
Abstract
The Fontan is a complex surgical procedure used as a palliative treatment for children with univentricular hearts. In the past, the mortality rate was high and the associated comorbidities as a result of the Fontan circulation were many. However, as research into the condition developed, better understanding has led to a massive reduction in early mortality and a rapidly increasing population of such patients surviving well into adulthood. This has led to a large surge in patients with congenital heart disease being referred for cardiac transplant assessment. According to research, listing these patients at the optimal time is the key to improving transplant outcomes. However, determining that optimal time is unclear and controversial. In this article, I address this issue by developing an optimal timing rule that accounts for the factors faced by specialist cardiologists in determining when transplant ought to be considered for this cohort of patients.
Introduction
The Fontan is a surgical procedure that was initially developed in 1971 as a palliative treatment for children born with a heart with only one ventricle. 1 The technicalities of the procedure are complex, and it was initially associated with very high mortality rates and significant postoperative complications. However, as research into the procedure, and the associated condition of the patient with acquired Fontan circulation progressed, mortality rates have declined, and in the majority of cases, patients grow and develop in a near-normal way and live with a good quality of life. 2 Coats and colleagues 3 have reported a “5-fold increase in Fontan patients, with a projected 60% increase over the next decade,” while Khairy and colleagues 4 and Gamba and colleagues 5 report that Fontan surgery survival exceeds 80% at 20 years postsurgery. However, they also point out that eventual failure of the Fontan physiology is inevitable prompting referral of the patient for assessment for heart transplantation. Indeed, over the past 15 years, there has been a 40% increase in transplantation of adults who were born with a heart condition (Congenital Heart Disease [CHD]), * and while the current proportion of transplants performed for Fontan failure is unclear, it is predicted that these patients will account for 70% to 80% of CHD transplantation in the future.2,6
However, according to Crossland and colleagues, 7 “The Fontan group has significant comorbidity with limited options for medical therapy8–11 and optimal timing for listing and transplanting these patients is therefore key to improving outcomes.” The point about optimal timing is also mentioned in Kenny et al., 2 who say that “determining the optimal timing for transplant in these patients remains unclear” and suggest that having an understanding of this “can help guide decision making in regards to listing.” Currently, the decision about the optimal time to list is based on the specialist clinicians’ experienced judgement, but there is no objective benchmark guiding this decision. “The timing of transplant in the late failing Fontan remains highly controversial and an area of developing expertise.” 2 Indeed, according to Polyviou and colleagues, 12 there is a need for tools that help guide them in the difficult decision-making around listing this high-risk group for transplantation.
In this article, I develop a decision rule that clinicians can use to determine the optimal time to list individual patients with a Fontan physiology for heart transplantation. Clinical judgement based on experience is extremely important in the decision to list and should not be discounted, but having such a rule will be an additional tool that can assist them in devising the optimal management strategy for patients with a failing Fontan. The main benefits of the rule I derive are that it is easy to apply and serves as an objective benchmark. The reason this research is so worthwhile is that in those patients with Fontan failure who do survive a transplant, long-term survival is comparable with other diagnoses, 7 and according to Burch and colleagues, 13 long-term “cardiac transplant (survival) for adult CHD is better than cardiac transplant for all other causes.” However, to get to this stage, Fontan patients must be listed and subsequently transplanted at the right time.
This rule must account for a number of factors. On the one hand, transplantation carries huge risk for a Fontan patient owing to multiple prior surgeries, immunological sensitivities, and multi-organ involvement. 2 According to Karamlou and colleagues, 14 “Patients with CHD wait longer on the list than non-CHD patients and carry a higher waiting list mortality.” These considerations, combined with the unrelenting progression of physiological failure should prompt early consideration of transplantation in apparently stable patients2,15 before they become too unwell and their risk of death posttransplant (if they get that far) is too high.
On the other hand, listing patients too early is not ideal. Even for apparently stable patients, the surgery is high risk. Posttransplant, the patient is on immunosuppression therapy for the rest of their lives, which places them at high risk of serious infection. Indeed, this is only one of a number of such considerations outlined in Kenny et al. 2
In terms of the model, the doctor has the choice to list the patient at time t or to wait until some future time. In making this decision, three features are very important: 1) irreversibility in the sense that once the patient is transplanted, this cannot be reversed * ; 2) flexibility—if the doctor decides not to list the patient at time t, she may do so in the future so that it is not a now or never decision; and 3) uncertainty—the outcome from performing the transplant is always uncertain ex ante. Thus, the doctor’s choice about whether or not to list a patient is a real option; that is, she has the option to list the patient now or she can “watchfully wait,” which preserves the option to list in the future. The important point about real options is that waiting has value owing to the uncertainty of the outcome and the irreversible nature of the decision. The idea is that deferring a decision may allow for more information to be revealed that may be valuable for the decision to list; for example, it may prevent a patient from being put through a very risky procedure in a suboptimal clinical state; or equivalently, the acquisition of more information may justify the decision to transplant in the future. “With deferred treatment, the passing of time offers a medical history and therefore increases information upon which a clinical decision can be made.” 16 In essence, the intention is to make a confident decision based on as much information as possible and the option to defer is valuable because it allows doctors to observe the progression on the Fontan failure as well as to gain more information about the patient’s clinical status. However, there is a cost to deciding to defer if the progression of the failing state is rapid and the optimal listing window is missed. The clinical status of the patient may deteriorate during the waiting period which may adversely affect the expected outcome. The value of waiting must be derived, via a method known as dynamic programming, by comparing these expected costs against the expected benefit from deferring.
According to Driffield and Smith, 16 immediate treatment versus watchful waiting has been assessed in other contexts. They give some examples of glue ear, small abdominal aortic aneurysms, among others. However, they also point out that these studies do not model deferral properly because they fail to incorporate the fact that should the clinical status of the patient begin to deteriorate significantly, the option to list can be exercised at any time and patient can be immediately listed. The model in this article overcomes this limitation because it accounts for flexibility over timing in the sense that there are no stipulations over when the patient can be listed. One example of such a stipulation could be that listing can only happen immediately or not at all.
The model is one of sequential sampling because it allows for a multiperiod perspective and will enable me to incorporate all of the dimensions just discussed. A similar approach has been applied previously in the context of health technology adoption. 17 The approach has also been applied in a wide range of other contexts to problems in, for example, corporate finance, 18 market microstructure, 19 migration, 20 and the environment. 21 The idea is that the cardiologist has a checklist of symptoms (which she determines) against which the clinical status of an individual patient is checked. These, along with the quality of the symptoms, that is, how good they are at predicting posttransplant outcome, enable the clinician to determine a patient-specific level that can be measured against two threshold values that are analytically derived in this article. If the patient’s level is above the upper threshold, the patient is deemed too well for transplant and will be reassessed in due course. If the level is below the lower threshold, the patient will be considered too unwell for transplant. However, if the level is between the two thresholds, the patient should be listed. During the listing period, while the patient waits for transplant, the patient will be routinely reviewed and his level will be redetermined accordingly. If the patient’s clinical status declines to the point of his level dropping below the lower threshold, he should be removed from the list.
The model accounts for the rate of clinical decline, that is, the number of comorbidities developed over a predetermined period. If, for example, that period is 6 months, then a patient who is reviewed after 1 year and has developed 2 comorbidities in that year has rate of decline of 1 comorbidity per 6-month interval. In other words, depending on the length of time between reviews, the number of comorbidities developed will be adjusted to a number per predetermined level; that is, it will be adjusted to a rate. This ensures consistency across patients who are reviewed at different intervals.
In principle, if their health subsequently improves, the patient will be reviewed and the decision rule reapplied. If the clinical status is such that he is well enough to be listed again, he can be relisted. However, owing to the nature of the disease progression of a failing Fontan, this is unlikely to happen in practice very often. Moreover, it is worth pointing out that, for cardiac transplantation in the United Kingdom, at least, it is not the practice for a patient to be listed if the clinician knows that if the patient were to be offered an organ, they would not be able to accept it. Indeed, if a listed patient develops an infection, they will be removed from the list, even for just a few days, and relisted once the infection clears.
The policy structure just described represents what happens in practical settings. Specialist cardiologists list patients they deem to be ill enough, but not too ill. As discussed above, if a listed patient becomes too ill, they are removed from the list. The analytic aim of this article is to determine points to delineate the boundaries of these regions.
I show that the longer the patient is expected to wait on the list before getting an organ, the shorter is his life expectancy if he does not have the transplant, and the faster his rate of clinical decline, the earlier he should be listed, that is, while he is still reasonably well. These results are plausible and intuitive and suggestive of the model’s usefulness in practice.
This article represents the first stage of a broader research agenda to determine a decision criteria with regard to optimal timing that specialist cardiologists can use in clinical practice. I demonstrate in this article the theoretical model underpinning the rule and examine it hypothetically. However, to make it fit for practice, the model needs to be incorporated in a simple software program that calculates the optimal decision once clinicians input the various parameter values pertaining to a specific patient. Moreover, some input parameters will require empirical estimation from past data, which is discussed in a later section and, finally, there are some limitations to the current model that are discussed in the Conclusion. The model should be adapted so that there are future versions of it that account for these limitations and the software program updated accordingly.
I also wish to point out that the practical tool is intended for use by cardiologists at specialist centers in which there is the expertise and risk appetite for transplanting patients with Fontan physiology. While there are a number of centers in the United Kingdom, for example, that perform cardiac transplants, only the Freeman Hospital in Newcastle upon Tyne performs transplants on patients with Fontan physiology. As such, it is the clinicians at that center that make the decision about listing such patients. Finally, it is worth pointing out that the model here is derived with the listing of Fontan patients for heart transplantation in mind. However, the techniques used are not specific to this issue and could be applied, in principle, to any decision about when to treat a patient in a vast array of clinical settings.
The rest of the article is organized as follows. In the second section, the description of the model is outlined. In the third section, the decision criteria are derived and are explained via the use of an example in the fourth section. In the fifth section, I discuss the model in terms of its plausibility for clinical use and also how the input parameters required can be estimated empirically. The sixth section concludes with a discussion of some of some of the limitations of the current model that ought to be incorporated into future versions of the model.
The Model Outline
At some time t, the doctor considers whether or not to list a patient for cardiac transplant. Note that t represents the time of any assessment that may come after or include the initial assessment, where
Prior to transplant and, therefore, prior to listing, there is uncertainty over the outcome of the transplant for that patient. At the time of the first assessment, before any tests on the patient have been conducted, the doctor has a prior belief of
Tests are conducted and the results of the tests serve as signals that are indicative of the patient’s posttransplant outcome and, thus, help alleviate some of the doctor’s uncertainty. There is a standard checklist for all patients undergoing such assessment against which their comorbidities are checked. This checklist accounts for the factors suggested by Kenny and colleagues, 2 which must be considered (e.g., multi-organ involvement, immunological sensitivities, and number of prior surgeries). Hereafter, I use the terms signals, comorbidities, and symptoms synonymously. For example, Patient i has the symptoms checked Yes in Table 1, and the existence (or not) of each symptom is deemed to be indicative of a Good or Bad outcome.
Example of Symptom Checklist
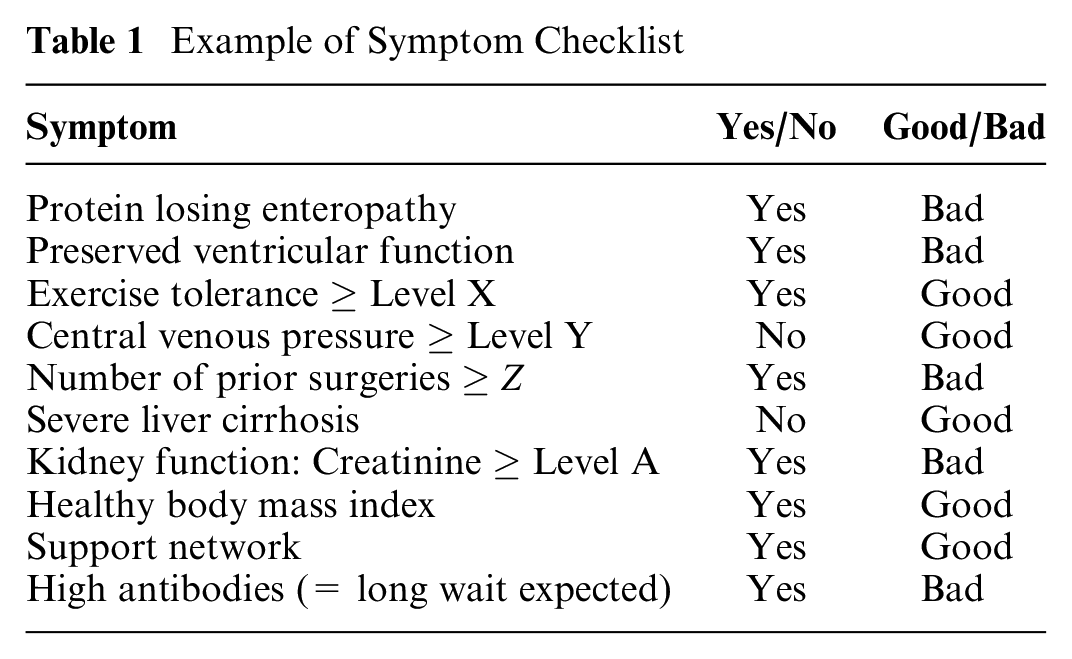
In this example, the number of signals indicative of a Good outcome (i.e., five symptoms) is exactly equal to the number of signals indicative of a Bad outcome. However, it is the quality of the signals that matter. Signals are deemed to be of high quality if they are a correct reflection of the true outcome. For example, if the acquisition of protein losing enteropathy (PLE) is indicative of a Bad posttransplant outcome, and the outcome of a high percentage of patients with PLE turns out to be Bad, then PLE is a high quality signal. In the model, however, the quality parameter, which is denoted by
Another important point about the comorbidities is that some are, naturally, more important than others. This is easily accounted for by considering a specific comorbidity in terms of its associated comorbidities. Take PLE for example. This comorbidity could be considered in terms of, for example, 1) level of albumin
For each patient, the number of signals, as well as their quality, will determine, at the time of assessment
With regard to the decision bounds, let
Patients can develop a new comorbidity at any time, and if they do, the doctor’s belief in a Good outcome is revised accordingly. For a patient that is listed, if their clinical status declines such that the belief
The decision bounds will account for a number of other factors. For example, the expected waiting time on the list is one such factor. If the patient is listed at time
The cost, in terms of life expectancy, of being listed is the patient’s current life expectancy without the transplant (defined earlier as
Another such factor is the rate of clinical decline of the patient. The patient’s development of further comorbidities is random. I let the the number of comorbidities they develop in, say, a 1-year horizon be denoted by
An important assumption underpinning the decision criteria is that the doctor making the decision is risk-neutral. The motivation for this is that the decision tool derived in this article provides an objective benchmark for all such specialist clinicians to use which does not take into account individual doctors’ appetite for risk. This ensures that by adhering to the rule, the decision by the doctor to list a patient is based solely on the factual information she has available about the patient’s clinical status and is not influenced by her subjective preferences. Hence, two patients with little clinical difference but with different doctors may receive opposing management strategies if the doctors do not adhere to such an objective criteria because, as long as this is the case, the doctor’s own appetite for risk would be a driving force underpinning the patient’s treatment. The discount rate used by the doctor is denoted by
This section outlined in detail the input parameters to the model that the doctors will use in determining the best decision with respect to an individual patient. The technical analysis will follow in the next section. However, for the reader’s convenience, I provide a comprehensive table in the online appendix that summarizes the discussion in this section.
Derivation of the Decision Criteria
In determining the optimal management strategy, the doctor chooses the strategy that maximizes the life expectancy of the patient. In this section, I derive the decision bounds
Suppose that at some point in time, the belief in a Good outcome is given by
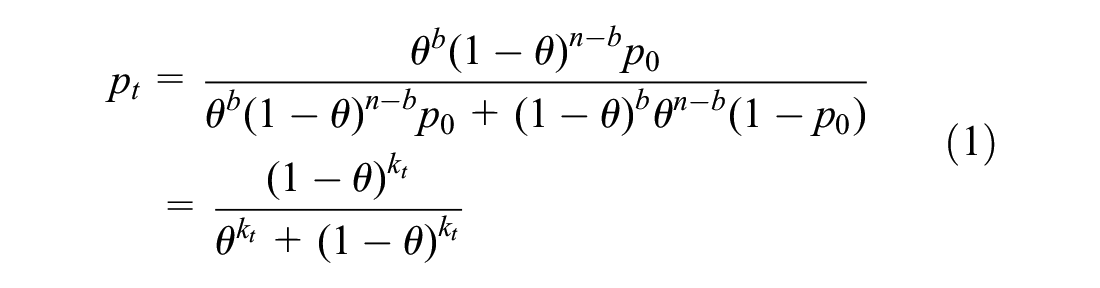
where
However, once a patient is listed, it is because they have acquired enough comorbidities relative to the upper threshold. When this is true, the acquisition of any further comorbidities implies they are progressively worsening to the point where they may be too ill. Hence, in the listing region, the acquisition of a comorbidity is indicative of a Bad posttransplant outcome. To account for this,
I rewrite

such that
In the section “Derivation of
Derivation of
To derive
His expected total life expectancy (TLE) from being listed now with an expected waiting time of

where
It is given by

subject to the condition that as

where

and

Note that this corresponds with Equation (11) from Thijssen and colleagues,
22
but with their
To determine

and

which yield

where

This belief is well-defined for
Derivation of
To derive
The value of the option to remove the patient from the list is derived in a similar way to that in Region 2. However, I assume that only negative signals arrive in this region; that is, once
This gives

subject to the condition that
A general solution, subject to this condition is given by

where

(cf. Equatios 7 and 8 in Thijssen et al.,
22
but recall that we do not consider positive signals so that their
It is easily verified from Equation (14) that
Therefore, the total value of being listed in Region 4 is given by the combined value from his expected life expectancy from being listed plus the value of the option to delist. Note that the expected life expectancy from being listed is given by Equation (3).


and the total Region 5 value is given by

This is underpinned by the same intuition as that for Equation (15). However, the difference is that in Region 4, the acquisition of one more comorbidity does not result in removal from the list, whereas it does in Region 5. As such, the value of the options to delist differs in these regions.

To determine

and

Replacing for

This threshold is a probability level. Thus, to be well-defined, it must be that
Listing Criterion
The listing criterion can be given in terms of

where

and

with
The optimal timing decision rule is given by
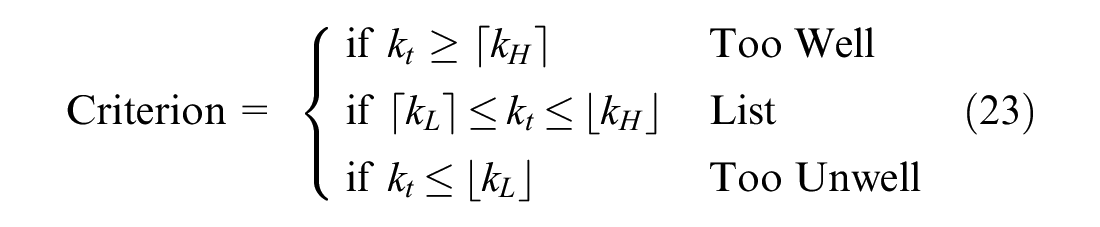
Note that working out
Discussion
In this section, I demonstrate that the implications obtained from the theoretical model indicate its plausibility for clinical use, and second, I discuss how the input parameters that are required could be estimated.
First, however, I make the following important point about the quality parameter

The effect of
As such, the model’s predicted effects of the parameters
The Scientific Registry of Transplant Recipients (SRTR) maintains 43 risk-adjustment models for assessing transplant program performance in the United States.
23
A feature of these models is the importance of certain comorbidities in predicting transplant outcome (analogous to the signal quality in this model). Snyder and colleagues
23
assess the performance of the SRTR models and find that, in general, posttransplant outcomes are difficult to predict. The C-statistics determining the models’ ability to distinguish between high- and low-risk transplants are wide-ranging and can be low. For the heart models, the C-statistics range between 0.67 and 0.83. Nevertheless, it is reasonable to assume that if the clinician has, based on their own experience and from the literature, chosen to include certain comorbidities in the checklist, they must be good predictors of the posttransplant outcome. Hence, I think it is appropriate to interpret the effects of the above-mentioned parameters for
Model Implications
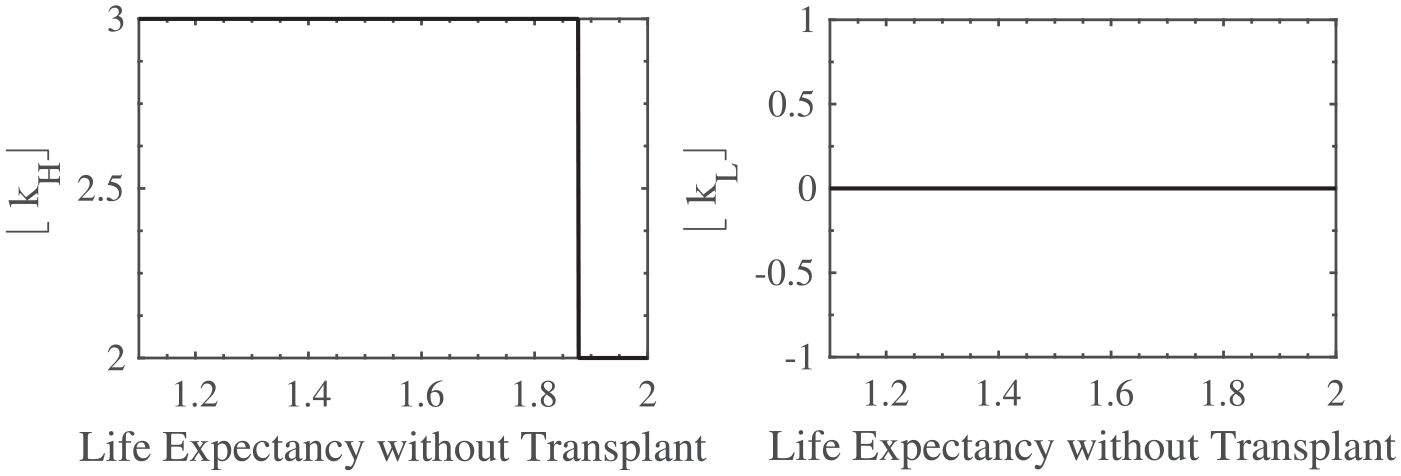
In Figures 2, 3, and 4, I show the impact, according to the model, of the expected waiting time, the patient’s life expectancy if they do not have the transplant, and their rate of clinical decline, respectively, on the optimal listing strategy. To interpret the findings, note that the higher the value of

The effect of
The effect of

The effect of
From Figure 2 (left hand plot), the model suggests that the longer the patient is expected to wait on the list before an organ becomes available, the earlier he should be listed; that is, while he is still relatively well. This makes sense because if the doctor were to wait too long, she risks listing the patient when his clinical status is poor, and in that case, with a long expected waiting time, the patient may not survive long enough to get the organ.
On the other hand, from the right hand plot of Figure 2, if the patient is listed, a change in the expected waiting time has no impact on the delisting threshold. Hence, if their comorbidities are not too many, they should remain on the list, irrespective of the expected waiting time. (
From Figure 3, the shorter is the patient’s life expectancy if he does not have the transplant, the sooner he should be listed. This is again, intuitive, because of the expected waiting time. Another way of looking at this is that if the patient’s life expectancy is relatively long without the transplant, he has time to wait, and therefore, he does not have to be listed immediately.
Furthermore, a change in
Finally, from Figure 4, the more comorbidities the patient is acquiring per year, the earlier he should be listed; that is, if his clinical status is quickly deteriorating, he should be listed promptly. Once again, this implication suggested by the model is plausible and intuitive. Moreover, it upholds the suggestion by Kenny et al. 2 and Everitt et al. 15 that the unrelenting progression of physiological failure should prompt early consideration of transplantation in apparently stable patients.
However, a change in the rate of clinical decline has no impact on the threshold at which the patient should be removed from the list. This implies that if the patient is listed, he should remain so until enough comorbidities are realized (i.e., until
To summarize, the three important factors that the doctor ought to consider when deciding the best management strategy for a given patient are the rate of clinical decline, the patient’s life expectancy if he does not have the transplant, and the length of time he is expected to wait on the list are all incorporated into the model. The effects of these factors on the optimal listing decision implied by the model are plausible and realistic, which further implies that this model is a credible one for use in clinical practice.
Parameter Estimates
To calculate the
We also need to estimate
At any given point in time, the transplant coordinators at the transplant center have a good idea of the average waiting time for a patient about to be placed on the list. Part of their job is to examine the national transplant list on a daily basis so they always have a good understanding of its current status. Furthermore, they can personalize this estimate somewhat depending on the individual patient. For example, they may be able to say that an individual patient placed on the list on a given day is expected to wait on average 2 months. However, this estimate may be different for another patient with unusually high antibodies if they were to be listed on that same day. This is deemed to be a comorbidity because such a patient is much harder to match, and anecdotal evidence suggests they wait much longer than patients with few antibodies. In that case, if such a patient was to be listed immediately, the estimated waiting time for them may be, for example, 2 months, rather than 2 months. Similarly, patients with more comorbidities will be placed on the urgent list rather than the routine list giving them priority. Hence, a patient on the routine list has a longer expected waiting time than a patient on the urgent list. As such, it is up to the transplant coordinators to provide this patient specific estimate for
Finally, we need an estimate for the signal quality parameter
Conclusion
This article views the decision to list patients with a Fontan physiology for cardiac transplantation as a real option. I develop a model to determine the optimal time to list such patients in response to the various suggestions in the literature that listing these patients at the optimal time is “key to improving outcomes.” 7 However, as yet, determining the optimal time remains unclear. 2 This article addresses this need by providing a timing model that can be made easy to use in practice, and is plausible and robust in terms of the underpinning intuition.
However, it is worth pointing out two important limitations to this model that future versions will aim to account for. The first is that there is no distinction between the urgent and routine lists. Patients that are deemed sick enough are placed on the urgent list where they gain priority over less ill patients, even if those patients were listed earlier. A future version of this model could aim to separate the listing region into routine or urgent; that is, whether the patient should be urgently listed or not. This has big consequences in terms of waiting time, but also, patients who are urgently listed must remain in hospital while they wait for the organ, whereas routinely listed patients can wait at home living a relatively more normal life.
A further limitation is the following. The Fontan circulation has a significant impact on the liver owing to increased portal hypertension. In some patients, this can result in severe cirrhosis of the liver, and as such, some patients undergoing transplant after a Fontan are deemed to be in need of a heart and liver transplant. Both organs must be from the same donor and the double transplant is performed as a single operation and the listing must be for two organs; in other words, a patient needing both must be listed as needing both organs. The current model is based on the assumption that the patient in in need of just a heart, but a future version of this model could potentially signal whether the patient should be listed for just a heart or for both organs simultaneously. I would envisage that those patients deemed to be in need of both should be listed earlier (i.e., with fewer overall comorbidities) than those needing just a single organ, according to the decision criteria to be derived.
Supplemental Material
sj-bib-1-mpp-10.1177_23814683211057472 – Supplemental material for A Decision Rule for Determining the Optimal Transplant Listing Window for Patients With a Fontan Physiology
Supplemental material, sj-bib-1-mpp-10.1177_23814683211057472 for A Decision Rule for Determining the Optimal Transplant Listing Window for Patients With a Fontan Physiology by Laura Delaney in MDM Policy & Practice
Supplemental Material
sj-pdf-2-mpp-10.1177_23814683211057472 – Supplemental material for A Decision Rule for Determining the Optimal Transplant Listing Window for Patients With a Fontan Physiology
Supplemental material, sj-pdf-2-mpp-10.1177_23814683211057472 for A Decision Rule for Determining the Optimal Transplant Listing Window for Patients With a Fontan Physiology by Laura Delaney in MDM Policy & Practice
Supplemental Material
sj-tex-3-mpp-10.1177_23814683211057472 – Supplemental material for A Decision Rule for Determining the Optimal Transplant Listing Window for Patients With a Fontan Physiology
Supplemental material, sj-tex-3-mpp-10.1177_23814683211057472 for A Decision Rule for Determining the Optimal Transplant Listing Window for Patients With a Fontan Physiology by Laura Delaney in MDM Policy & Practice
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.