
Abstract
Improvements in oral health including increased retention of natural teeth have given rise to a partially dentate older population. Replacement of missing natural teeth is important to improve function, aesthetics and quality of life for this patient group. A variety of options are available to replace missing teeth in partially dentate older adults, including fixed, removable and implant retained prostheses. This article will discuss the provision of removable partial dentures including treatment planning and denture design. When planning removable partial dentures, careful attention must be paid to stabilising the patient prior to delivering any prosthesis. Partial dentures should be designed to minimise the potential for plaque accumulation with carefully designed metal based frameworks. Acrylic resin can also be utilised with attention to detail to minimise the risk of damage to delicate supporting tissues. Removable dentures have the advantage that they can be readily added to in the event of further tooth loss which may be particularly relevant for older adults. Partial dentures which optimise support, retention and stability can function very successfully and significantly improve patients’ oral health related quality of life.
Keywords
Learning Objectives
Understand the role that removable dentures play in managing tooth loss for older patients
Understand the factors that contribute to successful outcome with removable dentures
Describe the need for planning for further tooth loss in older patients
Introduction
Epidemiological evidence shows that people are retaining their teeth later in life. According to the 2009 Adult Dental Health survey, 85 year old patients had an average of 14 teeth 1 which suggests that tooth replacement might be necessary in this cohort. Replacement of some missing teeth via resin retained bridges and acceptance of a shortened dental arch in appropriate cases provides a good solution but this is not always possible. This article will look at tooth replacement with removable partial dentures.
The perception of dentures is often negative for both patients and dentists. Even well-made dentures can result in dissatisfaction for some patients so it is important to discuss their attitude to denture wear at the outset and be both empathetic and realistic about what can be achieved. In spite of this, it has been shown that dentures can improve quality of life for patients.2,3
Principles of denture design
The general principles of denture design include providing appropriate support, stability and retention while maintaining a hygienic design that is free from covering gingival margins where possible. In addition to this, older patients may present with teeth that have a questionable long term prognosis, so planning for failure needs to be incorporated into the design.
Support
Support may be provided by teeth, the residual alveolar ridge, the hard palate or a combination of these depending on the pattern of tooth loss. Tooth support has two key advantages over mucosal support:
The degree of displacement of the denture under load is reduced
There is increased proprioceptive feedback from the periodontal ligament when teeth are loaded reducing the potential for tissue trauma and improving chewing function
Figure 1 demonstrates a case where inadequate support has led to tissue trauma. The outline of the existing denture can be seen imprinted on the mucosa, suggesting that full palatal coverage may be indicated. Tooth support is more readily provided by a metal framework denture incorporating rests (Figure 2). Correctly designed and positioned rests direct occlusal loads down the long axes of the supporting teeth and these loads are well tolerated by a healthy periodontal ligament.
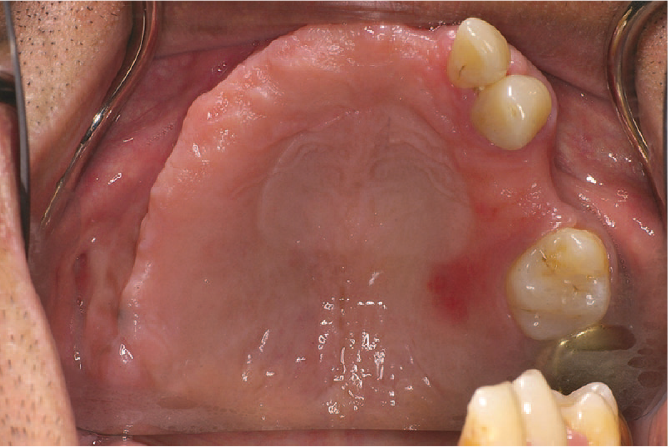
Mucosal trauma

Tooth supported denture
Acrylic resin dentures are more commonly prescribed in everyday practice as they are generally cheaper (at least in the short term) and quicker to provide. When tooth loss is more extensive and the advantage of tooth support is reduced, acrylic resin dentures may be preferred, particularly in the maxilla where palatal coverage can be used. While they derive support from the mucosa, some degree of tooth support can be provided by correctly extending the acrylic baseplate above the survey line of the supporting tooth (Figure 3). Unfortunately, the baseplate is commonly finished at or near the gingival margin, traumatising these delicate tissues and earning the epithet ‘gum stripper’ (Figure 4). Tooth retention in later life is strongly associated with improved quality of life so it is incumbent on the dental team to help the patient to preserve their existing dentition as much as possible and good denture design can contribute to this.
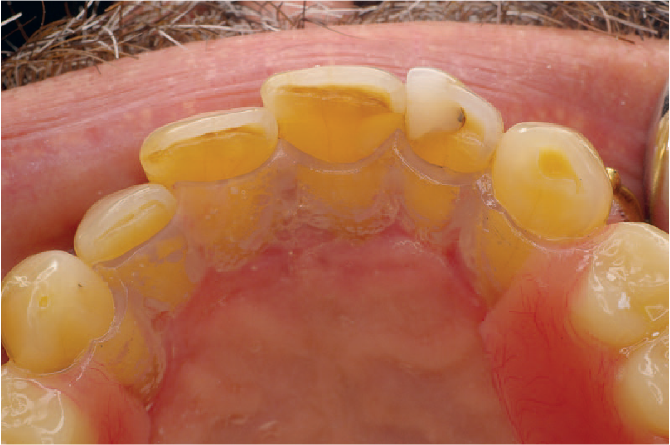
Acrylic border

Recession Associated with denture in situ
Patients often request for their denture to be constructed with reduced coverage, particularly in the palate where the denture may contribute to retching. In these circumstances the patient’s wishes need to be balanced against the need for good support. Retching is commonly associated with the thickness of the baseplate and the stimulatory effect this has on the tongue rather than its extension. Providing a thin palate in cobalt chromium may therefore be a more effective solution than an under extended acrylic plate.
Retention
Supporting teeth can also be used to retain dentures via the use of clasps. The effectiveness of clasps is enhanced by selecting an appropriate path of insertion for the denture and the use of guide surfaces. The ideal solution is to use a guide surface milled into a crown as this can be made perfectly parallel to the chosen path of insertion (Figure 5). However, this is a more expensive option and there needs to be justification for crowning the tooth.

Milled crown
The patient treated in Figure 6 was an older patient with cerebral palsy who struggled to maintain good oral hygiene. He had no previous denture wearing experience and the abutment teeth for the denture were slightly mobile. Rather than using clasps for retention, guide planes were employed to provide frictional retention. A cobalt chromium framework was used to keep the bulk of the denture to a minimum and was designed to allow for tooth addition in the future. This represents a pragmatic approach to denture construction as the abutment teeth were not ideal and the patient required a lot of support to maintain oral hygiene.

a) Framework in situ b) final denture in situ
The selection of teeth for clasping is often an afterthought and left to the technician, however, it should be a clinical decision. Many dental practices do not own a surveyor which is unfortunate as they can be bought quite cheaply and a few minutes spent selecting an appropriate path of insertion for a denture and positioning of clasps contributes significantly to retention. In many cases, only two clasps which are diametrically opposed will be sufficient to retain the denture, although it may be tempting to use more.
Stability
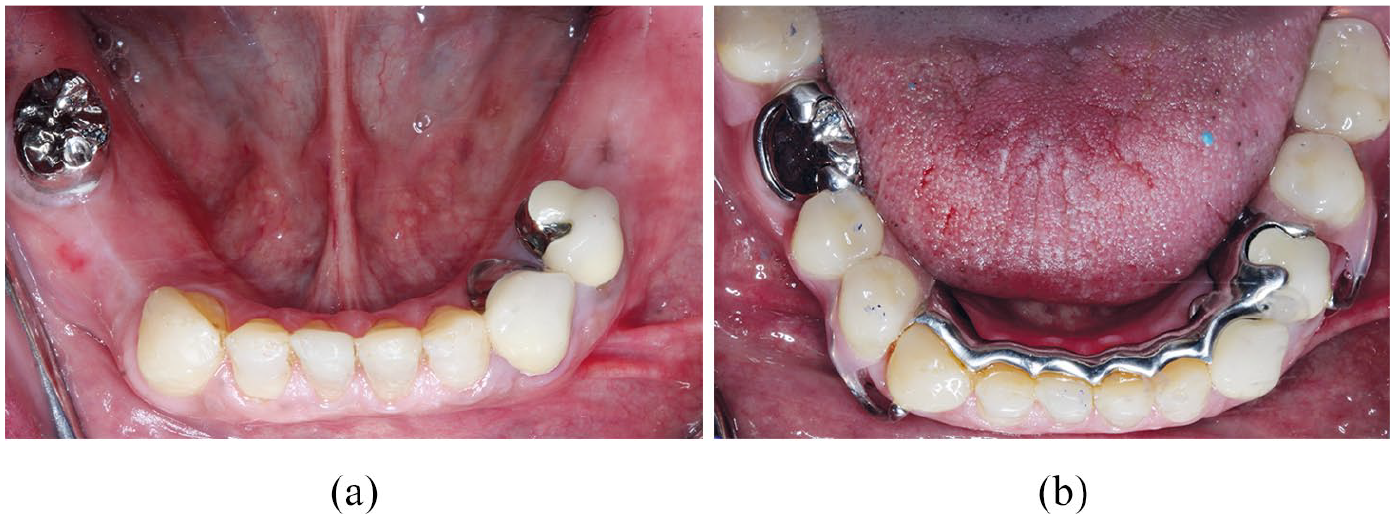
Denture stability is the resistance of the denture to displacement during function and destabilising forces may act through the occlusal, polished or fit surface. Retaining even a few teeth contributes significantly to the stability of the denture, particularly in the mandible, and this needs to be taken into account when treatment planning (Figure 7). Conversely, retaining one or two teeth in the maxilla will prevent the achievement of a peripheral seal and may reduce retention. In such cases, an overdenture or even strategic extraction may be indicated.

a) Before treatment b) after treatment
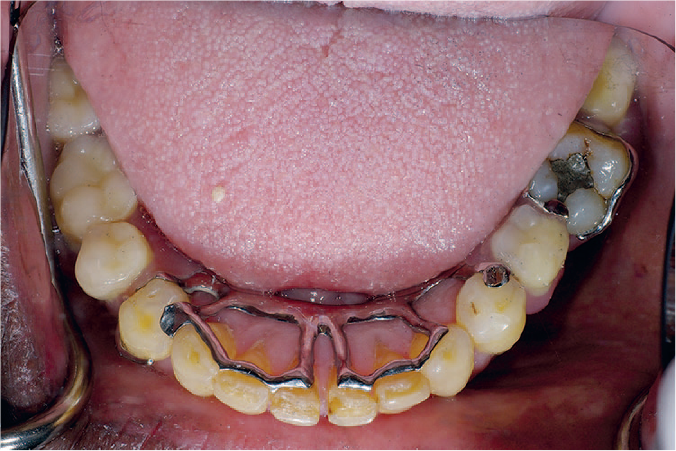
Bracing components in the denture will confer stability, although this may be at the expense of hygienic design. A dental bar with reduced gingival margin coverage (Figure 8) provides a solution to this scenario.

Example of hygienic design
Hygienic design
As long ago as 1952, DeVan stated that prosthodontics should concern itself with the preservation of remaining teeth over the replacement of those that are missing. Classic studies have demonstrated that covering gingival margins with removable prostheses results in an increase in the quantity and quality of plaque when oral hygiene is sub optimal.4,5
Dentures do not cause plaque to grow where the oral hygiene is good, but unfortunately the cohort of patients who benefit from dentures are often those who struggle with oral hygiene. 6 It is crucial therefore that dentures do not become slow, expensive extractors of teeth! Stabilisation of primary disease is important prior to commencing denture construction, and when this has been achieved, good denture design can help the patient to maintain oral health. There are two main ways that design can help:
Avoiding coverage of gingival margins with the denture connector. This is usually only possible with a metal based framework. Acrylic resin dentures may avoid margin coverage in the maxilla
Providing appropriate relief at the margin between the denture and the gingivae
As mentioned previously, bar connectors can be employed instead of plate connectors where appropriate. A European consensus document from 2002 on hygienic denture design clearly describes the principles and practice of this and is highly recommended reading. 7 Although these ideas have been present for decades and are widely taught, they are still not universally practiced, which may reflect ‘economic’ factors related to denture provision.
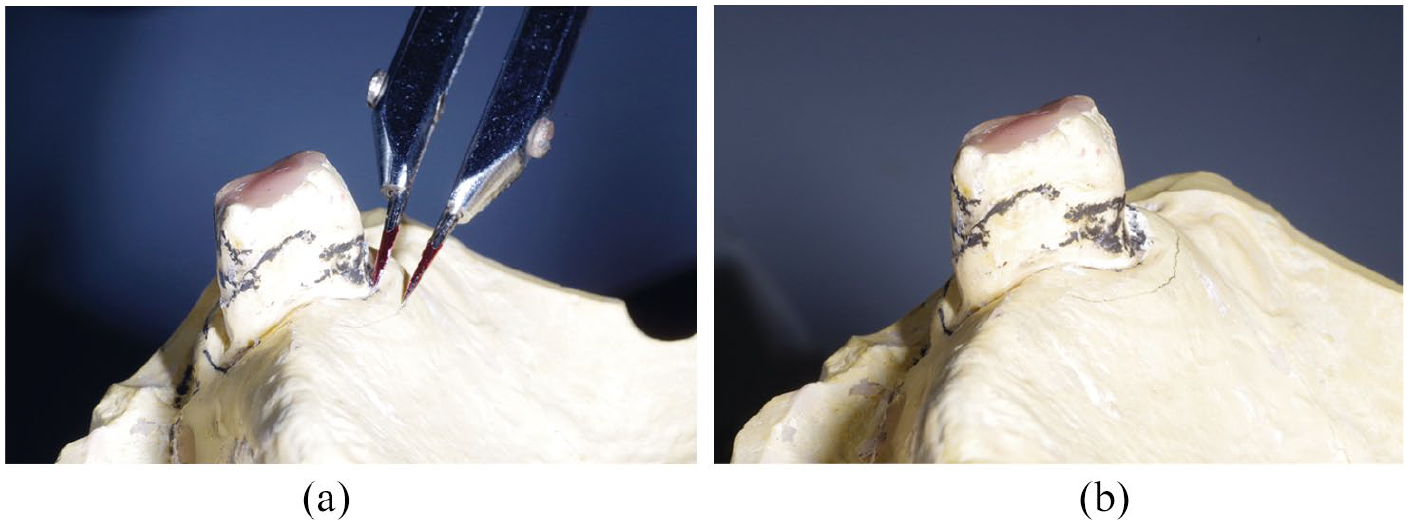
Hobkirk and Strahan 8 demonstrated that when gingival relief of up to three millimetres is provided at the junction between the denture and gingival margin, the gingival margin may hypertrophy into the space provided. They suggested that this enlargement was due to oedema and speculated that it makes plaque removal more difficult. Larger relief areas of 4 mm do not appear to result in such hypertrophy. This suggests that gingival margins should be widely relieved where possible or not at all (Figure 9a and b). Larger relief areas can be incorporated into the denture by asking the technician to block out an area of the cast between the survey line and a line marked 4mm from the gingival margin (Figure 10a and b).

a) Gingival relief b) no relief
a) Marking block out area b) block out area
Planning for failure
Older patients are more likely to present with a failing dentition due to the cumulative impact of tooth wear, periodontitis, caries and repeated restorations. It is difficult to assess the prognosis of individual teeth and evidence suggests that we are not very good at it, 9 with a tendency to condemn teeth that could survive given the appropriate therapy. 10 The problem when planning for removable partial dentures is that a ‘poor prognosis’ tooth may not provide a suitable abutment even if it’s short term survival can be assured. 11 In such situations, a pragmatic solution is to retain teeth and plan for their failure. This can help to stabilise new dentures and have a positive benefit on the patient’s psychological well-being (Figure 11a and b). Acrylic resin dentures are relatively easy to add to in the event of tooth loss and this may be achieved on an immediate basis, whereby the replacement tooth is added to an existing denture just prior to extraction, or shortly afterwards. 12 The denture may be regarded as transitional if further tooth loss is anticipated.

a) Poor prognosis teeth before b) poor prognosis teeth with denture
Cobalt chromium framework dentures are generally more costly and time consuming to fabricate, so the need to plan for failure becomes more important if the patient is to avoid a costly remake.
Planning for further tooth loss can be achieved by:
Providing metal backing on abutment teeth to facilitate adding an acrylic tooth to the denture. The case in Figure 12 shows upper right lateral incisor previously root canal treated and restored with a post crown. There is radiographic evidence of apical radiolucency but the tooth is asymptomatic. The patient did not want the tooth investigated so a metal backing was provided in case problems arise in the future and the tooth was not deemed restorable
Rest seats and/or milled ledges can be incorporated into metal or ceramo-metal crowns, if it is anticipated that a denture will be required in the future
Providing additional tooth support adjacent to poor prognosis tooth. Figure 13 shows a metal framework at the try-in stage. The design maximises support where teeth exhibit extensive attachment loss while at the same time being relatively hygienic (Figure 14)
Endodontically treated teeth which are used as a terminal abutment in a free end saddle exhibit a higher degree of failure than vital teeth. 13 Siting a rest on the mesial side of the tooth, as in the RPI system, may counteract this and allow for ease of addition (Figure 15)
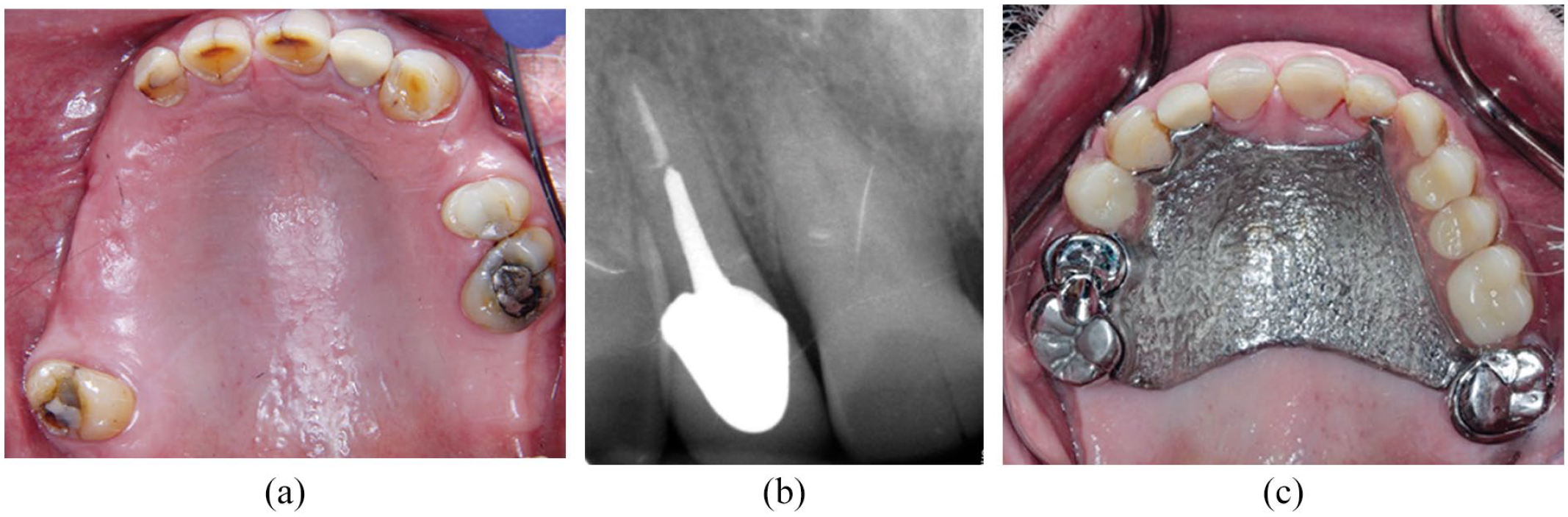
a) Plan for loss of UR2 b) UR2 radiograph c) denture in situ

Planning for failure - framework in situ
a) FES case before treatment b) FES denture in situ
Use of a mesial rest adjacent to a free end saddle (right side)
Planning for success
Where teeth require extracoronal restorations, it can be of benefit to incorporate design features into the restorations to enhance the success of the denture. 14 So called ‘smart’ crowns may have milled ledges, rest seats and contours for clasp assemblies. They have the advantage over precision attachments in that they have lower complication rates which may be more suitable for the older patient. 15 However, tooth preparation may be more destructive if it is to incorporate the proposed features.
In Figure 16, the patient was provided with four ceramo-metal crowns incorporating a ledge for a planned dental bar. The denture design needs to precede tooth preparation and must be conveyed to the technician along with the crown prescription. It is helpful to include a diagnostic wax up of the proposed crowns to reduce the chance of design errors.

Milled crowns and denture
Another consideration in treatment planning is how to manage failing bridge work subsequent to dismantling and stabilising the dentition. It is often worthwhile to construct single ‘smart crowns’ rather than longer span bridges to enhance a denture. Although this commits the patient to a removable prosthesis, it is easier to maintain which is an important consideration for the older patient.
Dentures and tooth surface loss
As teeth are retained later in life, they will be subject to greater tooth surface loss. In many cases a physiological level of tooth surface loss can be monitored without the need for restorative intervention. However, when the tissue loss becomes severe, or when it is associated with tooth loss, partial dentures may be needed. It is beyond the scope of this article to discuss the management of tooth surface loss in detail, but there are a couple of factors, in particular, that need to be considered when planning dentures:
Does the vertical dimension need to be increased or merely restored back to its correct level? In the former case, the patient will present with a normal freeway space and may require a diagnostic denture to assess tolerance to the new vertical dimension. In the latter case, the freeway space is increased and may be associated with a forward slide of the teeth from the initial contact with the mandible in the retruded position. Restoring the patient in this retruded position is usually more straightforward and a diagnostic denture may not be required to test tolerance to the new vertical dimension
Is the tooth surface loss so extensive that the denture needs to compensate for it via the use of onlay, overlay or overdenture in the design? Figure 17 shows a case where a temporary denture was provided for an 82 year old lady with no previous denture wearing experience. Although the junction between the tooth and denture surface is quite obvious, it was concealed by the lip line and was worn satisfactorily before proceeding to definitive treatment
One problem associated with managing tooth surface loss with dentures is the potential for fracture of the prosthesis. It may be necessary to increase the bulk of material used to counteract this which may result in problems with tolerance, particularly if the patient is wearing a prosthesis for the first time at a later stage in their life.
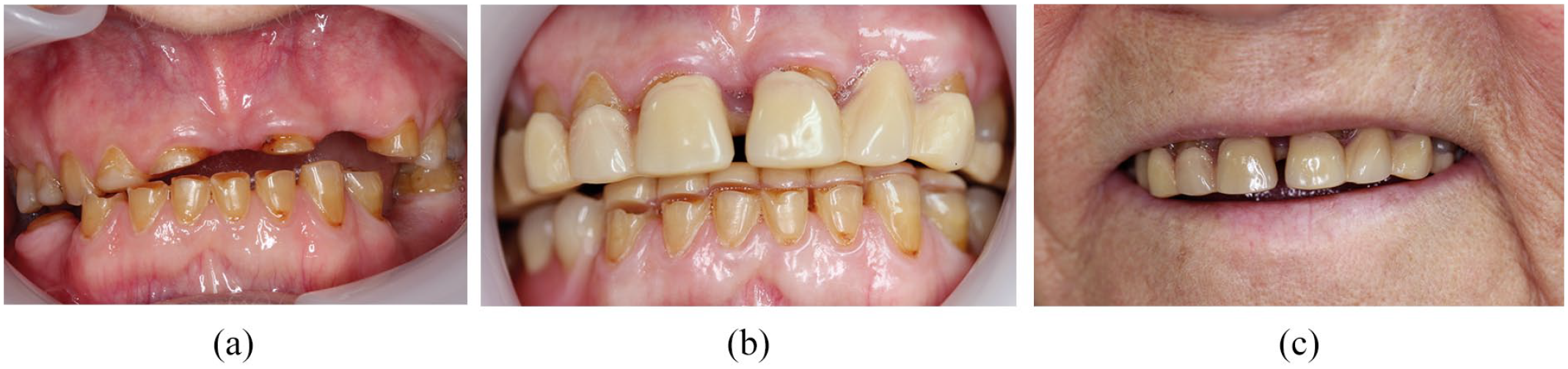
a) TSL anterior view b) temporary dentures in situ c) temporary denture facial view
Conclusion
Although people are retaining their teeth later in life, the need for partial dentures will remain for the foreseeable future. Partial dentures can provide satisfactory outcomes for patients if they are designed to provide optimum support, stability and retention and to be hygienic. Stabilisation of the mouth prior to the provision of dentures is crucial to ensure that oral health does not deteriorate after treatment and regular follow up is required. As wearing a prosthesis may increase the risk of oral disease, recall intervals should be adapted accordingly. Where tooth survival is in doubt, appropriate denture design may anticipate further tooth loss to minimise the need for remakes.