
Abstract
Introduction:
This review presents a scoping review exploring the characteristics of value-based oral health care (VBOHC) and the potential to transform the delivery of dental services. VBOHC represents a shift from the traditional fee-for-service model, which prioritises service volume, to a system focused on improving patient outcomes, enhancing preventive care, and optimising cost-efficiency.
Objectives:
To identify and synthesise the defining characteristics of VBOHC and assess the potential to enhance patient outcomes, cost-efficiency, and care delivery in dental systems.
Methods:
Following methodology per the Joanna Briggs Institute and guidance per PRISMA-ScR reporting (Preferred Reporting Items for Systematic Reviews and Meta-analyses extension for Scoping Reviews), a scoping review was undertaken to include literature discussing VBOHC across various health care settings. Searches were undertaken in 6 relevant databases. Peer-reviewed quantitative and qualitative studies published in English were included and thematically analysed. A total of 50 studies were included after 185 studies were screened.
Results:
This research identifies several defining characteristics of VBOHC, including prevention and early intervention, patient-centred care, shared decision making, and outcome-based compensation. The scoping review highlights how VBOHC emphasises preventive care to reduce the incidence of severe dental conditions, particularly benefiting vulnerable populations with limited access to regular care. By encouraging proactive engagement with oral health, VBOHC improves long-term patient outcomes while reducing health care costs. Additionally, VBOHC promotes shared decision making, fostering a collaborative relationship between providers and patients, which enhances patient satisfaction and adherence to treatment plans. For providers, the transition to VBOHC requires significant operational and cultural changes, including adopting new workflows focused on outcomes, incorporating digital health technologies, embracing team-based care models, and integrating dental services into broader health care systems.
Conclusion:
This review concludes that VBOHC is characterised by patient empowerment and a patient-centred whole system approach. However, successful implementation requires addressing the challenges associated with transitioning from the fee-for-service model, particularly through provider support, infrastructure investments, and policy reforms.
Knowledge Transfer Statement:
The findings of this scoping review can inform policy makers, dental professionals, and health service planners seeking to implement value-based oral health care models. By understanding the core characteristics, this evidence can support more sustainable, equitable, and efficient dental care delivery across a range of health care settings.
Keywords
Introduction
Value-based oral health care (VBOHC) represents a paradigm shift from the traditional fee-for-service (FFS) model to one that emphasises the value of care provided to patients.
The traditional FFS model in dentistry incentivises providers based on the volume of services delivered, often leading to an emphasis on dental procedures rather than on preventive care or long-term patient health (Hegde and Haddock 2019). This model can result in unnecessary treatments, increased costs, and variability in care quality. In contrast, VBOHC is characterised by incentive structures that link reimbursement to patient outcomes and measurable improvements in oral health. Across the literature, VBOHC is described as aiming to improve care quality, patient experience, and cost efficiency (Boynes et al 2020).
The concept of VBOHC is deeply rooted in the broader movement toward value-based health care (Dawda et al 2022). Oral health is crucial to overall health and is fundamental to well-being and quality of life. Oral health shares common risk factors with major chronic diseases, such as heart disease, diabetes, and cancer (Hegde and Haddock 2019). Despite these shared risk factors and clinical markers, there are significant policy differences between oral and general health care, largely due to differing funding mechanisms. These structural differences appear to influence how value-based approaches are adopted and implemented within oral health settings.
The VBOHC approach aims to address persistent challenges, such as high treatment costs, unequal access to care, and inconsistent patient outcomes (Hegde and Haddock 2019). Preventive care and risk assessment are also integral to VBOHC, as they help identify potential oral health issues before they escalate, thereby reducing the need for costly interventions (Martin et al 2020).
The purpose of this scoping review is to explore the current landscape of VBOHC, examining key components, implementation strategies, and impacts on patients and health care providers.
Although several studies have examined individual components of value-based health care within dentistry, there are no existing narrative, scoping, or systematic reviews that specifically synthesise evidence on VBOHC. By reviewing existing literature, this study aims to identify the benefits and challenges associated with VBOHC, highlight gaps in current research, and propose directions for future investigation.
Methods
The methodology for this scoping review was developed following guidelines provided by the Joanna Briggs Institute and PRISMA-ScR checklist (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews). The protocol for this scoping review was registered with the Open Science Framework (ID h3vg5).
The population of the study included dental health care providers and patients, which allowed for a holistic view of value-based care, incorporating the perspectives of those delivering and receiving care.
The concept of interest in this review is the characteristics of VBOHC, such as the values of different stakeholders of key strategies and measures. Focusing on these key characteristics aligns with the core principles of value-based care.
The context covers any general dental health care setting, inclusive of the public, private, and academic sectors.
Eligibility of the studies included any primary, secondary, or grey literature that provided insights into the concept of value-based dental health care. This inclusivity of grey literature was necessary to ensure a comprehensive understanding of the topic, given the relatively limited amount of research available, and was subsequently not subjected to quality assessment.
Additional eligibility criteria included limiting the review to English-language publications and studies published within the last 20 y.
Database Searches
A 3-step search strategy was employed in this review.
The first step involved conducting an initial limited search of the Ovid MEDLINE database. This search allowed the review team to refine the strategy for subsequent searches. In the second step, the review team conducted a more extensive search across multiple databases using the keywords and index terms identified in the initial search.
MeSH terms included “value-based health care,” “oral health,” “dental care,” and “dentistry.”
Additional index terms used for further insurance of data collection were “value based care,” “value-based healthcare,” “value based health care,” “value based model,” “value based framework,” value based system,” and “dental health.”
The databases searched included Ovid MEDLINE, EBSCOhost, the Cochrane Library, CINAHL, and the Joanna Briggs Institute Evidence-Based Practice Database. The search strategies used for each database are detailed in the appendices of this report. These databases were selected because they are widely used in health care research and are known to include a broad range of literature relevant to the topic of value-based care. These searches were completed by 19 June 2025.
These database searches were conducted alongside the search for grey literature within Google Scholar. Specific search terms related to value-based health care and dentistry were input and reviewed up to 10 pages.
Selection Process and Data Extraction
Data screening was done by 2 researchers (R.B. and H.K.) for titles/abstracts and full text in pairs.
The first stage of screening involved a single reviewer examining the titles and abstracts of all studies identified in the search to assess their eligibility against the inclusion criteria. Studies that clearly did not meet the inclusion criteria were excluded at this stage. The remaining studies were then subjected to a full-text review, which was conducted by 2 reviewers.
Any disagreements between the reviewers during screening or data extraction were resolved through discussion. If consensus could not be reached, a third reviewer was consulted to make the final decision.
The data extraction tool was created under the guidance of the Joanna Briggs Institute’s reviewer manual regarding key information for extraction. Data extraction was conducted with a standardised form to capture author, country, value-based health care model, funding, delivery models, and outcomes (Appendix 6).
The VBOHC model was documented if used and categorised according to how each study defined or conceptualised VBOHC.
Funding models were classified according to the payment mechanisms described and measured by documenting the specific reimbursement structure used, such as FFS, shared savings programs, value-based purchasing, global budgeting, bundled care budget, and other.
Delivery models were categorised by the model of care, such as primary care, hospital or agency, tele- or videoconference, and other.
Outcomes were recorded for provider/organisation, health care professional, and patient via a narrative synthesis approach examining the quality impact and the cost impact.
Changes Made to the Protocol
The original protocol for this scoping review included all dental health care settings. However, during the initial stages of the research, it became evident that areas such as oral and maxillofacial surgery, as well as cosmetic dentistry, were too broad and outside the primary focus of this review. As a result, the scope was refined to concentrate on general dentistry health care settings.
Results
Selection Process
The database search for this scoping review retrieved 185 studies: 134 from peer-reviewed literature and 51 from grey literature (Fig. 1).
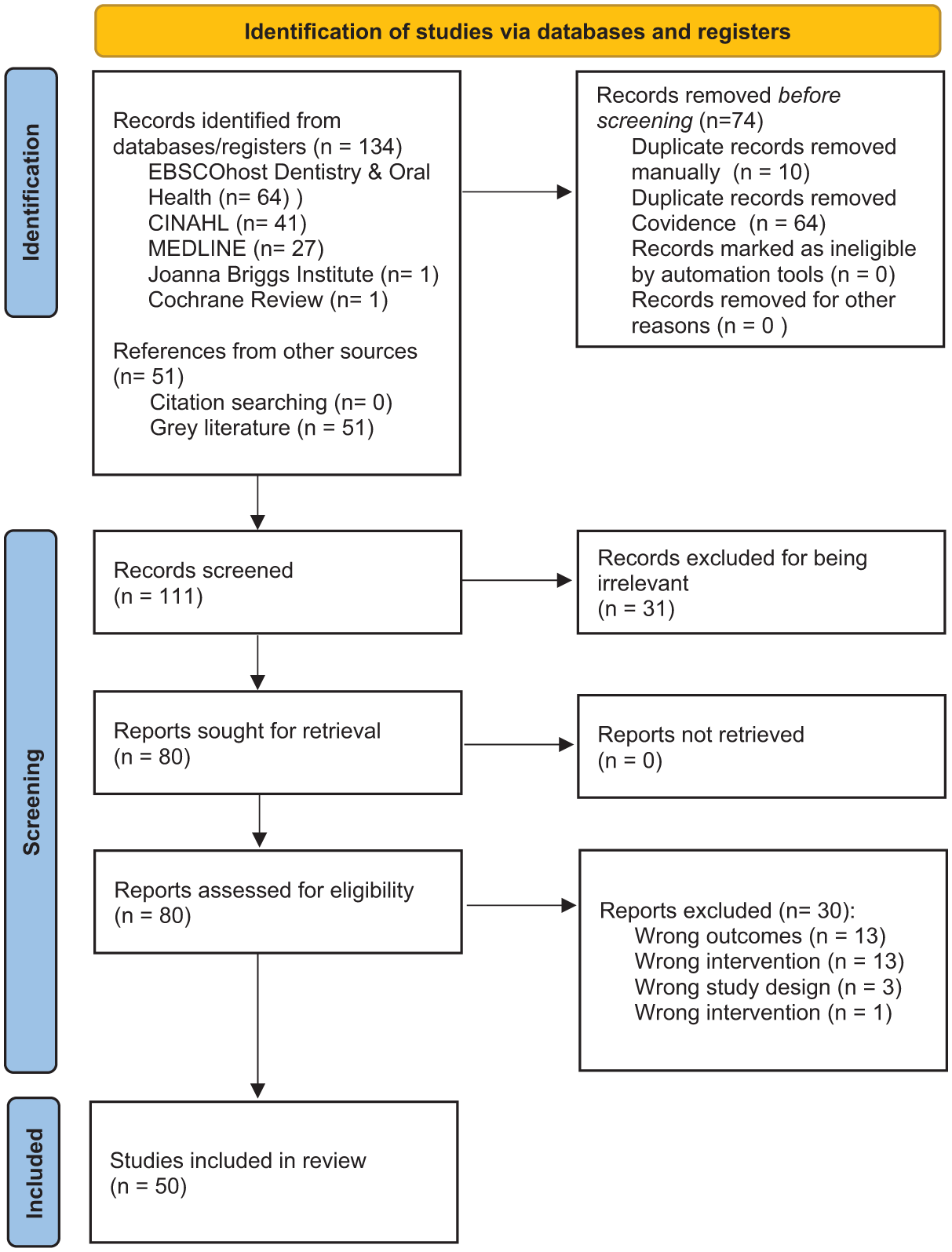
PRISMA-ScR diagram flowchart illustrating the process of study selection.
After removal of 74 duplicates, 111 records underwent title and abstract screening. Of the screened articles, all of those that did not demonstrate compliance to the eligibility criteria were excluded, resulting in 61 exclusions based on relevance (31), outcomes (13), interventions (13), study design (3), or patient population (1).
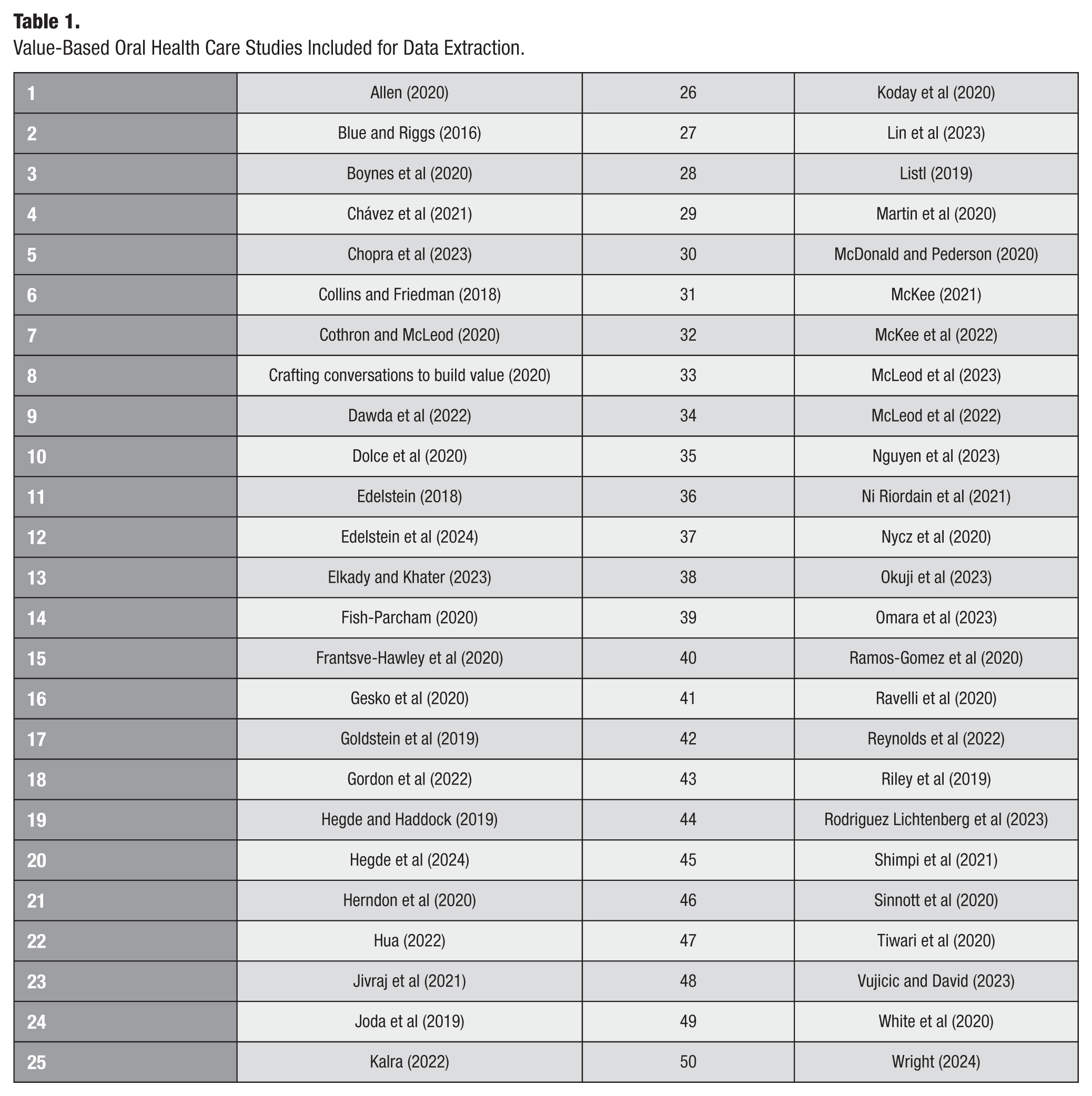
In total, 50 studies met all inclusion criteria and were carried forward for data extraction (Table 1).
Value-Based Oral Health Care Studies Included for Data Extraction.
Study Characteristics
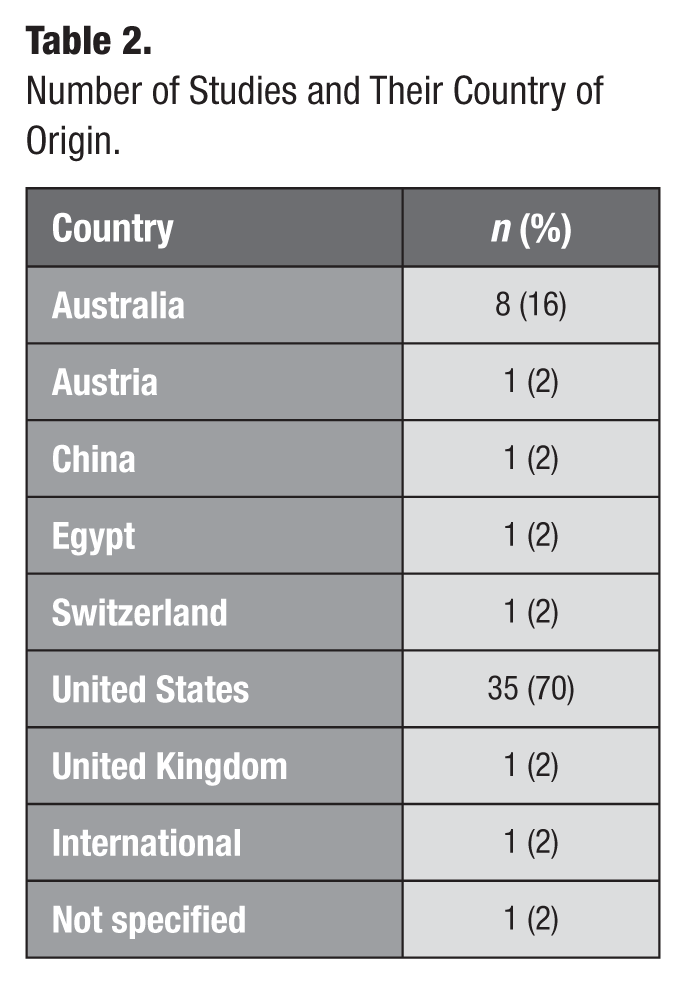
All studies that reported the location of their project (Table 2) were conducted in developed countries (n = 49). The study by Ni Riordain et al (2021) was conducted internationally as a collaboration. Overall, 88% of studies originated from English-dominant countries.
Number of Studies and Their Country of Origin.
Study Design
A diverse range of study designs was included in the body of research, reflecting the multifaceted approaches taken to explore various aspects of the topic (Fig. 2). Some studies reported multiple models, funding mechanisms, delivery approaches, or outcomes; therefore, a single study could be included in >1 category.
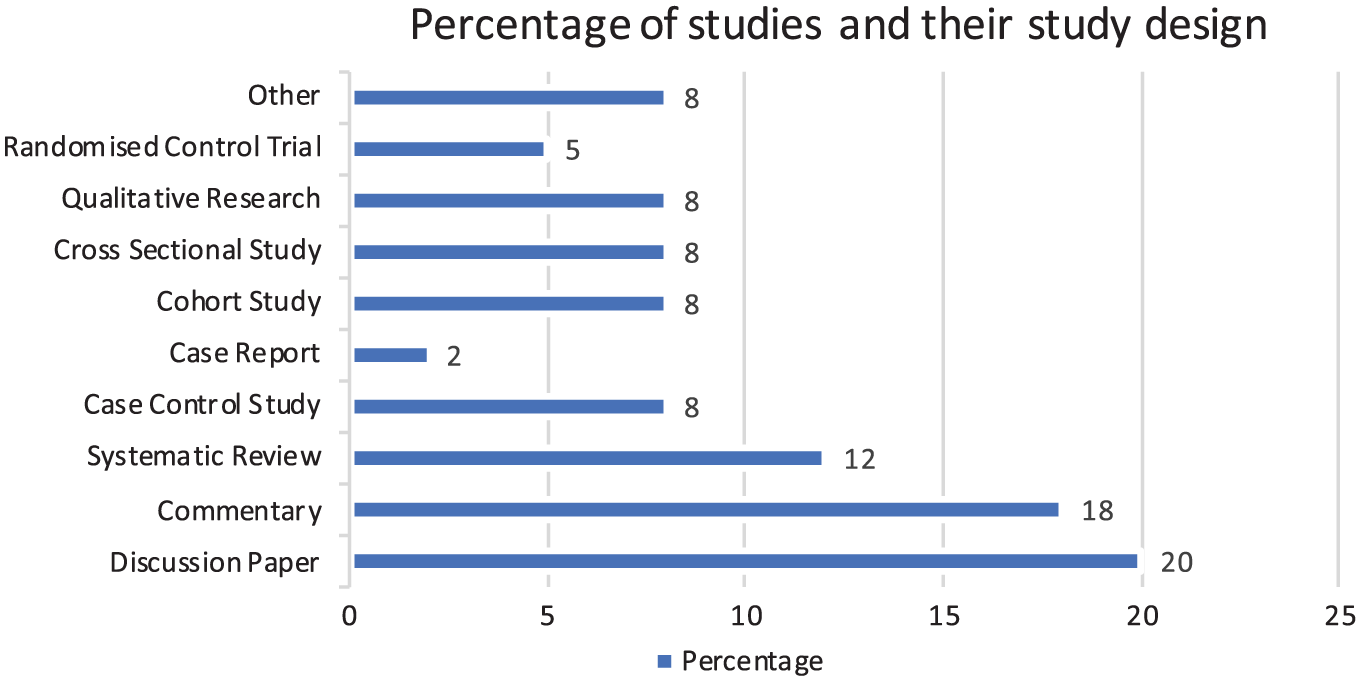
Percentage of studies and their study design.
Discussion articles and commentaries were used frequently, with 40% of studies employing this methodology. Systematic reviews accounted for 12%, whereas case-control studies, cohort studies, and cross-sectional studies accounted for 8% each.
Additionally, qualitative research was used in 4 studies (8%) to explore patient and provider perspectives.
Study Interventions Implemented
The various studies in this body of work had distinct interventions, varying in how they focused on transforming traditional dental care through VBOHC. While these studies shared the common goal of enhancing patient outcomes and optimising costs, their focuses and methodologies differed, reflecting the diverse nature of challenges in the field of dentistry. A variety of interventions were implemented, targeting key areas such as prevention, patient-centred care, and the integration of technology to enhance care delivery and efficiency.
VBOHC Framework
The introduction of a codesigned VBOHC framework was central to almost half of the interventions (Collins and Friedman 2018; Edelstein 2018; Hegde and Haddock 2019; Joda et al 2019; Boynes et al 2020; Herndon et al 2020; White et al 2020; McKee 2021; Gordon et al 2022; McKee et al 2022; Chopra et al 2023; Lin et al 2023; Nguyen et al 2023). The frameworks emphasised improving patient-centred care and driving better health outcomes through a multidisciplinary approach. The use of patient-reported outcome measures (PROMs) and patient-reported experience measures were integral to the process for 12% of the studies (Listl 2019; Ni Riordain et al 2021; Hua 2022; Reynolds et al 2022; Omara et al 2023). This patient-centred approach allowed for a more tailored care model, with feedback loops ensuring that the services provided aligned with what mattered most to patients. As a result, patient satisfaction and health outcomes improved. PROMs and patient-reported experience measures highlighted significant gains in patient-reported oral health quality of life, especially in terms of functional and aesthetic outcomes.
A key aspect within the VBOHC framework was the transition to value-based payment models. A significant intervention, present in 20% of the studies, was the shift from FFS models to value-based payment systems (Blue and Riggs 2016; Collins and Friedman 2018; Edelstein 2018; Hegde and Haddock 2019; Riley et al 2019; Boynes et al 2020; Nycz et al 2020; Dawda et al 2022; Gordon et al 2022; Vujicic and David 2023). These models incentivised dental providers to prioritise prevention, interdisciplinary collaboration, and improved patient outcomes. The study revealed that value-based payment models not only enhanced the quality of care but also fostered a more cost-effective system, particularly by reducing the frequency of unnecessary procedures. Dental practitioners, motivated by the outcomes-based payment structure, were more inclined to adopt preventive practices and focus on long-term health improvements.
Preventive and Minimally Invasive Care
Another key intervention was the implementation of, or focus on, preventive and minimally invasive dentistry frameworks, which focused on early disease detection and management. Minimally invasive dentistry was a central theme in >50% of the studies (Blue and Riggs 2016; Edelstein 2018; Riley et al 2019; Allen 2020; Boynes et al 2020; Dolce et al 2020; Fish-Parcham 2020; Gesko et al 2020; Herndon et al 2020; McDonald and Pedersen 2020; Nycz et al 2020; Ramos-Gomez et al 2020; Sinnott et al 2020; Tiwari et al 2020; Chávez et al 2021; Dawda et al 2022; Gordon et al 2022; Kalra 2022; McLeod et al 2022; Chopra et al 2023; Lin et al 2023; McLeod et al 2023; Nguyen et al 2023; Vujicic and David 2023; Wright 2024). Through this intervention, dental care shifted from a reactive model to a more proactive approach that emphasised risk stratification and personalised prevention plans. Preventive treatments such as sealants and fluoride applications were prioritised, and the results indicated a notable reduction in the incidence of caries and periodontal disease among participants. The integration of these models into daily dental practices not only enhanced the overall health outcomes but also reduced the need for complex and costly treatments.
Patient-Clinician Collaboration
The development of a standardised set of patient-centred outcomes, particularly the Adult Oral Health Status Set, aimed to enhance value-based care by aligning clinical outcomes with patient priorities. The integration of the Oral Health Impact Profile into clinical care facilitated the collection of PROMs in 14% of the studies (Herndon et al 2020; McKee 2021; Ni Riordain et al 2021; Hua 2022; Lin et al 2023; Omara et al 2023; Wright 2024).
In the review, 12% of the studies encompassed the implementation of shared decision-making (SDM) frameworks that allowed patients to actively participate in their treatment choices (Allen 2020; Crafting conversations to build value 2020; Cothron and McLeod 2020; Jivraj et al 2021). This intervention was particularly effective in aligning care with the informed preferences and values of patients, which led to higher satisfaction and better adherence to treatment plans. The use of SDM, supported by clear communication strategies from dental teams, empowered patients to make decisions that balanced clinical evidence with their personal preferences, thereby enhancing the patient experience.
Digital Dentistry
Multiple studies included content regarding digital dentistry (Blue and Riggs 2016; Joda et al 2019; Cothron and McLeod 2020; Nycz et al 2020; Gordon et al 2022; McKee et al 2022). One of the interventions involved the development and implementation of a user-friendly teledentistry platform (McKee et al 2022). This platform aimed to provide remote access to oral health care, particularly focusing on simplicity and inclusivity for patients with low digital literacy. The platform supported virtual consultations for preventive care and early disease management. Teledentistry reduced geographic barriers to access and minimised the need for in-person visits, which was especially beneficial in underserved areas. The intervention yielded positive results in terms of patient engagement and satisfaction. Patients reported ease of use, and there was an observed increase in the early detection of oral health issues.
Common Barriers
The studies highlighted several recurring barriers to the successful implementation of VBOHC models and related interventions in dental and broader health care systems (Table 3). A consistent challenge across 80% of studies was the entrenchment of FFS models, as seen in the breakdown of barriers to specific studies in Appendix 7. This traditional payment structure is misaligned with VBOHC principles, creating significant resistance to transitioning toward outcome-based care. Many private health care providers, across 22% of studies, accustomed to the financial incentives of FFS, expressed reluctance to adopt new models that link compensation to patient outcomes, citing concerns over financial risks and potential disruptions to established workflows (Blue and Riggs 2016; Collins and Friedman 2018; Goldstein et al 2019; Cothron and McLeod 2020; Dolce et al 2020; Koday et al 2020; Nycz et al 2020; Sinnott et al 2020; Chávez et al 2021; Jivraj et al 2021; Gordon et al 2022; McLeod et al 2023; Edelstein et al 2024).
Barriers and Facilitators of Implementing Value-Based Oral Health Care.
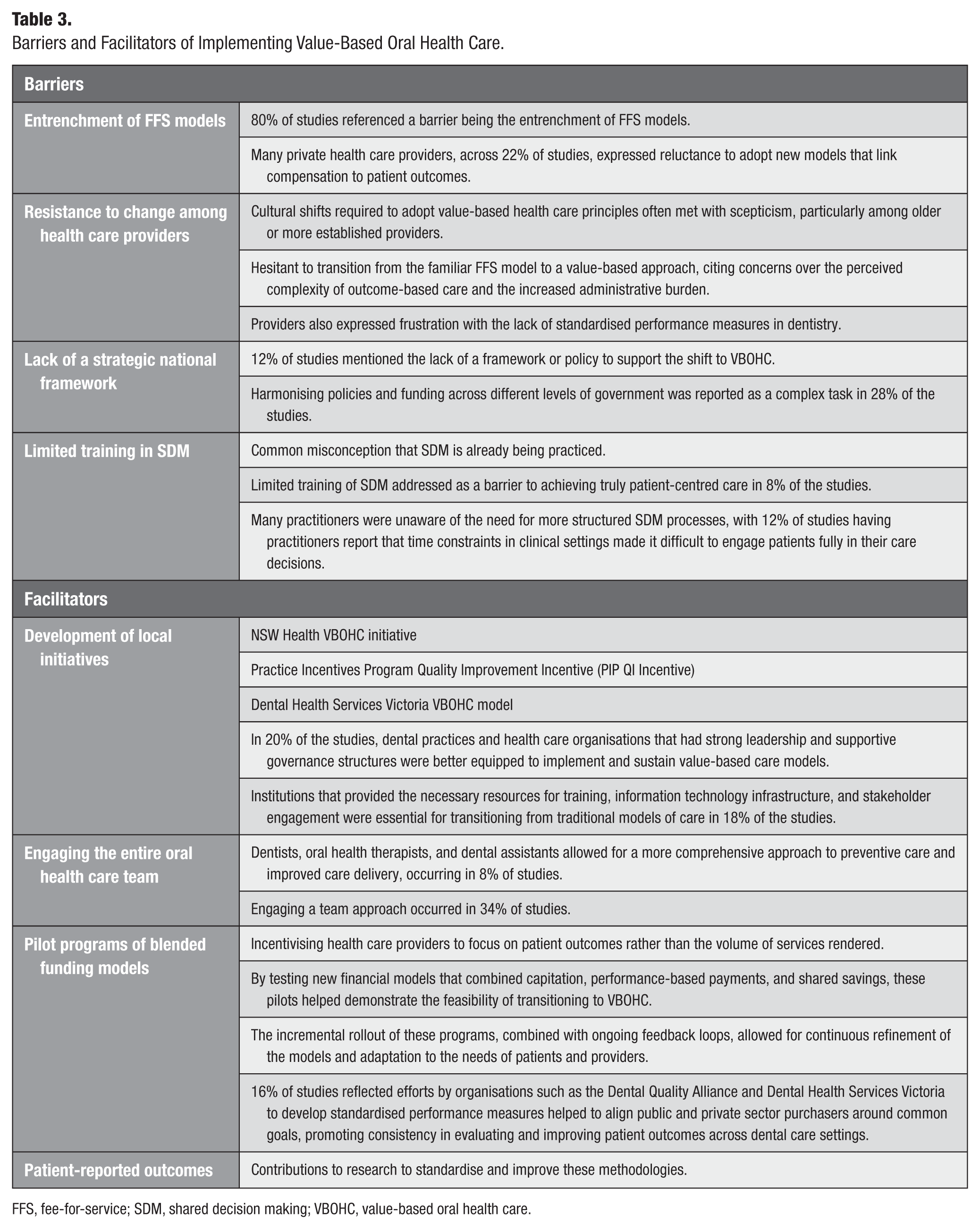
FFS, fee-for-service; SDM, shared decision making; VBOHC, value-based oral health care.
Resistance to change among health care providers was another common theme. Cultural shifts required to adopt value-based health care principles often met with scepticism, particularly among older or more established providers. Many studies noted that dental practitioners, for example, were hesitant to transition from the familiar FFS model to a value-based approach, citing concerns over the perceived complexity of outcome-based care and the increased administrative burden (Blue and Riggs 2016; Collins and Friedman 2018; Goldstein et al 2019; Cothron and McLeod 2020; Koday et al 2020; Nycz et al 2020; Sinnott et al 2020; Jivraj et al 2021; Gordon et al 2022; McLeod et al 2023; Edelstein et al 2024). Providers also expressed frustration with the lack of standardised performance measures in dentistry, which makes it difficult to evaluate success and ensure consistency across practices.
Another pervasive barrier identified was the lack of a strategic national framework supporting the shift to VBOHC, as mentioned in 12% of studies (Hegde and Haddock 2019; Dolce et al 2020; Martin et al 2020; Dawda et al 2022; Okuji et al 2023; Hegde et al 2024). The absence of cohesive nationwide policies to guide and incentivise VBOHC adoption complicates efforts at the local, state, and federal levels. Harmonising policies and funding across different levels of government was reported as a complex task in 28% of the studies (Blue and Riggs 2016; Edelstein 2018; Hegde and Haddock 2019; Listl 2019; Dolce et al 2020; Fish-Parcham 2020; Chávez et al 2021; Dawda et al 2022; Kalra 2022; McKee et al 2022; Chopra et al 2023; Nguyen et al 2023; Vujicic and David 2023; Hegde et al 2024). Without a unified strategy, providers are left navigating a fragmented system, limiting the scalability and sustainability of value-based health care initiatives.
Furthermore, limited training in SDM and the misconception that SDM is already being practiced were highlighted as barriers to achieving truly patient-centred care in 8% of the studies (Allen 2020; Boynes et al 2020; Crafting conversations to build value 2020; Tiwari et al 2020). Many practitioners were unaware of the need for more structured SDM processes, with 12% of studies having practitioners report that time constraints in clinical settings made it difficult to engage patients fully in their care decisions (Joda et al 2019; Allen 2020; Dolce et al 2020; Elkady and Khater 2023; McLeod et al 2023; Edelstein et al 2024).
Common Facilitators
The studies highlighted several key facilitators that enabled the successful implementation of VBOHC models and innovations in dental care (Table 3). These facilitators helped overcome barriers such as entrenched FFS models, limited data infrastructure, and resistance to change, ultimately supporting the transition to patient-centred, outcome-focused care.
One of the most important facilitators identified was the development of local initiatives, such as the NSW Health VBOHC initiative, collaborative commissioning, Dental Health Services Victoria VBOHC, and the Practice Incentives Program Quality Improvement Incentive (PIP QI Incentive) (Hegde and Haddock 2019; McKee 2021; Nguyen et al 2023). These initiatives promoted the adoption of VBOHC by encouraging regional collaboration and providing targeted funding and incentives for health care providers.
In 20% of the studies, dental practices and health care organisations that had strong leadership and supportive governance structures were better equipped to implement and sustain value-based care models (Joda et al 2019; Allen 2020; Crafting conversations to build value 2020; Dolce et al 2020; Gesko et al 2020; White et al 2020; Chávez et al 2021; Elkady and Khater 2023; Omara et al 2023; Edelstein et al 2024). These institutions provided the necessary resources for training, information technology infrastructure, and stakeholder engagement, which were essential for transitioning from traditional models of care in 18% of the studies (Collins and Friedman 2018; Joda et al 2019; Cothron and McLeod 2020; Koday et al 2020; Martin et al 2020; Tiwari et al 2020; Dawda et al 2022; Omara et al 2023; Edelstein et al 2024). In particular, engaging the entire oral health care team, including dentists, oral health therapists, and dental assistants, allowed for a more comprehensive approach to preventive care and improved care delivery, occurring in 8% of studies (Blue and Riggs 2016; Dolce et al 2020; Lin et al 2023; McLeod et al 2023).
Another critical facilitator was the introduction of blended funding models through pilot programs, occurring in 34% of studies (Collins and Friedman 2018; Edelstein 2018; Hegde and Haddock 2019; Goldstein et al 2019; Riley et al 2019; Dolce et al 2020; Herndon et al 2020; McDonald and Pedersen 2020; Sinnott et al 2020; Jivraj et al 2021; McKee 2021; Dawda et al 2022; McLeod et al 2022; McLeod et al 2023; Rodriguez Lichtenberg et al 2023; Vujicic and David 2023; Hegde et al 2024). These models provided an alternative to traditional FFS payment structures, incentivising health care providers to focus on patient outcomes rather than the volume of services rendered. By testing new financial models that combined capitation, performance-based payments, and shared savings, these pilots helped demonstrate the feasibility of transitioning to VBOHC. The incremental rollout of these programs, combined with ongoing feedback loops, allowed for continuous refinement of the models and adaptation to the needs of patients and providers.
Finally, growing awareness of the importance of patient-reported outcomes and the contributions of research to standardise and improve these methodologies were key facilitators in driving VBOHC forward. An overall 16% of studies reflected efforts by organisations such as the Dental Quality Alliance and Dental Health Services Victoria to develop standardised performance measures to help align public and private sector purchasers around common goals, promoting consistency in evaluating and improving patient outcomes across dental care settings (Edelstein 2018; Herndon et al 2020; McKee 2021; Kalra 2022; McKee et al 2022; Nguyen et al 2023; Lin et al 2023; Hegde et al 2024).
Discussion
The key question guiding this review—“What are the characteristics of VBOHC?”—has been explored through various perspectives, including patient outcomes, provider practices, and the broader health care system. VBOHC prioritises prevention, early intervention, and patient-centered outcomes, in contrast to the reactive volume-driven FFS model. It emphasises routine screenings, fluoride treatments, and education to reduce severe dental issues and costly procedures. VBOHC supports SDM and promotes better health equity, especially for underserved populations. For providers, it offers cost savings through bundled payments and coordinated care. However, it also requires system adjustments, staff retraining, and overcoming resistance to change.
While VBOHC shares core principles with general value-based health care, such as outcome focus and care coordination, it faces distinct challenges. Access to dental care tends to be more inconsistent and inequitable, especially for low-income or rural populations. Unlike general health care, dental services frequently lack established pathways for integrating preventive approaches or collaborating across disciplines. These structural challenges make the shift to VBOHC more complex and demand targeted strategies tailored to the dental sector.
To advance VBOHC, targeted policy and operational actions are needed. These include increasing investment in preventive dental care, supporting workforce development to enable team-based models, and aligning oral health services with general health care systems. Standardising outcome measures and expanding the use of digital tools such as teledentistry and PROMs will enhance quality and access. Policies should focus on equity and sustainability, especially for high-need populations.
Current research on VBOHC is limited in scope and duration. There is a lack of long-term studies on clinical and economic outcomes, as well as insufficient comparative analyses across different populations and care settings.
The current literature has been biased toward high-income countries. Key gaps include evaluating the cost-effectiveness of VBOHC models, understanding the scalability of pilot programs, and capturing patient experiences more systematically. More rigorous large-scale studies are needed to guide policy and practice, particularly across diverse settings.
In addition, this scoping review itself is limited by the breadth and variability of available terminology. Much of the available evidence is qualitative, with inconsistent definitions of “value,” making comparisons across models challenging. The reliance on published English-language literature may also have introduced bias by excluding models implemented or evaluated in non-English-speaking contexts, subsequently also limiting studies from low- and middle-income countries.
This raises concern for how applicable these findings would be in broader geographic areas, and future research should consider how VBOHC principles can be adapted to local cultural norms, health system structures, and patient preferences. This should include structured examinations of VBOHC models in low- and middle-income countries, including evaluations within differing financing arrangements, workforce capacities, and care delivery infrastructures.
Conclusion
VBOHC is characterised by patient empowerment and a patient-centred whole system approach, enabling better coordination across health conditions and the care spectrum. These characteristics distinguish VBOHC from traditional FFS models by promoting a more holistic, efficient, and patient-focused approach to care. However, successful implementation requires addressing the challenges associated with transitioning from the FFS model, particularly through provider support, infrastructure investments, and policy reforms.
Author Contributions
R. Bentley: contributed to acquisition, analysis, and interpretation, drafted and critically revised the manuscript; C. Liu: contributed to analysis and interpretation, critically revised the manuscript; H. Khalil: contributed to conception and design, data acquisition, analysis, and interpretation, critically revised the manuscript. All authors gave their final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jct-10.1177_23800844261435909 – Supplemental material for Characteristics of Value-Based Oral Health Care: A Scoping Review
Supplemental material, sj-docx-1-jct-10.1177_23800844261435909 for Characteristics of Value-Based Oral Health Care: A Scoping Review by R. Bentley, C. Liu and H. Khalil in JDR Clinical & Translational Research
Supplemental Material
sj-pdf-2-jct-10.1177_23800844261435909 – Supplemental material for Characteristics of Value-Based Oral Health Care: A Scoping Review
Supplemental material, sj-pdf-2-jct-10.1177_23800844261435909 for Characteristics of Value-Based Oral Health Care: A Scoping Review by R. Bentley, C. Liu and H. Khalil in JDR Clinical & Translational Research
Footnotes
Author Note
The authors declare that no generative artificial intelligence was used in the creation of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
This scoping review did not generate primary research data. All data analysed in this study were derived from publicly available, peer-reviewed, and grey literature sources, which are cited in the reference list. No new datasets were created or deposited in a public repository.
A supplemental appendix to this article is available online.