
Abstract
Introduction:
Sarcopenia is loss of both muscle mass and function with age and is associated with inadequate protein intake. However, evidence to suggest an association with oral health is less clear.
Objective:
To scope peer-reviewed published evidence (2000–2022) pertaining to oral function in relation to sarcopenia and/or protein intake in older people.
Methods:
CINAHL, Embase, PubMed, and Scopus were searched. Included were peer-reviewed studies measuring oral function (e.g., tooth loss, salivary flow masticatory function, strength of muscles of mastication, and tongue pressure) and a measure of protein intake and/or a measure of sarcopenia (appendicular muscle mass and function). Full article screening was conducted by 1 reviewer with a random 10% screened in duplicate by a second reviewer. Relevant content pertaining to study type, country of origin, measures of exposure, and outcomes and key findings was mapped and the balance of data showing a positive versus null association of oral health with outcomes charted.
Results:
Of 376 studies identified, 126 were screened in full, yielding 32 included texts, of which 29 were original articles. Seven reported intake of protein and 22 reported measures of sarcopenia. Nine distinct oral health exposures were identified, with ≤4 studies relating to any one of these measures. Most data were cross-sectional in nature (27 studies) and from Japan (20 studies). The balance of data showed associations between tooth loss and measures of sarcopenia and protein intake. However, the balance of data pertaining to any association between chewing function, tongue pressure, or indices of oral hypofunction and sarcopenia was mixed.
Conclusion:
A broad range of oral health measures have been studied in relation to sarcopenia. The balance of data suggests that tooth loss is associated with risk, but data pertaining to the oral musculature and indices of oral hypofunction are mixed.
Knowledge Transfer Statement:
The findings of this research will increase awareness among clinicians of the amount and nature of evidence pertaining to the relationship between oral health and risk of compromised muscle mass and function, including data showing that loss of teeth is associated with increased risk of sarcopenia in older people. The findings highlight to researchers the gaps in the evidence and where further research and clarification of the relationship between oral health and risk of sarcopenia is warranted.
Introduction
An adequate dietary protein intake is important in maintaining muscle mass and function in older age (65+ y), thereby helping to mitigate sarcopenia (Paddon-Jones et al. 2015). Sarcopenia refers to the pathologic reduction in skeletal muscle mass and strength and, consequentially, loss of function (Muscaritoli et al. 2010; Cruz-Jentoft et al. 2014). It is diagnosed through having both low muscle strength and low muscle mass and is associated with adverse health outcomes, including falls and fractures, cardiac and respiratory diseases, reduced cognitive function, loss of independence, increased risk of hospitalization, and increased mortality (Senior et al. 2015). Sarcopenia affects 5% to 50% of older people depending on gender, age, pathological conditions, and diagnostic criteria (Papadopoulou 2020).
In older adults, reduced masticatory performance (e.g., tooth loss, reduced chewing and biting ability, low salivary flow, stomatitis, reduced tongue pressure) may affect the ability to consume adequate dietary protein (Sheiham et al. 2001; Mendonça et al. 2018). It can therefore be postulated that compromised oral function may contribute to nutritional deficits, including low intake of protein, that contribute to loss of muscle mass and the development of sarcopenia. However, sarcopenia is a whole-body disease and affects not only skeletal muscles but also the muscles involved in mastication and swallowing (Machida et al. 2017). Reduced tongue pressure is a symptom of sarcopenia (Buehring et al. 2013). However, tongue pressure is also reduced with age independently of sarcopenia (Machida et al. 2017; Sakai, Nakayama, Tohara, Kodama, et al. 2017), and age-related decrease in tongue pressure could affect dietary intake, thus contributing to risk of sarcopenia. Therefore, it can be postulated that the direction of effect between food intake and sarcopenia, as well as between some elements of oral health (e.g., tongue pressure, lip pressure, occlusal force and function, and strength of the muscles involved in mastication) and sarcopenia, may be bidirectional. With the overall aim of identifying what is known about the relationship between diet, oral function, and risk of sarcopenia, the objective was to conduct a scoping review to map existing data pertaining to this area and to identify potential gaps in the evidence. The specific aim was to scope the existing published evidence pertaining to compromised oral health, intake of dietary protein, and presence of sarcopenia. The specific objectives were to 1) to identify existing peer-reviewed evidence pertaining to any relationship between different elements of compromised oral health and i) risk of sarcopenia, ii) intake of dietary protein, and iii) both, and 2) to map available data by study type and volume of information, geographic location, measures of oral health and function, measures of sarcopenia employed, and measures of protein intake, along with an overview of findings and the balance of data showing an association versus no association. The outcomes will inform on existing evidence pertaining to oral function and risk of sarcopenia, whether there has been sufficient research in this area, and where gaps in data exist. The results will inform future development of research studies in oral health, protein intake, and sarcopenia.
Methods
The review was conducted according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) (Tricco et al. 2018) and Joanna Briggs Institute methodology for scoping reviews (Peters et al. 2021). The protocol was published on FigShare (Teo and Moynihan 2022).
Population, Context, and Concept
Participants were older adults (generally aged 65 y and over), including those diagnosed with type 2 diabetes mellitus or with under- or overnutrition. Excluded were studies with a specific focus on participants with acute or chronic diseases (e.g., cancer, kidney disease, liver disease).
The concept of interest was oral function in relation to sarcopenia and/or intake of dietary protein. Included were studies measuring oral function (e.g., by tooth loss, reduced salivary flow [dry mouth, xerostomia], masticatory function, bite force, and strength of muscles of mastication, tongue pressure) and a measure of protein intake (e.g., g/d, percent contribution to energy intake, achieving/not achieving intake reference values) and/or a measure of sarcopenia (which had to include a measure of both muscle mass and of muscle function). Studies measuring muscle function (i.e., handgrip strength, walking speed, physical frailty) without a measure of muscle mass were excluded. Excluded also were studies that measured dietary protein intake and risk of sarcopenia but without a measure of oral health/function. Studies that measured presbyphagia (sarcopenic dysphagia) without a measurement of general sarcopenia were excluded.
The context was data from populations in any country from any type of intervention or epidemiological study dated from 2000 to January 2022 to capture the global perspective published this century.
Types of Information
Included were peer-reviewed studies (randomized controlled trials [RCTs], nonrandomized trials, quasi-experimental studies, and reviews) that contained data relevant to the PCC with at least an abstract written in English. Protocols, abstracts, preprints, conference proceedings, thesis, gray literature, and any other non-peer-reviewed articles were excluded.
The PCC mnemonics (population/concept/context) was used to define all searches across the online databases. First, the concept was broken down into “oral function,” “sarcopenia,” and “dietary protein.” Alternative terminologies for these concepts were determined and recorded in a logic grid. This led to the generation of initial search terms. An initial scoping search was performed on PubMed using MeSH thesaurus terms and common terms to determine the search sensitivity and the need for more concept synonyms and variations to be added to the logic grid. This was replicated for the other databases (CINAHL, Embase, and Scopus) by searching for the major concepts and their synonyms, while identifying more concepts, synonyms, and variations to be added. The logic grids were adapted to work accordingly to the specific rules of each online database. The text words contained in the title and abstract of retrieved articles in the initial search were analyzed, in addition to all the MeSH/Emtree terms used to index the articles. Next, a second search using all identified keywords and indexed terms was conducted across all included databases. The final logic grids recorded for each online database are presented in the Appendix to the protocol (Teo and Moynihan 2022). The reference lists of included articles (after full-text screening) were searched for additional sources.
Study Selection
In terms of studies selection, PCC mnemonics (population/concept/context) guided the eligibility criteria for relevant studies. Resulting hits were imported into Covidence software (Veritas Health Innovation) after removal of duplicates. A primary screening of titles and abstracts was conducted by 2 independent researchers (JLT, PM) to eliminate articles that were clearly outside of the inclusion criteria. Any differences between the reviewers’ decisions were resolved through discussion. If consensus was not reached, a third-party reviewer was consulted.
A secondary screening on included full texts was conducted by 1 reviewer (JLT). A random 10% sample of all full-text studies was screened in duplicate by a second reviewer (PM), and interrater reliability was assessed. The reference list of included studies was also searched for additional studies. Reasons for exclusion were recorded at this stage. Any differences between reviewers’ decisions were resolved through discussion. If consensus was not reached, a third-party reviewer was consulted. The process of duplicate screening a 10% sample of articles was repeated until >95% agreement between reviewers was achieved. Articles excluded at full-text screening are presented in Appendix Table 1 along with reason for exclusion. The stages of article identification and screening are reported in a PRISMA-ScR chart (Fig. 1).
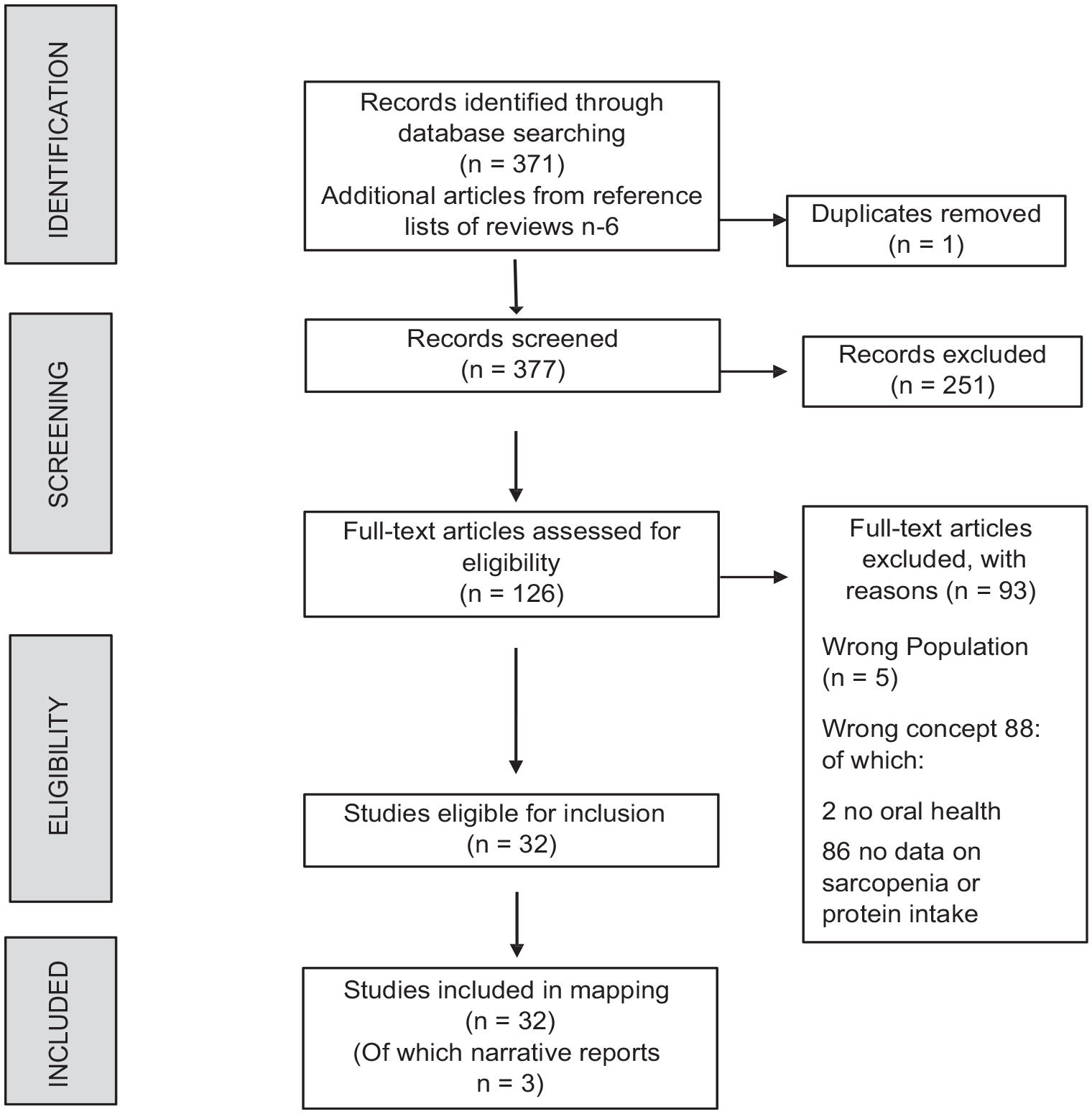
Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) flowchart.
Data Charting/Mapping
Data charting of included studies was conducted by 1 reviewer and checked by a second reviewer. During data charting, a mapping spreadsheet was developed using Microsoft Excel to ensure a systematic data-mapping process. The key information mapped included author(s), year of publication, origin/country of origin (where the source was published or conducted), aims/purpose, population and sample size, exposure variables and how these were measured (i.e., oral health measures), relevant outcome variables and how these were measured (i.e., methods to assess risk of sarcopenia and dietary protein intake), duration of the study (for intervention and cohort studies), and key findings that relate to the topic (PCC). These data are given in Appendix Table 2. Charting of the articles was trialed by 1 reviewer for an approximately 10% sample of identified studies and was modified accordingly to include relevant data across all articles. The results were described narratively in tabulated form, with the balance of studies showing positive or null associations between the oral health exposure and the outcome (sarcopenia/low protein intake) presented in harvest plots (Fig. 2).
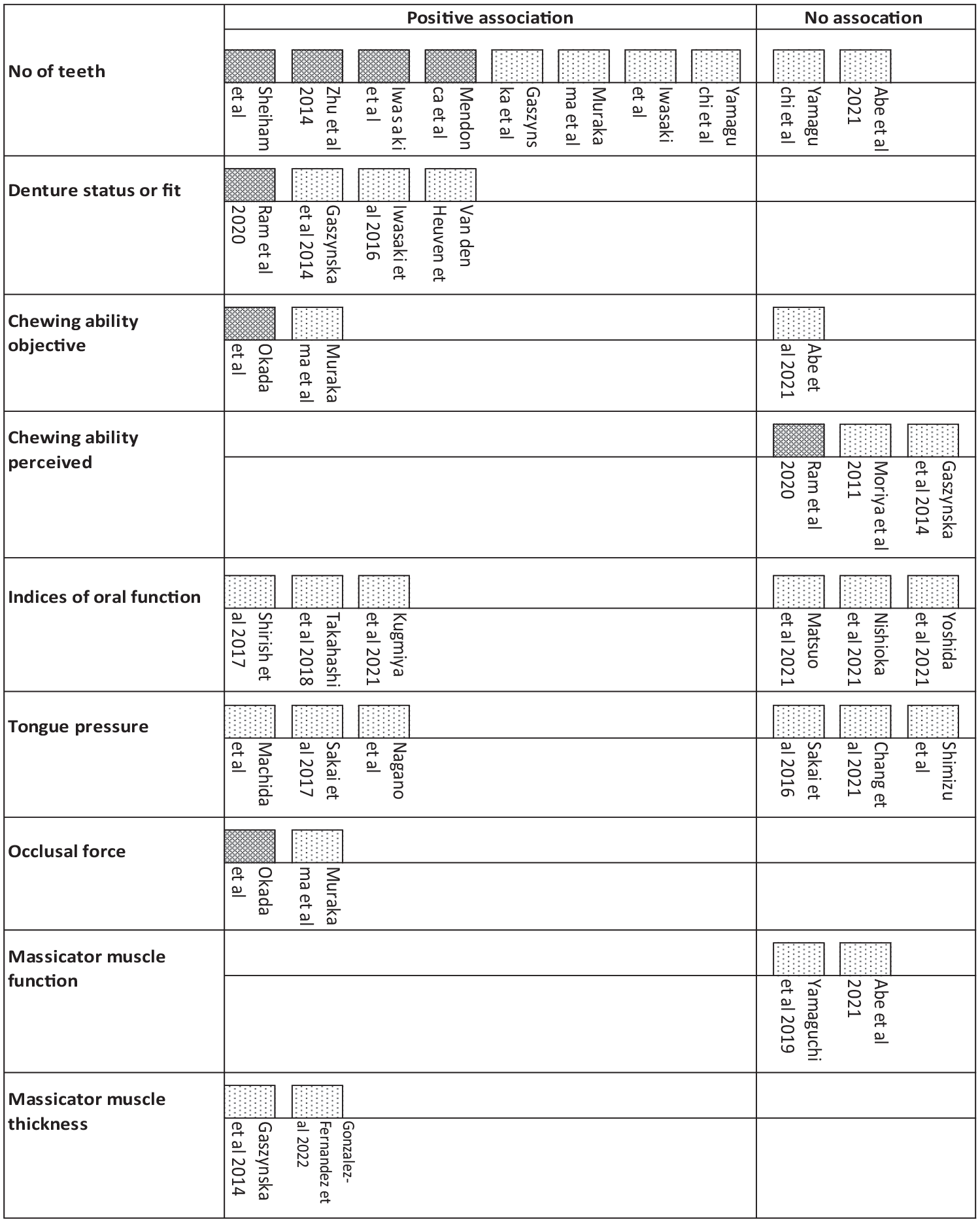
Harvest plot to illustrate the balance of studies showing an association between compromised oral health indices and (
Results
Figure 1 presents the PRISMA-ScR flowchart. Of 376 studies identified, 126 were included for full-text screening, of which 93 were excluded (see Appendix Table 1), resulting in 32 included texts. This included 3 narrative reviews/opinion pieces (Azzolino et al. 2019; Fujishima et al. 2019; Watanabe et al. 2020) that did not include any original data. Remaining studies (n = 29) were grouped according to review questions into those that reported on the impact of oral health on 1) intake of protein (n = 7) (Sheiham et al. 2001; Zhu and Hollis 2014; Okada et al. 2015; Iwasaki et al. 2016; Mendonça et al. 2018; Nagano et al. 2020; Ram et al. 2020) and 2) measures of sarcopenia (n = 22) (Okada et al. 2010; Moriya et al. 2011; Gaszynska et al. 2014; Murakami et al. 2015; Gaszynska et al. 2017; Iwasaki et al. 2017; Machida et al. 2017; Sakai, Nakayama, Tohara, Kodama, et al. 2017; Sakai, Nakayama, Tohara, Maeda, et al. 2017; Shiraishi et al. 2017; Takahashi et al. 2018; van den Heuven et al. 2019; Yamaguchi et al. 2019; Abe et al. 2021; Chang et al. 2021; Kugimiya et al. 2021; Matsuo et al. 2021; Nishioka et al. 2021; Shimizu et al. 2021; Yoshida et al. 2022; González-Fernández et al. 2021). No studies were identified that reported the association between oral health measures and both intake of protein and a measure of sarcopenia. Of the 7 studies that reported on the impact of oral health on intake of protein, 1 was an intervention study (Nagano et al. 2020), 1 was a cohort study (Iwasaki et al. 2016), and 5 studies had cross-sectional data (Sheiham et al. 2001; Zhu and Hollis 2014; Okada et al. 2015; Mendonça et al. 2018; Ram et al. 2020). Three studies were of Japanese populations (Okada et al. 2015; Iwasaki et al. 2016; Nagano et al. 2020), 2 of UK populations (Sheiham et al. 2001; Mendonça et al. 2018), 1 of a US population (Zhu and Hollis 2014), and 1 from New Zealand (Ram et al. 2020). All 22 studies that reported on an association between oral health exposure and measures of sarcopenia included cross-sectional analysis (see Appendix Table 2). The majority of these data came from studies of Japanese older adults (n = 17) (Okada et al. 2010; Moriya et al. 2011; Murakami et al. 2015; Iwasaki et al. 2017; Machida et al. 2017; Sakai, Nakayama, Tohara, Kodama, et al. 2017; Sakai, Nakayama, Tohara, Maeda, et al. 2017; Shiraishi et al. 2017; Takahashi et al. 2018; Yamaguchi et al. 2019; Abe et al. 2021; Kugimiya et al. 2021; Matsuo et al. 2021; Nishioka et al. 2021; Shimizu et al. 2021; Yoshida et al. 2022). Data also came from Poland (n = 2) (Gaszynska et al. 2014; Gaszynska et al. 2017), Spain (n = 1) (González-Fernández et al. 2022), Taiwan (n = 1) (Chang et al. 2021), and the United Kingdom (n = 1) (van den Heuven et al. 2019). There were no data from the Americas, Africa, or Australasia. Table 1 summarizes information on the various oral health exposures that have been explored in relation to protein intake or measures of sarcopenia (muscle mass and muscle strength) and the frequency with which these measures were applied across studies. Table 2 groups studies by outcome (protein intake/sarcopenia) and summarizes each study, including country, aims, population, oral health exposure, outcome measures, and key findings.
Summary of Measures of Exposure (Oral Health) and Outcome (Protein Intake and/or Measure of Sarcopenia) with the Number of Studies Reporting the Application of the Measure.
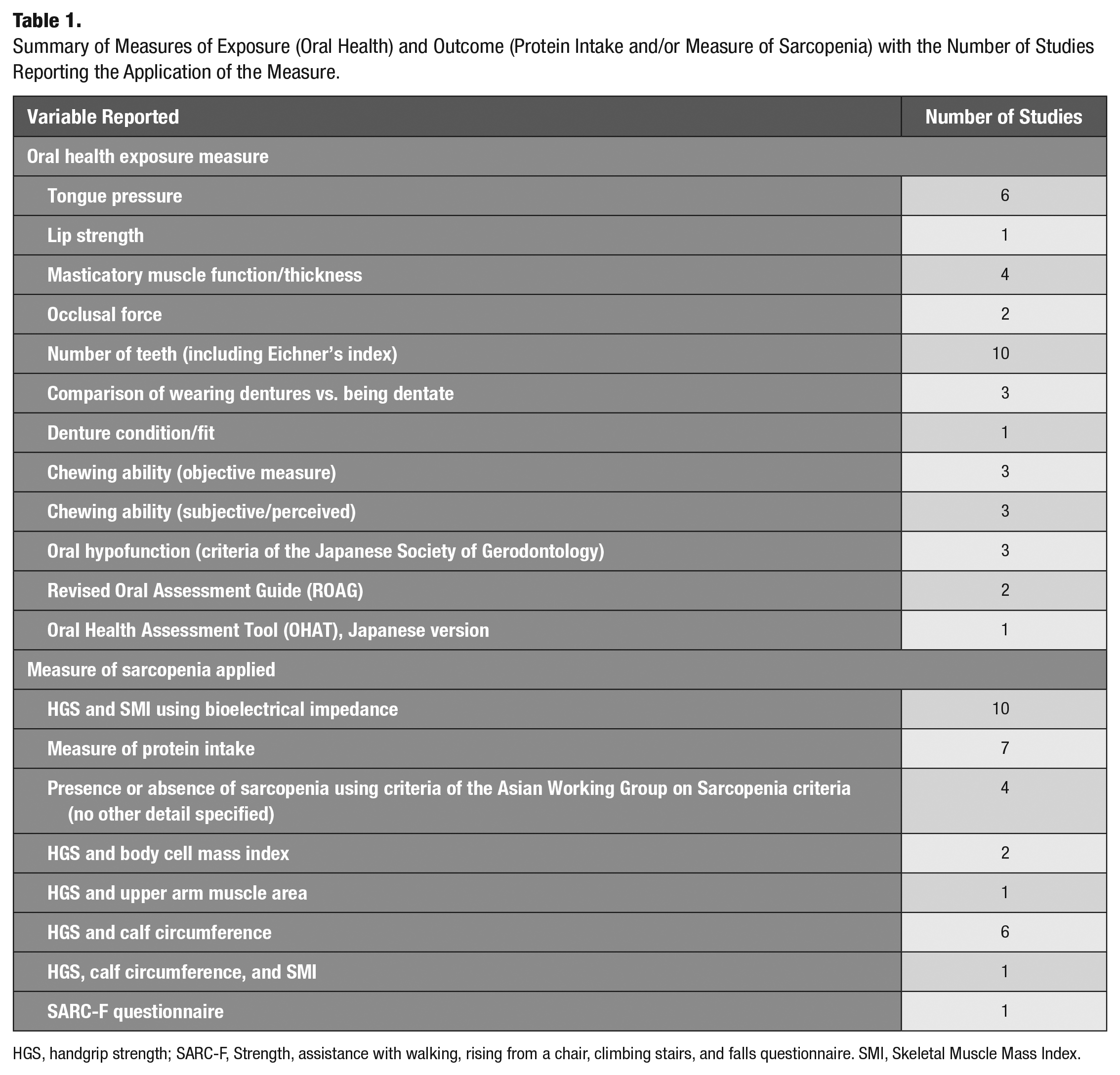
HGS, handgrip strength; SARC-F, Strength, assistance with walking, rising from a chair, climbing stairs, and falls questionnaire. SMI, Skeletal Muscle Mass Index.
Summary of Included Studies.

AMA, arm muscle area; BCMI, body cell mass index; BMI, body mass index; CC, calf circumference; Co-MS, coexistence of malnutrition and sarcopenia; CI, confidence interval; CRP, C-reactive protein; EAR, estimated average requirement; EI, energy intake; FFQ, food frequency questionnaire; FTU, functional tooth units; HGS, handgrip strength; IQR, interquartile range; JSG, Japanese Society of Gerodontology; LiLACS, Life and Living in Advanced Age Cohort Study; MMEI, masseter muscle echo intensity; MMT, masticator muscle tension; MNA, Mini Nutritional Assessment; MNA-SF, Mini Nutrition Assessment Short Form; MTP, maximum tongue pressure; MUST, Malnutrition Universal Screening Tool; NHANES, Nutrition and Health Examination Survey; NRS, nutrition-related sarcopenia; NS, not significant; NZ-NRV, New Zealand Nutrition Reference Values; OHAT, Oral Health Assessment Tool; OR, odds ratio; ROAG, Revised Oral Assessment Guide; SARC-F, strength, assistance with walking, rising from a chair, climbing stairs, and falls questionnaire; SES, socioeconomic status; SMI, Skeletal Muscle Mass Index; SMM, skeletal muscle mass; Y/N, yes/no.
For each measure of compromised oral function, the balance of studies indicating a positive versus null association between this measure and risk of sarcopenia is presented in Figure 2.
Discussion
The aim of this study was to scope the peer-reviewed literature pertaining to the relationship between compromised oral health and risk of sarcopenia and/or intake of dietary protein and to map available data by study type and volume of information, geographic location, measures of oral health and function, measures of sarcopenia employed, and measures of protein intake, along with an overview of findings and the balance of data showing an association versus no association. Overall, the findings show that despite the identification of a substantial body of evidence overall (contained in 29 articles), the evidence included a diverse number of measures of oral health that related either to the status of the dentition or to the oral musculature. No more than 4 studies related to any 1 oral health exposure and an outcome (sarcopenia or protein intake). Most data pertaining to the relationship between measures of compromised oral health and sarcopenia are cross-sectional in nature and from Japan, with limited data from the United States and Europe and no data from Latin America, Australia, or Africa, despite age-related sarcopenia being a global condition.
The balance of data shows an association between sarcopenia with loss of natural teeth, wearing dentures, lower occlusal force, and masticatory muscle thickness. The balance of data also shows that the number of natural teeth is associated with protein intake. The data suggest no association between presence of sarcopenia and perception of reduced chewing function or reduced masticator muscle function, with data on objective measures of chewing function showing mixed findings (Fig. 2). The balance of data pertaining to studies measuring tongue pressure or indices of oral hypofunction (e.g., Oral Health Assessment Tool [OHAT], Revised Oral Assessment Guide [ROAG], and oral hypofunction as define by Japanese Society of Gerodontology (JSG) was also mixed. A concept diagram summarizing balance of data pertaining to the association between oral health and sarcopenia is presented in Figure 3.
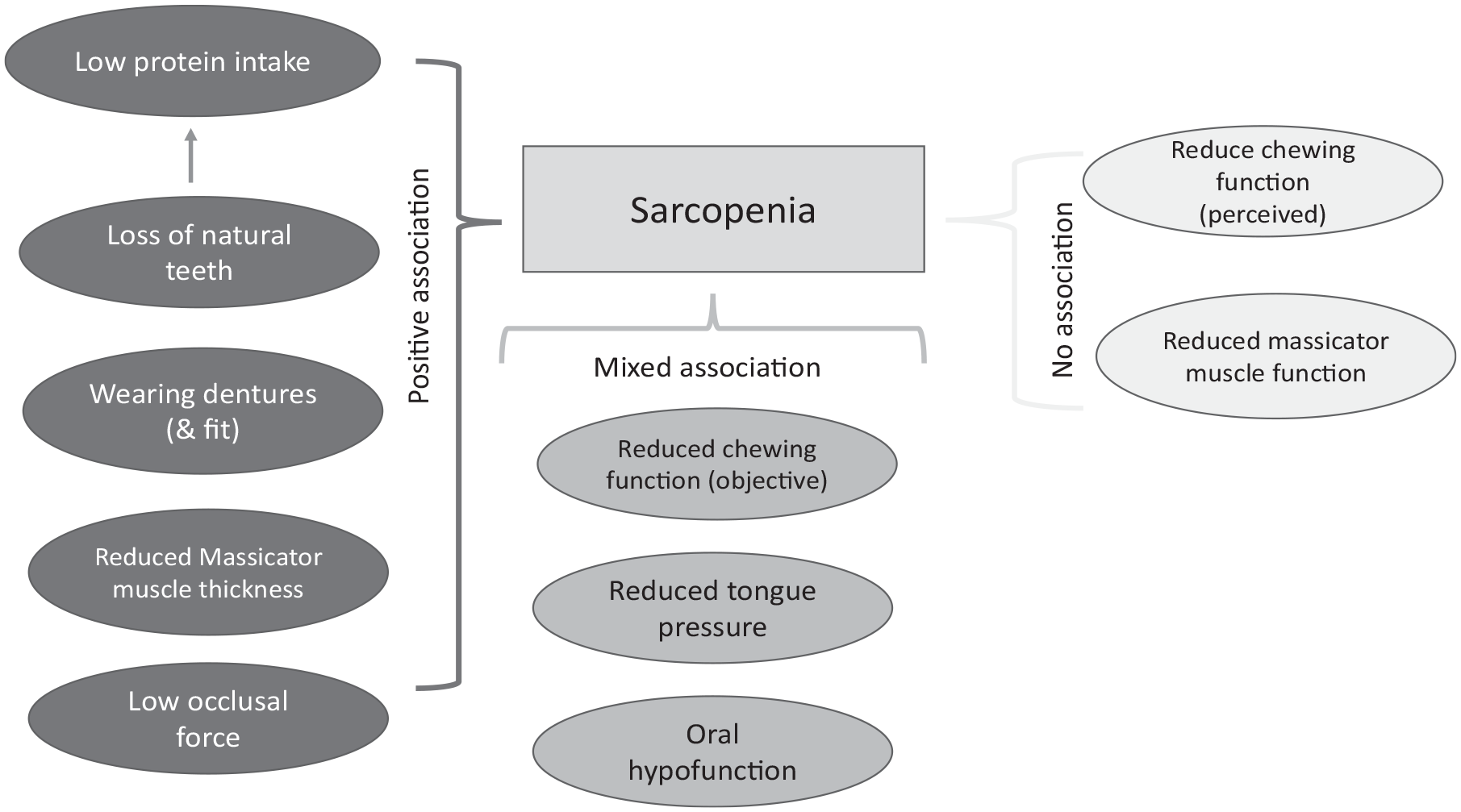
Concept diagram summarizing the balance of data pertaining to the association between oral health measures and sarcopenia.
The findings relating to number of teeth, which included longitudinal data, suggest that tooth loss may have an adverse effect on the intake of dietary protein; this could contribute to loss of muscle mass and function. This suggests that preserving natural dentition has a role to play in the prevention of sarcopenia through enabling the consumption of adequate dietary protein. Research has shown that intervention with dietary protein coupled with physical activity can increase muscle protein synthesis. To maintain muscle protein synthesis, a protein intake of 1.2 g/kg/d with 20 to 25 g with each meal has been suggested (Bollwein et al. 2013; Cruz-Jentoft et al. 2014), yet data identified in this review showed a lower tooth count was associated with protein intakes below 0.8 g/kg/d (Mendonça et al. 2018), and wearing dentures was associated with not meeting the estimated average requirement (the amount estimated to be adequate for 50% of a population) of 0.75 g/kg body weight (Ram et al. 2020). More attention is needed to support patients with tooth loss to consume adequate protein intake. Tooth loss may also affect other dietary factors such as intake of fiber and of fruits and vegetables (a good source of antioxidants), which were not explored in this review but probably are dietary risk factors in the etiology of sarcopenia (Welch et al. 2020). The findings cannot, however, rule out that those experiencing tooth loss eat a less healthy diet throughout life, which could place them at increased risk of developing sarcopenia in later life, independently of oral health status.
Only 3 studies included objective measures of chewing function, with 2 studies showing a positive association (Okada et al. 2010; Murakami et al. 2015) and 1 no association (Abe et al. 2001). These mixed findings may relate to the measure of chewing function used: Abe et al. (2001) counted bolus particles following chewing a gummy bear, whereas the other studies used color-changing chewing gum, which may give a more precise measure.
Over a quarter of studies reporting measures of sarcopenia assessed oral status using mixed-variable indices, such as the OHAT (Chalmers et al. 2005), ROAG (Ribeiro et al. 2014), and oral hypofunction (as defined by the JSG; Minakuchi et al. 2018). The mixed balance of data from these studies (3/6 reporting an association) may reflect the diverse measures included in such assessments. For example, in the assessment of oral “hypofunction,” having 3 of 7 criteria (relating to oral hygiene, oral dryness, occlusal force, tongue-lip, motor function, tongue pressure, masticatory function and swallowing function) classifies a person as having oral hypofunction. It is possible, therefore, that the nature of oral hypofunction in some people relates predominantly to dental-related elements (oral hygiene, masticatory function dryness), whereas for others, it relates predominantly to oral muscle function. Further exploration of data from these studies could help elucidate the relative impacts of tooth loss versus muscular impact, which would help to determine the direction of effect. The mixed balance of data relating to reduce tongue pressure and sarcopenia was not anticipated as it has been postulated that sarcopenia is a whole-body disease affecting the muscles of the oral cavity as well as skeletal muscles (Shimizu et al. 2021), and therefore one would expect sarcopenia to proportionally affect the muscles of mastication and skeletal muscles. Further scrutiny of data, including quality assessment (which was outside the remit of this scoping review), may help to shed light on the mixed findings. Moreover, longitudinal data are needed to elucidate the direction of effect between loss of tongue pressure and skeletal sarcopenia in order to establish whether oral health intervention to maintain tongue pressure has a role to play in the prevention of sarcopenia.
Authoritative definitions of sarcopenia, defined by the European Working Group on Sarcopenia in Older People (Cruz-Jentoft et al. 2014) and the Asian Working Group on Sarcopenia (Chen et al. 2020), stipulate that diagnosis of sarcopenia should include a measure of low muscle mass and either a measure of low muscle strength or low physical function, and both provide culturally appropriate cutoff values. Therefore, to be included in the current review, studies required a measure of muscle quantity and strength or function regardless of the methods used to assess these parameters. Most included studies used HGS to assess muscle function; however, a variety of methods assessed muscle mass (Table 1). The measures used may have affected the accuracy and precision; for example, muscle mass assessment measured using bioelectrical impedance is likely to be a more precise measure compared with anthropometric measures such as limb circumference. The use of different measures makes cross-study comparisons complicated; however, the aim of this review was to map the volume, nature, and direction of effect and not to assess effect size. Meta-analysis of data in any future systematic review would require uniformity in the definition of sarcopenia and its measurement.
Limitations of the Scoping Review
This scoping review only included data published since 2000 and therefore may have missed evidence published before this cutoff date. The review also did not include the gray literature and non-peer-reviewed articles such as preprints and abstracts. Moreover, the limited resources available for this research dictated that only articles that had an English abstract were included and did not allow for translation of full articles not published in the English language, meaning that some data may have been missed.
Future Research
Much of the existing data are cross-sectional in nature, and more longitudinal data and intervention studies are required to clarify whether the association between oral hypofunction and sarcopenia is a cause of effect or bidirectional. Elucidating the direction of effect will inform on whether oral intervention has a role to play in the prevention of sarcopenia. Moreover, because no studies were identified that reported the association between oral health measures and both intake of protein and a measure of sarcopenia, future studies should consider exploring if intake of protein and/or other dietary factors mediate any association between tooth loss and risk of sarcopenia.
Despite being included as a characteristic of oral hypofunction, this review identified no study specifically investigating any association between oral dryness and risk of sarcopenia. Oral dryness affects masticatory performance (Pedersen et al. 2002) and therefore is likely to affect ability to eat and nutritional intake. This warrants further investigation. This review specifically explored data pertaining to the condition of sarcopenia, and therefore articles reporting on the symptoms of physical frailty only but without reference to a measure of both muscle function and muscle mass were excluded: 47 articles fell into this category (Appendix Table 1).
Most of the available data pertaining to the association between oral health and sarcopenia identified in this review come from Japan (>75% of studies). However, with a growth in the aged population, sarcopenia is an increasing global public health issue: a recent systematic review estimates the global prevalence at approximately 10% in populations aged 60+ y (Shafiee et al. 2017). However, there is some suggestion that prevalence is considerable higher (~20%) in non-Asian populations (Shafiee et al. 2017). Therefore, analysis of data from cohort studies of older populations from a diversity of countries is needed to fully understand the significance of oral health in aging well from a global perspective.
Conclusion
This study has identified and mapped the broad range of oral health measures that have been studied in relation to the condition of sarcopenia. The balance of data shows that tooth loss is associated with risk, but data pertaining to oral musculature are mixed. More research, including data from longitudinal and intervention studies, especially from geographical locations outside of Japan, is needed to fully elucidate if oral health intervention has a role to play in preventing the condition of sarcopenia.
Author Contributions
P.J. Moynihan, contributed to the conception and design, data interpretation of the data, drafted the manuscript; J-L. Teo, designed the search strategy and mapping charts, data interpretation of the data, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jct-10.1177_23800844231157259 – Supplemental material for Exploring Oral Function, Protein Intake, and Risk of Sarcopenia: A Scoping Review
Supplemental material, sj-docx-1-jct-10.1177_23800844231157259 for Exploring Oral Function, Protein Intake, and Risk of Sarcopenia: A Scoping Review by P.J. Moynihan and J-L. Teo in JDR Clinical & Translational Research
Footnotes
Acknowledgements
The authors thank Vikki Langton, liaison librarian, The University of Adelaide, for her advice on the literature searches.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: P. Moynihan is a member of the Oral Health Advisory Council of Haleon (formally GlaxoSmithKline Consumer Healthcare) and her institution receives a fee with respect to this. J-L. Teo declares no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was made possible with an Adelaide Dental School Summer Student Scholarship.
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.