
Abstract
Objective:
Professionalism is essential in dental education, yet limited research has examined the barriers and challenges dentists face and how these affect their professional identity. This study addressed this gap by exploring dentists’ perceptions of professionalism, identifying workplace challenges, analyzing contributors to their professional identity development, and gathering recommendations to enhance professionalism education within dental education.
Methods:
A purposive sample of practicing dentists was recruited in the Metro Vancouver area of Canada. Semi-structured interviews were conducted using a piloted interview guide. These interviews, held via Zoom, were analyzed using template analysis in NVivo (version 14) by QSR International.
Results:
Ten dentists participated in the study. They identified patient-centered care, effective communication, adherence to ethical standards, and maintaining boundaries as key aspects of professionalism. While work experience reinforced professional identity, findings suggest a possible disconnect between professional identity formation and ethical behavior, emphasizing the need for deliberate and guided self-reflection. Participants also reported insufficient training in ethics and interprofessional collaboration, highlighting gaps between their understanding of professionalism and the education they received. They recommended improved professionalism training, stricter institutional oversight, and better workplace dynamics to support ethical decision-making.
Conclusions:
This study emphasizes the need for a strategic approach to foster professionalism in dental education, including enhanced professionalism training, promoting professional behavior in dental practice, and potentially revising licensing and oversight frameworks. Future research could examine broader contextual effects, such as regional or cultural influence on professional identity, to develop a more holistic understanding of professionalism in dentistry. These insights can inform dental educators in refining curricula to ensure that dentists provide patient care that adheres to the highest ethical and caring standards.
Knowledge Transfer Statement:
This study explores how practicing dentists in Canada understand professionalism and form their professional identities, revealing gaps in ethics training, interprofessional collaboration, and workplace support. It highlights a gap in improved professionalism education and institutional oversight. Dental educators, regulators, and policymakers can use these insights to revise dental curricula, ensuring that future dentists are better equipped to navigate ethical challenges and deliver patient-centered care grounded in strong professional values.
Keywords
Introduction
Dentistry is a profession with health-service obligations to the public (Ozar and Sokol 2002). The value of dental care extends beyond individual perceptions, as it plays an important role in people’s overall well-being. Since oral health directly affects patients’ ability to maintain both their physical and mental health, dentists must prioritize patients’ oral health over advancing their own interests (Ozar et al. 2018). Thus, professionalism is a cornerstone of dental practice, influencing both the quality of patient care and the profession’s reputation (ADEA Statement on Professionalism in Dental Education 2017; Welie 2004). Accrediting bodies recognize it as essential and mandate its inclusion in the dental education curricula (Curriculum Guidelines on Ethics and Professionalism in Dentistry 1989). In North America, the American and Canadian Dental Associations emphasize professionalism through statements outlining core values such as competence, fairness, accountability, integrity, respect, and so forth, which serve as guidelines for dental practitioners (ADEA Statement on Professionalism in Dental Education 2017; Canadian Dental Association [date unknown]).
While dental educators acknowledge the importance of professionalism, they often struggle to effectively “teach” it. Although professionalism encompasses more than just ethical practice, most of the professionalism education in dental schools has traditionally focused on ethics and ethical reasoning. Nearly 2 decades ago, Bertolami (2004) critiqued the dental ethics curricula, arguing that the traditional ethics courses were only teaching about ethics rather than instilling ethics in a way that would foster positive change in behavior. He emphasized the need for introspection and personalization in ethics education, suggesting that curricula should help students reflect on their core beliefs and better understand themselves—“who they really are, what they really want, and what they really believe and why” (p. 418).
When dentists face high overhead costs and intense competition in a saturated market, professionalism can be jeopardized. This highlights the need for more discussions on revitalizing professionalism in dentistry. While some studies explore students’ or the public’s perspectives on professionalism, there is a notable lack of research focused on dentists’ own views (Ashar and Ahmad 2014; Franzén 2020; Holden et al. 2022; Cunningham et al. 2024). Our rapid scan of the literature indicates a scarcity of studies on how real-world barriers and challenges shape dentists’ professional identity. This study addresses this gap by examining multiple dimensions of professionalism from practicing dentists’ perspectives, including both their views and the factors influencing their evolving professional identity. By understanding dentists’ real-world experiences, this study provides valuable insights into the obstacles they face when making ethical decisions in their practice. These findings can guide educators in making informed adjustments to dental curricula.
Therefore, this study aimed to understand Canadian dentists’ perspectives on professionalism, explore workplace barriers and challenges that affect their professional identity and conduct, identify factors shaping their evolving professional identity, and gather their recommendations for strengthening dental professionalism.
Method
Research Paradigm
This research is grounded in a constructivist philosophical paradigm, which emphasizes the active role of individuals in shaping their understanding of the world through personal experiences and social interactions (Creswell and Creswell 2018). Professional identity formation (PIF) is inherently subjective, shaped by complex, socially embedded processes, while professionalism develops through socialization, mentorship, and practice (Cruess et al. 2019). The constructivist perspective is appropriate for exploring how practitioners interpret and internalize professionalism in dentistry, recognizing that knowledge and identity are co-constructed through social interactions and institutional frameworks.
Researcher Characteristics, Reflexivity, and Trustworthiness
The first author (J.H.K.) is a registered dental hygienist with clinical and teaching experience in dental education. This background facilitated rapport with participants and an in-depth understanding of the professional context. However, the insider perspective also required ongoing reflexivity to guard against assumptions and bias. Memo writing and supervisory discussions with H.v.B. were used to ensure critical self-awareness throughout the research process. The second author (H.v.B.) is not a dental clinician but has more than a decade of experience in dental education. Her outsider perspective provided valuable critical distance and helped challenge clinical assumptions, contributing to analytic rigor. This interdisciplinary collaboration balanced professional insight with educational critique, shaping the study’s approach and interpretation.
To further enhance the trustworthiness of this qualitative study, several strategies were used in alignment with Lincoln and Guba’s (1985) criteria for establishing rigor. Prolonged engagement was achieved through in-depth interactions with the data, enabling the researcher to develop a comprehensive understanding of participants’ experiences and the contextual nuances of dental practice (Lincoln and Guba 1985). Member checking was conducted by sharing preliminary themes and interpretations to confirm the accuracy and resonance of the findings with their lived experiences (Lincoln and Guba 1985).
To address dependability, a code–recode strategy was used. Selected segments of transcripts were reanalyzed at different points in time and compared to assess consistency in coding and thematic development. Collectively, these strategies contributed to the credibility and dependability of the findings, reinforcing the trustworthiness of the study’s interpretations.
Study Design, Participants, and Development of Interview Questions
This qualitative study used semi-structured interviews for data collection and template analysis (TA) for data analysis. Each participant completed a 1-h interview. The development of the interview questions was informed by a review of the literature on professionalism and PIF in dentistry and the broader health professions. In addition, insights gained from a previous qualitative study with dental students contributed to the refinement of the interview guide (Kwon et al. 2022). That earlier research explored students’ perceptions of professionalism, their professional identity development, and their views on the effectiveness of professionalism education. Themes from that study—such as students’ motivations for entering the profession, their concerns about professional role expectations, the most important qualities they attribute to a dentist, and their recommendations for improving professionalism education within their program—helped shape the current interview guide. These questions were designed to explore how practicing dentists reflect on their own professional development, the factors that influence their evolving professional identity, and the extent to which their experiences in practice align or diverge from the ideals introduced during their dental education. The guide also sought to elicit dentists’ perspectives on improving professionalism education in dental programs, providing continuity from earlier work with students to insights from clinical practitioners.
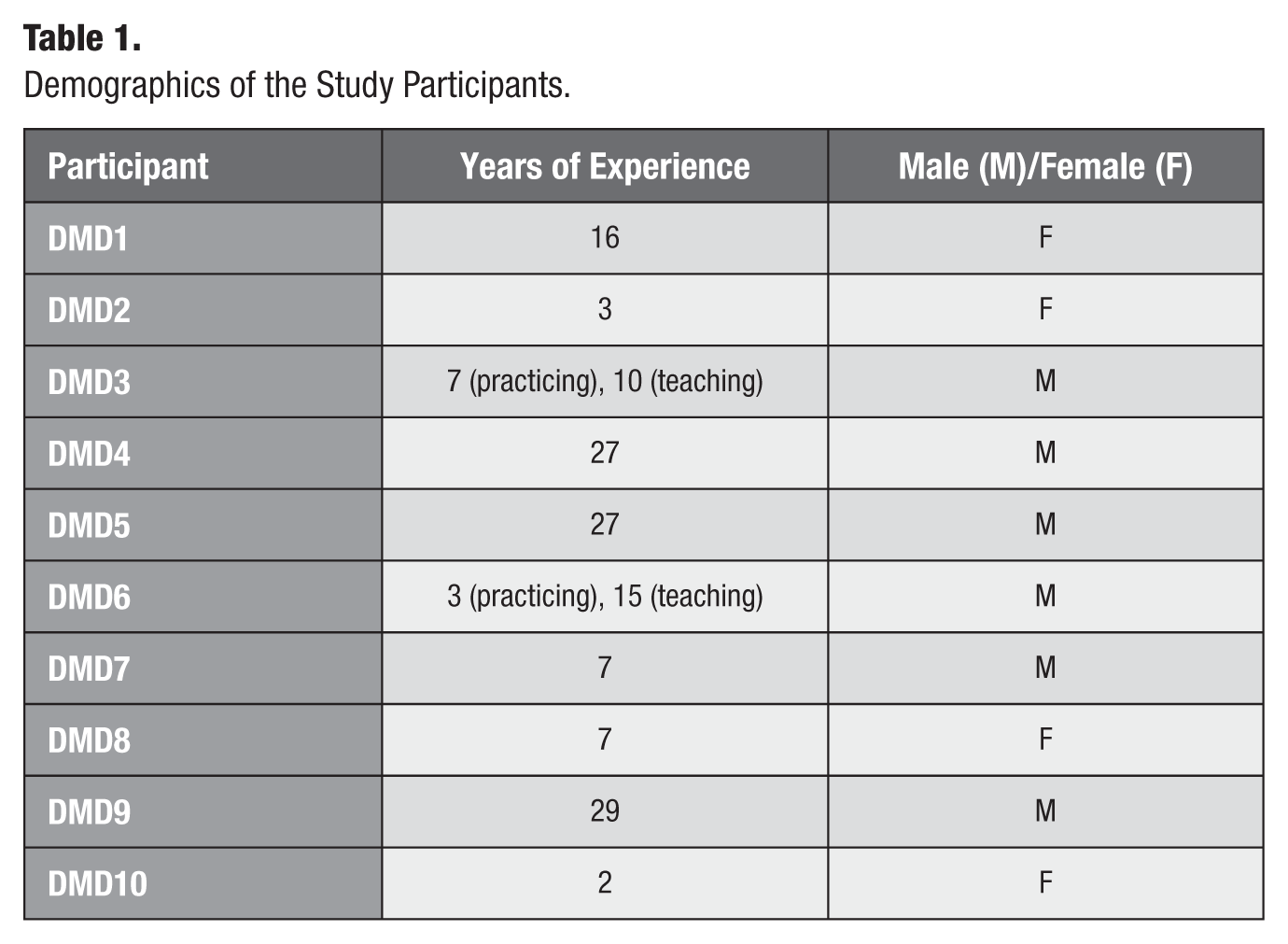
The inclusion criteria required participants to be fluent in English and to have completed the Doctor of Dental Medicine program in Canada. Purposive sampling was used to target the desired population. Recruitment advertisements were posted on a Facebook group page dedicated to dental professionals in Vancouver, British Columbia, from December 1, 2021, to December 31, 2021. Interested dentists contacted the researcher (J.H.K.) directly, after which eligibility was confirmed against the inclusion criteria. Between January 1, 2022, and March 1, 2022, participants were selected to represent a range of demographic and professional characteristics, including differences in age, gender, years of practice, and practice settings (see Table 1). Each participant was compensated with a $25 coffee gift card for participation. Consistent with qualitative research conventions, the sample size was determined by data saturation when no new themes were emerging from the data, suggesting sufficient depth had been reached to address the study objectives (Morse 2015; Creswell and Creswell 2018).
Demographics of the Study Participants.
Ethics Approval
This study was approved by the University of British Columbia (ethics approval No. H21-03350).
Data Collection, Consent, and Data Processing
Before each interview, the researcher explained the process, privacy concerns, and anonymization procedure. Participants signed a written consent form and emailed it back to the researcher before interviews were conducted via Zoom. Only audio was recorded. At the start, the researcher (J.H.K.) reiterated the procedure, and participants gave a verbal agreement to proceed.
The audio recordings were transcribed with the help of online transcription software (Otter.ai), and the researcher (J.H.K.) manually corrected any transcription errors, replacing names with numerical codes to ensure anonymity. The original audio files and transcript versions containing identifiable information were deleted after verification, with only the anonymized transcripts retained for analysis. The transcripts were then imported into NVivo (version 14). Data collection and analysis, conducted from January to March 2022, concluded with 10 transcripts once data saturation was reached.
Data Analysis
Template analysis
To analyze the data, TA as described by King was used (King 2004; King and Brooks 2017). TA is a form of thematic analysis that emphasizes the use of hierarchical coding while allowing for flexibility to meet the specific needs of a study (King and Brooks 2017). It can be applied to any textual data, such as interview transcripts, diary entries, focus groups, and questionnaire responses (King 2004). The technique involves creating a coding “template” (a priori themes) based on a subset of data, which is then applied to the rest of the data and refined as needed (King 2004). Unlike other thematic approaches, TA does not dictate a predetermined sequence of coding levels. Instead, it encourages the researchers to thoroughly develop themes where the data are the richest, specifically in areas where the research questions are being addressed (Lockett et al. 2012).
Philosophical position of this TA
One advantage of TA is its flexibility in accommodating diverse philosophical perspectives, ranging from realism to radical constructivism, rather than being bound to a single epistemology. Realism is similar to positivist approaches in quantitative research, which seeks to uncover universal truths, while radical constructivism focuses on understanding multiple subjective perspectives and the role of social and cultural contexts in knowledge construction (King 2004).
This study adopts the limited realist position, which attempts to navigate between extremes of strict realism and radical constructivism. It commits to a realist ontology combined with a constructivist epistemology (King and Brooks 2017). This means that there is an external reality that can be understood through empirical investigation, while also acknowledging that researchers are inevitably influenced by their own perspectives and cannot completely detach from their social context (King 2004).
Creating the initial template and the “final” template
The interview topic guide served as the foundation for the initial template. Four a priori themes were identified based on the interview topics: “Professionalism as defined by the dentists,” “Barriers and challenges experienced at workplaces,” “Experience influencing professional identity formation (PIF),” and “Suggestions for improving professionalism.” This initial template comprehensively covered all the key interview topics.
During the analysis, the researcher (J.H.K.) refined the template while coding the text. The first 2 interviews were coded and then adjustments were made. Afterward, the final template was developed and applied to the remaining 8 interviews. To illustrate the data analysis process using TA, an overview figure was created. See Figure 1.
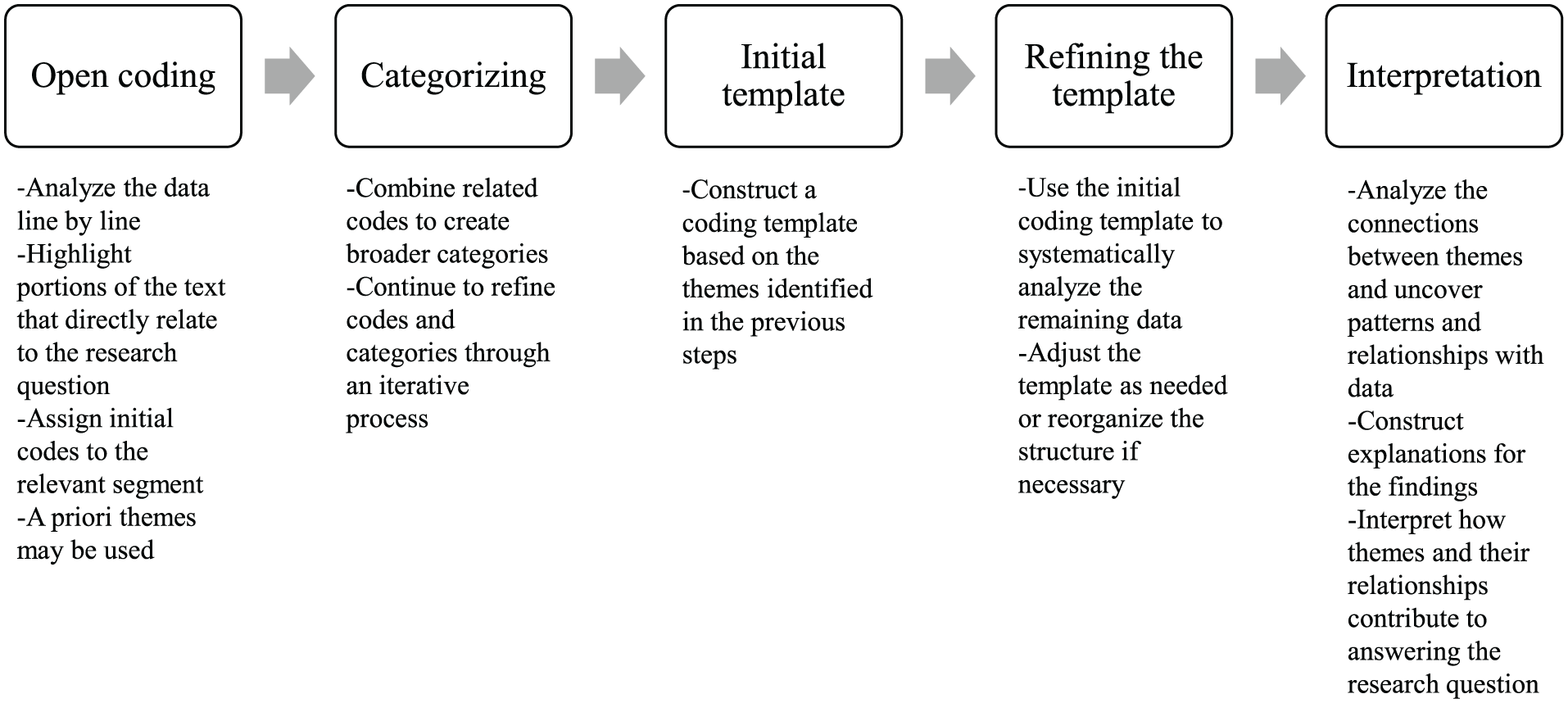
Data-coding process in the template analysis. Overview of the template analysis process used in this study, outlining the steps from open coding and categorization to refining the template and interpreting the data.
Results
A total of 10 individual interviews were conducted. The demographic profiles of the participants are summarized in Table 1.
As described in the “Data Analysis: Template Analysis” section, this study focused on 4 specific domains: (1) understanding how dentists perceive professionalism, (2) identifying barriers and challenges they encounter in their professional environment that may affect dental professionalism, (3) examining the factors influencing their evolving professional identity, and finally, (4) exploring their recommendations for improving dental professionalism. The results of the data analysis are organized around these 4 domains, where we uncovered valuable insights to report.
Domain 1: Dentists’ Perspectives on Professionalism
One objective of this study was to understand participants’ definitions of dental professionalism. Their responses were categorized into 4 themes: “patient-centered approach,” “communication and interaction,” “adherence to professional standards and ethics,” and “personal and professional boundaries.” Figure 2 illustrates these insights.
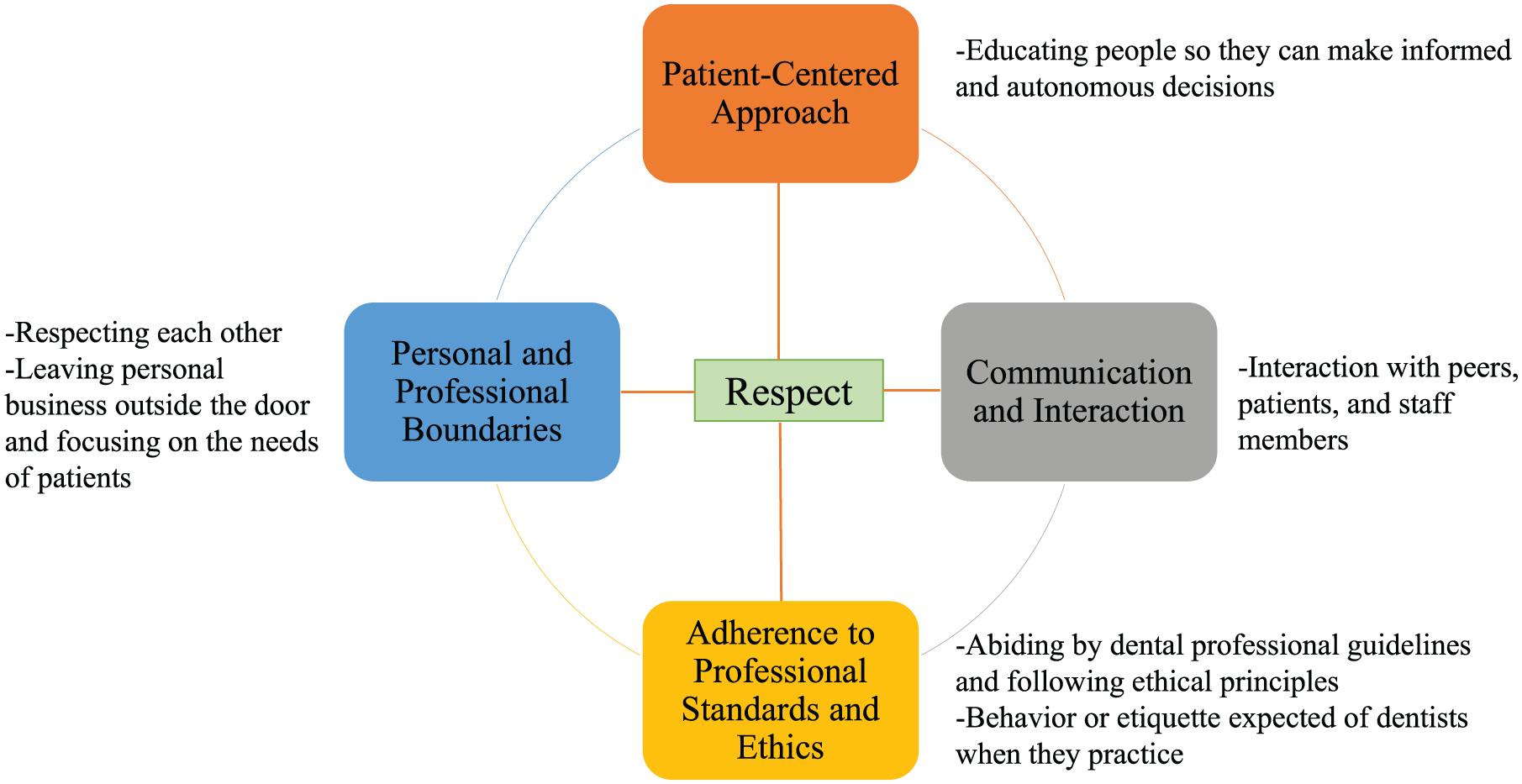
Interviewed dentists’ definitions of professionalism. Key themes reflecting how dentists conceptualize professionalism, including a patient-centered approach, communication and interaction, adherence to professional standards and ethics, personal and professional boundaries, and respect.
Participants described a patient-centered approach as “educating people so that they can make informed and autonomous decisions” (DMD 1, 2, 8, 9, and 10). They emphasized that professionalism involves “positive interaction with peers, patients, and staff” under the theme of “communication and interaction.” Another key theme, “adherence to professional standards and ethics,” highlighted the importance of following “professional etiquette and behaving in a manner expected of their profession” (DMD 3, 4, and 7). Finally, participants cited “personal and professional boundaries,” stressing the need for “respect, and setting aside personal matters to focus on patient needs” (DMD 5, 6, and 9). In Figure 2, respect is central to the themes, as it was frequently mentioned as a core aspect of professionalism.
Domain 2: Barriers and Challenges at Workplaces
Participants were asked about workplace obstacles affecting their dental professionalism, with findings summarized in Table 2. Four themes emerged from the data analysis, reflecting perceived workplace challenges: (1) professional conduct and communication, (2) dental practice environment, (3) patient-related factors, and (4) interprofessional relationships and collaborations. Among the 10 interview transcripts, “professional conduct and communication” and “dental practice environment” contained the most references to professionalism challenges.
Barriers and Challenges Experienced by the Interviewed Dentists.a
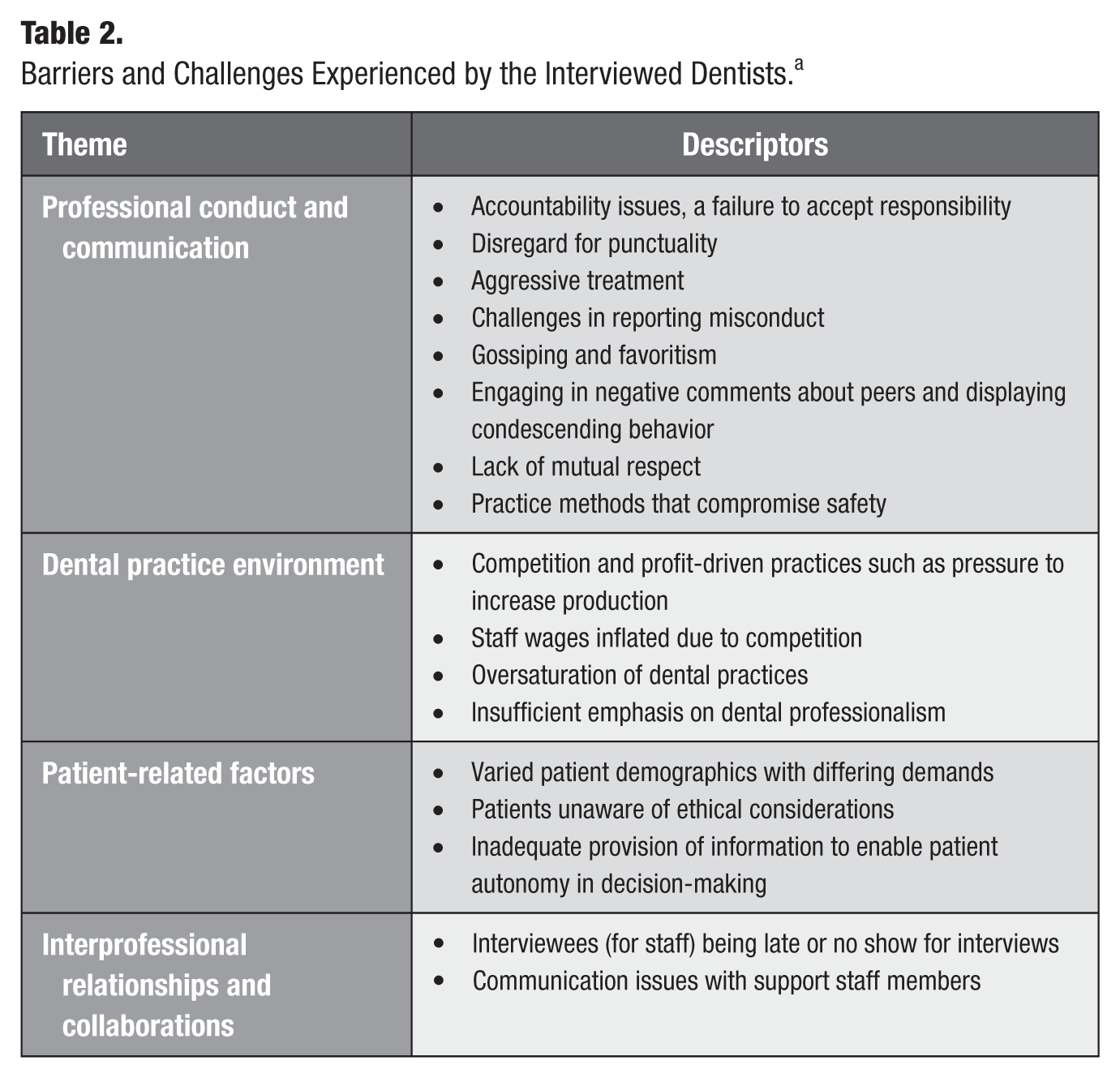
Under “professional conduct and communication,” dentists discussed observing both their own and others’ patient care practices. They highlighted several unprofessional behaviors, such as accountability issues, failure to accept responsibility, disregard for punctuality, aggressive treatment, difficulties in reporting misconduct, gossip, favoritism, negative comments about colleagues, condescending behavior toward peers, lack of mutual respect, and overlooking unsafe practices. The following are example quotes from this theme.
This is the dentistry issue . . . there’s way more dentists than patients that are available. And it depends on the region you are working for. An example is there are conflicting treatment plans and the patient shops around, goes to different offices, and some dentists, you know, say something negative about the other dentists who saw the patient. That’s unprofessional, really, you know, it should be addressed directly with the with the dentist. They shouldn’t talk about a different dentist behind the back or, you know, cause a situation to conflict with the patient. (DMD 10) The only thing that I have seen is basically when a patient comes to me and says that, so and so dentist told me that I need to get eight fillings done. And that’s one example where I look in the mouth. And I'm like, yeah, no, I don’t think so. You know, so that’s where I always saw that there was overtreatment plan. That’s one big thing that really sort of bothered me along the way when I graduated. I realized that changing these old fillings was actually not making much of a difference because there was nothing really wrong with them besides being old and then I became much more conservative. But yeah, I guess the biggest issue I’ve seen is, overtreatment. (DMD 9)
In addition, under the theme of “dental practice environment,” the dentists identified competition and profit-driven pressures, such as production demands, inflated staff wages, oversaturation of dental practices, and insufficient emphasis on dental professionalism, as key challenges to maintaining professional standards (see Table 2). Selected quotes illustrating this theme are presented below.
So that’s the barrier, . . . they have to come up with certain production numbers and how they come about that number. It’s up to them. But clearly, that can lead to unethical behavior, right? So for a dentist who’s just out of school, or who has a large mortgage, or lots of payments, have a brand new family, there’s that pressure to produce. . . . And yes, that can push them push them in the direction of a little bit of an unethical decision making process. . . . (DMD 4) Competition, that’s a very common thing in dentistry with among dentists, they can be with each other. So a lot of dentist and doing unprofessional acts in order to, you know, make a buck, basically, to make some money. (DMD 5)
Domain 3: Dentists’ Recommendations for Enhancing Professionalism
The interviewees’ suggestions for improving professionalism, representing the most substantial data in the transcripts, were categorized into 3 themes: “professionalism education and training,” “institutional responsibilities and oversight,” and “staff and workplace dynamics.”
Theme 1: Professionalism education and training
Building on their definitions of professionalism, the participant dentists strongly advocated for improvements in professionalism education. They emphasized the need for professionalism to be taught explicitly and comprehensively within the dental curricula.
Specifically, the interviewees highlighted the importance of incorporating more ethics scenarios, role-playing activities, and small-group discussions focused on professionalism. Two specific quotes below highlight this recommendation.
What do you do if you see poor dentistry? Or if your patient talks about the previous dentists recommending stuff that you personally would not recommend? Yeah, they didn’t really talk to us about that at school, regarding how to deal with those issues. You kind of have to figure it out on your own when you’re working. So I guess there are no real guidelines. I mean, they just tell you not to talk poorly of other dentists. (DMD 4) . . . we did have one ethics course . . . but I don’t remember really talking specifically about what you would do in this situation. When you haven’t had a busy month, and you’re at the month end. You’ve got high overheads to pay and the patient comes in. And they’re interested in some crowns, but they could clearly do with fillings. What do you do? So I don’t remember ever having that discussion, and I don’t think there was enough emphasis placed in school on that type of decision-making process or how to handle that when you get out. (DMD 5)
The dentists further argued that interprofessional learning and an emphasis on recognizing individual limitations should be integral parts of the dental curriculum, as these elements are critical to improving patient care.
I think there are multiple things that can be incorporated in dental curriculum. To learn, a lot of real cases needs to be discussed, like complex case that involves multiple disciplines to resolve the issue. And you need to obtain different consultations before you proceed with it. I think it brings interdisciplinary views to the dentist because a lot of people in dentistry think dentistry is one man’s job. They are the dentist so they think they can do everything. . . . You have to know your own limitations . . . I think making people recognize their limitations is an important thing from the time that they're in dental school. . . . Once you recognize your own limitations, you know at what point you need to involve other disciplines of dentistry in your treatment plan, and then bring the best outcome for the patient. (DMD 2) Like you know what you are capable of and what you are not, you know. . . . Because a lot of us come out thinking we’re just supposed to do everything, but then it’s not necessary. (DMD 6)
For certain clinical procedures, the interviewees believed that more training hours should be required to avoid breaching professionalism.
For example, people doing sinus lifts, or just surgery where they take a weekend course. There is not enough training . . . standards should be put in place to make sure practitioners get a set number of hours of training. It can’t just be like an afternoon session, watching videos, or listening to a lecture to tell you how to do a certain procedure, and then you’re good to go. I think you have to have hands-on clinical experience. And I think that would be good at the university, if they have that capability of just having these one-month courses, where you get a . . . certificate at the end of it, proving that you actually got the training in . . . providing that treatment. (DMD 3)
Role modeling is crucial to enhance professionalism education. The following quote is one of many examples from our interviewees: The best way to teach is for the instructors to model that. So role modeling, yeah. There were people there that I respected and I thought were professional, and you want to emulate them some way. There are others that you see that aren’t like that, and you don’t want to be like them. (DMD 5)
Theme 2: Institutional responsibilities and oversight
The interviewed practicing dentists emphasized health authorities’ responsibilities and oversight, even giving ideas such as limiting the number of practitioners per area and enforcing stricter regulatory compliance, which was illustrated in the following quote.
If there was a way, I think it would be best to, somehow cap the number of dentists practicing in a specific region to benefit everybody in the end. (DMD 1)
They emphasized the need to reassess licensing standards fairly, especially for internationally trained dentists. See the following quotes.
I think it comes down to enforcing the professional standards of the College because we all are regulated by the College. And that’s who grants the license. For example, if you graduated from UBC, or if you graduated from some university somewhere else in the world, there shouldn’t be two standards saying, Okay, this UBC grad had the training. So they should be treated differently than somebody who graduated elsewhere because they don’t know. Just don’t give a license to that person. We should be all treated the same. (DMD 7) The College will only respond if there’s a complaint. That’s the only thing. But when they grant the license, I don’t know how rigorous the process is. I do think sometimes it’s quite easy to get a license after you pass the examination for dentists nowadays. It doesn’t vet the kind of people who are in the profession anymore. (DMD 9)
The participant dentists’ tolerance of misconduct is not high, and they believed in tougher screening and harsher punishment for those who don’t abide by the guidelines. There was even a suggestion to have auditors sent out to the offices at random.
. . . let’s say, a student who plagiarizes. That’s like a complete no. So, they should be basically kicking the student out. Like it’s part of this is misconduct, not just in dental but in any field. That’s lying. If you cheat in school, you’re going to cheat in life. (DMD 6) I don’t think they [those who don’t abide by the rules] should be in a healthcare profession, because they will hurt people. (DMD 8) Well, there’s got to be a real punishment for those that are caught. Yeah. Like a real punishment is not like a few hundred dollar fine. That does absolutely nothing. If they get their license taken away, or, or something like that, then it’s more of a real punishment. (DMD 9) . . . just like a secret audit of what’s being done in the office . . . I’m sure it will be legally challenged but at least you put the fear of that into the dentists too, so that they will behave accordingly. (DMD 5)
Theme 3: Staff and workplace dynamics
The interviewed dentists also called for promoting better treatment of staff, fostering a team-oriented mindset, and addressing mistreatment issues directly. The 2 quotes below illustrate this finding.
I don’t know if this is helpful or not. But this is speaking from my own experience of owning a dental practice. . . .I think that if you can set up a practice,. . .where you treat your staff in a respectable way, and you treat your patients in a respectable way. And you yourself set it up so that you get treated in a respectable way . . . from the very beginning, you’ll be happier, and you’ll make better decisions as you go along. And you’ll be able to practice longer. I think that one of the biggest stresses when I first had my own practice was letting certain staff members mistreat me, letting patients mistreat me a lot, or taking advantage of me . . . just abusing my time, abusing my services in terms of not paying or, again, not showing up. Get rid of the patients and the staff that just make your life miserable. And if you can do that as soon as possible, you’re going to have a better career, you’re going to be happier. And it might be a bit more painful at the beginning because you won’t be as busy but it will help you in the long run. (DMD 9) . . . it [workplace] should be more of a team mentality more than anything. (DMD 1)
Based on the quotes, participants emphasized that creating a respectful, team-oriented work environment, in which both staff and patients are treated with dignity, is essential for long-term career satisfaction and success, while addressing mistreatment early on can lead to a healthier, more sustainable practice.
Domain 4: Dentists’ PIF
In examining the progression of dentists’ professional identity development, my focus centered on identifying key contributors to this evolution. For the participants, unlike dental students, I explored how their work experiences and challenges encountered in their professional environment shaped their evolving professional identity. These influencers are illustrated in Figure 3.
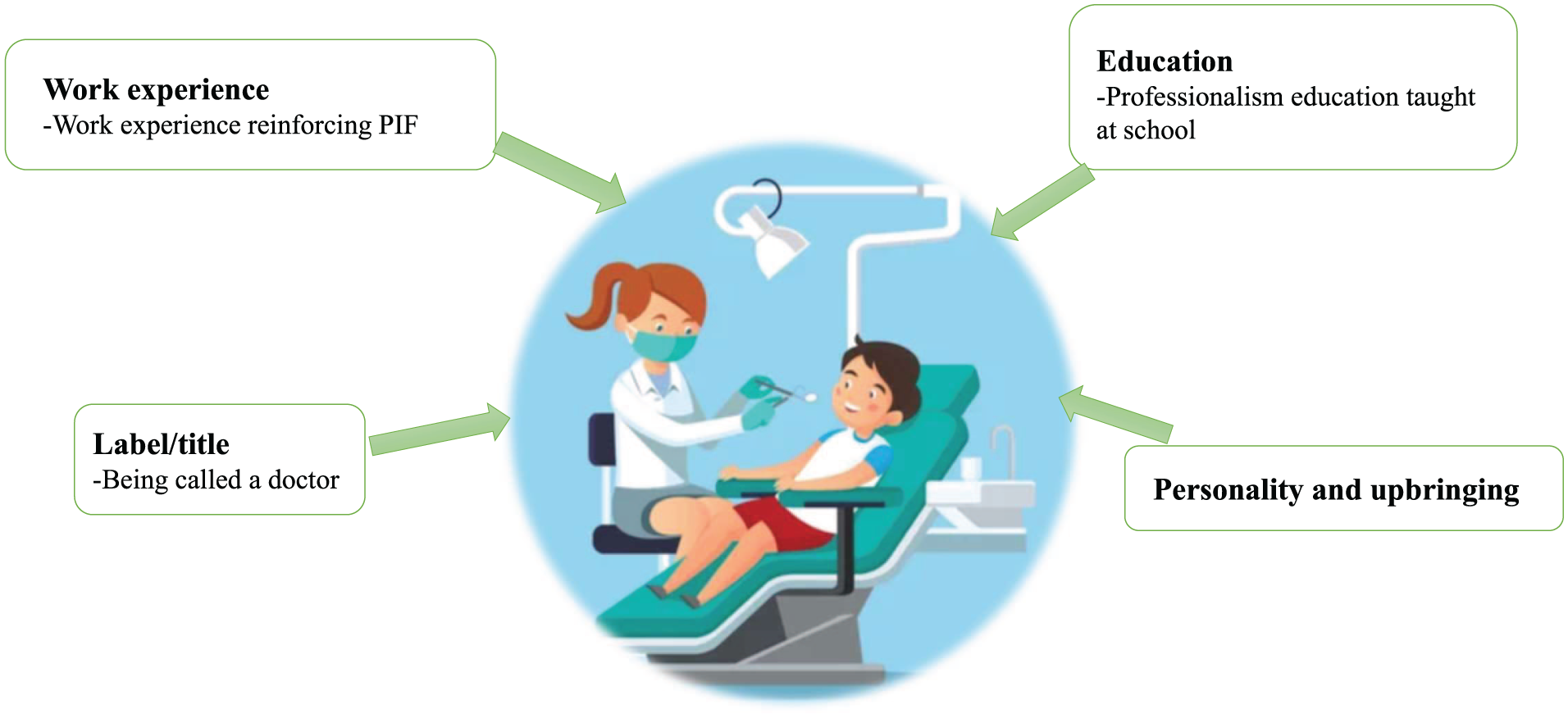
Influencers of dentists’ professional identity formation. Factors influencing professional identity formation among practicing dentists, including education, work experience, personality and upbringing, the role of the professional title, and experiences that reinforce their sense of professional identity.
Analysis of the interview transcripts revealed that hands-on work experience was crucial in shaping the dentists’ professional identities. This factor is closely tied to domain-specific self-efficacy, a key contributor to dental students’ PIF in the authors’ other study (Kwon et al. 2022). For students, developing clinical confidence through repeated practice and successful outcomes is critical, as their professional identity heavily depends on mastering clinical skills. Similarly, for practicing dentists, work experience strengthens and solidifies their professional identity as they navigate real-world patient care and ethical challenges. The confidence they gain from managing complex cases mirrors the way students build self-efficacy through clinical practice. This continuous interaction between experience and growing competence not only enhances clinical skills but also reinforces their identity as confident and capable dental professionals.
As they practiced more, their sense of being a dentist strengthened. Some noted that experience led them to adopt more conservative treatment approaches, while others did not experience this shift. In addition, reducing financial burdens and gaining experience empowered them to make more ethical decisions. The following quotes illustrate these perspectives: I think your professional identity becomes stronger the more you are exposed to cases as years go by and the more you put your skills into practice. Some challenges that you see at the beginning of your practice that took longer to resolve it, you can resolve it faster as you get more experience. You become more efficient at addressing them. (DMD 5) . . . it comes down to those pressures of when you first start practicing and having expenses. A patient comes in and they’re like, “Hey, Doc, I just need a checkup. Do you see anything wrong in my mouth?” “Oh, you got some old fillings, but they totally look fine besides they look a little old. Let’s just leave them alone and keep an eye on them.” If that patient came 25 years ago, a couple of years into my practice, I probably would have said, “you never know what’s happening underneath them. Let’s change them.” And to be honest, it was probably at the end of the day, I thought, Okay, I’ve got to produce something because it was my own practice. And I need to pay the assistants, I need to pay the front desk. I need to pay my rent. I need to pay my mortgage. Yeah, let’s do these fillings because they look old. And again, “Oh, you got 100% insurance. It’s covered. Why don’t you do it? Let’s get it done.” So I would have done that. But to be honest, reducing my financial burdens along the way has helped me to be more conservative. But clearly, yeah, the experience along the way has changed my mindset in terms of the decisions I would have made then versus now. (DMD 9)
Another key factor highlighted was the impact of the label or title of “doctor,” which influenced their feelings and behavior, often fostering a greater sense of responsibility. They reported that this title reinforces a sense of accountability, serving as a constant reminder of their professional roles and expectations. The societal weight attached to the title provides external validation and influences how dentists perceive themselves within the profession. Therefore, within dental education, discussing the weight of the title “doctor” could be valuable for PIF. The following quotes illustrate this: It feels good to be called a doctor after graduation. . . . I think that from the beginning, there’s just a higher expectation of your behavior in everything that you do. When someone needs help with something, even when it’s not dental related, “Oh, I've got this doctor helping me. It’s going to be better than someone who’s not a doctor.” People have that sort of feeling. Dr. So and So, can you come in to help me fill this form, asking me to help them with some paperwork at the mosque? Oh, Dr. So and So, if you can do this for me versus, you know, Bob down the road there. So, there’s more of a responsibility right off the bat. (DMD 5) I do feel more responsible. People will look up to me more in terms of, that’s not coming again, from a prideful manner. That’s just that people expect more of you. When they’re calling me doctor, they expect a certain type of behavior and a certain type of decision-making. Or just a certain type of demeanor with them when dealing with them. So, yes, you do feel more responsible when they call you their doctor. (DMD 10)
Some participants felt that upbringing and personality play a significant role in shaping their intrinsic values and how dentists practice professionally. As discussed later, this factor is closely connected to the dentists’ individual identities, which serve as the foundation for their professional identities (Cruess et al. 2016). Individual identity encompasses a person’s core values, beliefs, traits, and life experiences, all of which are significantly influenced by their upbringing and inherent personality. The following quotes illustrate this: In my personal opinion, it just depends on how they were brought up and on and, and what their personal views are. I mean, it’s like, if you have a person who is not nice, you can tell them what is nice and what is not nice, but they will never be a nice person. (DMD 7) I think it’s a personality . . . I think it comes down to the person and their upbringing, like how your family has raised you and what your moral compass is. And I think, if you are that kind of person, you would go in that direction. And if you’re not, if you’re raised a certain way, if you’re a certain kind of person, you wouldn’t do that. . . . Not everybody responds to this kind of pressure. (DMD 4)
The study participants believed that the education they received also played an important role in shaping the kind of dentist the participants became, as reflected in the following quote: I went to UBC. I remember the first day, we had this course called “Doctor, Dentist, Patient, and Society” or something like that. And the first thing we learned was the word “empathy.” And we modeled that and it stayed with me until today. That’s something I learned. And if we were taught, this becomes part of who you are as a dentist, as a doctor. That’s what you’re supposed to do. (DMD 1)
Based on the quotes, participants highlighted that their professional identity was shaped by a combination of factors, including the responsibility associated with being called “doctor,” their upbringing and personal values, the effect of their education, and hands-on experience, with many noting that, over time, reduced financial pressures and increased experience allowed them to make more ethical and conservative treatment decisions.
Discussion
The discussion builds directly on the themes presented in the “Results” section. Drawing from the illustrative quotes analyzed in the results, we identified core themes that were analyzed in greater depth in the discussion to highlight their broader significance.
PIF as the Focal Point
Participants identified core values such as patient-centered care, clear and effective communication, adherence to professional standards and ethical guidelines, and maintenance of professional and personal boundaries as essential aspects of professionalism. These values generally align with widely accepted definitions of professionalism within medical and dental communities (Stern 2006; Zijlstra-Shaw et al. 2011; ADEA Statement on Professionalism in Dental Education 2017).
Interestingly, some senior dentists we interviewed noted that at the beginning of their practice, the concept of being “called a doctor” emerged as a factor that could enhance their sense of responsibility and contribute to their professional identity. This finding appears to support identity theory (McCall and Simmons 1978) and social identity theory (Turner 1987), which propose that titles such as “doctor” act as markers of group affiliation and that individuals’ social identities frequently transition to embody the norms and behaviors linked to that role (Stets and Burke 2000). This behavior adjustment could bolster the significance of their title as individuals strive to align with the group’s values and standards (Turner 1987; Stets and Burke 2000).
Given that this finding emerged from participants who have been practicing for 25 y or longer, future research might explore whether the title of “doctor” similarly shapes the professional identity of junior dentists. If the title indeed plays a role, it could be beneficial to incorporate discussions on the expectations associated with the “doctor” title into dental education, in line with social identity theory, where the title is seen as a symbol of social responsibility.
Bridging the Gap in Professionalism Education
The dentists’ responses indicated a gap between their understanding of professionalism and the professionalism education they received. A key concern was the reported lack of training opportunities in crucial areas such as managing ethical dilemmas and fostering interprofessional collaboration. However, it is important to consider the potential influence of reflection bias, in which individuals may reinterpret past experiences based on their current perspectives, potentially affecting the accuracy of their recollections. To assess whether professionalism education was indeed insufficient, a review of past dental curricula would be necessary, alongside further research to explore how professionalism training was structured and perceived at the time of instruction.
Although courses in dental ethics are commonly included across dental curricula in North America, a rapid review of dental program offerings indicates that professionalism is rarely presented as a standalone course. Instead, professionalism is embedded as a core theme throughout dental education, often conveyed implicitly through role modeling, the hidden curriculum, and the broader institutional culture (Joynt et al. 2018). While these elements play a significant role in shaping students’ professional development, they can vary widely in consistency and effectiveness. In contrast, most dental schools do offer a dedicated course in dental ethics. A central framework commonly used in these courses is principlism, which emphasizes ethical decision-making through 4 core principles: autonomy, beneficence, nonmaleficence, and justice (Beauchamp and Childress 2001).
To address this education gap, the dentists recommended more comprehensive professionalism education approaches that are in the form of case-based discussions, role-playing exercises, and group presentations. These activities could help strengthen students’ critical thinking, reflective abilities, and decision-making skills, particularly in navigating ethical challenges or responding to patient requests for nonessential procedures. Future studies could further investigate the impact of these educational strategies on the development of professional identity.
Communication and Collaboration
The interviewees emphasized the importance of communication skills in facilitating effective professional interaction with patients, colleagues, and staff. The professionalism literature underscores the significance of interactions with patients, colleagues, and communities (Bossers et al. 1999). Our findings from interviews with dentists further reinforce the need to integrate dedicated and enhanced communication skills within dental curricula. Such integration would better prepare future dentists for complex conversations, enable them to demonstrate empathetic reasoning, and help them build rapport and trust with patients.
In addition, the interviews revealed that fostering interprofessional collaboration through small-group learning activities was strongly recommended by the dentists. This approach, they argue, better prepares students for the collaborative demands of modern health care delivery. This recommendation aligns with existing research in dental education, which underscores the benefits of small-group learning in enhancing communication and collaboration skills (Lopez et al. 2022).
Workplace Culture and Professionalism
An important yet unsurprising finding from the interviews with dentists was the impact of workplace dynamics on professional conduct. According to Kegan’s theory of meaning making pertaining to identity formation, 3 key aspects shape adults’ identity: cognitive, emotional, and social (Kegan 1982; Kegan 1994). The health care workplace is where most social interactions occur, whether between clinicians and patients, clinicians and staff, or clinicians and other clinicians.
Our participants described that, in some cases, the behaviors of other dentists contributed to professionalism challenges. Moreover, pressure to meet quotas, cover overhead costs, and manage insufficient support staff were identified as threats to professionalism. While dental schools cannot predict the specific workplace environments their students will encounter, they can promote and establish mentorship programs focused on ethical decision-making and teamwork. The economic challenges of running a dental clinic could also serve as a real-life scenario in which students can engage and develop their own ethical solutions.
Disconnect between Professionalism and Professional Identity in Dentistry: Experience versus Ethics
Stern (2006) argued that clinical competency is 1 of the 3 foundational elements of professionalism. However, in the context of dental education, it is equally important to emphasize values, ethics, and interpersonal skills, given that dentistry is a relational profession centered on patient care. Developing these dimensions is essential for shaping well-rounded dental care professionals.
Interviews with participants suggested that while clinical practice experiences appeared to strengthen clinicians’ sense of professional identity, these experiences did not always lead to stronger ethical and professional behavior. External pressures, such as a competitive market environment, may influence clinicians’ professionalism. This suggests that practical wisdom should not always be assumed with the accumulation of experience. The dentists’ responses suggest that without deliberate and guided self-reflection, PIF may not consistently get integrated and translate into professional behavior.
The gap became more apparent during the interviews. Only 1 dentist explicitly acknowledged personal areas for improvement, while many others focused on external factors—such as patients, education, or workplace environment—rather than critically reflecting on their own roles in maintaining professionalism. Further research is needed to explore how guided reflection can be better internalized to support ethical and professional development.
Awareness and Empowerment
Raising awareness about professionalism issues and empowering dentists to embody professional qualities and behaviors requires a multifaceted effort from educational institutions, regulatory bodies, dental professional associations, and individual practitioners. Comprehensive professionalism education during dental school, along with ongoing continuing education programs such as conferences, webinars, and other educational events focused on professionalism issues in dentistry, may be beneficial. From this study, participants recommended case-based scenarios and small-group discussions as effective tools for enhancing professionalism. They also emphasized stricter penalties for professional misconduct.
Some dentists noted that with more experience and reduced financial stress, they felt more “empowered in professionalism” and could better prioritize patient care. Greater clinical expertise and reduced financial pressures appeared to give them the freedom to focus on patient needs rather than economic demands. However, further research is needed to better understand how these factors influence professional behavior over time.
Limitations and Future Directions
A key limitation of this study is its small and specific demographic, which limits its transferability beyond Canada. Future research should include a larger and more diverse group of dentists from broader regions, as well as other dental professionals, such as hygienists and certified dental assistants, to gain a more comprehensive understanding of professionalism within dental practice dynamics. In addition, as the study focuses on practitioners in Vancouver, the findings are influenced by the regional practicing culture. Expanding the investigation to explore how different cultural and professional contexts shape dentists’ professional identity would provide a more nuanced perspective.
Such an expansion would allow for a broader examination of the contributors to professionalism identified in this study, offering a more complete understanding of the challenges faced in the dental profession. Furthermore, future research could investigate the effectiveness of various teaching methods in professionalism education and assess the role of regulatory bodies in promoting and enforcing professional standards. These insights could help address the accountability concerns raised by participants and inform improvements in dental education and professional development.
Conclusion
This study suggests that dental education plays a crucial role in shaping professionalism and professional identity, as perceived by practicing dentists in a metropolitan area in Canada. As outlined in the “Discussion” section, the findings from the dentists offer valuable insights into how professionalism education within the Canadian dental curriculum can be enhanced. In summary, these insights emphasize the need for a stronger focus on structured self-reflection, additional support to bridge the gap between theoretical understanding and the practical application of ethics, small-group scenario-based learning to improve communication and collaboration, and fostering a culture of professionalism in both education programs and workplaces by a combination of institutional leadership, mentorship, and continuous professional development, supported by effective licensing and oversight mechanisms from the College.
Author Contributions
J.H. Kwon, contributed to conception and design, data acquisition, analysis, and interpretation, drafted the manuscript; H. von Bergmann, contributed to interpretation, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jct-10.1177_23800844251413578 – Supplemental material for Exploring Dentists’ Views on Professionalism and Identity Formation: A Template Analysis Study
Supplemental material, sj-docx-1-jct-10.1177_23800844251413578 for Exploring Dentists’ Views on Professionalism and Identity Formation: A Template Analysis Study by J.H. Kwon and H. von Bergmann in JDR Clinical & Translational Research
Supplemental Material
sj-pdf-2-jct-10.1177_23800844251413578 – Supplemental material for Exploring Dentists’ Views on Professionalism and Identity Formation: A Template Analysis Study
Supplemental material, sj-pdf-2-jct-10.1177_23800844251413578 for Exploring Dentists’ Views on Professionalism and Identity Formation: A Template Analysis Study by J.H. Kwon and H. von Bergmann in JDR Clinical & Translational Research
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
This study is based on qualitative interview data. In accordance with institutional ethics approval and to protect participant confidentiality, verbatim transcripts and full interview datasets cannot be shared publicly. De-identified data excerpts are included in the article. The coding framework used in the analysis is provided as a ![]() to support transparency of the analytic process.
to support transparency of the analytic process.
A supplemental appendix to this article is available online.