
Abstract
Introduction:
In the United States, dentists are one of the leading prescribers of opioids and antibiotics. Because dental schools are the training grounds for future dentists, it is crucial to understand how prescribing has changed and why these medications are being prescribed in academic settings.
Objectives:
The objective of this research was to describe the prescribing trends and factors associated with opioid and antibiotic medication prescribing at US academic dental institutions between 2011 and 2020.
Methods:
Data from electronic dental records collected through the BigMouth data repository from 9 anonymized dental institutions between 2011 and 2020 were used. Prescribing rates were defined as the percentage of patients who received an opioid/antibiotic prescription. The primary outcome was whether at least 1 opioid or antibiotic medication was prescribed at the encounter. Monotonicity and statistical significance of prescribing trends by year were assessed using the Mann–Kendall test, and a statistical analysis using an adjusted multilevel mixed-effects logistic regression model was performed to identify significant patient-, visit-, and dental provider–level factors associated with prescribing of these medications.
Results:
In total, 5,720,166 patient encounters from 905,426 patients had aggregate opioid and antibiotic prescribing rates of 2.0% and 2.7%, respectively, between 2011 and 2020. For both medications, a downward prescribing trend was observed from 2013, which increased in 2020. Opioid prescribing was most likely for young adults aged 15 to 24 y (odds ratio [OR] = 5.26;95% confidence interval [CI]: 4.99–5.55) and by oral surgeons (OR = 10.03; 95% CI: 8.02–12.55). Antibiotic prescribing had a higher odds for patients aged >65 y (OR = 5.04; 95% CI: 4.62–5.49) and by periodontists/implant specialists (OR = 6.21; 95% CI: 4.96–7.78). Multiple treatments at the same dental visit and pain-associated dental procedures were associated with statistically significantly higher odds of being prescribed both medications.
Conclusion:
There are significant differences in opioid and antibiotic prescribing by dentist specialty, patient age, whether the dental visit had multiple treatment procedures, and whether 1 or more postoperative dental pain–associated procedures were performed.
Knowledge Transfer Statement:
This study provides an understanding of patient-, dentist-, and visit-level factors associated with opioid and antibiotic medication prescriptions issued by clinicians at academic dental institutions in the United States. The results can contribute further to predict clinical scenarios related to the prescribing of these medications and the development of specific interventions to reduce inappropriate and excessive opioid and antibiotic medication prescribing.
Keywords
Introduction
Dentists are the leading prescribers of opioid and antibiotic medication in the United States. They are one of the major specialties prescribing immediate-release opioids (Volkow et al. 2011), with opioids accounting for approximately one-third of all prescriptions issued by dentists (Levy et al. 2015). Nearly half of opioid-related drug overdose deaths can be attributed to prescription opioids, and 1 in 16 patients receiving an opioid prescription after surgical procedures becomes a long-term opioid user (Farooqi et al. 2020). Dentists frequently prescribe opioids for traumatic, surgical, and inflammation-inducing procedures, particularly those involving the extraction of third-molar teeth, implant procedures, and root canal treatments (Denisco et al. 2011; Mutlu et al. 2013). The high rate of opioid prescribing continues, despite studies showing that nonsteroidal anti-inflammatory drugs (NSAIDs) and acetaminophen are just as effective at treating many postsurgical cases as opioids are (Wong et al. 2016). Moreover, it is estimated that each year, more than 1 million opioid pills prescribed for pain management related to third molar extraction remain unused, which may serve as a source for nonmedical use and increase the lifetime risk of future opioid abuse (Lutfiyya et al. 2018). While opioid prescribing may be warranted in certain cases in which the patient has contraindications to NSAIDs and acetaminophen, it is necessary to follow the current prescribing guidelines (American Dental Association 2016; Dowell et al. 2022) in such cases to ensure that lowest possible effective dose for the shortest duration is prescribed.
In the United States, according to the Antibiotic Resistance Threats Report by the Centers for Disease Control and Prevention in 2019, at least 2.8 million people are affected with antibiotic-resistant infections annually, resulting in more than 35,000 deaths. Most antibiotic prescribing occurs in the outpatient setting (Suda et al. 2018), with dentists writing 10% of those prescriptions (Hicks et al. 2015; Suda et al. 2016; Durkin et al. 2017). In 2016, 26 million antibiotic medications were prescribed by dentists alone, up from 24 million in 2013 (Roberts et al. 2017). Clinically, antibiotics are frequently inappropriately prescribed for managing acute dental conditions (Cope et al. 2016), where they may be of little clinical benefit (Dailey and Martin 2001), as such ignoring established guidelines, some of which indicate limited prophylactic prescribing only in patients with certain cardiac conditions or those that are immunocompromised or to treat active infections (American Dental Association Council on Scientific Affairs 2004; Fluent et al. 2016; Lockhart et al. 2019).
While some studies (McCauley et al. 2018; Alghofaily et al. 2019; Shemkus et al. 2020) in groups of dentists or at single dental institutions have been conducted to assess opioid and antibiotic prescribing, there is a lack of recent evidence in a nationwide sample of prescriptions across multiple academic dental institutions. Because dental schools are the training grounds for future dentists, it is crucial to understand how prescribing has changed and why these medications are being prescribed in academic settings. Thus, the objective of this research was to identify the factors and trends associated with opioid and antibiotic prescribing at academic dental institutions between the years 2011 and 2020 in the United States.
Methods
Data Source and Study Sample
To attain the research objectives, this study used the Consortium for Oral Health Research and Informatics (COHRI) BigMouth (Walji et al. 2014) database queries to extract and quantitatively analyze data from electronic dental records (EDRs; axiUm) across 9 academic dental institutions in the United States (BigMouth Partnering Dental Institutions 2024). The study sample included data on all dental patient visits, opioid, nonopioid analgesic, and antibiotic medications prescribed at these institutions by residents and faculty between the years 2011 and 2020.
Data Processing and Classification
Different tables of the extracted data were joined to create patient encounter–level data. An encounter was defined as a patient visit with at least 1 treatment or prescription within ±7 d of treatment. All medications were classified based on their drug group and drug class (Appendix Table 2). Dental treatments requiring surgical manipulation of oral soft and hard tissues were classified as dental pain–associated procedures based on a literature review of the evidence (Gupta et al. 2018b) and the expert opinions of dental clinicians (Appendix Table 3). Because dental students cannot directly prescribe without faculty authorization, the prescriptions in which the provider was a dental student were attributed to the authorizing faculty provider.
Data Analysis
The outcome/dependent variable was whether at least 1 opioid or antibiotic medication was prescribed at the encounter. Descriptive statistics were calculated to describe the underlying data with frequencies, percentages, mean, and standard deviation as appropriate. Prescription rates were defined as the percentage of patients who received opioid/antibiotic prescriptions, calculated by dividing the number of the encounters that had at least 1 opioid or antibiotic prescription by the total number of encounters. Trends in prescribing between 2011 and 2020 were assessed for statistical significance using the Mann–Kendall test.
Given the inherent clustering of patient encounters within dental providers, multilevel mixed (MLM) effects models were used to conduct the analysis. The predictor variables assessed at encounter level (level 1) were patient’s gender, age, race, multiple procedures, and pain-associated procedure being performed at the encounter. The predictor variables assessed at dental provider level (level 2) were the provider’s clinical role (resident or faculty) and their dental specialty. Unadjusted 2-way logistic regression for assessing the association with outcome variables was done for every predictor variable, and the percentage of outcome variable for each predictor category was also reviewed to check if any predictors could be eliminated in the MLM model. Any categories of predictor variables that had less than 1% of the outcome variable were eliminated from the model. We tested whether eliminating these categories would not result in loss of any meaningful associations in the model by using 1-way analysis of variance. The intraclass correlation coefficient (ICC) was calculated to compare the variances contributed by the encounter and dental provider clusters to prescription differences. Multilevel models were developed starting from a null model for whether an opioid/antibiotic was prescribed without any predictors, an intermediate model including select encounter-level and provider-level predictors, and a full model including all predictors. The intermediate and final models were compared using the likelihood ratio test to determine which model fit better. The final model adjusted for patient’s age, gender, whether they had undergone a postoperative pain-associated dental treatment, whether they had multiple treatments, the dental provider’s clinical role/type, and their dental specialty. All models had fixed effects for level 1 and random effects for level 2 variables with random intercept. The 1-factor-at-a-time approach of sensitivity analysis was used to exclude the 2020 data and gauge the effect. All quantitative statistical analyses were performed at the standard significance level (a = 0.05) using Stata Statistical Software release 15 for StataCorp LP.
Results
A total of 5,720,166 patient encounters having at least 1 dental procedure associated with 905,426 patients and 16,395 dental care providers from 9 dental institutions across the United States between the years 2011 and 2020 were included in this study. Figure 1 shows the number of encounters that were excluded, the reasons for their exclusion, and the number of encounters in the final dataset used for analysis. Table 1 shows the distribution of the variables with corresponding number and proportion of encounters. The associated number of patients and providers are included in Appendix Table 1.
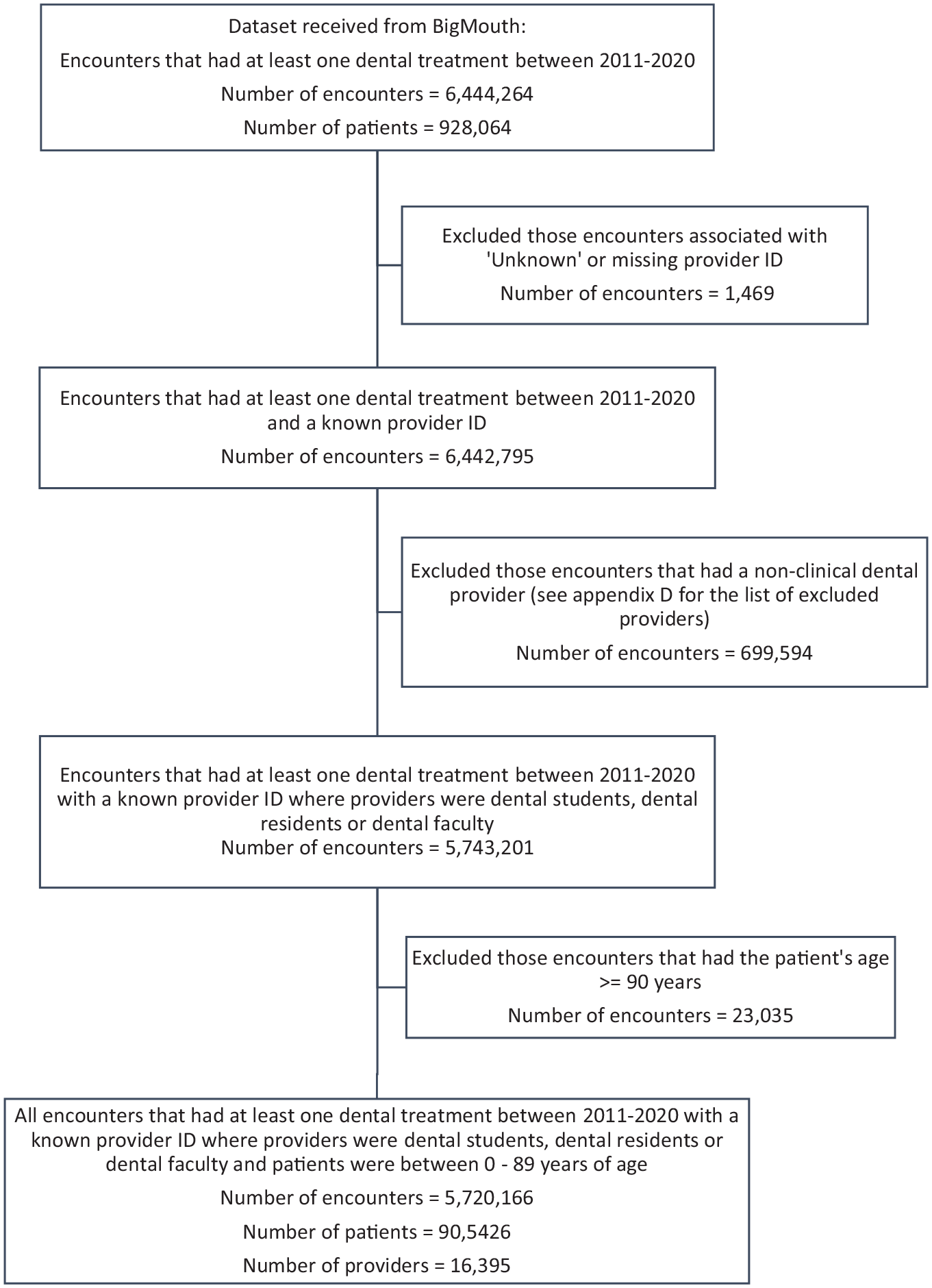
Flowchart showing the number of encounters and associated number of patients and dental care providers who were included or excluded at each data preparation step.
Distribution of All Variables by Number and Proportion of Encounters.
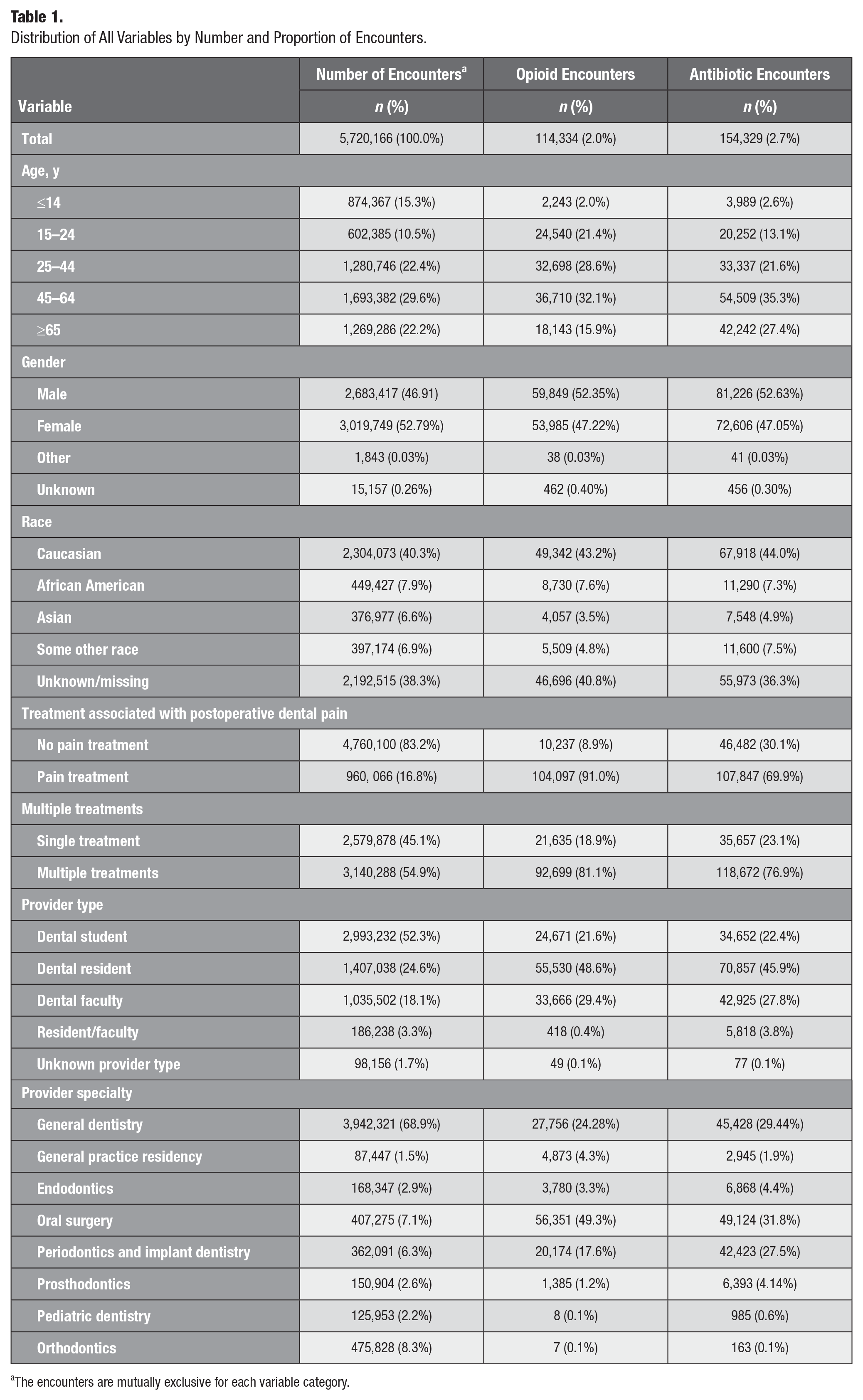
The encounters are mutually exclusive for each variable category.
Trends in Prescribing across the Years
Overall, between the years 2011 and 2020, the opioid-prescribing rate was 2.0%, and the antibiotic prescribing rate was 2.7%. The percentage of encounters with at least 1 opioid prescription sharply decreased between 2015 and 2018 from 2.8% to 1.01% but increased in the year 2020, with a statistically significant downward trend (P = 0.002). For antibiotic prescribing, there was a slight gradual decrease in prescribing between 2013 and 2018 from 2.99% to 2.45% followed by an increase in prescribing from 2018 to 2020, with no statistical significance for the overall downward trend (P = 0.09). Figure 2A shows the change in opioid and antibiotic prescribing between 2011 and 2020.
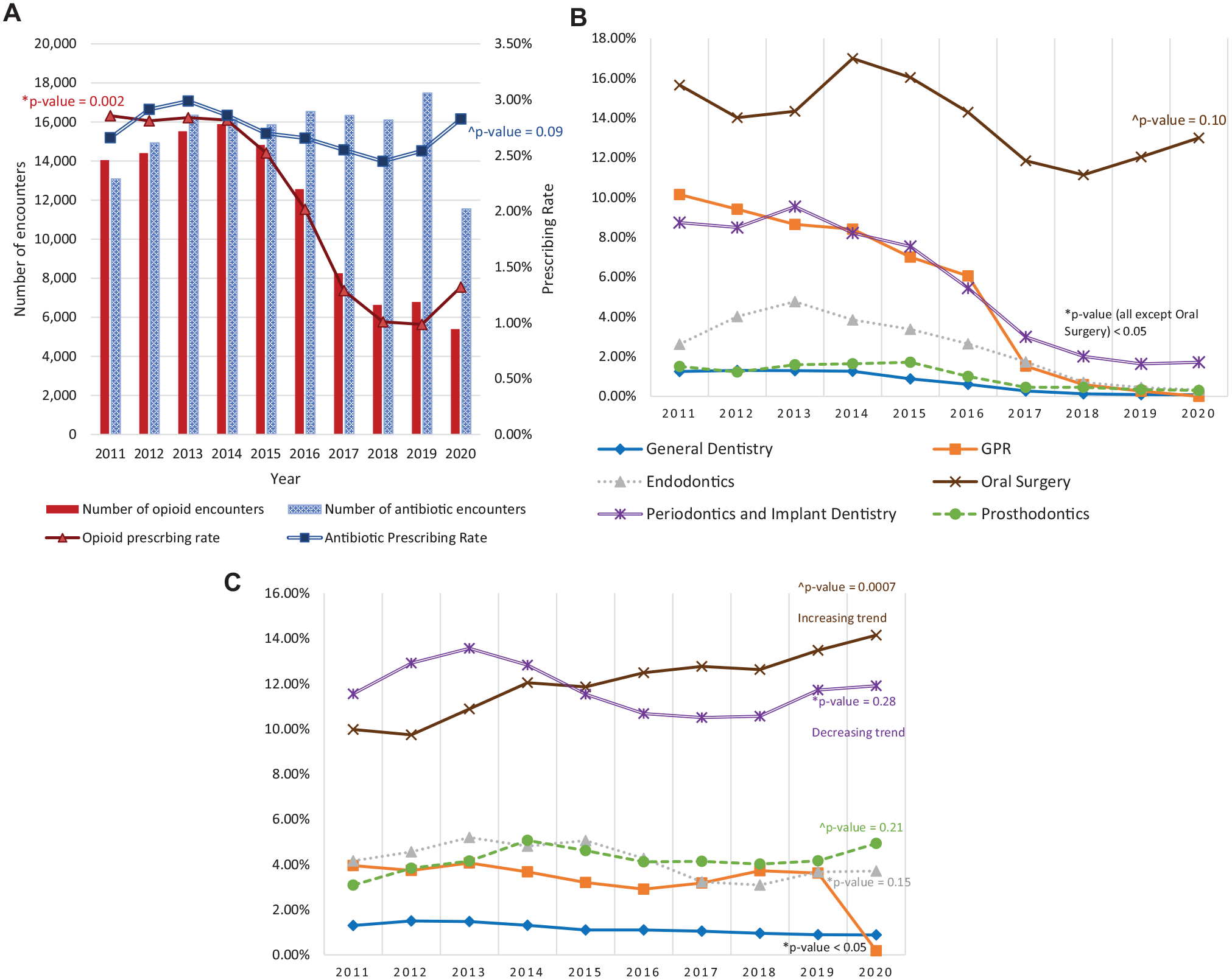
Trends in opioid and antibiotic prescribing from 2011 to 2020. (
Trends in opioid prescribing by dental providers’ specialty
Opioid prescribing by oral surgeons was 15.65% in 2011, declined from 16.99% in 2014 to 11.14% in 2018 (not statistically significant, P = 0.10), and showed an upward trend reaching 13% in 2020. Oral surgeons were consistently the highest prescribers of opioid medication across all years. While prescribing by all specialties decreased to less than 2% by the year 2020, opioid prescribing by oral surgeons increased to 13% in the year 2020. The downward trend in opioid prescribing was drastic for providers who were from the specialty periodontics and implant dentistry, which declined from 9.54% in 2013 to 1.71% in 2020 (P = 0.0007). Figure 2B shows this trend in opioid prescribing between 2011 and 2020 by providers from different specialties.
Trends in antibiotic prescribing by dental provider specialty
Antibiotic prescribing for most specialties was constant, with a slight increase or decrease across the years, except for oral surgery and periodontics and implant dentistry. A decline in antibiotic prescribing by periodontists from 13.57% to 10.56% was observed between 2013 and 2018, increasing up to 11.91% in 2020. Oral surgeons had a statistically significant (P = 0.0007) increasing trend in antibiotic prescribing, rising from 9.97% to 14.15% between 2011 and 2020. Figure 2C shows the trend in antibiotic prescribing between 2011 and 2020 by providers from different specialties.
Statistical Analysis for Assessing Predictors Associated with Opioid and Antibiotic Encounters
All variables showed a statistically significant (P < 0.05) association with inflated estimates for measures of association in an unadjusted 2-way logistic regression model. The ICC for an empty MLM effects model with dental provider as the cluster-level variable for the outcome variable of at least 1 opioid prescription at the encounter was 0.5849 (95% confidence interval [CI]: 0.5755–0.5942) and at least 1 antibiotic prescription at the encounter was 0.5132 (95% CI: 0.4998–0.5265), indicating that 58% of the chances of an opioid prescription and 51% of the chances of an antibiotic prescription can be explained by between-provider (i.e., provider-level) differences. The likelihood-ratio (LR) test comparing the nested intermediate model (level 1 predictors [patient’s age, pain-associated treatment, and multiple treatments] and all provider-level predictors) with the full model was statistically significant (P = 0.000), indicating that the full model with all encounter- and provider-level predictors fit better. The model controlled for all level 1 and 2 predictors, and the odds ratios were interpreted considering the reference categories of all included predictors in the model. Sensitivity analysis conducted to check for impact of the year 2020 on the results found that the directionality and magnitude of the associations with their statistical significance remained unchanged with and without the 2020 data. A difference of only a few decimal points was found in the estimates.
Factors associated with opioid prescribing
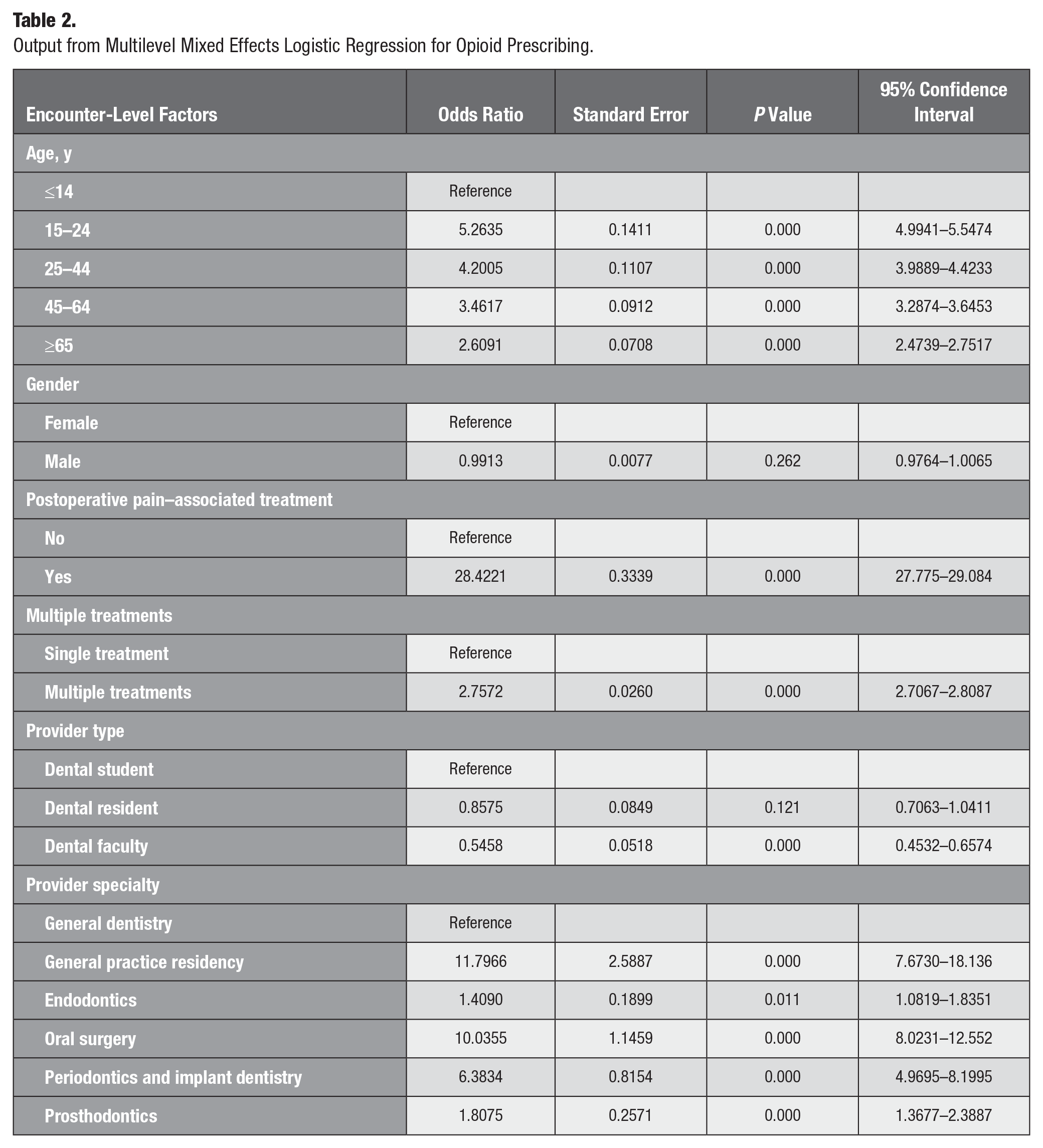
Table 2 shows that at the encounter level, the odds of being prescribed an opioid gradually decreased for each age category, with the highest odds being associated with patients between ages 15 and 24 y who had 5.26 (P = 0.000; 95% CI: 4.99–5.55) times greater adjusted odds. Encounters that had at least 1 treatment associated with postoperative dental pain on the same day had 28.42 (P = 0.000; 95% CI: 27.77–29.08) times more adjusted odds of being prescribed an opioid as compared with other encounters. Encounters that had multiple treatments on the same day had 2.73 (P = 0.000; 95% CI: 2.71–2.81) times higher adjusted odds of an opioid prescription than those with a single treatment. Encounters in which the provider was an oral surgeon had 10.03 (P = 0.000; 95% CI: 8.02–12.55) times more adjusted odds and those in which the provider belonged to the periodontics and implant dentistry specialty had 6.38 (P = 0.000; 95% CI: 4.97–8.20) times more adjusted odds of having an opioid prescription compared with encounters in which the provider was a general dentist. The lowest odds of opioid prescribing among all specialists was seen in endodontists with 1.41 (P = 0.000; 95% CI: 1.08–1.83) times higher adjusted odds of prescribing an opioid as compared with general dentists. Table 2 shows the adjusted odds ratios for all predictors included in the MLM model except for race.
Output from Multilevel Mixed Effects Logistic Regression for Opioid Prescribing.
Factors associated with antibiotic prescribing
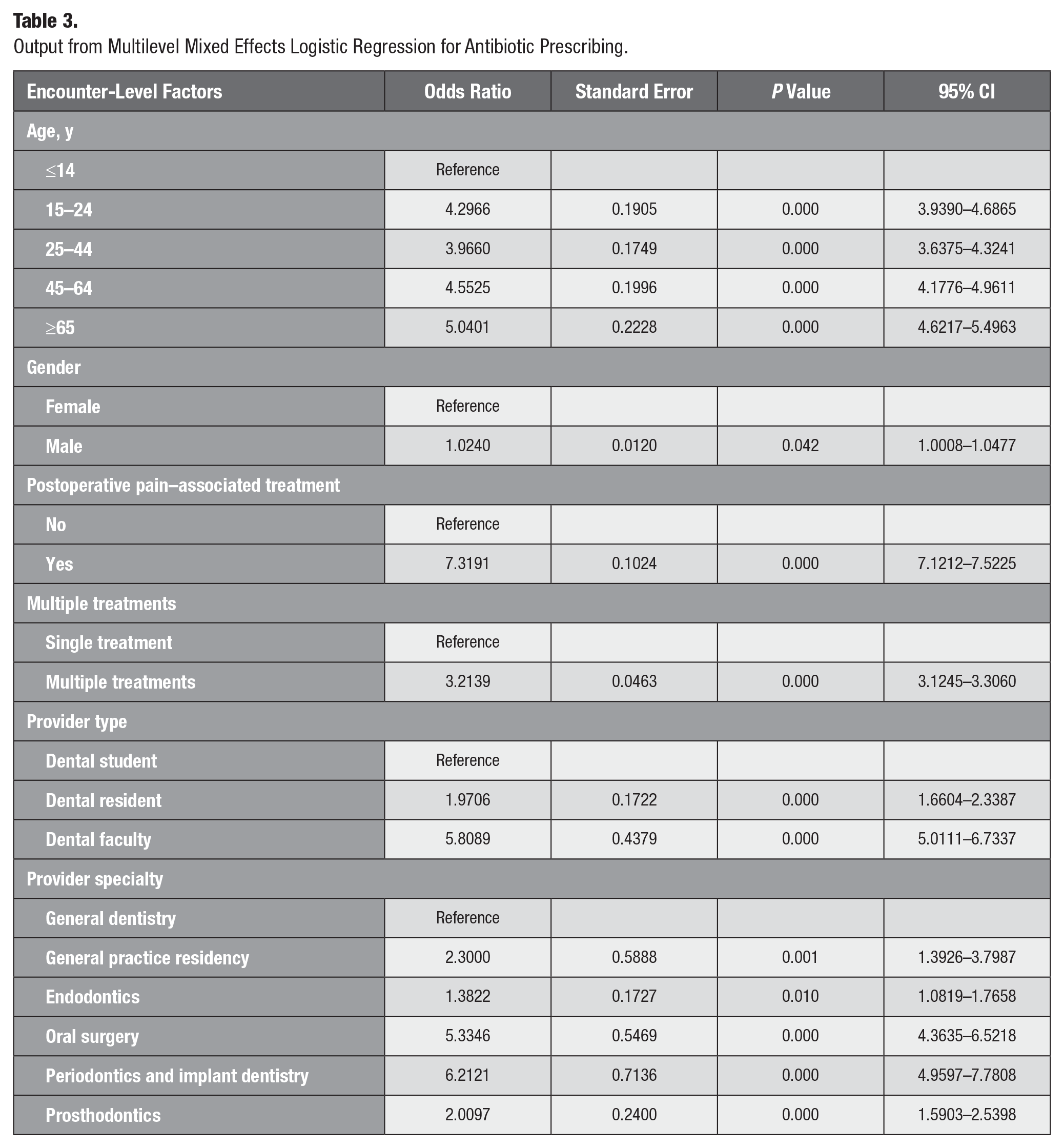
Table 3 shows that at the encounter level, all patient age categories had a statistically significant higher odds of being prescribed an antibiotic as compared with those patients from age category 0 to 14 y. Encounters that had at least 1 treatment associated with postoperative dental pain on the same day had a 7.32 (P = 0.000; 95% CI:7.12–7.52) times greater adjusted odds of being prescribed an antibiotic as compared with encounters that had no such treatment. In addition, encounters that had multiple treatments on the same day had a 3.21 (P = 0.000; 95% CI:3.12–3.31) times higher adjusted odds of an antibiotic prescription than those that had a single treatment. Encounters with dental faculty as the provider had a 5.81 (P = 0.000; 95% CI:5.01–6.73) times and encounters with dental residents as providers had 1.97 (P = 0.000; 95% CI: 1.66–2.34) times greater adjusted odds of an antibiotic prescription as compared with encounters in which the provider was a dental student. Encounters in which the provider belonged to the periodontics and implant dentistry specialty had a 6.21 (P = 0.000; 95% CI: 4.96–7.78) times higher adjusted odds, and those in which the provider was an oral surgeon had a 5.33 (P = 0.000; 95% CI: 4.36–6.52) times higher adjusted odds of an antibiotic prescription as compared with encounters in which the provider was a general dentist. The lowest odds of antibiotic prescribing among all specialists was seen in endodontists, with a 1.38 (P = 0.01; 95% CI:1.08–1.76) times greater adjusted odds of prescribing an antibiotic as compared with general dentists. Table 3 shows the adjusted odds ratios for all predictors included in the MLM model except for race.
Output from Multilevel Mixed Effects Logistic Regression for Antibiotic Prescribing.
Discussion
Analysis of data from 9 US institutions found that of all dental patient encounters that had at least 1 treatment procedure across the years 2011 to 2020, 2% had an opioid prescription and 2.7% had an antibiotic prescription. The decrease in opioid and antibiotic prescribing between 2015 and 2018 may be associated with increased awareness among dentists about prescribing of these medications, new or revised opioid and antibiotic prescribing guidelines (American Dental Association 2016; Dowell et al. 2016) that were published during this time, and the mandated use of prescription drug monitoring programs in specific institutions or US states. The increase in the prescribing of opioids and antibiotics in 2020 may be attributed to the dental clinical care regulations during the COVID-19 pandemic. Dentistry was noted to be the most at-risk profession associated with COVID-19 infection as compared with other occupations (Gamio 2020) owing to the clinically invasive, aerosol-generating nature of dental treatments and proximity of dental care providers to their patients during dental procedures. This concern and guidelines from Centers for Disease Control, Occupational Safety and Health Administration and American Dental Association led to clinics and dental institutions to limit care to patients needing emergency/urgent dental care with nonurgent dental care visits being postponed to limit the spread of COVID-19 until appropriate measures for minimizing this risk were known and available (Beltrán-Aguilar et al. 2021). We found that the number of dental treatment encounters was reduced and the number of opioid and antibiotic prescriptions increased in the year 2020, similarly noted in studies conducted in the United Kingdom (Thompson et al. 2022; Falola et al. 2023), to provide symptomatic relief from pain and to treat infection while there was an inability to provide timely dental care or to treat infections and pain that were a result of postponed or delayed dental care. Studies from other countries such as Scotland (Duncan et al. 2021) and Australia (Mian et al. 2021) found a similar increase in dental prescribing of these medications during the COVID-19 pandemic to manage acute dental conditions.
Twenty-two percent of all opioids and 23% of schedule II opioids were prescribed to 15- to 24-y-olds, and this age group had a 5.26 times greater odds of receiving an opioid prescription at a dental treatment visit. Another study found that dental opioid prescriptions for 11- to 18-y-old children and adolescents increased from 99.7 to 165.9 per 1,000 dental patients between 2010 and 2015 (Gupta et al. 2018b), and dentists prescribed 25% of first opioids in this age group (Gupta et al. 2018a). A dental visit might be the first opioid exposure for adolescents/young adults, typically after the extraction of third molars, and can create a source of unused opioids for later use or others to use. This is concerning because it is known that opioid-naïve adolescent/young adult patients whose first exposure to opioids was through a dentist had higher rates of opioid use after 90 to 365 d and subsequent diagnoses associated with opioid abuse or overdose (Schroeder et al. 2019). Further research specific to patients receiving opioid medications, especially those in the age group of 15 to 24 y, is necessary to study the type/dose/quantity of opioid prescribed, whether it was their first opioid medication, and whether there were any leftover pills that could create a source of unused opioids for future use and to understand their postoperative pain experience to inform safer prescribing. We found a higher odds of antibiotic prescribing in those aged 65 y and older, followed by 45- to 64-y-olds, which could include those who have had prosthetic joint replacement surgeries and certain cardiac conditions that may require prophylactic antibiotic prescriptions. Further research investigating the guideline concordance of these prescriptions is needed to determine whether the prescribing of these medications is truly warranted or is excessive and inappropriate.
Most (91%) opioid and (70%) antibiotic prescriptions were associated with dental procedures accompanied by postoperative dental pain owing to surgical manipulation of gingival, periapical tissues, bone, or perforation of oral mucosa. This is similar to other studies in which the authors found that 88.7% (US Military Health Systems study: 2008–2017; Richard et al. 2021) and 82.8% (US publicly and privately insured patients: 2013–2018; et al. 2021) of dental opioid prescriptions were for surgical procedures such as extraction, alveoplasty, endodontic therapy, and implant procedures. In a study conducted using claims data between 2009 and 2015, the authors found that 90.7% of dental visits with antibiotic prophylaxis involved some type of gingival manipulation and/or mucosal incision (Suda, Calip, et al. 2019). Although there is some evidence from past research (Suda, Calip, et al. 2019; Suda et al. 2020) during the years 2011 to 2015 on the appropriateness of these prescriptions, further research identifying the guideline concordance of these prescriptions, based on the dental procedures and recently published guidelines, is needed to determine the extent of excessive/inappropriate prescribing of these medications.
This study found greater odds of opioid and antibiotic prescribing by dental specialists as compared with general dentists. Among all specialists (excluding pediatric dentistry and orthodontists), oral surgeons and providers from the specialty periodontics and implant dentistry had greater odds and endodontists had the least odds of prescribing opioids and antibiotics. A study by Durkin et al. (2019) had similar findings wherein oral and maxillofacial surgeons prescribed the most antibiotics, followed by periodontists and endodontists. While much research has not been done to compare prescribing between dental specialties, understanding the factors leading to this increase in prescribing, specifically by periodontists and oral surgeons, is imperative. Our findings, along with those seen in other studies, indicate the need for future research to understand the factors associated with this prescribing behavior and implement dental specialty–specific ways to decrease prescribing.
This study provided updated estimates and demonstrated trends in prescribing to add new knowledge about dental specialty–specific prescribing rates. This is a timely topic of great public health significance. It addressed the need to understand factors associated with prescribing of these medications (Suda, Durkin, et al. 2019). The key strengths of this study include the improved precision of estimates and the ability to conduct meaningful analyses in subgroups stemming from advantages of using a large dataset (Ehrenstein et al. 2017). The findings from this research are impactful due to the advantages of using data from an EDR, which is the primary location and legal record of accurately structured treatment and prescription data in a standardized format. This ensures that the findings are evidence based, without any manipulation of data. The strengths of this research from an epidemiologic perspective are that such data minimize selection bias, increase external validity, have minimal reporting bias, and are replicable and reproducible. While the study mapped and classified missing data points for variables such as provider type and specialty based on other data fields available in the EDR, such as the provider’s title/role, it was unable to handle the large proportion of missing data for the race variable because it was never entered in the system and there was no proxy data field. Future studies could include prescription-associated medical conditions, diagnoses, and the presence of infection to study the reasons for prescriptions and over-/underprescribing of these drugs based on the published guidelines and evidence. The findings are limited to opioid and antibiotic prescribing in 9 US academic dental settings, which may be influenced by institutional factors as well, such as academic institution–specific prescribing processes, workflows, policies, and recommendations, which were not accounted for in this study. The findings may differ in private dental clinics and dental hospital settings.
Conclusion
Both opioid and antibiotic prescribing rates by dentists at US academic dental institutions declined between 2013 and 2018 but increased in 2020. There are significant differences in opioid and antibiotic prescribing by dentist specialty, with providers from oral surgery, general practice residency, and periodontics and implant dentistry having higher prescribing rates and greater odds of prescribing, while endodontists had a lower odds of prescribing as compared with other specialties and general dentists. The findings of this research have identified trends and factors associated with opioid and antibiotic prescribing in dental academic settings in the United States, which could lead to predicting and preventing future prescriptions and the tailoring of interventions that will reduce the prescribing of these medications.
Author Contributions
S. Tungare, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; A.-I. Yansane, contributed to conception, design, data analysis and interpretation, critically revised the manuscript; S. Gantela, K.K. Kookal, contributed to design, data acquisition and analysis, critically revised the manuscript; S. McCurdy, M. Krause, S. Sharma, contributed to conception and design, critically revised the manuscript; M. Walji, contributed to conception, design, data acquisition, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jct-10.1177_23800844251320335 – Supplemental material for Factors Associated with Opioid and Antibiotic Prescribing at US Academic Dental Institutions: 2011 to 2020
Supplemental material, sj-docx-1-jct-10.1177_23800844251320335 for Factors Associated with Opioid and Antibiotic Prescribing at US Academic Dental Institutions: 2011 to 2020 by S. Tungare, A.-I. Yansane, S. Gantela, K.K. Kookal, S. McCurdy, T.M. Krause, S. Sharma and M. Walji in JDR Clinical & Translational Research
Footnotes
Acknowledgements
Data for this research were obtained from the BigMouth Dental Data Repository. The authors thank the BigMouth Dental Data Repository team for providing the data and support in data management. The authors thank Dr. Katie Suda, an expert in the field of dental antibiotic and opioid prescribing and a leading figure in the field of dental antibiotic stewardship, for her guidance in this research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.