
Abstract
Keywords
Shared decision making between patients and their health care provider is a well-recognized goal throughout health care.1–3 It is especially important in situations where the consequences of treatment decisions are irreversible, complicated, uncertain, and severe. 4 An example of such a scenario is the patient’s decision to receive a durable left ventricular assist device (LVAD), a decision that involves a highly invasive treatment strategy with complex trade-offs that affect patient survival and quality of life over an extended period.
LVAD therapy is one of the limited treatment options for patients with end-stage heart failure (HF). Initially used to bridge patients to a heart transplant, LVADs are now also offered as a destination therapy to patients who are ineligible for a transplant. Use of an LVAD can extend survival and increase quality of life,5,6 but also requires significant changes in daily life, investment of time and money from the patient and their caregiver, and presents a risk of severe adverse events such as stroke and infection. 7
End-stage HF patients typically experience a long, slow disease progression that can leave them physically and emotionally exhausted by the time of LVAD decision making. 8 They often have made several other medical decisions during their disease progression, such as use of statins 9 or implantable cardiac defibrillator. 10 They may also be cognitively impaired from their disease. 11 Additionally, many HF patients perceive the decision to receive an LVAD as choice between life and death, without other “real” options. 12 These factors make designing a decision support tool for LVAD implant a complicated endeavor, requiring a balance of accessibility and comprehensive educational information without being overwhelming.
The primary goal of this study was to characterize the decision support needs of end-stage HF patients during the LVAD implant decision process. A secondary goal was to identify which variables had the most influence on patient engagement, to inform the development of a decision support tool.
Methods
A paper-based survey was developed by biomedical engineering researchers at Carnegie Mellon University (CMU) that included domains related to patient interaction with their cardiologist, interest and comfort with medical information related to their condition, and familiarity with quantitative data visualizations. (The full survey is included in the Supplemental Materials.) The survey protocol was approved by the institutional review boards at CMU and Allegheny General Hospital (AGH). All study participants provided written informed consent and were not compensated for participating in the study.
Patient Cohort and Data Collection
Patients were enrolled at AGH between May 2015 and April 2016. Adult (age ≥18 years) patients who were New York Heart Association (NYHA) class III to IV and referred to the advanced heart failure program in the outpatient setting for LVAD evaluation were recruited to participate in the survey. Device indication (destination therapy or bridge to transplant) was not collected at the time of surveying, as decisions to implant had not been made. Patients unable to provide consent due to mental or physical inability were excluded. Surveys were administered by a study coordinator prior to the patients’ clinic visit and could skip questions. All patients who began the survey completed it (n = 35).
Data Analysis
Survey responses were coded into nominal variables for analysis. Missing data elements were classified in their own category, missing, and were not imputed. Descriptive statistics were analyzed in SPSS.
Survey data was analyzed by the Bayesian Search method in GeNie 2.2 (BayesFusion LLC, Pittsburgh, PA). Model background knowledge was organized such that follow-up or dependent survey questions were secondary to initial or stand-alone questions. The network structure was learned over 20 iterations, with a sensitivity of 10% and prior link probabilities of 0.05, 0.01, and 0.001, to assess the stability of the links. The number of iterations it took to achieve the best model version was 12, 3, and 1, respectively. Results were visualized as a directional nodal network, with the arcs between nodes representing the influence between responses, the arc pointing to the dependent variable, and their thickness indicating the strength of the association. 13 Variables without any relationships were shown as nodes without any arcs.
Analysis of the open-ended last question was performed by grounded theory method. Three of the authors (LCL, LB, AN) evaluated the open-ended responses independently, developing codes for the content as they reviewed the responses. They convened to review their coding and discuss any difference of opinion. The final coding was agreed upon and then categorized into six topics: non-answers, expressions of uncertainty, health outcomes, technical information, expressing emotions, and treatment decision.
Results
We surveyed 35 patients using a 44-item questionnaire. Patients were 83% male, predominantly NYHA class III (n = 15, 43%), with an average age of 60 years (range 25–78 years). Most of the patients were in clinic for a follow-up visit (n = 11, 31%) or consultation (n = 15, 43%), but some were being seen in anticipation of LVAD implant (n = 5, 11%). The respondent cohort is summarized in Table 1.
Patient Demographics
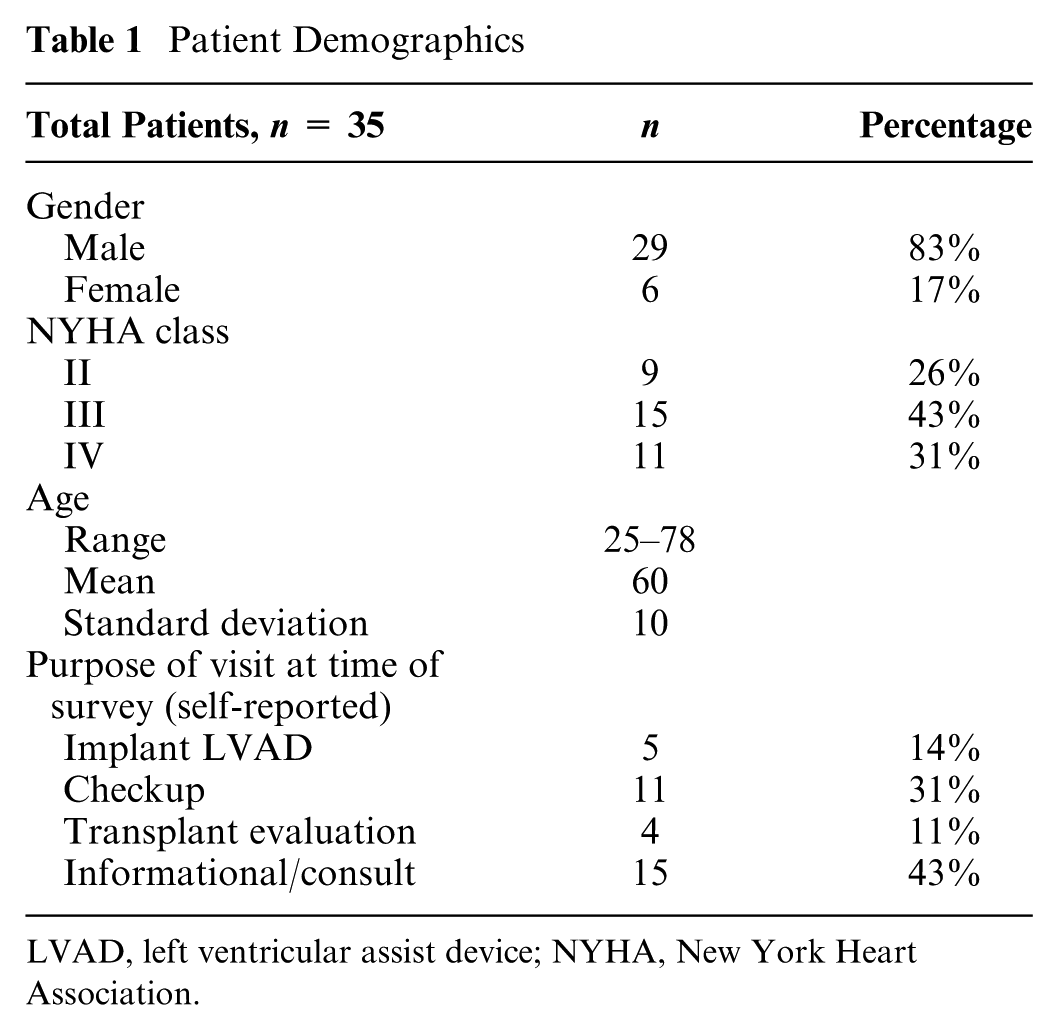
LVAD, left ventricular assist device; NYHA, New York Heart Association.
Awareness of Condition and Interaction With Physician
Responses related to awareness of condition and interaction are summarized in Table 2. Most patients knew their cardiologist (97%), felt comfortable discussing their physical and emotional state with their medical team (91%), preferred communicating with their doctor in person (83%), but would use an email or message system if it was available (54%). When interacting with their doctor, most patients reported spending over 60 minutes talking about their condition (89%) and were satisfied with the duration of their interaction (66%).
Awareness of condition and interaction with physician
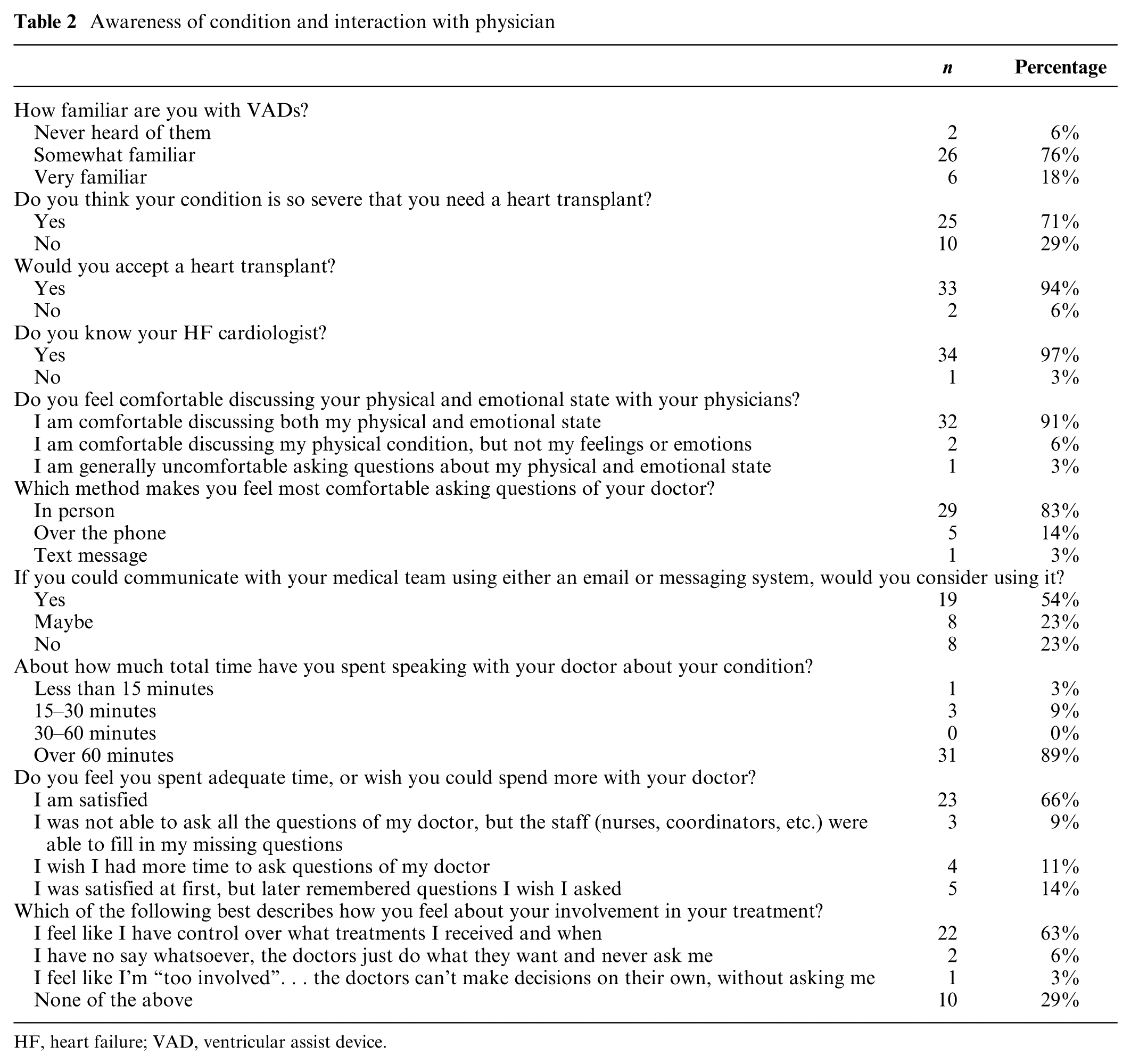
HF, heart failure; VAD, ventricular assist device.
Information Seeking Habits
Responses related to patient information seeking habits are summarized in Table 3. In terms of learning more about their health, most patients expressed the desire to view their medical records (74%) but had not ever requested to see them (74%). Most patients did do online research about LVADs (57%). While most patients had not used a decision support tool in any context (65%), many thought a roadmap of their health care progression would be useful (46%). They also believed that a website or computer program with their prognosis would be useful (51%) and were interested in accessing videos of patients telling stories of their implant experiences (57%).
Information seeking habits

Technology Use and Numeracy
Responses related to technology use and numeracy are summarized in Table 4. Most patients did not use a smartphone (51%) or tablet (66%) but did use a computer at least occasionally (69%). Most patients were very comfortable understanding bar graphs (63%), line graphs (60%), and pie charts (80%). Fewer patients were very confident interpreting survival curves (37%).
Technology use and numeracy

Free-Text Response Analysis
In response to the open-ended question, “If you could imagine a computer wizard that could answer all your questions, what would you ask?” participants gave responses that fell into six categories: Non-answer, Uncertainty, Health outcomes, Technical Information Seeking, Expressing Emotions, and Treatment Decisions (Table 5). The most common response was the non-answer, followed by health outcomes. LVADs and heart transplants were mentioned twice each in the Treatment Decisions category.
Responses to free text question, “If you could imagine a computer wizard that could answer all your questions, what would you ask?”

LVAD, left ventricular assist device.
Bayesian Search Results
Bayesian search analysis was used to explore relationships between patient features and engagement. At the 0.05 prior probability threshold, there were two networks involving 18 of the 35 input variables (Figure 1). In the larger network, “comfort discussing health with physician” was connected to familiarity with LVADs, patient diagnosis, whether the patient knew their cardiologist, whether patient had requested electronic health record (EHR) in the past, preferred method for communicating with clinicians, and use of the website HeartHope.com . The second network had two variables, both addressing self-reported numeracy: comfort understanding line graphs connected to comfort understanding bar graphs. The strongest associations between variables were whether the patient knew their diagnosis and the amount of time they had spent discussing treatment (0.67), comfort interpreting line graphs and comfort interpreting bar graphs (0.56), and doing online research using WebMD (0.52).

Bayesian model of patient responses with link probability threshold 0.05. Each question in the survey is represented by a node. Arcs between nodes represent relationships between responses to these questions. Arc direction indicates the directionality of the relationship, with the arc pointing at the dependent node. Arc thickness indicates the strength of the association. The range for strength of relationship is 0.14 (between Comfort discussing health with physician and Know your cardiologist?) to 0.67 (between Know Diagnosis and Amount of time discussing treatment).
At the 0.01 prior probability threshold, there were four networks involving 10 of the 35 input variables (Figure 2). These networks were the following: 1) websites used for online research; 2) the comfort with, and time spent, discussing health with physicians; 3) desire to understand condition and experience requesting EHR; and 4) self-reported numeracy. The strongest relationships were doing online research with using WebMD (0.77), using WebMD with HeartHope (0.59), and amount of time discussing with physicians and comfort discussing health with physician (0.47).

Bayesian model of patient responses with link probability threshold 0.01. The range for strength of relationship is 0.23 (between Time spent discussing and Comfort discussing health with physician) to 0.77 (between Did online research? and WebMD).
From 0.05 to 0.01 prior probability, the direction of the relationship between desire to understand condition and experience with requesting EHR flipped, indicating that the relationship is present, but not strongly causative one way or another. Drilling into the interactions in the third network: patients who had previously asked for their records but could not understand them (7%) indicated the least interest in health engagement (47% uninterested compared with 12% for patients who had not viewed their records and 4% for patients who had viewed and understood them).
At the 0.001 prior probability threshold, only 3 variables were interconnected (Figure 3). These were the relationships between online research and websites used.

Bayesian model of patient responses with link probability threshold 0.001. The range for strength of relationship is 0.51 (between Other and WebMD) to 0.57 (between WebMD and HeartHope.com).
Discussion
This survey shows that the end-stage HF population is largely amenable to engage in their health care, with most patients comfortable discussing their health with their doctors (91%), satisfied with their participation in treatment decisions (66%), and interested in accessing their health records (74%). However, when asked if they had sought out their records in the past, most had not (74%).
A Bayesian learning algorithm was used to look for relationships between the variables affecting patient engagement. Interestingly, patient age, gender, and NYHA status were not associated with any of the other responses in the study. Studies of these features on heart failure patient activation and self-care have varied results: younger age was found to be slightly associated with better activation,14–16 while other studies found the opposite,17–19 and still others found no difference due to age. 20 For gender, there is similar disparity in the literature: some studies find better engagement in women14,21 others in men,17,19 while other studies find that gender-related features like marital status or type of disease (diastolic heart failure, which is more common in women) add nuisance to the gender effect.15,22 Increased disease severity has been shown to be connected to better patient self-management16,17,23 but was not shown to have an impact on patient activation. 14 Differences in age and disease severity effect may be related to the specific outcome being measured. Though patient activation and self-care are similar in result, the specifics of the measures are different. Increased patient activation measure tends to align with younger, healthier patients, while increased self-care with the older, sicker patients.
The Bayesian network analysis showed that comfort talking to physicians was integral to patient engagement, as demonstrated by the links to patient’s knowing their diagnosis, familiarity with VADs, and previously requesting their EHRs. This is consistent with prior studies, where patients who expressed more comfort in their communication with their physician had better activation, 24 satisfaction, 25 and adherence to treatment.26,27 With increasing sensitivity of the Bayesian network learning, comfort communicating with physician was linked to time spent talking to the physician. This connection between time spent communicating and comfort or satisfaction is also established in the literature. 28
At both the 0.05 and 0.01 prior probabilities, there was a link between the patient’s desire to understand their condition and their experience with previously requesting their medical information. This can be interpreted as a relationship between engagement and patient health literacy (represented here as the ability to understand an EHR). This relationship is consistent with a prior findings in cancer patients where health engagement was correlated with highest level of patient education 29 and with a study finding that subjective patient numeracy and satisfaction with physician communication were inversely related. 30 Additionally, patients may feel discouraged from not understanding their health information and therefore be less likely to try to engage again.
Grounded theory analysis showed patients’ desire for information about their health outcomes. Interestingly, there was little expressed desire for technical information about the treatment options (9%, n = 3). This is usually a focus of patient education in decision support tools.31,32 The feature most mentioned was the desire to have prognostic information (34%, n = 12). While current decision support tools do not provide a personalized prognosis for patients, our research group has developed and validated mortality predictions,33,34 with the goal of including this information in a patient-facing decision support tool.
Heart transplant was mentioned twice in the open-ended question answers, despite the study and questions focusing on LVAD treatment. This may be due to a tendency for “wishful thinking,” where a heart transplant is the more desirable treatment option than the LVAD. This can be described by uncertainty management theory, 35 that patients may choose pieces of information to focus on to feel more hope. This was also seen in an LVAD patient interview study, where destination therapy LVAD patients expressed their belief that they would most likely get a heart transplant. 12
Most patients did not answer the open-ended question (n = 14, 40%), which may have been due to the patients’ lack of comfort verbalizing their concerns to someone (in this case, the research coordinator) in a clinical setting. From a design standpoint, a support tool that can be used privately by the patient may provide an opportunity for engagement when patients may otherwise feel uncomfortable. Examples of success with a nonhuman interactive tool have been seen in the mental health space: with the use of artificial intelligence to provide therapy to patients with posttraumatic stress disorder 36 and use of a chatbot with college students dealing with depression. 37
This study has several implications for the design of an LVAD decision support tool. Inclusion of content beyond technical information, like patient prognosis, videos of patients talking about their treatment experiences, and roadmaps of disease progression is important for patients to fully grasp the risks and implications of their treatment decision. Presentation of material must be accessible for users with lower health literacy, especially given the cognitive impairment already present in this patient population. An interface that can be used privately is important for supporting patients who may not be comfortable discussing their health with their physicians. Responses about use of technology indicated that while most patients are not using a smartphone or tablet regularly, many are using computers. There is potential for a personalized, “smart” decision support tool that expands on the current paper-based tools already developed.38,39
Limitations
Recruitment for this survey was conducted with patients attending the clinic for an informational discussion, follow-up, or evaluation for LVAD or heart transplant; therefore, sampling may be biased toward patients with more compliant health practices. The design of the survey questions was meant to cover a wide range of information about patient engagement in an exploratory fashion. The survey did not use validated metrics like patient activation measure, 40 decision conflict scale, 41 or the controlled preferences scale. 42 It also did not include metrics of patient cognitive impairment or socioeconomic status, which may affect patient engagement.11,29 The low number of patients surveyed in this study limits the utility of the Bayesian network analysis for making predictions. 43 Future work would be to construct a larger survey study to focus on the role of numeracy on patient engagement in this unique population, particularly in the context of delivering prognostic information.
Conclusion
HF patients being considered for LVAD implant are generally inclined to engage with their health decision making; however, those who had not understood their health information in the past or who had poor numeracy indicated low interest in, or comfort with, health care engagement. There is a need for a decision support tool that can be accessible for patients of all numeracy levels to guide patients when considering an LVAD implant.
Supplemental Material
CORA_Interview_questions_online_supp – Supplemental material for Factors Affecting Health Care Engagement of Patients With End-Stage Heart Failure: An Exploratory Survey Study
Supplemental material, CORA_Interview_questions_online_supp for Factors Affecting Health Care Engagement of Patients With End-Stage Heart Failure: An Exploratory Survey Study by Lisa Carey Lohmueller, Aakanksha Naik, Luke Breitfeller, Colleen K. McIlvennan, Manreet Kanwar, Srinivas Murali, Carolyn Rosé and James F. Antaki in MDM Policy & Practice
Footnotes
Acknowledgements
Thanks to co-investigators Dr. Robert Tonks (at Duke at the time of the study) and Catherine Siegfried (AGH) for recruiting patients and administering surveys.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided entirely by an R01 grant from National Institutes of Health/National Heart, Lung, and Blood Institute (R01HL086918). The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
Authors’ Note
Survey study was performed at Allegheny General Hospital with analysis performed at Carnegie Mellon University, Language Technologies Institute.
Patient data were collected for this study using informed consent at Allegheny General Hospital and is not available for public access. Interested parties can contact the corresponding author to establish a data use and sharing agreement. Models developed from these data are available on the project website (![]() ).
).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.