have a P value >0.20 to leave the model during stepwise selection. 59 The regression modeling included only participants with complete data on all potential factors. A “preferred not to answer” response to sociodemographic questions was considered as missing data. Selection of the final model was based on the Bayesian information criterion. We also performed a sensitivity analysis at the 25/100 threshold for the CSDC, as scores below this cutoff are associated in the literature with implementing decisions. 51 Statistical analyses were performed using SAS 9.4 (SAS Institute Inc.).
Ethics Approval
Ethics approval was obtained from the Research Ethics Board of the Integrated University Health and Social Services Center of the Capitale-Nationale, Quebec, Canada. Respondents gave their consent to participate in the study after being informed in a language that they understood of the drawbacks and risks of the project, the voluntary nature of their participation, that their data would be used only for scientific purposes and treated in complete confidentiality. The data are stored on secure servers.
Results
Participants
Of 29,628 panelists invited to participate, 14,102 visited the first page of the survey (47.6%), about 30% more than the usual response rate for Leger panel members, showing a high interest in the topic. A total of 2458 panelists were disqualified because they were 64 on the date of the survey and not yet 65. Among the 699 who were eligible (4.96%), 239 withdrew and 460 completed the survey and were considered for our analysis (Figure 1). The average age of participants was 72.5 y, and 50.3% were female. Table 1 shows the detailed characteristics of the participants. The prevalence of about 5% of panelists who were receiving home care services is a ratio similar to that observed in a previous study with Leger panelists (8%) 32 and in the Canadian population as a whole (4%). 60 Professional support services received by participants were mostly for medical treatments (37.6%), for home maintenance (31.1%), and for food preparation (25.7%).
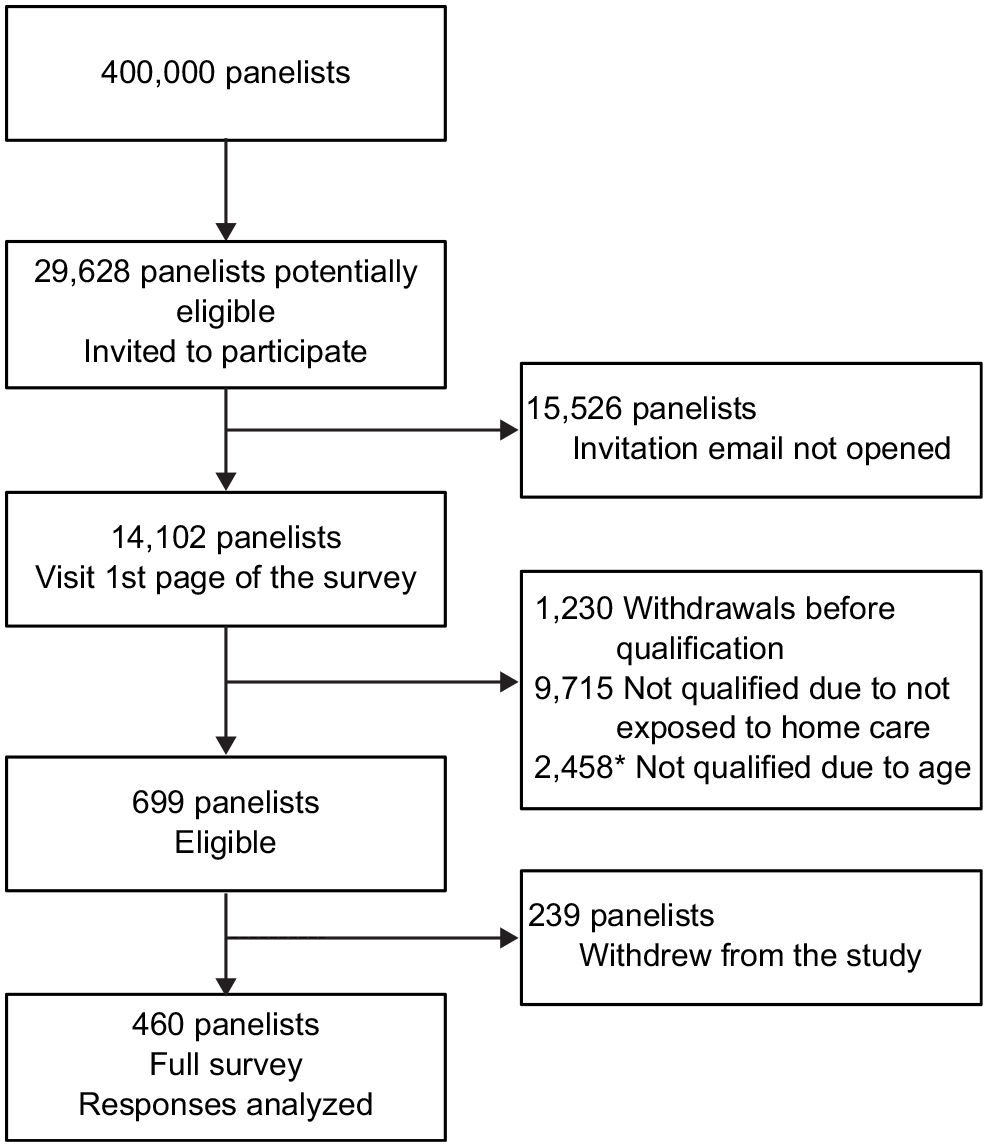
Flow chart of participant recruitment.
Characteristics of the participants (N = 460)

Numbers may not total 460 in all cases because of approximations; the sum of the approximations may result in a difference of +1 or −1 in the total.
Canadian dollars.
Of the 239 participants who withdrew, 73.7% were from Ontario and Quebec, and the mean age was 73.4 y. The sociodemographic characteristics of the 81 withdrawn participants who provided them were similar to the characteristics of participants who completed the survey, except that 45.5% were female and 66.2% had English as their first language.
Data collection was performed from March 13 to 29, 2020. The World Health Organization declared COVID-19 a pandemic on March 11, and lockdown in Canada occurred on March 19. One-third of the included participants completed the survey before this date, and we observed no changes over the period of data collection, suggesting that COVID-19 had little impact on our results.
Types of Difficult Decisions
Participants’ decisional needs cover multiple aspects and difficult decisions were about housing and safety (53.5%), managing health conditions (24.4%), and end-of-life care (8%; Tables 2 and 3). Under the housing and safety category, decisions points related to home safety, moving, and fall prevention were most frequently reported (Table 3). Other than with their care team, participants reported they had made these decisions with a spouse (43.5%), alone (27%), or with their children (25.5%).
Respondent Descriptions (N = 460)
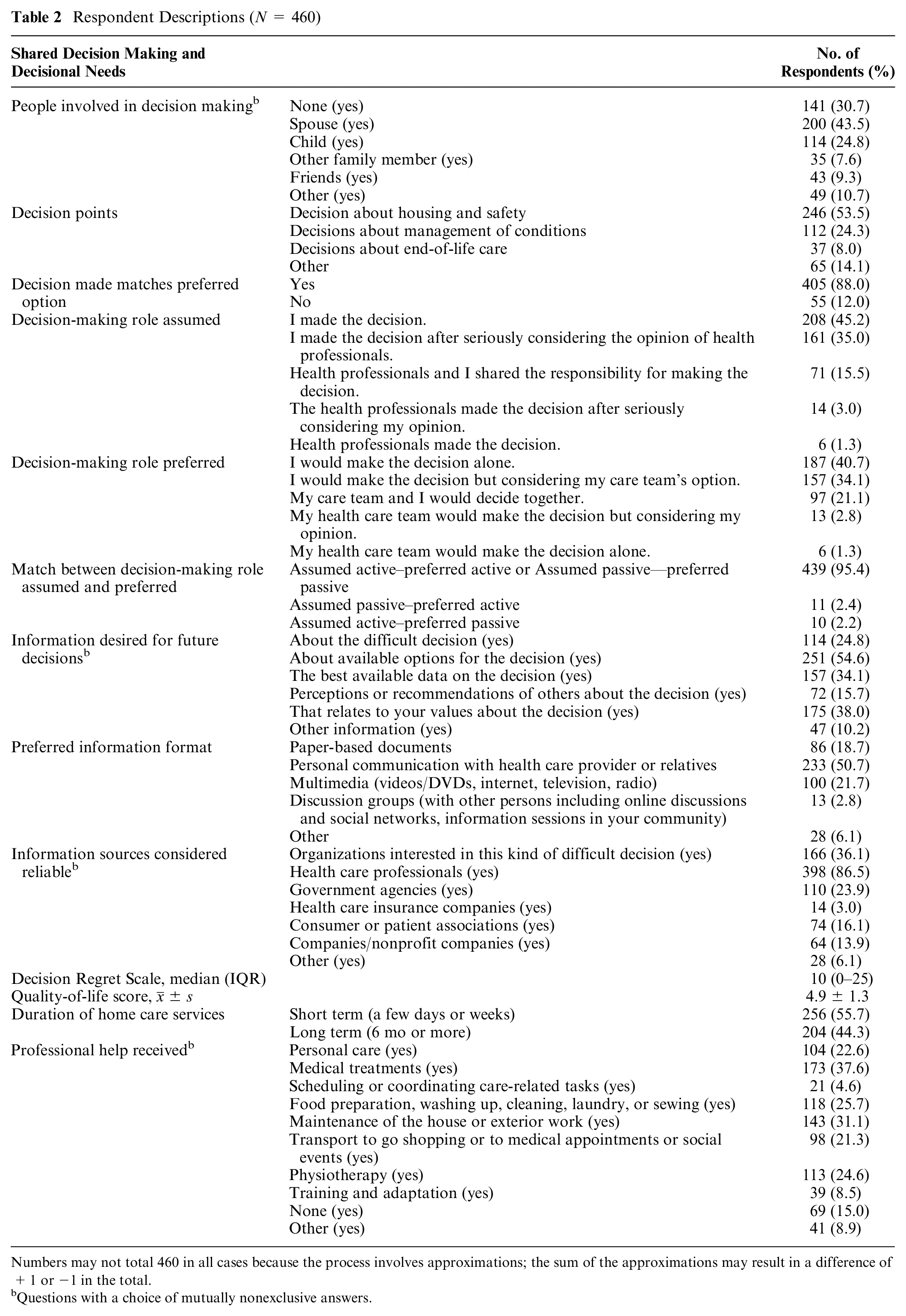
Numbers may not total 460 in all cases because the process involves approximations; the sum of the approximations may result in a difference of +1 or −1 in the total.
Questions with a choice of mutually nonexclusive answers.
Descriptive Statistics of Decision Points (N = 460)

We calculated the percentages of clinically significant decisional conflict for each decision. The respective denominators correspond to the number of total participants for each decision.
CSDC and Its Associated Factors
Overall, 14.6% of respondents had experienced CSDC (DCS above the threshold of 37.5) when faced with their difficult decision (Table 4). In the house and safety category, the most difficult decision was whether to ask for help at home or not, whereas in the health care decisions, the most difficult decision was about pain management, and in the end-of-life decisions, the most difficult decision was about palliative care. CSDC was most frequent among those who chose end-of-life decisions; that is, of the total 460 respondents, 37 (8%) chose end-of-life decisions as the most difficult, and 6 of those 37 (16.2%) had DCS scores above the 37.5 threshold (Table 3). The final list of factors associated with CSDC included household size = 1 person (odds ratio [OR] [95% confidence interval {CI}]: (1.81 [0.99, 3.33]; P = 0.27), household size = 3 persons (2.66 [0.78, 8.98]; P = 0.83), and household size = ≥4 persons (6.91 [2.23, 21.39]; P = 0.014); preferred option not matching the decision made (4.05 [2.05, 7.97]; P < 0.001); passive role in decision making (5.13 [1.78, 14.77]; P = 0.002); and poor quality of life (0.70 [0.57, 0.87]; P < 0.001; Table 5).
Descriptive Statistics According to Decision Categories (N = 460)

Percentages of CSDC were calculated for each decision category. The respective denominators correspond to the number of participants for each decision category. CSDC, clinically significant decisional conflict; DCS, Decisional Conflict Scale.
Factors Associated with CSDC, DCS >37.5 of 100 (n = 420)

CI, confidence interval; CSDC, clinically significant decisional conflict; DCS, Decisional Conflict Scale; OR, odds ratio.
The mean score for decision regret was 13.77 (s = 15.54), and its association with decisional conflict was statistically significant (Spearman correlation coefficient = 0.56; P= 0.0001).
Discussion
This decisional needs assessment of older adults receiving home care informed us about their most difficult decisions, why they were difficult, and the level of CDSC associated with the decisions. Housing and safety decisions were the most frequently mentioned, while end-of-life decisions elicited the highest level of decisional conflict. CSDC was experienced by 14.6% of participants. Household size, preferred option not matching the decision made, passive role in decision making, and poor quality of life were the factors associated with CSDC. Our results lead us to make the following observations.
First, the frequency of decisions related to home safety, moving decisions, and fall prevention is congruent with the evidence that prompted the Canadian Home Care Association’s initiative “Am I Safe” to help people in home care reduce the likelihood of falls.61,62 A systematic review found that the experience of falls and feelings of insecurity or fear were among the factors influencing housing decisions among frail older adults. 56 Our results highlight that health decisions faced by older adults in home care in Canada are far broader than medical decisions and include decisions about where to live and staying safe at home. In addition, by the end of the data collection period for our study, COVID-19 outbreaks were starting in nursing homes in Canada.63,64 Early in the pandemic, 2 patient decision aids were developed in Canada to support the decision of whether or not to move older adults out of retirement or nursing homes. They were downloaded more than 10,000 times in 2 wk.64–66 This high number of downloads together with our survey results stresses an urgent need for decision support felt by older adults in Canada for their decisions about home and safety.43,67 It also suggests that well-supported decision making about home and safety could have reduced the harm experienced in long-term residential care. 68
Second, almost 1 in 10 of our participants experienced CSDC. These older adults may delay decisions or feel unsure about following through. 57 They may also experience more decision regret and ultimately dissatisfaction with and loss of trust in the health care system in general.10,51,53 Notably, older adults who identified end-of-life care decisions as the most difficult also showed the highest prevalence of CSDC. These results are particularly important in the context of the COVID-19 pandemic, where end-of-life decisions were often left to the last minute and made without support from caregivers. This is a key area to prioritize for decision support interventions targeting older adults receiving home services.
Third, we identified a number of factors associated with CSDC, some of which have been identified before. Taking into account that the category of reference was 2, we observed that the more the household size increases, the more CSDC increases and becomes significant at 4 people or more in the home (4 or more compared to a household of 2). The larger the family, the more opinions there are about what option to choose. The older adult must take them into account and evaluate the decision’s impact on each person. They may be handling more sources of pressure and have more difficulty playing the role they desire in the decision process. Indeed, they may not have control over the final decision 69 : our results show that when the decision made was not the preferred option, the odds of CSDC were 4 times higher than when they matched. In this case, the mismatch may not be due to lack of SDM; perhaps the decision was made by others or was made when certain options were no longer available. Whatever the reason, a mismatch is a clear signal of CSDC. Furthermore, the CSDC was 5 times higher when the older adult took a passive role in decision making. Indeed, the literature supports that playing (or preferring) an active role improves the decision-making process.26,43,70 In addition, our study showed that, as supported by the literature, older adults with a higher quality of life were protected to some extent from experiencing CSDC.15,71,72
Limitations and Strengths
Some of our results are based on decisions made as much as a year ago, which may have caused information bias (recall bias) leading to overestimation or underestimation of the measure of association. Second, our sample may not be representative of all older Canadians receiving home care services, such as those with no internet connection or computer skills, who could not participate in the survey. Also, as study participants were self-selected as home care recipients, it is possible that at least some of them did not actually receive home care. Third, some demographic categories (ethnicity, first language, province, information format) were grouped together, which could result in data loss. This may have been exacerbated by the snowball sampling used to build the panel. The survey likely excluded many Indigenous people, cultural groups, and those without English or French. However, to the best of our knowledge, this is the largest population and Web-based survey in the world to date on decisional needs of older adults receiving home care services. 39 Finally, this survey took place during a COVID-19 lockdown in Canada and may thus reflect decisional needs of older adults in the home care sector under exceptional circumstances. However, perhaps this context has served to better highlight their preexisting and future needs.73,74
Conclusion
In our sample, the older adults receiving home care services in all 10 provinces of Canada had unmet decisional needs and a significant proportion experienced CSDC. The most frequently identified type of difficult decision was about housing and safety but the greatest prevalence of CDCS concerned end-of-life decisions. CDCS can be detected and reduced through decision support interventions and patient involvement in decision making. Our results will help develop strategies for implementing SDM among older adults receiving home care services in Canada, such as decision support tools that address their most difficult decisions, that is, “opt for medical assistance to die or not” or “whether to move or not” and factors that increase their risk of CSDC.
Supplemental Material
sj-docx-2-mpp-10.1177_23814683221124090 – Supplemental material for Difficult Decisions for Older Canadians Receiving Home Care, and Why They Are So Difficult: A Web-Based Decisional Needs Assessment
Supplemental material, sj-docx-2-mpp-10.1177_23814683221124090 for Difficult Decisions for Older Canadians Receiving Home Care, and Why They Are So Difficult: A Web-Based Decisional Needs Assessment by Alfred Kodjo Toi, Ali Ben Charif, Claudia Lai, Gérard Ngueta, Karine V. Plourde, Dawn Stacey and France Légaré in MDM Policy & Practice
Supplemental Material
sj-pdf-1-mpp-10.1177_23814683221124090 – Supplemental material for Difficult Decisions for Older Canadians Receiving Home Care, and Why They Are So Difficult: A Web-Based Decisional Needs Assessment
Supplemental material, sj-pdf-1-mpp-10.1177_23814683221124090 for Difficult Decisions for Older Canadians Receiving Home Care, and Why They Are So Difficult: A Web-Based Decisional Needs Assessment by Alfred Kodjo Toi, Ali Ben Charif, Claudia Lai, Gérard Ngueta, Karine V. Plourde, Dawn Stacey and France Légaré in MDM Policy & Practice
Footnotes
Acknowledgements
We thank our caregivers advisors Emmanuelle Aubin, Ron Beleno, Carolyn Candfiel, and Kathy Kastner. We thank Louisa Blair for editorial assistance with manuscript preparation. We also thank the Université Laval Statistics Consulting Services, Imane Benasseur, Codjo Djignéfa Djade, and Ghizlane Messaoudi for their help with data analysis.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided entirely by a Foundation Grant (FDN-159937) from the Canadian Institutes of Health Research (CIHR). The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report. FL holds a Tier 1 Canada Research Chair in Shared Decision Making and Knowledge Translation. ABC is funded by the Fonds de recherché du Québec-Santé (FRQ-S). The funders are not involved in the project
Author Contributions
AKT, KVP, and FL contributed to the conception and design of the study. KVP and FL coordinated data collection in collaboration with Leger Marketing. AKT, GN, ABC, CL, and FL contributed to the data analysis. AKT drafted the manuscript overseen by ABC, CL, DS, and FL. All authors revised the manuscript critically for important intellectual content, gave final approval of the version to be published, and agreed to be accountable for all aspects of the study.
Authors’ Note
This work was presented as a poster at the the Research Day of the Population Health and Optimal Health Practices of the CHU de Québec Research Centre, June 4, 2021, and at the 49th NAPCRG Annual Meeting, June 24, 2021.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.