
Abstract
Introduction
With the efficacy of antiretroviral therapy (ART), HIV infection has evolved into a chronic disease, bringing with it new complexities of care such as multiple comorbidities and polypharmacy, which in turn suggests the need for new care models. 1 Similar to other chronic conditions, HIV is best managed by primary care providers (PCPs) collaborating with HIV specialists and allied health care providers.
Care for people with HIV is increasingly complex, requiring a continuum of care from primary prevention to viral suppression, as well as the management and prevention of other chronic physical and mental health conditions. HIV differs from the vast majority of chronic conditions because it is infectious, meaning that there is also a preventative aspect to HIV care for patients at risk but not infected. At one time this solely concerned counseling about safe sexual practices, but since 2012, when the US Food and Drug Agency approved ART for prophylactic use, it has included the possibility of pre-exposure prophylaxis (PrEP). People who are at high risk of HIV can now be prescribed daily antiretroviral medications before and after potential exposure, to be used in combination with other approaches to prevent infection. PrEP was approved by Health Canada in 2016.
HIV-specific outcomes are related to physician HIV experience.2,3 For family physicians with less HIV experience, the involvement of HIV specialists in the care provided to their HIV-positive patients can mitigate potential disparities. Electronic consultation can improve access to HIV specialist expertise in a primary care-dominated model of delivery. While the use of electronic consultation (eConsultation) in care for people living with HIV has not yet been described in the literature, there have been several studies on the use of telemedicine and remote consultation to connect health care providers to HIV specialists.4–9 For example, the University of Washington and Mountain West AIDS Education and Training Center developed a real-time video-based HIV program that connects community providers to both a multidisciplinary specialist team and to peer providers. 10 HIV Warmline, a free telephone consultation service in the United States, has been used to provide live HIV management advice to PCPs. 4 This service resulted in high rates of satisfaction, with the majority of PCPs reporting improved confidence in caring for people with HIV and avoided unnecessary specialist referrals.4,5 In the study of another telemedicine service to aid HIV management in a prison setting, telemedicine resulted in a greater proportion of patients with virologic suppression, appropriate ART use, patient compliance, and a higher mean CD4 count. 11
Our objective was to describe the use and impact of the Champlain BASE eConsult service in the care of people living with and at risk for HIV by characterizing the topics of eConsult usage, the nature of the responses, and the value and utility of the service as reflected in survey feedback from PCPs.
Methods
We conducted a convergent parallel design mixed methods study 12 of eConsult cases submitted by PCPs to HIV specialist providers. Quantitative and qualitative data were collected concurrently, but were analyzed separately. Quantitative results (HIV specialist type, question type, and PCP disposition) were used to triangulate the qualitative findings, which in turn were used to further understand the quantitative results, thereby integrating the two. 13
Champlain BASE eConsult
The Champlain BASE eConsult service provides a secure, web-based system that allows for asynchronous communication between PCPs and specialists. A detailed description of the service has been reported previously. 14 In summary, PCPs can submit questions regarding patient care and attach any accompanying files (e.g., laboratory results, images, data from electronic medical records) to an appropriate specialty of their choice. Unlike most of the other eConsult specialties, the HIV service allows PCPs to ask questions not only of medical specialists but also of pharmacists and social workers. In our jurisdiction, specialists are remunerated for their consultation. The PCP and the specialist can exchange dialogue and request additional information until the case is closed by the PCP. To close a case, PCPs are prompted to participate in a mandatory close-out survey to assess the value and utility of the eConsult service. This survey asked about the outcomes and value of the eConsult service, and solicited feedback from the PCP.
Setting
The Champlain BASE eConsult service is offered in the Champlain Local Health Integration Network (LHIN), a health region in Eastern Ontario, Canada, and is in the process of being adopted by other jurisdictions across the country. The demographic and health profiles of this region, where approximately 2,000 people are living with HIV 15 and approximately 1400 PCPs provide their services, are similar to the rest of Ontario. 16 The health care system in Canada is publicly funded, and medically necessary services are covered through provincial health insurance plans.
Data Collection
The Champlain BASE eConsult service collects data on the patient, PCP, and specialist, including patient date of birth and sex, PCP and specialist gender, clinic postal code, and the type of PCP (i.e., MD or nurse practitioner). All records of communication through the eConsult platform and any attached files are saved in the consultation record. PCP submission time, specialist response time, specialist self-reported billing time for answering the consultation, and the close-out survey responses are all collected.
In addition to the written questions from PCPs and the written responses to those questions from specialist providers, we used the data from two different versions of the five-question PCP close-out survey: the original version (Appendix A) and an updated version that was employed starting October 2016 (Appendix B).
Analysis
Descriptive statistics were used to analyze PCP survey responses and data collected by the eConsult service, including PCP provider type, patient age and sex, specialist type, response time, and specialists’ self-reported billing time.
To establish an overview of the range of topics, two team members, one of them a PCP with experience providing care for people living with HIV, individually classified each eConsult by question type using a predefined list based on validated taxonomy, 17 consistent with the analyses of other eConsult cases.18–20 They compared their results to ensure concordance and resolved disagreements by meeting with the rest of the review team.
We used constant comparative method to analyze the written data records. 21 Three team members (JP, ES, MF) independently coded the eConsult questions and responses without a preconceived framework, to identify initial codes, comparing each segment of data with other segments for similarities and differences. Team members met to discuss the codes and their relevance in relation to the research questions and established initial overarching themes and a corresponding coding framework. Through iterative independent coding, we modified the framework to create separate themes for the two separate populations involved, people living with HIV and people at risk for acquiring HIV, and to identify dimensions and properties that are specific to these themes. The final framework was reviewed and approved by the review team.
Results
Quantitative Results
Between February 2015 and December 2017, 21 PCPs in the Champlain LHIN submitted 46 eConsults to HIV specialists. A summary of PCP and patient characteristics are available in Table 1. Twenty-six cases (56.5%) were answered by an HIV specialist physician, one case (2.2%) was answered by an HIV pediatrician, one case (2.2%) was answered by an HIV social worker, and the remaining 18 cases (39.1%) were answered by a pharmacist specializing in HIV treatment.
Primary Care Provider (PCP) and Patient Characteristics of eConsults Sent to the HIV Specialty Group

The response times ranged from 45 minutes to 16 days, with a median response of 1 day and 18 hours from time of submission to first response from the specialist. Response times were 3 days or less for 65.2% of cases. The majority (63.0%) of specialist self-reported billing times (i.e., the time the specialist took to answer) were 10 to 15 minutes or less (see Figure 1).

HIV eConsult specialist self-reported billing times (February 2015 to December 2017; n = 46).
The taxonomy classification showed that the most common question type was drug treatment (58.7%), followed by management (19.6%) and diagnosis (13.0%; Table 2). For the 27 drug treatment questions, 14 cases pertained to how to prescribe a particular drug (51.9%), whereas 6 cases asked about drug interactions.
Classification of Question Type of eConsults (n = 46)

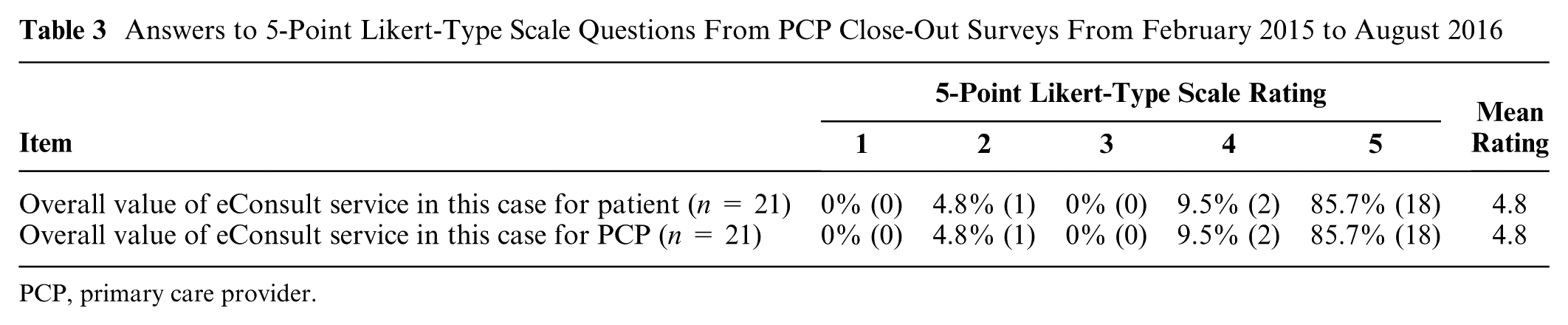
The answers to the 5-point Likert-type scale questions of the PCP close-out survey are summarized in Tables 3 and 4. PCPs highly valued the eConsult service (average rating 4.8/5). Overall, across both surveys, PCPs indicated that they received good advice for a new or additional course of action in 58.7% of cases, where 56.5% indicated that they would be implementing the specialist’s advice and 2.2% indicated they are not able to implement. In the remaining 41.6% of cases, PCPs were able to confirm their original course of action that they could implement. In 10.9% of cases, referral was originally contemplated but now avoided.
Answers to 5-Point Likert-Type Scale Questions From PCP Close-Out Surveys From February 2015 to August 2016
PCP, primary care provider.
Answers to 5-Point Likert-Type Scale Questions From PCP Close-Out Surveys From October 2016 to December 2017

PCP, primary care provider.
Qualitative Findings
Thematic Analysis
Thematic analysis of the eConsult logs showed a marked divide between those that concerned patients living with HIV (n = 29) and those that concerned patients at risk of contracting HIV (n = 17). The former were predominantly about complexities of care, whereas the latter were predominantly about PrEP. There was little, if any, thematic overlap between the two patient populations. For this reason, the thematic analysis of the consultation logs was similarly divided.
Complexities of Care for People Living With HIV
The consultations concerning patients living with HIV spanned a range of issues falling under the general heading of complexities of care such as comorbidities and drug interactions, vaccines, comorbidity management, affordability, and testing.
Comorbidities and drug interactions
The most common question PCPs asked (9/29) had to do with drug interactions resulting from treatment for comorbidities. These were invariably answered by the HIV Pharmacist. In some cases the PCPs had checked themselves, and were double checking by eConsult: “As per Lexicomp, no drug interactions but we were hoping to double check with you” (C6). The comorbidities in question ranged from sinusitis to depression and anxiety to nausea. The questions sometimes also involved dosing levels and/or frequencies.
Vaccine indications
A smaller number of questions (5/29) were similar in asking about appropriateness of and indication for vaccines for conditions such as shingles, hepatitis B, MMR, and yellow fever. A typical brief question was about the shingles vaccine: “His last CD4 was . . . and VL is undete[c]table (see attached). Do you think it is safe to give to him with his . . . CD4 count?” (C33). The majority of these questions (4/5) were answered by an HIV Specialist. All but one were answered succinctly, most notably, “Yes” (C35).
In one case concerning the shingles vaccine Zostavax, the HIV Specialist provided extensive evidence for the recommendation, including details from “a guideline recommendation” (C19), references and links to the US and Canadian guidelines, and a consultation with another HIV Specialist: So, you have two ID/HIV-ologists who say OK, one guideline which says OK in principle, one guideline which says no, and one guideline which says no evidence (of safety and efficacy). I would go ahead, and warn the patient about possible fever. (C19)
Affordability
Equally common were questions about ART coverage and affordability. These questions concerned patients having difficulty affording their ART medications. “[D]ifficulty affording her Complera Pts works is covering 70% Can not afford her co-pay $600/ mo Has missed 3 days of pills—contacted us today. Could you please help us/her WE have also advised her to contact you” (C43). Questions about affordability were most often answered by the HIV Pharmacist, except in one case, where the HIV Social Worker responded to a question that the HIV Pharmacist subsequently responded to as well. These responses tended to exhibit a shared care approach.
Testing
Three questions pertained predominantly to aspects of testing, such as type and frequency: “How often shall I run her viral load, metabolic profile (normal in November) and CBC [complete blood count] with CD4/CD8 ratio . . . given change in medication. Is 3 months ok?” (C15).
Other
The remaining three consultations concerned prenatal care, a patient who was requesting referral to the HIV Specialist, and an unknown reason.
Suggestion of Coordinated Care
Consultations often exhibited the suggestion or invitation from the specialist to engage in coordinated patient care. The HIV Pharmacist tended to suggest either multidisciplinary approaches to care, such as the following response in a question concerning affordability, “I suggest that we readdress this problem along with our Social worker to see what is the best solution for her” (C38), or to offer to coordinate care, as in the following response to a question about prenatal care, “If interested, I could coordinate it from our clinic” (C10).
Also notable in this regard was that this specialist did not simply assume that a patient would come to the HIV clinic, “If the patient is OK with the idea to come back to Mod G, you could send her back to see XXXX and we could discuss all options with her” (C37).
In some instances, the HIV Specialists also responded with a shared care approach, “So there is no need to send him here urgently, but certainly do so any time in the future you like” (C23). In other cases, though, specialists seemed to want to re-assume the coordination of care from the PCP. For example, when a PCP asked for suggestions for management of comorbidities, the HIV Specialist responded by simply saying, “Noted—booked in clinic for next week” (C22).
In another case, “Healthy HIV+ woman with a slightly tender indistinct mass on the floor of her mouth” (C30), the PCP asked, “Could this be related to HIV? Would you recommend any other investigations and/or a referral to ENT?” (C30). The HIV Specialist responded that “a mass on the floor of the mouth is exceedingly unlikely to be related to HIV” (C30), and therefore concurred with “an immediate referral to ENT.” However, the HIV Specialist also requested a referral, saying, “I will also see YYY in Module G” (C30). It is unclear from the exchange why the HIV Specialist felt the need to directly reassume care in this way.
Some responses were supplemented by attaching or providing links and references to journal articles or guidelines, or suggestions of other resources. These kinds of responses aimed to help the PCP to facilitate the current care and to deal with similar instances in the future. The HIV Pharmacist, in particular, frequently used the response as a teaching opportunity by providing a detailed response using relevant literature and experience. In most cases, the specialists and PCPs tended to work together as a community of practice to create more efficient strategies for care, and seemed to specifically acknowledge one another’s involvement, as with this common closing line from a PCP: “Thank you for sharing your expertise and knowledge and participating in this patient’s health care” (C26).
Patients at Risk for HIV
The majority of eConsults (11/17, 64.7%) concerning patients at risk were about PrEP, with the balance covering questions about post-exposure prophylaxis, sero-discordance, and testing to confirm HIV-status.
Prescription of pre-exposure prophylaxis
PCPs consulted with specialists only about initiating PrEP; no questions were asked concerning patients already prescribed PrEP. The majority of PrEP eConsults (8/11, 72.7%) were initiated by PCPs because their “patient is interested on starting PrEP” (C1) or the patient “requested PREP treatment” (C18). In three cases, PCPs had questions regarding PrEP without patients asking for it. PCPs described in detail patients’ risk profiles, including sexual health behaviors and recreational substance use, specifically when the inquiry was for patients who were men who have sex with other men (MSM), which made up the majority of cases (8/11, 72.7%).
Questions tended to be asked in detail about indications for PrEP, how to prescribe it, and available resources and guidelines to manage the patients’ care. Specialists did not provide detailed answers to these PrEP questions and requested referrals for all cases. One specialist explained why the patient would be a good candidate for PrEP and another outlined the importance of safer sexual practices counselling, but in no cases were any knowledge or resources shared with the PCPs that would enable them to initiate and manage the care of a patient on PrEP.
Other
Seven cases involved serodiscordance, patients at risk of HIV who are in a long-term relationship with partners living with HIV. The majority of questions for these patients (5/7, 71.4%) related to PrEP as well. PCPs also inquired about the frequency of HIV testing, “Wife is HIV positive, on retroviral therapy. They are using condoms for intercourse. How frequently would you recommend that he have HIV testing” (C42), as well as about the possibility of having children, “Is there a way he can hope to have [kids], with limited risk for him to be infected?” (C46). In one case, the PCP asked about how to prescribe post-exposure prophylaxis (PEP) for a patient who was recently exposed to HIV.
Discussion
We have demonstrated that eConsult is highly valued and effectively provides expert advice, guidance, and education to PCPs related to their patients living with and at risk for HIV. Given that in our jurisdiction many people with HIV receive care from PCPs who have limited experience with HIV management, 22 eConsult can facilitate the delivery of comprehensive and coordinated care by connecting PCPs to a group of medical and allied health professionals with HIV expertise.
The HIV eConsult service includes pharmacists and social workers as specialists that can be consulted. Though the majority of eConsults were sent to HIV medical specialists, over one third were sent to HIV pharmacists, emphasizing the importance and complexity of drug treatment for people with HIV and the value of allied health professionals. Other studies have also demonstrated improvements in health outcomes from integrating allied health professionals into the primary care of HIV. 23 The most common question types asked involved drug treatment and management, highlighting the medical complexity of people living with HIV and the coordination of care. This is also reflected in the common themes that emerged from the eConsults: 1) complexities of care for people living with HIV and 2) suggestion of coordinated care. The prevalence of comorbidities and the complexity of drug treatment emphasize the need for collaborative care and ongoing education of PCPs, to provide the best standard of care for people living with HIV. 1
HIV prevention as an aspect of care for patients at risk for HIV is also a common issue for PCPs, in particular in relation to PrEP. Since those who are at risk for HIV will receive care from PCPs rather than HIV specialists, 24 access to specialist advice through eConsult can be a valuable resource. However, rather than guiding the PCP through strategies for PrEP delivery and management, specialists recommended the patients be referred to the HIV specialist in the region with PrEP expertise. PCPs participating in eConsult for their patients at risk for HIV were not well informed about the use of PrEP, likely as it was approved for use by Health Canada in February 2016, 25 halfway through the study timeline, and was only included in the formulary of publicly covered drugs in Ontario in September 2017. 26 However, surveys have shown that providers feel that it lies within their scope of practice, and that primary care is an appropriate setting for this aspect of HIV care.27–29 A study done using a Project ECHO telehealth program to deliver PrEP education showed that providers reported improved knowledge about, and increased likelihood of providing, PrEP. 30
The lack of PCP knowledge is compounded by the fact that there are not enough HIV specialists to meet projected demand for PrEP. 29 Although the number of PrEP initiations in Canada is small at present, this will likely change with increasing awareness. 29 As PrEP use expands, the need for HIV specialist advice is likely to grow to help deal with, for example, unexpected adverse effects from the medications, nonadherence, and exposures to potentially drug-resistant HIV. With increasing awareness and requests from patients and the accessibility of guidelines, including the Centers for Disease Control and Prevention PrEP Guidelines in the United States 31 and the Canadian guideline on PrEP, 32 we anticipate specialists will become increasingly confident and better able to provide PrEP recommendations to PCPs through eConsult. 33 We also anticipate this approach would reduce the need for face-to-face referrals while increasing the overall uptake of PrEP.28,*
To our knowledge, this study is the first to report on the use of an eConsultation system for access to HIV specialists. However, there were some limitations. First, we had a small sample size of 46 eConsults from 21 different PCPs, a very small fraction of the PCPs in the region. There were eight different specialists, with only one being from HIV pharmacy and one from HIV social work. In the future, we anticipate more specialists on the service as eConsult is adopted by other regions and provinces. The small sample size resulted in the decision to conduct a thematic analysis rather than classify the question content based on predefined categories as done in previous studies.18,20 The cases were for patients in the Champlain LHIN, which may limit generalizability to other regions. Additionally, the value and impact of the eConsult service was measured subjectively through close-out surveys answered by the PCP, which may not reflect the perspectives of the patients or specialists involved. Though PCPs reported positive experiences, we do not know whether eConsults led to improved clinical outcomes of patients or if the actual number of referrals to HIV specialists were reduced. However, we would anticipate a reduction in the number of referrals based on our research in this area. 34
In conclusion, PCPs are well able to care for the complex needs of people living with HIV or at risk for HIV. The eConsult service is instrumental in supporting PCPs because it is an efficient way for communication and education between PCPs and HIV specialists and enables specialists to disseminate information including guidelines and to facilitate care coordination. With increased promotion 32 and uptake of PrEP, such a service has the potential to support the efficient collaboration between PCPs and specialists in the fight to reduce HIV transmission while providing the most appropriate care to their patients.
Supplemental Material
Kendall_et_al_-_HIV_eConsults_-_Medical_Decision_Making_-_Appendix_A_online_supp – Supplemental material for Evolving Toward Shared HIV Care Using the Champlain BASE eConsult Service
Supplemental material, Kendall_et_al_-_HIV_eConsults_-_Medical_Decision_Making_-_Appendix_A_online_supp for Evolving Toward Shared HIV Care Using the Champlain BASE eConsult Service by Claire E. Kendall, Janessa E. Porter, Esther S. Shoemaker, Rachel Seoyeon Kang, Michael Fitzgerald, Erin Keely, Amir Afkham, Lois Crowe, Paul MacPherson, Ron Rosenes, Philip Lundrigan, Christine Bibeau and Clare Liddy in MDM Policy & Practice
Supplemental Material
Kendall_et_al_-_HIV_eConsults_-_Medical_Decision_Making_-_Appendix_B_online_supp – Supplemental material for Evolving Toward Shared HIV Care Using the Champlain BASE eConsult Service
Supplemental material, Kendall_et_al_-_HIV_eConsults_-_Medical_Decision_Making_-_Appendix_B_online_supp for Evolving Toward Shared HIV Care Using the Champlain BASE eConsult Service by Claire E. Kendall, Janessa E. Porter, Esther S. Shoemaker, Rachel Seoyeon Kang, Michael Fitzgerald, Erin Keely, Amir Afkham, Lois Crowe, Paul MacPherson, Ron Rosenes, Philip Lundrigan, Christine Bibeau and Clare Liddy in MDM Policy & Practice
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this project was provided through the Canadian Institutes of Health Research (CIHR) under Grant FRN TT5-128270. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
Authors’ Note
The work reported in this article was carried out at the C.T. Lamont Primary Health Care Research Centre, Bruyère Research Institute, Ottawa, Canada. Preliminary results from this study were presented at the 28th Annual Canadian Conference on HIV/AIDS Research (CAHR) in 2018.
Supplemental Material
*
As of August 2018, the eConsult service has included HIV PrEP as its own option, to allow PCPs to submit questions specifically related to that topic and ensure these questions get assigned to the most appropriate HIV specialist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.