
Abstract
Background:
Oral health is an integral aspect of overall well-being and quality of life. Population groups such as two-spirit, lesbian, gay, bisexual, transgender, and queer, including other sexual and gender minorities (2SLGBTQ+), have reported poor oral health outcomes. Therefore, the aim of this review was to investigate the extent and scope of the literature describing 2SLGBTQ+ oral health outcomes, including unmet oral health needs and patterns of oral health care service utilization, as well as the risk factors affecting both.
Methods:
A comprehensive search strategy was developed to review the scope of the literature pertinent to unmet oral health needs and factors affecting access to oral health care among 2SLGBTQ+ members, globally. In total, 6 databases were searched with a combination of keywords relevant to 2SLGBTQ+ oral health status and oral health care utilization.
Results:
Our review identified 10 studies that met the eligibility criteria. Five out of 10 studies were based in India, 4 in the United States, and 1 in Brazil. Two studies reported poorer oral health outcomes among transgender people as compared with cisgender people, while 2 studies reported similar patterns of dental service utilization between their transgender and cisgender participants. Five studies explored the personal and structural risk factors associated with poor oral health outcomes, including financial affordability and income level and perceived discrimination, including instances of misgendering in health care settings. However, further comprehensive studies must be conducted to validate the trends and findings reported by the studies in the review and to generate data from diverse regional contexts.
Conclusions:
Our review identified that the extent of the literature in this research area is sparse and scarce. The evidence indicates poorer oral health status among 2SLGBTQ+ communities. Wider studies with diverse, representative samples are required to gain a comprehensive understanding of 2SLGBTQ+ oral health outcomes.
Knowledge Transfer Statement:
The results of this review will undoubtedly be important for many years to come as 2SLGBTQ+ oral health equity is prioritized by experts in public health dentistry. This review will allow other researchers to understand and fill literature gaps regarding 2SLGBTQ+ oral health outcomes, furthering this area of research.
Keywords
Background
The 2SLGBTQ+ community includes those who identify as two-spirit, lesbian, gay, bisexual, transgender, queer, or choose to identify with another related or adjacent term (Schreiber et al. 2021). According to the Insitut Public de Sondage d’Opinion Secteur’s (IPSOS) LGBT+ Pride 2021 Global Survey (Boyon 2021), approximately 2% of those surveyed identified as gender nonconforming, which includes transgender and nonbinary people. Transgender people are those whose gender identities do not match their sex assigned at birth—including nonbinary people (GLAAD 2021). Terms such as gay and lesbian have been used to refer to men and women, respectively, who are attracted to the same gender, and two-spirit is a term commonly used among Indigenous communities to describe someone “whose behaviors or beliefs may be interpreted by others to be uncharacteristic of their sex” (Jacobs et al. 1997).
The 2SLGBTQ+ community experiences greater social, environmental, and physical barriers to health care that lead to health disparities, including higher rates of mental health concerns such as anxiety and depression (Rainbow Health Ontario 2020; Schreiber et al. 2021). Stigma and discrimination are significant barriers to health care experienced by 2SLGBTQ+ individuals, especially gender-diverse people (Bauer and Scheim 2015; Schwab et al. 2022). For instance, transgender people are likely to experience strong resistance to social inclusion and high rates of prejudice and discrimination as a result of their gender identity (Rainbow Health Ontario 2020). In certain cases, it is necessary for 2SLGBTQ+ people to hide their identity to receive adequate care without feeling belittled or stigmatized (Schwab et al. 2022).
Substance use and abuse are also issues of note for 2SLGBTQ+ community members. A 2020 survey suggested that self-reported substance use patterns differ significantly between sexual minority adults, as compared with heterosexual adults (Substance Abuse and Mental Health Services Administration 2020). Additionally, 2SLGBTQ+ people are particularly at risk for HIV infection (HIV.gov 2022). Jessani et al. (2021) found that injection drug use and HIV infection were significantly associated with decayed teeth and that the odds of having decayed, missing, and filled teeth were twice as high for people living with HIV and hepatitis C virus (HCV) (Jessani et al. 2021).
The burden of oral health diseases is significant for 2SLGBTQ+ people, especially transgender people (Manpreet et al. 2021). For instance, a larger proportion of transgender people—compared to cisgender people—have reported experiencing oral ulcers, leukoplakia, nicotinic stomatitis, or an oral malignancy (Manpreet et al. 2021). Most of these individuals were also reported as having dental caries, poor oral hygiene, or periodontal disease (Marlecha et al. 2020). Furthermore, when compared on the decayed, missing, and filled teeth (DMFT) index, transgender people consistently scored significantly higher—signifying poorer oral health—than their cisgender counterparts, and transgender people report being largely unsatisfied with their oral health quality (Manpreet et al. 2021; Prates et al. 2021).
In addition to the burden of untreated oral diseases, 2SLGBTQ+ people face social barriers specific to the context of dental offices; for instance, some have reported experiencing stigma and discrimination due to their gender identity while accessing dental care services, consequently avoiding future dental visits (Macdonald et al. 2019).
With this context in mind, the aim of this scoping review was to investigate the extent of the literature regarding 2SLGBTQ+ oral health status and barriers to oral health care service utilization globally. The specific objectives were to investigate the 1) scope of the current literature regarding the unmet oral health treatment needs of the 2SLGBTQ+ community, 2) scope of current literature regarding oral health care utilization by 2SLGBTQ+ people, and 3) personal and structural risk factors reported in the literature that affect unmet oral health needs and access to oral health services for 2SLGBTQ+ people.
Methods
The Joanna Briggs Institute (JBI) Reviewers Manual was employed as a reference due to its methodological approach to scoping reviews (Aromataris and Munn 2020). The JBI Manual provides guidelines for authors to follow, with separate chapters focused on the synthesis of different types of evidence, for various types of review questions (Aromataris and Munn 2020). The manual was employed as a reference tool to clarify questions regarding the scoping review process; chapters 11.1, 11.2, and 11.3, named “Introduction to Scoping Reviews,” “Development of a Scoping Review Protocol,” and “The Scoping Review and Summary of the Evidence,” respectively, were consulted prior to registering the protocol to ensure our methods were sound. It was on the recommendation of the JBI Manual to register the scoping review protocol with the Open Science Framework—detailed below—given that PROSPERO has noted scoping reviews are ineligible for registration in their database (Aromataris and Munn 2020).
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) reporting guidelines for this review (Tricco et al. 2018; Page et al. 2021); a completed PRISMA-ScR checklist has been included as Supplement 1.
A protocol for this scoping review was registered prior to beginning study screening in the Open Science Framework (doi.org/10.17605/OSF.IO/AJE89). The preregistered protocol details pertinent information regarding selection criteria, as well as the data extracted from the included publications. This was done to ensure maximal transparency in the scoping review process and to demonstrate that our original intention with the scoping review matched our methodology.
Inclusion Criteria
This review sought studies that reported on the oral health status and patterns of oral health care utilization and access of 2SLGBTQ+ individuals. The relevant study population included 2SLGBTQ+ people with any oral health status or oral health care outcome. English-language papers from any global context were included, with no date restrictions applied. All study designs, including qualitative, quantitative, and mixed methods, were included in this review. Both peer-reviewed publications and gray literature were considered.
Exclusion Criteria
When reviewing publications during screening, the following criteria were used to exclude studies:
Focus not relevant to study objectives—studies that do not discuss the oral health status of 2SLGBTQ+ individuals and their patterns of oral care utilization
Outcomes not relevant to study objectives—studies that do not report oral health or oral care utilization outcomes
Language—studies written in a language other than English
Full-text unavailable—studies without their full-text available online
Search Strategy
The search strategy was developed by I.F. and A.J.—in consultation with T.T. and a research librarian—with the purpose of identifying literature pertaining to the oral health status of 2SLGBTQ+ community members, as well as their patterns of oral health care service utilization and access. This includes both published and unpublished, gray literature; gray literature was identified from the Global Dissertations and Theses database using the same search strategy as the other databases, adjusting the search format based on the mechanics of the database. The searches for all literature were conducted on March 25, 2023, thereby including literature published until this date; Google Scholar was search on March 21, 2023, during the time when the search strategy for the other databases was being finalized. The key concepts and related search terms are included in Table 1. The databases searched were Medline, Embase, Scopus, CINAHL, Google Scholar, and Dissertations & Theses Global (ProQuest). For a detailed view of our search strategy, refer to Appendix A.
Key Concepts and Relevant Search Terms.
Reference Management
Full references were imported from each database search into Covidence (2023), which was used to remove duplicate results. All remaining references entered a 2-stage screening process: title and abstract screening followed by full-text screening. All publications’ full texts were found online, and thus no communication with authors of the reviewed studies was necessary.
Study Screening
Two stages of screening were used to identity relevant studies. The first stage of screening reviewed only the titles and abstracts of the articles and was completed by one reviewer (I.F.). The second stage was full-text review, which was conducted by 2 independent reviewers (I.F. and A.J.). Disagreements between reviewers were resolved via discussion.
Data Extraction
A standardized data extraction tool (Appendix B) was developed to compare relevant information between the included studies. The data extraction tool was piloted on 15% of the included studies and then refined to ensure that all relevant data were extracted. All amendments have been included in the refined version of the data extraction tool (Appendix C). The data extraction was completed and verified by I.F.
Data Analysis
The extracted data were exported from Covidence to a Microsoft Excel file and reviewed for any discrepancies with the information reported in the study manuscripts. The data were then imported to SAS 9.4 (SAS Institute 2013), which was used to perform descriptive analysis of the extracted study characteristics.
Risk of Bias Assessment of Included Studies
Although scoping reviews do not tend to assess the risk of bias of included studies, we believed it to be valuable for our purposes given the lack of robust study designs, to understand the quality of the evidence presented by the included studies. The included studies were assessed for their risk of bias using the CLARITY Group’s Risk of Bias Instrument for Cross-Sectional Surveys of Attitudes and Practices (CLARITY Group at McMaster University 2021). The instrument was chosen for its simplicity to understand as well as its ability to provide a broad summary based on 5 domains; the completed risk of bias instrument has been included as Supplement 2.
Results
Search Results
Our search results and screening process are detailed in the Figure. The search strategy yielded 138 articles: Medline (n = 23), Embase (n = 32), Scopus (n = 14), CINAHL (n = 43), Google Scholar (n = 3), and ProQuest (Dissertations & Theses Global) (n = 23). Following the removal of 33 duplicate results, 105 studies underwent title and abstract screening. Of these, 87 studies were excluded, leaving 18 to undergo full-text review. The full-text review flagged 8 studies that were excluded because they did not report explicitly on oral health status or oral health care service utilization and access-related outcomes. The remaining 10 studies were included in our review; refer to Appendix D for a list of included studies. The 10 studies then underwent data extraction.
Flow diagram of study selection. Adapted from Tricco et al. (2018). For more information, visit http://www.prisma-statement.org/.
Description of Included Studies
The data extracted from the included studies have been summarized in Table 2. Studies originated from India (n = 5) (Samuel et al. 2018; Marlecha et al. 2020; Prasanth et al. 2020; Manpreet et al. 2021; Kumar and Rai 2022), the United States (n = 4) (Schwartz et al. 2019; Adekugbe 2020; Raisin 2021; Ramos et al. 2021), and Brazil (n = 1) (Prates et al. 2021). All studies were published during or after 2018. Five studies (Samuel et al. 2018; Marlecha et al. 2020; Prasanth et al. 2020; Ramos et al. 2021; Kumar and Rai 2022) included a sample composed entirely of self-identifying transgender participants, and 3 (Adekugbe 2020; Manpreet et al. 2021; Prates et al. 2021) included both transgender and cisgender participants. Most studies (n = 6) (Samuel et al. 2018; Marlecha et al. 2020; Prasanth et al. 2020; Manpreet et al. 2021; Ramos et al. 2021; Kumar and Rai 2022) did not report on the race or ethnic status of participants included in their sample. Further, only 2 studies (Schwartz et al. 2019; Adekugbe 2020) included a breakdown of self-reported sexual orientation. All studies were observational in design (n = 10) (Samuel et al. 2018; Schwartz et al. 2019; Adekugbe 2020; Marlecha et al. 2020; Prasanth et al. 2020; Manpreet et al. 2021; Prates et al. 2021; Raisin 2021; Ramos et al. 2021; Kumar and Rai 2022). Commonly used sampling methods included convenience sampling (n = 4) (Samuel et al. 2018; Marlecha et al. 2020; Manpreet et al. 2021; Prates et al. 2021), snowball sampling (n = 2) (Prasanth et al. 2020; Kumar and Rai 2022), and voluntary sampling (n = 4) (Schwartz et al. 2019; Adekugbe 2020; Raisin 2021; Ramos et al. 2021). Four studies (Marlecha et al. 2020; Prasanth et al. 2020; Manpreet et al. 2021; Prates et al. 2021) included fewer than 100 participants, 4 (Samuel et al. 2018; Raisin 2021; Ramos et al. 2021; Kumar and Rai 2022) included between 100 and 400 participants, and 2 (Schwartz et al. 2019; Adekugbe 2020) included greater than 400 participants. Two studies (Adekugbe 2020; Raisin 2021) were unpublished, gray literature; both were master’s degree theses.
Included Study Characteristics and Findings.
CI, confidence interval; FTM, female-to-male; LGBTQ+, lesbian, gay, bisexual, transgender, queer; MTF, male-to-female; OR, odds ratio; SD, standard deviation; SE, standard error.
Proportion of transgender group.
Proportion of cisgender group.
Reported P value is for difference in proportion distribution between transgender and cisgender groups.
Reference is cisgender.
Reference is non-LGBTQ+, heterosexual.
Table 2 also includes information regarding the oral health status of participants. Seven studies (Samuel et al. 2018; Schwartz et al. 2019; Marlecha et al. 2020; Prasanth et al. 2020; Manpreet et al. 2021; Ramos et al. 2021; Kumar and Rai 2022) report the current oral health outcomes of participants, assessed objectively, whereas 3 (Adekugbe 2020; Prates et al. 2021; Raisin 2021) report self-perceived oral health status of study participants.
Of the 7 studies that reported clinical oral health outcomes, 4 (Samuel et al. 2018; Schwartz et al. 2019; Manpreet et al. 2021; Kumar and Rai 2022) reported overall DMFT index scores, with 3 also reporting the individual component scores of the DMFT index (i.e., number of decayed teeth, missing teeth, and filled teeth) (Samuel et al. 2018; Manpreet et al. 2021; Kumar and Rai 2022). The mean number of decayed teeth reported among transgender participants ranged between 1.40 and 4.60 teeth, the mean number of missing teeth ranged between 0.18 and 2.74 teeth, and the mean number of filled teeth ranged between 0.08 to 0.85 teeth (Samuel et al. 2018; Manpreet et al. 2021; Kumar and Rai 2022). Finally, 1 study reported that 73.60% of their sample of transgender participants had at least 1 cavity; furthermore, 58.60% and 47.10% had experienced a painful or decayed tooth during their lifetime respectively (Marlecha et al. 2020).
Two studies (Manpreet et al. 2021; Prates et al. 2021) compared transgender and cisgender groups, revealing poorer oral health status among transgender participants. Manpreet et al. (2021) reported that among transgender participants, the prevalence of oral ulcers, leukoplakia, and nicotinic stomatitis was 15.00%, 20.00%, and 27.50% respectively; among cisgender participants, these were 12.50%, 0.00%, and 20.00% respectively. Furthermore, Prates et al. (2021) examined self-perceived differences in dental treatment needs, reporting that 77.80% of transgender participants felt that they required dental treatment, whereas only 53.50% of cisgender participants reported the same (P = 0.026). The same study (Prates et al. 2021) also reported that 13.30% of transgender participants feel that they require dental prosthesis, whereas only 2.20% of cisgender participants report the same (P = 0.110). Comparisons between transgender and cisgender individuals are important for understanding specific differences that may have arisen due to differences in gender identity.
Periodontal health was also of concern among the studies examined. Two studies (Manpreet et al. 2021; Kumar and Rai 2022) reported outcomes based on the Community Periodontal Index (CPI) (Dhingra and Vandana 2011), and 1 study reported the Community Periodontal Index for Treatment Needs (CPTIN) (Prasanth et al. 2020). For example, Kumar and Rai (2022) reported the following based on their sample of transgender people: healthy periodontium (10.46%), bleeding only (37.91%), shallow pathological pocket (i.e., 4–5 mm) (28.10%), and deep pathological pocket (i.e., >6 mm) (23.53%). Another study—Prasanth et al. (2020)—reported similar findings as Kumar and Rai (2022) from their sample of 75 transgender participants, revealing that very few participants had a healthy periodontium (10.70%), while the majority of the participants showed various signs of periodontal disease (bleeding on probing: 17.30%; presence of calculus: 22.70%; shallow pathological pockets: 17.30%; and deep pathological pockets: 32.00%).
Our review found that while several studies have sought to understand the oral health status and treatment needs of 2SLGBTQ+ populations, the evidence is sparse with significant variation between the outcomes and findings reported. For instance, certain studies tend to focus on tooth health, reporting measures such as the DMFT index (Samuel et al. 2018; Schwartz et al. 2019; Manpreet et al. 2021; Kumar and Rai 2022), and some focus upon periodontal health, reporting the CPI or CPTIN indices (Prasanth et al. 2020; Manpreet et al. 2021; Kumar and Rai 2022). Additional comprehensive studies are needed to explore the diverse oral health outcomes of 2SLGBTQ+ people, preferably providing an objective and expert assessment of both tooth and periodontal health.
The findings reported by each study regarding oral health service utilization have been included in Table 2; 8 of the 10 studies reported findings for this objective (Samuel et al. 2018; Schwartz et al. 2019; Adekugbe 2020; Marlecha et al. 2020; Prasanth et al. 2020; Prates et al. 2021; Raisin 2021; Ramos et al. 2021). Two studies reported the reason for dentist visit (Adekugbe 2020; Marlecha et al. 2020), and 6 studies reported patterns of past oral health care utilization (Samuel et al. 2018; Adekugbe 2020; Marlecha et al. 2020; Prates et al. 2021; Raisin 2021; Ramos et al. 2021).
For instance, Marlecha et al. (2020) cited that transgender individuals accessing dental care did so due to tooth pain (30.00%), teeth becoming loose (25.70%), bleeding from gums (12.90%), or for a routine appointment (31.40%). Similarly, Adekugbe (2020) reported 19.40% of participants visit the dentist when they have a dental issue, 70.90% visit routinely, 6.20% cited other reasons, and 0.70% have never visited the dentist.
Regarding patterns of oral health care utilization, most studies (n = 6) (Samuel et al. 2018; Adekugbe 2020; Marlecha et al. 2020; Prates et al. 2021; Raisin 2021; Ramos et al. 2021) inquired about the frequency of dental care visits. For instance, 2 studies (Adekugbe 2020; Prates et al. 2021) reported results depicting that transgender and cisgender participants did not differ significantly in their patterns of dental service utilization.
Certain studies addressed only transgender participants specifically. Marlecha et al. (2020) reported that 60.00% of transgender participants had never visited the dentist, while Samuel et al. (2018) reported that 95.30% of transgender participants had not visited the dentist within the past 3 y. Such findings reveal significant shortcomings in existing dental service provision, such that certain studies (Samuel et al. 2018; Marlecha et al. 2020) identified problematic patterns of dental care utilization for transgender people.
Furthermore, Ramos et al. (2021) report the recency of dental care visits, reporting that 59.60% of their sample of men who have sex with men had visited the dentist within the past year; however, 40.40% visited more than 2 y prior. Finally, Raisin (2021) recorded the number of dental visits within the past year: none (43%), 1 (25%), 2 (19%), and 3 or more (13%). The aforementioned findings reveal stark differences in dental service utilization, emphasizing the importance of identifying factors which contribute to extreme differences in dental care access.
In total, 5 (Samuel et al. 2018; Adekugbe 2020; Marlecha et al. 2020; Raisin 2021; Ramos et al. 2021) of the included studies addressed either personal or structural risk factors. With respect to personal risk factors, 2 studies reported related items (Adekugbe 2020; Ramos et al. 2021). Having a higher income (i.e., dichotomized as greater than or less than $25,000) was associated with greater odds of having positive self-reported oral health status, whereas being transgender—as compared with being cisgender—was associated with lower odds of positive self-reported oral health status (Adekugbe 2020).
Ramos et al. (2021)—a study based in the United States—identified 4 variables that affected participants’ most recent dental visit, including employment status, education, income, and dental insurance coverage. A statistically significant difference was identified between the distribution of participant answers regarding the aforementioned 4 variables, comparing those reporting that they had visited the dentist within the past year and those having visited more than 2 y prior (Ramos et al. 2021). Self-perceived general health was also significantly correlated with dental visits, with those who visited the dentist within the past year having a significantly higher mean self-reported general health score, as compared with those having visited the dentist greater than 2 y prior (Ramos et al. 2021).
Regarding structural risk factors, 4 studies reported structural risk factors such as discrimination from dental care staff or being misgendered in health care settings; these articles included those from India and the United States (Samuel et al. 2018; Adekugbe 2020; Marlecha et al. 2020; Raisin 2021). Adekugbe (2020)—a study from the United States—identified 2 domains for which they collected information regarding structural factors that impact oral health. The 2 domains were experiences of discrimination and training of dentists regarding 2SLGBTQ+ health (Adekugbe 2020). Their findings indicated that 15.00% of participants had experienced discrimination in a dental care setting based on their gender identity, and 11.40% reported a past experience of discrimination based on sexual orientation (Adekugbe 2020). Almost half of the sample indicated it was very important for dentists to be trained on 2SLGBTQ+ issues (Adekugbe 2020). Raisin (2021) compared the expectations and the experiences of transgender participants while accessing dental care. Ninety-three percent of participants believed it was important to see a nondiscrimination policy regarding gender identity at dental clinics, but 60.00% reported never having seen such a policy (Raisin 2021). Furthermore, almost all participants reported expecting to be addressed by their correct pronouns when at a dental office, but 63.00% reported having been misgendered while accessing dental care in the past (Raisin 2021).
Finally, Marlecha et al. (2020)—a study from India—found that 54.30% of transgender people in their sample felt neglected in society, and 77.10% felt government intervention was necessary to help them improve their overall oral health. Another study from India, Samuel et al. (2018), reported that 60.50% of participants did not access dental care due to perceived nonadmittance, 35.80% for economic reasons, and 3.70% for another reason. As such, it is important to note that anti-2SLGBTQ+ discrimination can be experienced in many regional contexts, including both the United States and India.
Risk of Bias Assessment
The risk of bias assessment conducted using the CLARITY Group’s Risk of Bias Instrument for Cross-Sectional Surveys of Attitudes and Practices (2021) highlighted differences between studies in terms of the reliability of the results reported. Of the 10 included studies, 5 (Samuel et al. 2018; Adekugbe 2020; Marlecha et al. 2020; Raisin 2021; Kumar and Rai 2022) exhibited high risk of bias in at least one of the domains contained in the instrument. However, all studies (n = 10) (Samuel et al. 2018; Schwartz et al. 2019; Adekugbe 2020; Marlecha et al. 2020; Prasanth et al. 2020; Prates et al. 2021; Manpreet et al. 2021; Raisin 2021; Ramos et al. 2021; Kumar and Rai 2022) exhibited low risk of bias in the domain pertaining to response rate. Finally, 3 studies (Prasanth et al. 2020; Prates et al. 2021; Ramos et al. 2021) exhibited moderate to low risk of bias overall. The risk of bias assessment has been summarized in Table 3, color-coded with green representing low risk of bias and red representing high risk of bias.
Ratings of Included Cross-Sectional Studies Using CLARITY Group’s Risk of Bias Instrument for Cross-Sectional Surveys of Attitudes and Practices.
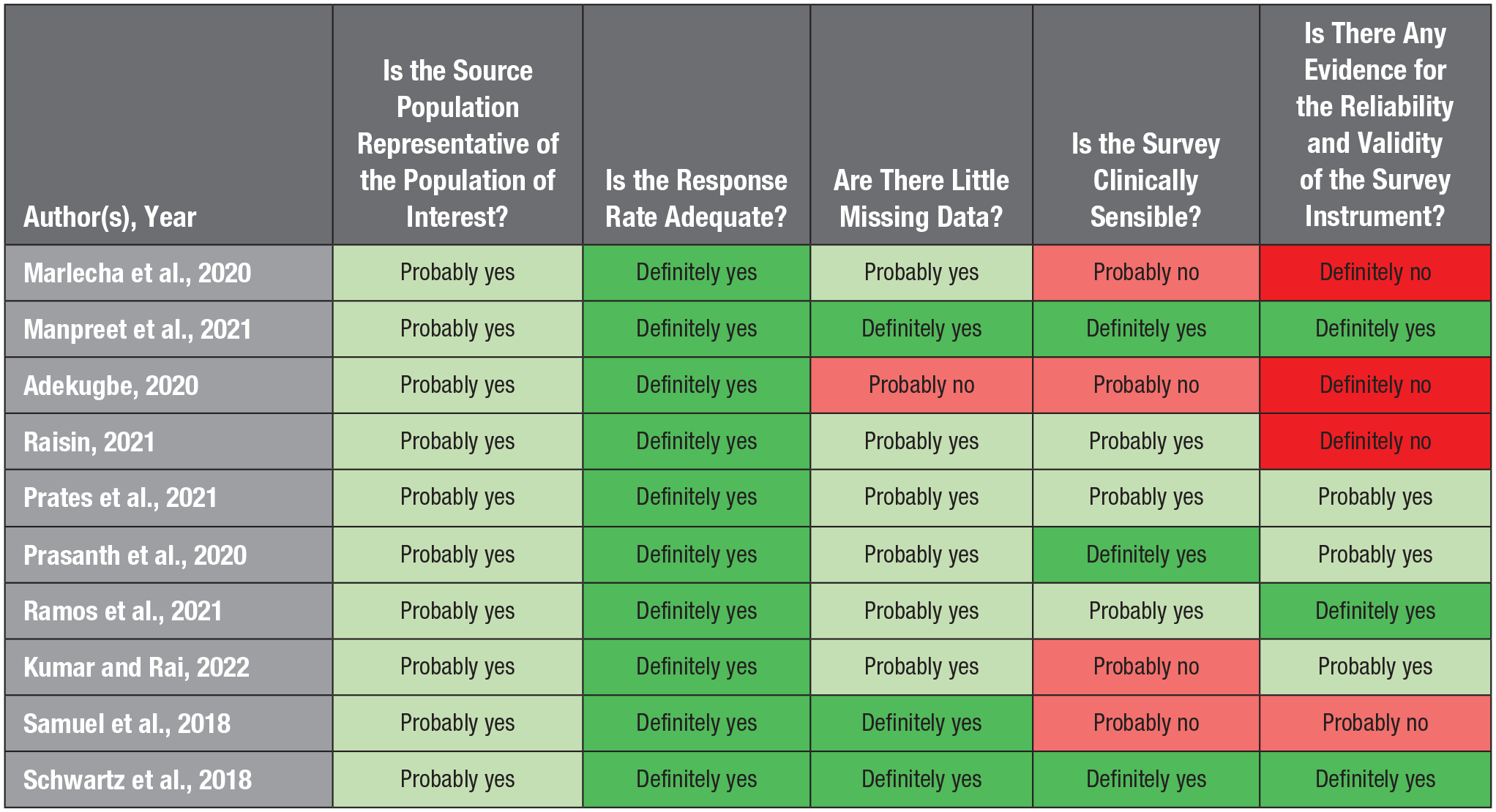
Green is indicative of low risk of bias and red is indicative of high risk of bias.
Discussion
This review aimed to identify the scope of literature regarding the unmet oral health treatment needs and oral health service utilization on 2SLGBTQ+ community members globally. Although research and advocacy regarding 2SLGBTQ+ health has grown in recent years, much work is necessary to achieve health equity for 2SLGBTQ+ people; existing laws and policies pertaining to sexual and gender minorities also impact the journey to achieving health equity (MacCarthy et al. 2015; ILGA World 2023). To date, homosexuality is still forbidden by law in 62 countries around the world and punishable by death in 11 countries (ILGA World 2023). According to a 2019 report by the International Lesbian, Gay, Bisexual, Trans and Intersex Association (ILGA), 37 countries possess laws that criminalize transgender people, with 11 countries explicitly banning transgender identities de jure (ILGA World 2019). Therefore, it is unsurprising that most of the health service research regarding 2SLGBTQ+ people originates from countries where 2SLGBTQ+ individuals have legal rights and access to health care. However, laws and policies do not always protect these community members against inherited heretics and discrimination (Clark 2014). Therefore, 2SLGBTQ+ individuals have reported greater proportions of health care challenges and needs than their non-2SLGBTQ+ counterparts (Hafeez et al. 2017). Most commonly reported health care challenges include higher rates of mental illnesses, including anxiety, depression, and substance abuse, with these health outcomes worsening for transgender subpopulations (Rainbow Health Ontario 2020).
Oral health research for 2SLGBTQ+ people has only recently begun to gain prominence, as the first study was published on this topic in 2018 (Samuel et al. 2018). This is likely indicative of growing interest in 2SLGBTQ+ oral health as an area of oral public health research. Although a scoping or systematic review has not been conducted on this topic before, it is unsurprising that India and the United States contribute the majority of studies on this topic, given the long history of transgender people within the Indian subcontinent and US efforts to foster 2SLGBTQ+ health research (Goel 2016; Bonvicini 2017).
Our results identified poorer oral health outcomes for 2SLGBTQ+ populations—namely, that 2 of 10 studies reported poorer oral health among transgender participants via direct comparison with cisgender participants (Manpreet et al. 2021; Prates et al. 2021). Moreover, our studies identified significantly higher self-perceived treatment need among transgender participants versus cisgender participants, with transgender people having a significantly higher prevalence of oral health conditions, including oral malignancies and ulcers (Manpreet et al. 2021). Such findings underscore the importance of understanding why 2SLGBTQ+ oral health outcomes are overwhelmingly poor in the limited existing literature. These findings are suggestive of several personal and structural risk factors that contribute to these oral health needs; Kia et al. (2021) explained that 2SLGBTQ+ community members face several psychosocial disparities such as housing crises, unstable sources of income, and barriers to education, including personal and structural factors as identified by our third objective. These personal and structural risk factors can have a significant impact on oral health outcomes. For structural barriers, our results highlighted that social exclusion and isolation played a key role in access to health care services—including oral health care utilization—leading to more treatment needs (Manpreet et al. 2021; Prates et al. 2021). This was due in part to discrimination experienced previously in oral health care settings, as well as perceived or expected isolation due to social exclusion (Manpreet et al. 2021; Prates et al. 2021). Similarly, lack of gender-sensitivity training and trauma-informed care, as well as experiences of discrimination within the health care system, has been reported to further diminish the trust and consequently utilization of health care services by marginalized populations, including 2SLGBTQ+ people (Alencar Albuquerque et al. 2016).
Although having a publicly funded health care system—such as in Canada—can be a positive influence on the utilization of health care services, this is not always the case with 2SLGBTQ+ people (Giblon and Bauer 2017). Giblon and Bauer (2017) revealed that transgender men are significantly more likely to report requiring health care in the past year but not receiving it, as compared with cisgender men. Similarly, a lack of understanding of the unique challenges and needs of 2SLGBTQ+ community members may inhibit their utilization of dental care service (Adekugbe 2020; Raisin 2021). Similar findings were reported by Schwab et al. (2022) in Saskatchewan, Canada, where 2SLGBTQ+ members reported lack of cultural sensitivity and empathy while accessing local health care services. Consequently, our review indicated that the 2SLGBTQ+ population accessed dental care more often for emergency reasons rather than for routine appointments (Elaine Muirhead et al. 2020). To address such lack of access to oral health care services, policymakers may consider subsidies that enable 2SLGBTQ+ people to access dental care: this is especially significant in regional contexts where oral or dental health care services are privately administered, meaning individuals pay for these services out of pocket or using private insurance, such as in the United States and Canada (Chari et al. 2022).
Stigma and discrimination are another set of factors that inhibit health care access and oral health service utilization for this population (Samuel et al. 2018; Raisin 2021). The 2SLGBTQ+ community members have reported being judged and mistreated by their health care providers, including by their family physician (Lee and Kanji 2017). Furthermore, about 25% of transgender people report feeling belittled by emergency medical staff (Bauer and Scheim 2015). This, compounded with the fact that approximately 21% of transgender people have chosen to avoid accessing emergency care when they needed it, speaks to the dangerous nature of antitransgender sentiment for the health of this community (Bauer and Scheim 2015). Schwab et al. (2022) reported 4 common themes derived from the experiences of 2SLGBTQ+ people with their health care providers, including perceived stigma in health care settings, health practitioners’ 2SLGBTQ+-specific knowledge, the need for 2SLGBTQ+ sensitivity training, and advocacy for health care policy reform. Such themes are important considerations for future health care best practices, given the potential impact it may have for increasing 2SLGBTQ+ health care utilization (Schwab et al. 2022).
In terms of study designs, all studies employed some form of nonrandom sampling, bringing into question the generalizability of the included studies’ findings. However, given the challenges with recruitment of marginalized populations, as well as the discrimination experienced by 2SLGBTQ+ community members, study participants may have otherwise been difficult to recruit (Gatlin and Johnson 2017; Sterzing et al. 2018). Gatlin and Johnson (2017) explain that the challenges of data collection within minority populations—such as the 2SLGBTQ+ community—include a lack of trust from the population for health-related research, a difficulty conveying the value of participation, and time constraints. When combined, a difficulty garnering interest in research participation and the time constraints that participation might present becomes a significant barrier to recruitment efforts, especially among 2SLGBTQ+ people (Gatlin and Johnson 2017). Therefore, strategies such as offering financial compensation for participants’ time, or employing community brokers who can help prospective participants understand the value of their participation as a marginalized person, should be introduced in the study design to target a larger sample population.
In summary, this review assessed the scope of the literature regarding the oral health status and patterns of oral health service utilization of 2SLGBTQ+ community members, determining that research is limited in amount. Future considerations must be given by oral health advocates for 2SLGBTQ+ populations, to ensure they are able to both access and derive benefit from oral health care services.
Given the limited geographic context of included studies, the findings cannot necessarily be generalized to other global settings. Furthermore, only 2 of the studies included a breakdown of participant-reported sexual orientation, and thus we were unable to generalize their findings to understand the experiences of all members of the 2SLGBTQ+ community. The employed search strategy also restricted results to only English-language papers, which is a limitation given we excluded any literature published in languages other than English; it should be noted, however, that the extent of this literature in languages other than English is unclear. Despite these limitations, this review provides a comprehensive scope of evidence available with regard to the unmet oral health needs of 2SLGBTQ+ community members, identifying gaps in the literature and providing direction for future research.
Conclusions
Our review concluded that the scope of literature with regard to the unmet oral health care need and patterns of oral health service utilization of 2SLGBTQ+ people is very limited, but the limited evidence showed poor oral health–related outcomes for 2SLGBTQ+ people. Studies lacked representation from diverse subgroups of 2SLGBTQ+ populations, particularly from two-spirit, nonbinary, and bisexual people. Thus, we require further robust, representative data to fully understand 2SLGBTQ+ oral health outcomes. Although some studies included validated scale measures (e.g., DMFT index) to report oral health status, our results also concluded a lack of robust research design, including insufficient sample size, and few reported clinical markers. Furthermore, risk of bias assessment revealed that as many as half of the included studies exhibit high risk of bias due to 1 or more components of their study design. Last, current evidence is insufficient for understanding the impact of outcomes such as race, socioeconomic status, and sexual orientation on oral health. Wider studies with representative samples and comprehensive information on sectoral and individual variables and their impact on oral health outcomes are indicated.
Author Contributions
I. Fakhrjahani, T. Tiwari, A. Jessani, contributed to conception, design, data analysis, drafted and critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jct-10.1177_23800844231206359 – Supplemental material for The Need for Comprehensive Analysis in Assessing Dental Caries Risk in HNC Patients after Radiotherapy
Supplemental material, sj-docx-1-jct-10.1177_23800844231206359 for The Need for Comprehensive Analysis in Assessing Dental Caries Risk in HNC Patients after Radiotherapy by S. Ghai in JDR Clinical & Translational Research
Footnotes
Acknowledgements
We thank Maren Goodman for her support and role in this review; she is the Teaching & Learning Librarian at Western Libraries who helped us refine our search strategy and identify helpful resources.
A supplemental appendix to this article is available online.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Not Applicable.
Availability of Data and Materials
All data collected and analyzed in this review are included in this articles and its appendices and supplements.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.