
Abstract
Background:
Previous studies have demonstrated a significant association between maternal oral health and pregnancy complications, including preterm birth (<37 wk). However, research on the impact of dental care utilization during pregnancy on these outcomes has produced both positive and negative results.
Objective:
The current study investigated the association between preterm birth and dental care utilization, focusing on dental visits for cleaning during pregnancy as well as the perceived benefits of oral health during pregnancy.
Methods:
This secondary data analysis cross-sectional study used data from the Pregnancy Risk Assessment Monitoring System in the United States from 2009 to 2021. Descriptive and multivariate logistic regression analyses were performed to examine the association between dental variables and preterm birth.
Results:
The study included 399,847 women with a recent single live birth, representing 21,218,114 women across 48 states and New York City. After adjusting for factors such as race and ethnicity, age, marital status, medical insurance type, education level, adequacy of prenatal care, and other medical variables associated with preterm birth, women who had dental visits for cleaning during pregnancy had a lower odds of preterm birth (adjusted odds ratio [aOR] = 0.90, 95% confidence interval [CI] [0.86, 0.93], P < 0.001) compared with those who did not. A significant association between prenatal dental cleaning and reduced preterm birth was observed only among women who perceived the benefits of oral health during pregnancy (aOR = 0.93, 95% CI [0.88, 0.97], P = 0.002) and among non-Hispanic White women (aOR = 0.88, 95% CI [0.83, 0.93], P < 0.001).
Conclusion:
This study revealed an inverse relationship between dental cleaning visits during pregnancy and preterm birth outcomes, notably among women who recognized the benefits of oral health and among non-Hispanic White women. The results emphasize the significance of dental visits and the perception of oral health benefits during pregnancy.
Knowledge Transfer Statement:
The study demonstrated an inverse association between dental visits for cleaning during pregnancy and preterm birth outcomes, with this relationship being significant among women who perceived the benefits of oral health during pregnancy and among non-Hispanic White women. These findings suggest that both the dental visits and the perception of oral health benefits may be important factors linked to preterm birth outcomes, with potential racial and ethnic variations. Policy makers and clinicians could integrate oral health care and prenatal oral health education into prenatal care as essential components of primary health care to improve both oral and overall health outcomes for women.
Introduction
Preterm birth, defined as the birth of an infant prior to 37 wk of gestation, is associated with multiple factors, including the mother’s race and ethnicity, age, socioeconomic status, Medicaid enrollment, and medical conditions such as hypertension or a history of smoking (Goldenberg et al. 2008; Shapiro-Mendoza and Lackritz 2012). Nationally, about 1 in 10 infants in the United States is born prematurely (Osterman et al. 2023; Martin et al. 2019). In 2020, the preterm birth rate was 14.4% among non-Hispanic Black women, compared with 9.1% among non-Hispanic White women (Osterman et al. 2023). This disparity has been extensively studied, with various social and environmental factors contributing to the inequity (Burris et al. 2019). While many premature infants grow and develop without complications, preterm birth can lead to long-term disabilities, placing a significant burden on families and health care systems.
Previous research on maternal populations has demonstrated a positive association between different maternal oral health outcomes, such as periodontal diseases, and adverse birth outcomes, including preeclampsia, low birth weight, and preterm birth (Ide and Papapanou 2013; Michalowicz et al. 2013; Papapanou 2015; Corbella et al. 2016; Beck et al. 2019). However, results from randomized controlled trials examining the impact of periodontal treatment as a way to improve oral health outcomes and subsequent improved birth outcomes have been mixed and inconsistent. While small-scale, single-center studies reported improved birth outcomes following periodontal treatment during pregnancy, larger multicenter studies did not show a significant association, likely due to variability in study designs and inconsistent disease definitions (Iheozor-Ejiofor et al. 2017; Beck et al. 2019; Bobetsis et al. 2020). A meta-analysis of case-control studies using categorical definitions of periodontal status found a strong association between periodontal disease during pregnancy and preterm birth, but pooled data from case-control studies using continuous periodontal measures, such as periodontal attachment loss and gingival bleeding, showed no significant association between gingival attachment loss and preterm birth (Ide and Papapanou 2013). Several factors, including the type and timing of periodontal examination relative to gestational age, the use of blinded examiners, and other confounders, can affect study quality and the strength of these associations (Ide and Papapanou 2013; Michalowicz et al. 2013; Papapanou 2015). Crucially, while treatment at dental facilities is important, daily oral hygiene practices also contribute to improved periodontal health. Yet, most studies do not account for these daily practices.
The proposed mechanism linking poor periodontal health to adverse birth outcomes includes periodontal pathogen infection in the feto-placental units and the body’s inflammatory response to such infection (Ren and Du 2017; Bobetsis et al. 2020). Several studies have detected periodontal pathogenic bacteria in feto-placental units (Fischer et al. 2019), and these pathogens have been shown to induce adverse birth outcomes, including preterm birth, in animal models (Ao et al. 2015; Stockham et al. 2015). Recent meta-analyses have suggested that periodontal treatment may protect against adverse outcomes such as preterm birth, prenatal mortality, and low birth weight (Le et al. 2021). However, the Cochrane review concluded that there is insufficient evidence to confirm the protective effect of periodontal treatment during pregnancy on preterm birth and low birth weight (Iheozor-Ejiofor et al. 2017). Therefore, further research is needed to explore the prevalence and interaction of these pathogenic bacteria beyond their mere presence in the feto-placental unit. Investigating the exact mechanisms and specific inflammatory responses triggered by these pathogens will be crucial in understanding their relationship with adverse birth outcomes (Fischer et al. 2019; Terzic et al. 2021). The National Institute of Dental and Craniofacial Research (NIDCR) recently published the report “Healthy Mouth, Healthy Body” in May 2024, summarizing 40 y of NIDCR-funded research, including studies on the link between periodontitis and adverse birth outcomes. The NIDCR is currently supporting 5 research projects aimed at understanding how maternal health during pregnancy affects oral health and development in young children (McMains 2024).
Prepregnancy health behaviors, such as dental visits for cleaning, can strongly predict dental visits during pregnancy (Boggess et al. 2010; Hayes et al. 2015; Umer et al., 2016; Robinson et al., 2021). Previous studies have shown that the strong association between dental cleanings before and during pregnancy suggests that an enabling environment and positive health decision-making among routine dental service users can carry over into pregnancy, independent of insurance coverage (Robinson et al. 2021). In addition, the perceived benefits of oral health during pregnancy are strongly linked to dental visits for cleaning during pregnancy. In a recent study on barriers to dental care, women who reported perceiving the benefits of oral health were more likely to visit the dentist for cleanings during pregnancy (Lee, Deshpande, et al. 2024).
The goal of the present study is to examine the association between preterm birth and dental visits for cleaning, stratified by prepregnancy dental visits and the perceived benefit of oral health during pregnancy. A previous study, using data from the Pregnancy Risk Assessment Monitoring System (PRAMS) of the Centers for Disease Control and Prevention (CDC), examined the relationship between dental service utilization during pregnancy and preterm birth outcomes based on data from 2004 to 2006 in 10 states (Hwang et al. 2012). That study found that women who did not receive dental cleanings had a greater odds of preterm birth (odds ratio [OR] = 1.23) than those who did, after adjusting for sociodemographic variables and medical conditions. The current study expands on this by including data from 48 states and incorporating newly collected information on prepregnancy dental visits and respondents’ perceived benefit of oral health during pregnancy, in addition to dental visits during pregnancy.
Materials and Methods
Dataset
This study used PRAMS data from 2009 to 2021. PRAMS collects population-based data on maternal attitudes and experiences before, during, and shortly after pregnancy through a combination of survey questions and birth certificate variables. The standardized data collection methodology is detailed in the literature and the CDC Model Surveillance Protocol (Shulman et al. 2006; Lee et al. 2022). Access to the data was granted through a data access agreement with the CDC. This study received an exemption from the Institutional Review Board of the Johns Hopkins School of Public Health.
Study Cohort and Sociodemographic Variables
The study population was limited to women with single live births. The term women is used here in accordance with the terminology employed in the PRAMS survey, as there is limited information on other pregnancy-capable genders. Women with missing responses regarding preterm birth and dental visits for cleaning during pregnancy were also excluded. Racial and ethnic groups were categorized as follows: non-Hispanic White women (White), non-Hispanic Black women (Black), Hispanic women, non-Hispanic Asian women (Asian), American Indian or Alaska Native (AI/AN) (Table 1), and others. Preterm birth was defined as a single live birth occurring prior to 37 wk of gestation, as indicated on the birth certificate (appendix). In addition, we included stress indicators during pregnancy, as a recent study using the same PRAMS database highlighted the association between stressful life events and low dental service utilization during pregnancy (Hedegaard et al. 1996; Testa et al. 2023).
Unadjusted Bivariate Analysis of Women with Preterm Birth (399,847 Women for a Weighted Number of 21,218,114 Women).
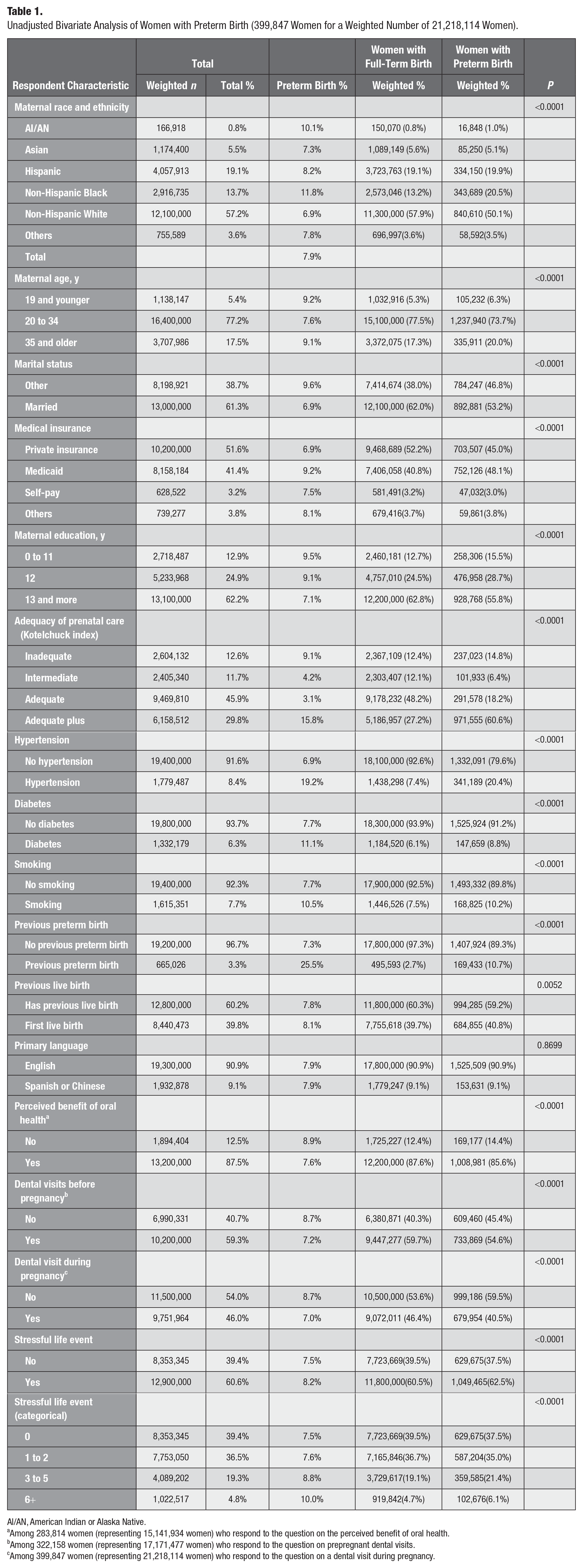
AI/AN, American Indian or Alaska Native.
Among 283,814 women (representing 15,141,934 women) who respond to the question on the perceived benefit of oral health.
Among 322,158 women (representing 17,171,477 women) who respond to the question on prepregnant dental visits.
Among 399,847 women (representing 21,218,114 women) who respond to the question on a dental visit during pregnancy.
All sociodemographic variables, medical conditions related to preterm birth, and the adequacy of prenatal care (as measured by the Kotelchuck index; Kotelchuck 1994; Shin and Song 2019) were obtained from birth certificate data linked to the PRAMS survey, as previously examined (Lee et al. 2022). Relevant medical conditions extracted from the PRAMS database included previous preterm birth, hypertension, smoking, and diabetes diagnosed at the time of birth (Table 1; Hwang et al. 2012; Iida 2017).
In addition, a variable for stressful life events was included if a woman responded “yes” to any of the survey questions regarding stressful life events. This variable was categorized by the number of stressful events during pregnancy. Income was excluded as a covariate in our analysis due to its correlation with payer types, such as Medicaid. While record-based information on payer type for dental care was not available, payer-type information for medical services derived from the PRAMS birth certificate data was used.
Dental Variables
Responses to survey questions regarding dental visits and the perceived benefits of oral health during pregnancy were recorded as binary (“yes” or “no”), with all other responses excluded (Table 1).
The dental-related survey questions included:
a. I had my teeth cleaned by a dentist or dental hygienist during pregnancy.
b. I knew it was important to care for my teeth and gums during my pregnancy.
c. I had my teeth cleaned by a dentist or dental hygienist 12 mo before pregnancy.
The subject-reported response to the PRAMS core survey item, “I had my teeth cleaned by a dentist or dental hygienist during my pregnancy,” indicates nonemergency dental service utilization.
Given that prepregnancy dental cleaning has been shown to be strongly associated with dental cleaning during pregnancy in previous studies (Robison et al. 2021), we stratified our regression analysis into 2 groups: women who received dental cleaning in the 12 mo prior to pregnancy and those who did not. In addition, our analysis was stratified based on women’s responses regarding the perceived benefits of oral health and their dental visits for cleaning prior to pregnancy.
From 2009 to 2021, all states included a question about dental visits for cleaning in the PRAMS survey. However, only the phase 7 (2012–2015) and phase 8 (2016–2019) databases included questions regarding dental visits for cleaning both before and during pregnancy, as well as the perceived benefits of oral health during pregnancy. Therefore, the size of the sample population was indicated for each analysis.
Analysis
An unadjusted bivariate analysis was conducted to examine differences in baseline characteristics between women who had full-term births and those who experienced preterm births. Significant differences were tested using a chi-squared test (Table 1). The analysis also included comparisons of dental visits during or prior to pregnancy and the perceived benefits of oral health between these 2 groups of women. Primary language was not included in the multivariate regression models, as the unadjusted bivariate model did not reveal any significant differences (P < 0.01) between women with full-term births and those with preterm births.
In multivariate logistic regression models, the adjusted ORs (aORs) for preterm birth were calculated for the prenatal dental visit variable, adjusting for the mother’s race and ethnicity, age, marital status, insurance type, education level, adequacy of prenatal care, previous history of preterm birth, and other medical conditions related to preterm birth, such as hypertension, smoking, and diabetes (Table 2). The association was further analyzed using stratification by (1) prepregnancy dental visits for cleaning and (2) perceived benefits of oral health. We utilized Stata 17 to account for PRAMS’s complex weighting and oversampling methodology in this study.
Multivariate Logistic Regression Models for Preterm Birth Outcomes (323,235 Women for a Weighted Number of 17,902,494 Women).
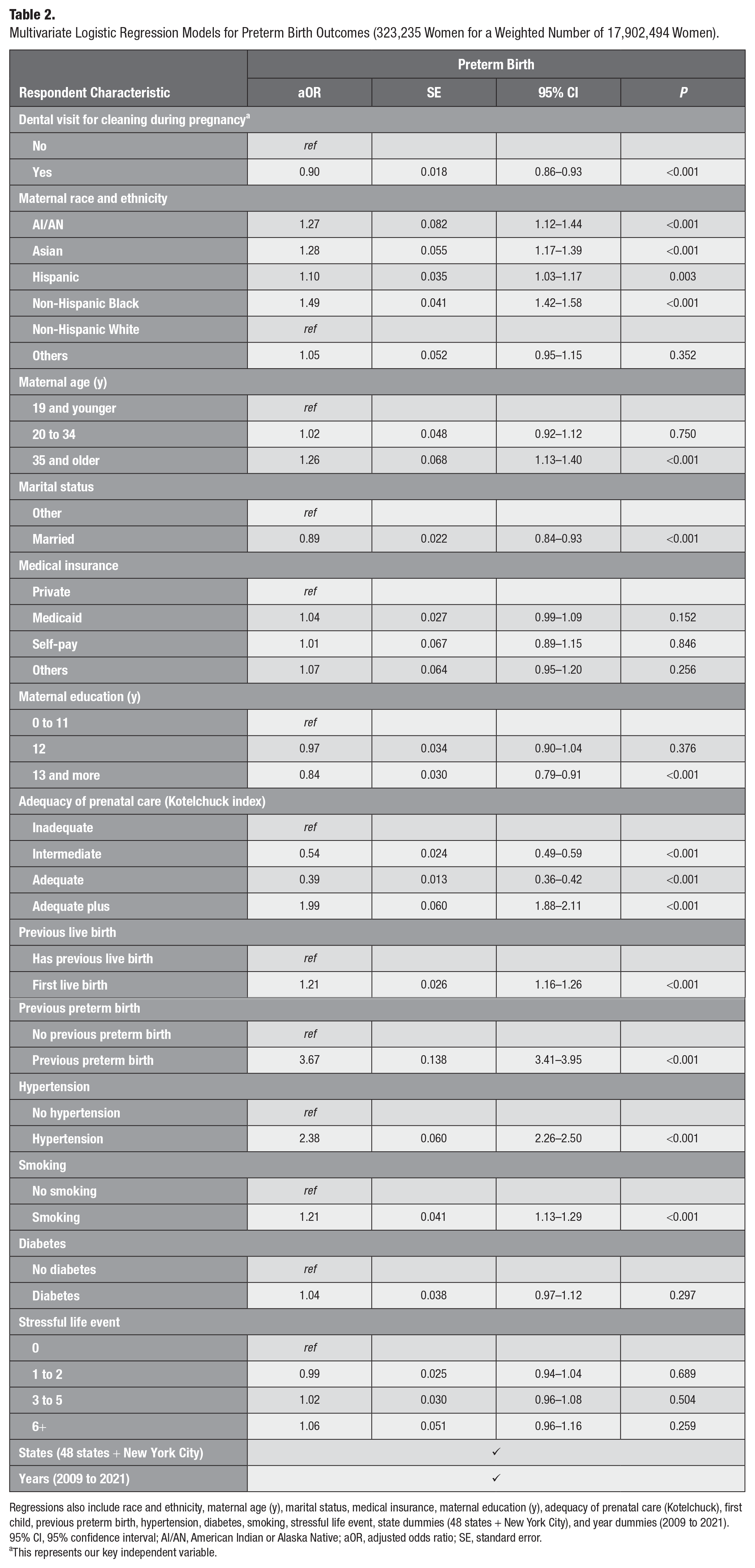
Regressions also include race and ethnicity, maternal age (y), marital status, medical insurance, maternal education (y), adequacy of prenatal care (Kotelchuck), first child, previous preterm birth, hypertension, diabetes, smoking, stressful life event, state dummies (48 states + New York City), and year dummies (2009 to 2021).
95% CI, 95% confidence interval; AI/AN, American Indian or Alaska Native; aOR, adjusted odds ratio; SE, standard error.
This represents our key independent variable.
Results
Unadjusted Bivariate Analysis of the Overall Characteristics
After applying inclusion and exclusion criteria, the analysis resulted in a sample of 399,847 women representing 21,218,114 women from 48 states and New York City. The differences in sociodemographic characteristics between women with full-term birth and those with preterm birth are listed in Table 1.
The average preterm birth rate was 7.9%. The percentage of preterm births was higher among Black women (11.8%), Hispanic women (8.2%), Asian women (7.3%), and American Indian or Alaska Native (AI/AN) women (10.1%) compared with White women (6.9%). Women who experienced preterm births tended to be either 35 y or older (9.1%) or 19 y and younger (9.2%), unmarried (9.6%), enrolled in Medicaid (9.2%), and less educated (9.5%). In addition, they had inadequate prenatal care as indicated by the Kotelchuck index (9.1%) or were more likely to be classified as high-risk pregnancies requiring more prenatal visits (15.8% Adequate Plus Kotelchuck index). Women with preterm births were also more likely to have a greater number of stressful life events during pregnancy and to have medical complications, including hypertension, diabetes, smoking, and a history of previous preterm births (see Table 1). All of these differences were statistically significant at a P value of less than 0.01.
In the unadjusted bivariate model, all dental variables were significantly associated with preterm birth outcomes. Women with preterm births were less likely to have visited a dentist for cleaning both before (54.6%) and during pregnancy (40.5%) compared with women with full-term births (59.7% and 46.4%, respectively; chi-squared test, P < 0.0001).
Multivariate Logistic Regression Models for Preterm Birth Outcomes
When adjusted for the mother’s race and ethnicity, age, marital status, insurance type, education, first trimester prenatal visits, previous live births, and medical conditions known to be associated with preterm birth risk (including previous preterm births, hypertension, smoking, diabetes, and stressful life events), women who had a dental cleaning during their pregnancy exhibited a 10% lower odds of experiencing a preterm birth compared with those who did not have a dental cleaning (aOR = 0.90, 95% confidence interval [CI] [0.86–0.93], P < 0.001; Table 2).
Stratifying by prepregnancy dental cleaning, both women who received dental cleaning during pregnancy (aOR = 0.90, 95% CI [0.84–0.96], P = 0.001) and those who did not (aOR = 0.88, 95% CI [0.81–0.95], P = 0.002) showed significantly lower odds of preterm birth after adjusting for race and ethnicity, age, and other covariates (Table 3). However, when the analysis was stratified by perceived benefits of oral health, the significant association between dental visits for cleaning during pregnancy and preterm birth outcomes was observed only among women who perceived the benefits of oral health during pregnancy (aOR = 0.93, 95% CI [0.88–0.97], P = 0.002; Table 4). Finally, the associations between prenatal dental visits for cleaning and preterm birth outcomes were examined, and the statistically significant association was observed only among White women (aOR = 0.88, 95% CI [0.83–0.93], P < 0.001) and not among women from other racial/ethnic backgrounds (Table 5).
Multivariate Logistic Regression Models for Preterm Birth Outcomes, Stratified for Prepregnancy Cleaning (150,397 Women for a Weighted Number of 8,498,073 Women).
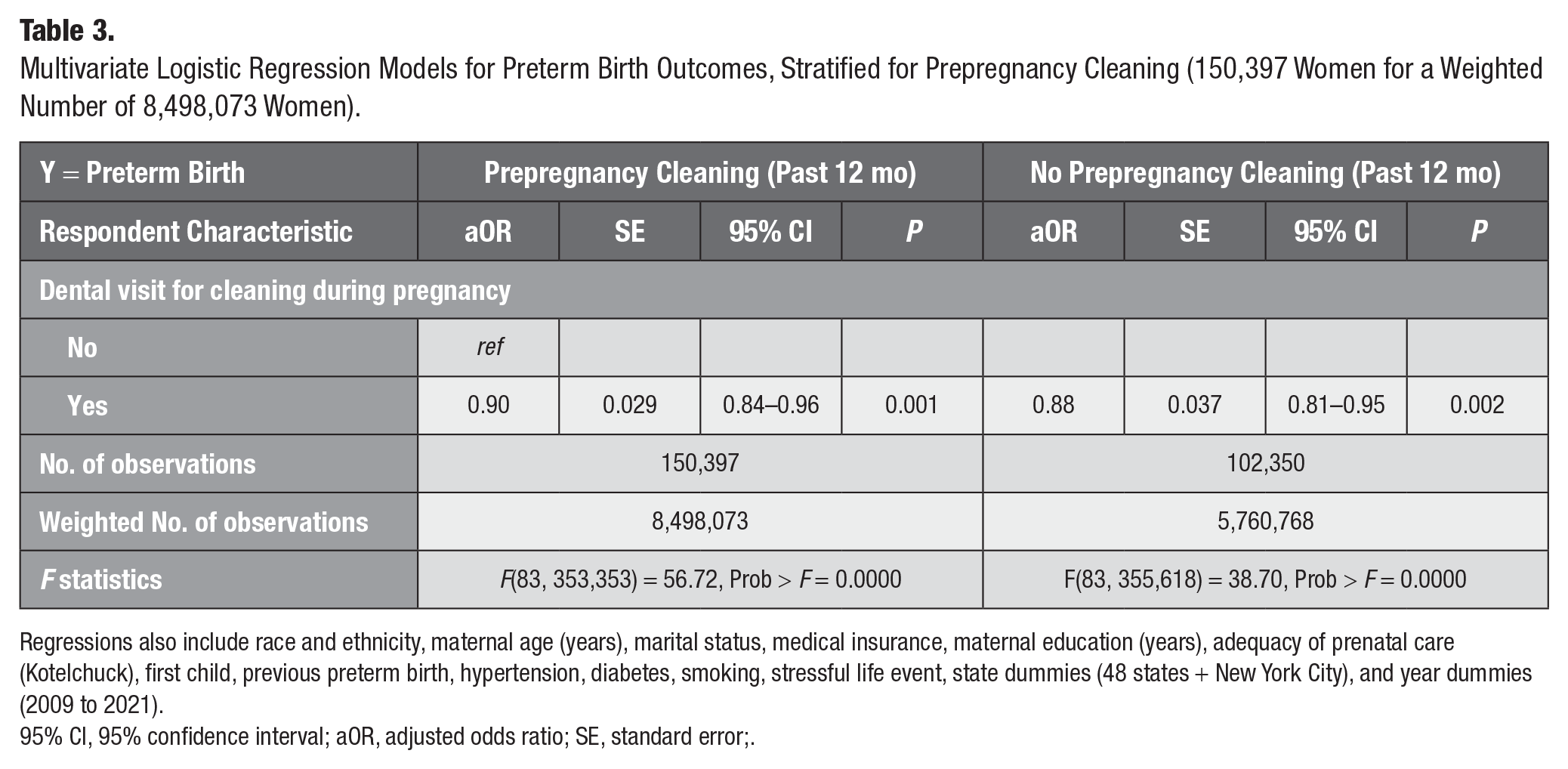
Regressions also include race and ethnicity, maternal age (years), marital status, medical insurance, maternal education (years), adequacy of prenatal care (Kotelchuck), first child, previous preterm birth, hypertension, diabetes, smoking, stressful life event, state dummies (48 states + New York City), and year dummies (2009 to 2021).
95% CI, 95% confidence interval; aOR, adjusted odds ratio; SE, standard error;.
Multivariate Logistic Regression Models for Preterm Birth Outcomes, Stratified for Perceived Benefits of Oral Health (204,608 Women for a Weighted Number of 11,213,601 Women).
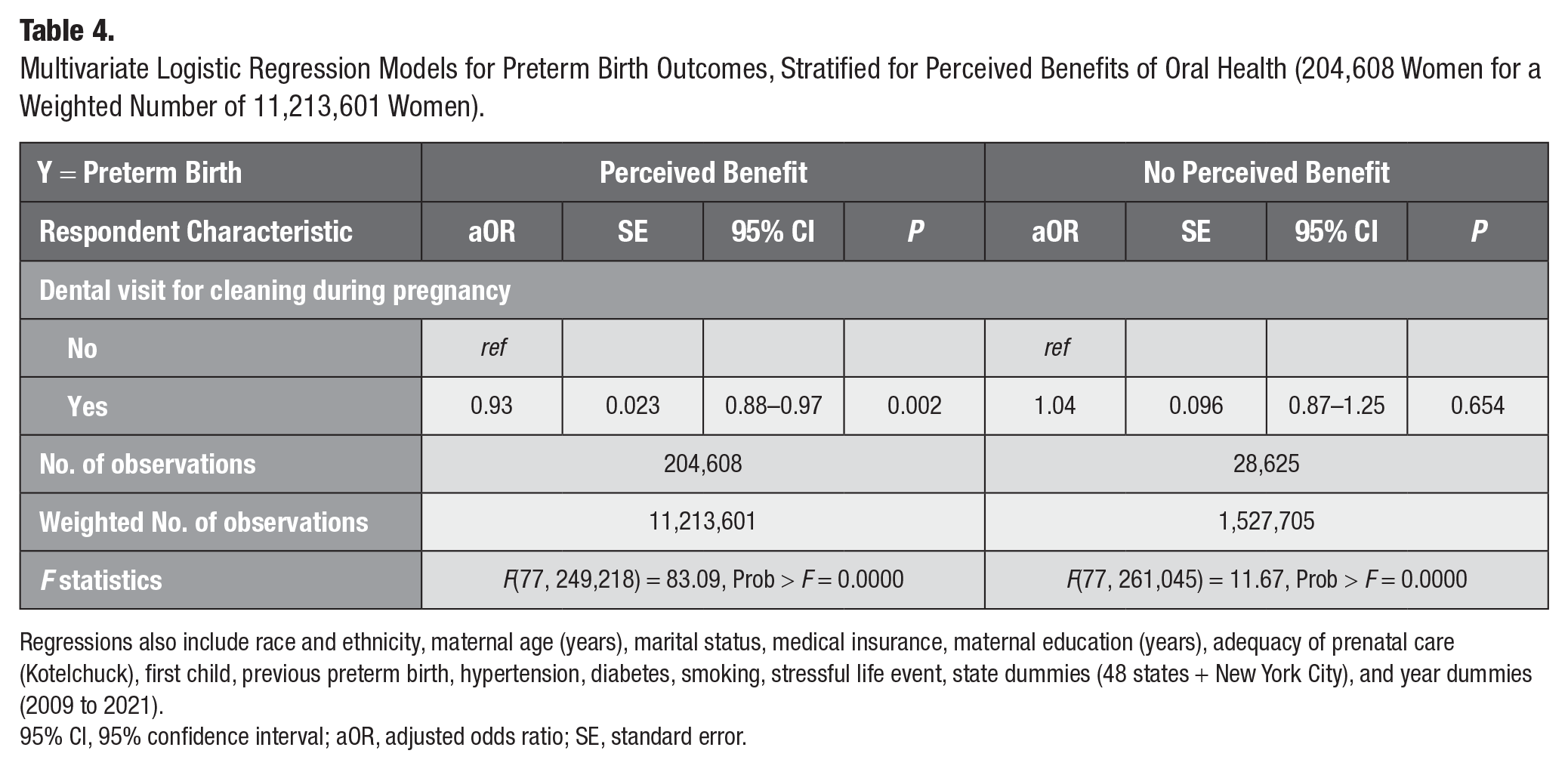
Regressions also include race and ethnicity, maternal age (years), marital status, medical insurance, maternal education (years), adequacy of prenatal care (Kotelchuck), first child, previous preterm birth, hypertension, diabetes, smoking, stressful life event, state dummies (48 states + New York City), and year dummies (2009 to 2021).
95% CI, 95% confidence interval; aOR, adjusted odds ratio; SE, standard error.
Multivariate Logistic Regression Models for Preterm Birth Outcomes, Stratified for Race and Ethnicity.
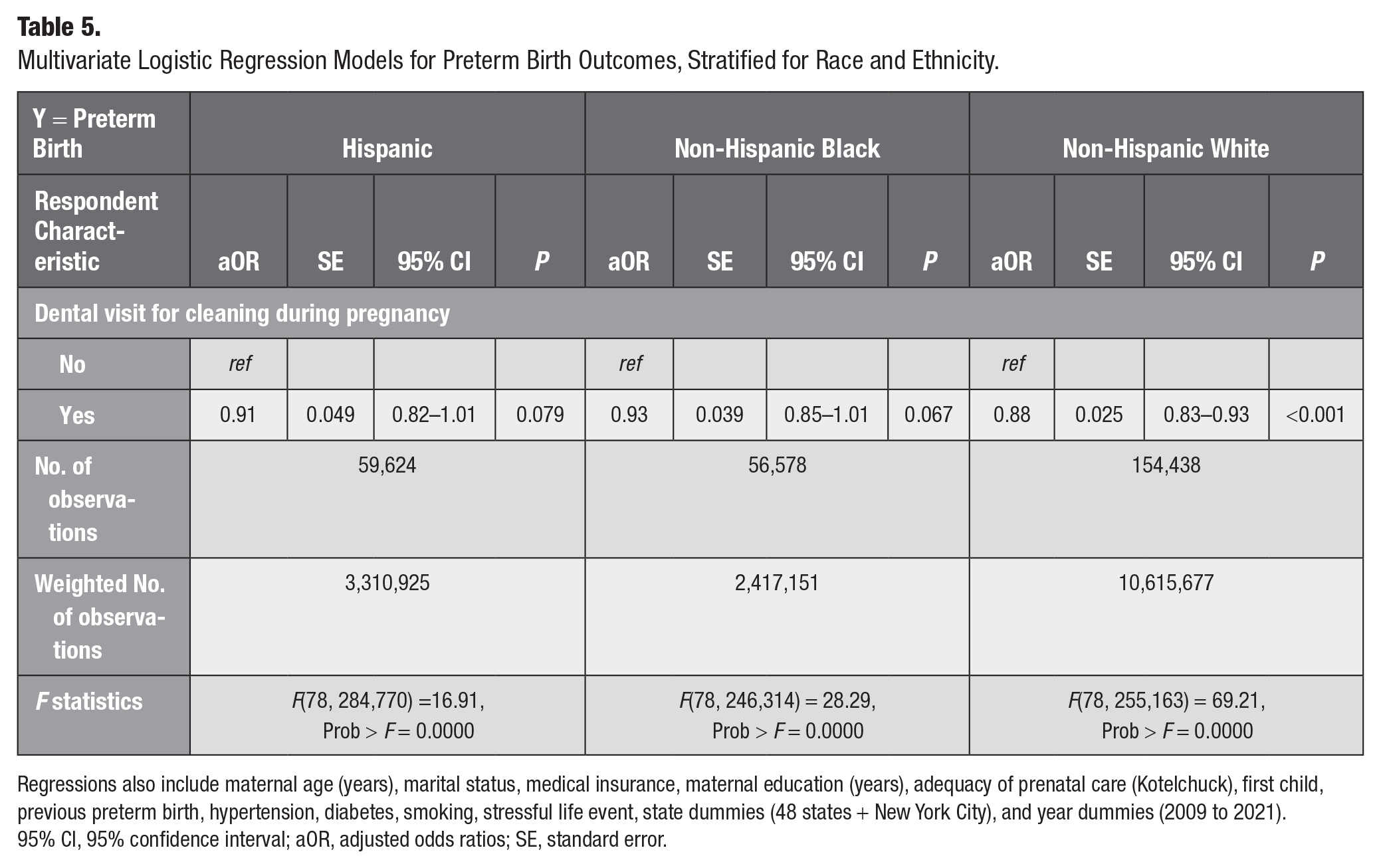
Regressions also include maternal age (years), marital status, medical insurance, maternal education (years), adequacy of prenatal care (Kotelchuck), first child, previous preterm birth, hypertension, diabetes, smoking, stressful life event, state dummies (48 states + New York City), and year dummies (2009 to 2021).
95% CI, 95% confidence interval; aOR, adjusted odds ratios; SE, standard error.
Sensitivity Analysis
The results remained consistent (aOR = 0.90; 95% CI [0.86–0.93]) when analyzed as a binomial variable for stressful events during pregnancy instead of as a categorical stress variable (Appendix Table 2). In addition, a separate analysis for the years 2020 and 2021 was conducted, coinciding with the COVID-19 pandemic period when most dental care services were suspended at least for a few months. The magnitudes of the associations observed during these years were similar to those found in the full sample (2009 to 2021; Appendix Table 3).
Discussion
This cross-sectional analysis of PRAMS data from 2009 to 2021 included approximately 400,000 women from 48 states and New York City, representing a weighted total of more than 21 million women. The study found that dental visits for cleaning during pregnancy were inversely associated with preterm birth outcomes after adjusting for sociodemographic factors, adequacy of prenatal care, and other preterm birth risk factors. These findings reinforce and expand on a previous study using PRAMS data from a decade earlier (Hwang et al. 2012), further confirming the link between dental cleanings during pregnancy and a lower preterm birth risk.
The findings can be interpreted within a complex body of literature on the association between oral health and preterm birth. Research on the relationship between oral health and preterm birth reveals a complex interplay between periodontal infections and pregnancy outcomes. Although the causality has been shown in animal models, a Cochrane review and other studies found insufficient evidence to definitively confirm these protective effects (Iheozor-Ejiofor 2017; Ren and Du 2017; Bobetsis et al. 2020).
The association between dental visits for cleaning and birth outcomes is shaped by broader contextual factors. Enabling factors such as dental coverage and providers’ willingness to treat pregnant women play a crucial role in dental service utilization during pregnancy. Despite numerous national and state-level prenatal oral health guidelines published in the last decade (Oral Health Care During Pregnancy Expert Workgroup 2012; Committee on Health Care for Underserved Women 2013), dental service utilization among pregnant women has declined over time, unlike among children, which may limit opportunities for timely oral health education to promote healthy behaviors (Kumar et al. 2023; CDC 2024). Research shows that pregnant women who received oral health education and dental supplies significantly increased the frequency of toothbrushing and flossing while also reducing their intake of sugary drinks as compared with a control group (Chibulka et al. 2011). This underscores that improving women’s oral health requires more than just clinical treatment—it hinges on the perception of oral health benefits and consistent daily hygiene practices. Pregnant women’s beliefs and attitudes toward oral health are essential in enhancing both home care routines and oral health outcomes.
Whether perceived oral health benefits can reliably serve as a proxy for daily oral hygiene practices remains debatable. According to the health belief model, perceived benefits are a primary driver of healthy behaviors. A recent study demonstrated that perceived benefits predict dental cleaning behavior (Fallahi et al. 2023), and greater oral health knowledge leads to improved daily oral hygiene practices (Armin and ElSalhy 2014; Naavaal et al. 2019). The significant association found in this study between prenatal dental cleanings and preterm birth outcomes among women with perceived oral health benefits highlights the importance of oral health beliefs as a potential precursor to good hygiene habits, healthy eating, and other positive health behaviors. This includes practices such as daily toothbrushing, flossing, mouth rinsing, and mindful food and beverage choices, all of which may synergize with professional dental cleanings to better protect maternal and fetal health.
Future research should investigate the relationship between dental service utilization and oral health status from the prepregnancy stage through the postdelivery period (Barillas and Lee 2022; Lee, Ramphoma, et al. 2024). This study demonstrated that the association between dental visits for cleaning and preterm birth outcomes was stronger among women who did not receive dental cleaning before pregnancy compared with those who did. The larger decrease in the odds of preterm birth among women without prepregnancy cleaning suggests a potentially greater impact of prenatal cleaning in this group. In contrast, the effect of dental cleaning during pregnancy may be smaller for women with prepregnancy cleanings, as these women are more likely to have already been taking better care of their oral health, reducing the difference in outcomes. From a clinical perspective, a single scaling or cleaning session may not be sufficient to improve periodontal health, especially since periodontal infections can occur early in pregnancy and potentially affect the fetus. Therefore, prepregnancy counseling should incorporate both oral health education and referral to dental care to create a healthier environment for both mothers and fetus.
Although racial and ethnic variation in the association between dental visits for cleaning and preterm birth was not the primary focus of this study, the finding that the association was significant only among White women is intriguing. Future research should investigate how this relationship varies across different racial and ethnic groups and address the underlying causes of such disparities.
There are several limitations inherent to the cross-sectional secondary data analysis design used in this study. Recall bias and socially desirable responses could affect the reliability of the dental variables, as they were based on self-reported survey responses. In addition, the lack of temporal data limits the ability to fully assess the relationship between dental visits and perceived oral health benefits during pregnancy. Another limitation is the absence of objective insurance information for dental care during pregnancy, as the PRAMS birth certificate data provided information only on medical insurance. Despite these challenges, this study contributes valuable findings to the field by highlighting the positive association between dental care during pregnancy and improved birth outcomes, emphasizing the importance of perceived oral health benefits. The study further distinguishes itself by controlling for an important confounder, stressful events during pregnancy, which was not addressed in previous studies.
Conclusion
This study found an inverse association between dental visits for cleaning during pregnancy and preterm birth outcomes, particularly among women who perceived the benefits of oral health during pregnancy. This finding underscores the importance of both dental visits for cleaning and the perception of oral health benefits during pregnancy. To improve maternal and child health, health systems should integrate oral health care as a key component of primary and perinatal care, along with health education initiatives that promote the oral health of women of childbearing age. Future research should investigate the variation in this association in different racial/ethnic women.
Author Contributions
H. Lee, contributed to conception, design, data acquisition, analysis, and interpretation of data, drafted and critically revised the manuscript; N. Hong, contributed to data analysis, critically revised the manuscript, who is supported by the BK21 FOUR (Fostering Outstanding Universities for Research), funded by the Ministry of Education (MOE, Korea), and the National Research Foundation of Korea (NRF); T. Janevic, contributed to data interpretation of data, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jct-10.1177_23800844251318698 – Supplemental material for Prenatal Dental Visits, Perceived Benefits of Oral Health, and Preterm Birth Outcome, 2009–2021
Supplemental material, sj-docx-1-jct-10.1177_23800844251318698 for Prenatal Dental Visits, Perceived Benefits of Oral Health, and Preterm Birth Outcome, 2009–2021 by H. Lee, N. Hong and T. Janevic in JDR Clinical & Translational Research
Footnotes
Acknowledgements
We thank the PRAMS Working Group, which includes the PRAMS Team, Division of Reproductive Health, CDC, and the following PRAMS sites for their role in conducting PRAMS surveillance and allowing the use of their data: PRAMS Alaska, PRAMS Alabama, PRAMS Arizona, PRAMS Colorado, PRAMS Connecticut, PRAMS Washington D.C., PRAMS Delaware, PRAMS Florida, PRAMS Georgia, PRAMS Hawaii, PRAMS Iowa, PRAMS Illinois, PRAMS Indiana, PRAMS Kansas, PRAMS Kentucky, PRAMS Louisiana, PRAMS Massachusetts, PRAMS Maryland, PRAMS Maine, PRAMS Michigan, PRAMS Minesota, PRAMS Missouri, PRAMS Mississippi, PRAMS Montana, PRAMS North Carolina, PRAMS North Dakota, PRAMS New Hampshire, PRAMS New Jersey, PRAMS New Mexico, PRAMS New York, PRAMS New York City, PRAMS Ohio, PRAMS Oklahoma, PRAMS Oregon, PRAMS Pennsylvania, PRAMS Puerto Rico, PRAMS Rhode Islands, PRAMS South Dakota, PRAMS Tennessee, PRAMS Texas, PRAMS Utah, PRAMS Virginia, PRAMS Vermont, PRAMS Washington, PRAMS Wisconsin, PRAMS West Virginia PRAMS. PRAMS Wyoming. We also thank the mothers who participated in the PRAMS survey.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received financial support for the open access publication of this article from Seoul National University.
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.