
Abstract
Background:
Social justice, empathy, and social responsibility are emerging themes in dentistry. Many dental faculties have started incorporating these concepts into their curriculum, but our knowledge of the effectiveness of these initiatives remains limited.
Purpose:
The objective of this study was to understand how students and educators perceive the role of social justice education, if any, in the undergraduate dentistry program.
Methods:
This qualitative study was performed by using semistructured interviews with students, professors, and clinical faculty at the Université de Montréal dental school from January to May 2020. Eighteen participants were recruited through purposeful sampling until saturation. The interviews were recorded and transcribed integrally. They were coded with QDA Miner 5.0 (Provalis). Thematic analysis was undertaken to elucidate emerging themes via qualitative methodology.
Results:
Five themes emerged from the results. Certain students were more inclined to be interested in social justice and participate in voluntary community-based activities. There were gaps in current teaching methods, including a lack of exposure to alternative treatment plans (e.g., extractions vs. endodontic treatments) better suited to patients’ financial or social situations. Some barriers to teaching were identified, the most important being a lack of time. Desired teaching of social justice would include increased awareness and active student participation and taking responsibility to motivate action to produce social change. The application of social justice in dentistry involves care that is accessible and adapted to a patient’s individual needs.
Conclusion:
The results of this study provide valuable insight for the development of a social justice education curriculum in dentistry that can be evaluated and validated to train socially competent dentists who can provide patient-centered care to the community.
Knowledge Transfer Statement:
The results of this study can be used by dental educators and administrators who are looking to incorporate social justice education into their dental school undergraduate curriculum. The findings serve as a starting point to foster discussions and inspire change to reduce inequalities within the dental health care system.
Keywords
Introduction
In 1978 the World Health Organization declared that health is a fundamental right of all human beings. Health inequities exist not only among countries but within societies. As such, in many jurisdictions, governments have an important responsibility of ensuring access to health care for their population.
It is well known that individuals who benefit from a higher socioeconomic status are in better health than their underprivileged counterparts (Watt 2007). This phenomenon is reflected in oral health. An Australian study showed an inverse linear correlation between socioeconomic status and 2 determinants of oral health: the OHIP-14 (Oral Health Impact Profile–14) and missing teeth (Sanders et al. 2006). These findings were not found to be related to personal negligence. When it comes to health determinants, the importance of socioeconomic factors and health care systems is often underestimated (Jarvis and Wardle 2006).
As health care professionals, dentists have a social responsibility to work toward decreasing oral health disparities. Health care is a fundamental human right, and as such, all members of society should have access to the care that they require. To ensure social justice is to ensure that the system in place allows for equitable access to resources, which includes equitable access to health care.
The mechanisms of oppression in our society are complex, and the consequences of injustice are seen at many levels (Adams 2007). Indeed, persons with social identities that are not privileged in society face significant barriers to health care. These populations are often underserved when it comes to their oral health. Attitudes toward underserved populations are variable and can be influenced by characteristics such as age, gender, race, and socioeconomic background (Davidson et al. 2007; Carreon et al. 2011). Clinical and nonclinical experiences affect dentists’ desire to treat the underserved, as do contextual considerations, such as the communities to which they are exposed (Davidson et al. 2007; Alraqiq et al. 2020). These factors influence dentists’ willingness to treat vulnerable and underserved populations. One study showed that only 46% of dentists who completed their return of service in an underserved area continued treating vulnerable populations afterward (Mofidi et al. 2002). In the United States, less than half of dentists participate in Medicaid (American Dental Association 2016). While dentists feel responsible for patients who seek their care, they do not seem to feel professionally obliged to treat the underserved (Chen et al. 2016). Some data indicate that dentists are not as interested in public health as they are in other aspects of dentistry. In a survey of 410 graduating dental students and recent graduates, no respondents wanted to specialize in public health, while the other specialties were chosen by between 2% and 8% of respondents (Dhima et al. 2012). A study conducted in the United Kingdom on student career choices concluded that medical students were more motivated by altruism while dental students were more motivated by remuneration and the nature of the profession (Crossley and Mubarik 2002). Alarmingly, students have shown a tendency of becoming less altruistic during dental school (Coulter et al. 2007).
The goal of social justice education (SJE) is to help students become more aware of societal injustices, to examine and be critical, and to recognize their own positions in systems of oppression to motivate action to interrupt oppressive patterns and bring on societal change (Adams et al. 2007). Dental education is increasingly focused on patient-centered care (Eriksen et al. 2008). Dentists have a contract with society, which implies that they place patients’ needs before their own (Project 2002). As such, altruism is a key component of developing dental students’ professional identities.
The application of social justice has traditionally been associated with the concept of developing professionalism in dental education. Professionals distinguish themselves not only by their levels of knowledge and skills but also by the confidence that they inspire from the public and their commitment to serving their communities (Beemsterboer 2006). In 2006, Graham suggested 3 time points where evaluating dental student professionalism can be optimized to better serve the community: before, during, and after dental school. Many dental schools have incorporated SJE into their curricula (Bedos et al. 2018). The Dental Pipeline Program proved to be successful in increasing underrepresented dental students and using community-based dental education to prepare students to treat vulnerable populations (Carreon et al. 2011). Nonetheless, there is still a need to better understand the barriers to the incorporation of SJE to train socially competent dentists (Noushi et al. 2020).
To understand what can be done during the undergraduate curriculum to train dental students to be socially competent, this study sought to answer the following question: How do students, clinical instructors and professors, and the Université de Montréal School of Dentistry perceive the incorporation of SJE into the undergraduate curriculum? The aims of this study were 1) to understand how students and educators envision social justice in their curriculum, 2) to identify barriers to SJE, if any, and 3) to examine how dental schools can better train socially competent dentists by incorporating SJE into their programs.
Method
This study was reviewed and approved by the Université de Montréal Institutional Review Board (CERC-19-075-D). An interpretive approach based on grounded theory methodology was used for this qualitative research study. Grounded theory seeks to explain a phenomenon by generating a theory based on data acquired in the field (Creswell et al. 2007). The strength of this type of research is to better understand complex phenomena within a specific context.
The research field was the dental school at the Université de Montréal. The undergraduate dental program consists of a 5-y curriculum combining theoretical, preclinical (laboratory), and clinical teaching. The research team was composed of professors with knowledge of qualitative research methodology and an interest in reducing social inequities. The principal researcher conducting the interviews was a professor who taught subjects unrelated to the current research topic. The supervising researcher was an expert in qualitative research as well as social justice, equity, and diversity in the dental curriculum.
Participants were aware that their decision to participate or not, as well as their answers, would have no impact on their academic standing. A purposeful sampling method was used. Students, clinical instructors, and professors at the Université de Montréal were recruited through flyers and email to participate. To be included in the study, participants must have been ≥18 y old, francophone, and members of the dental school for at least 4 mo. This was to ensure that the data were reflective of each participant’s personal experience at the dental school. Written informed consent was obtained from all participants.
A sociodemographic questionnaire was completed by all participants. Individual semistructured interviews based on a data collection tool with open-ended questions were conducted by the primary researcher, in person or virtually due to the COVID-19 pandemic, until saturation was achieved. Interviews lasted between 20 min and 1 h and were conducted between January and May 2020. The goal was to allow the participants to develop their ideas and have freedom of expression on the topic.
Interviews were recorded and transcribed integrally for coding and analysis with QDAMiner 5.0 (Provalis). The data were digitally coded by the primary researcher using an open coding scheme. A random sample of the data was countercoded by an external researcher, and intercoder reliability of 91% was observed. Codes were then grouped into categories. Emerging themes were analyzed and interpreted, and a conceptual framework was created. Triangulation was ensured by having different sources of information, which allowed the research team to obtain a portrait of the current situation from various viewpoints. Participants’ information remained confidential.
Results
In total, 18 participants composed the study sample: 7 students, 7 clinical instructors, and 4 professors. Clinical instructors were community-based dentists who supervised students in clinic. Professors were those with an academic teaching position at the university, including theoretical and clinical teaching as well as research, who also treated patients in private practice. Students from 4 of the 5 y of dental school were represented. Eleven women and 7 men participated in the study. Eight participants identified as Canadian, 4 as Canadian and another ethnicity, 4 as another ethnicity, and 2 did not answer the question.
Five themes emerged from the data: student characteristics, current teaching methods, barriers to teaching, preferred teaching, and application of social justice. Students were perceived to exhibit differences in their social consciousness, which influenced their desire to serve their communities. Social consciousness was seen as something internal to the individual. Intrinsic values were found to influence participants’ attitudes toward social justice. In general, students were perceived to come from privileged backgrounds.
Most participants (15/18) declared that current teaching of social justice was rather implicit and that it was briefly mentioned in some classes but mostly implied in daily interactions. There were no specific courses dedicated to teaching social justice. Certain notions were covered in other courses, such as ethics, philosophy, law, and populational approaches. In the clinical setting, exposure was also variable, and clinical staff members had different approaches to if, how, and when social justice was discussed. Not surprising, there was no formal evaluation on social justice in the current curriculum. Students and teachers agreed that the dental school setting provides exposure to a diverse population, including different racial, cultural, and socioeconomic groups. Outreach clinics, where students may have rotations, aim to offer services without judgment or discrimination to marginalized communities, such as new immigrants, people in financial difficulty, members of the LGBTQ+ community, and those experiencing homelessness. However, many of these extramural rotations in underserved communities and populations are voluntary; therefore, many students lack exposure to these diverse groups.
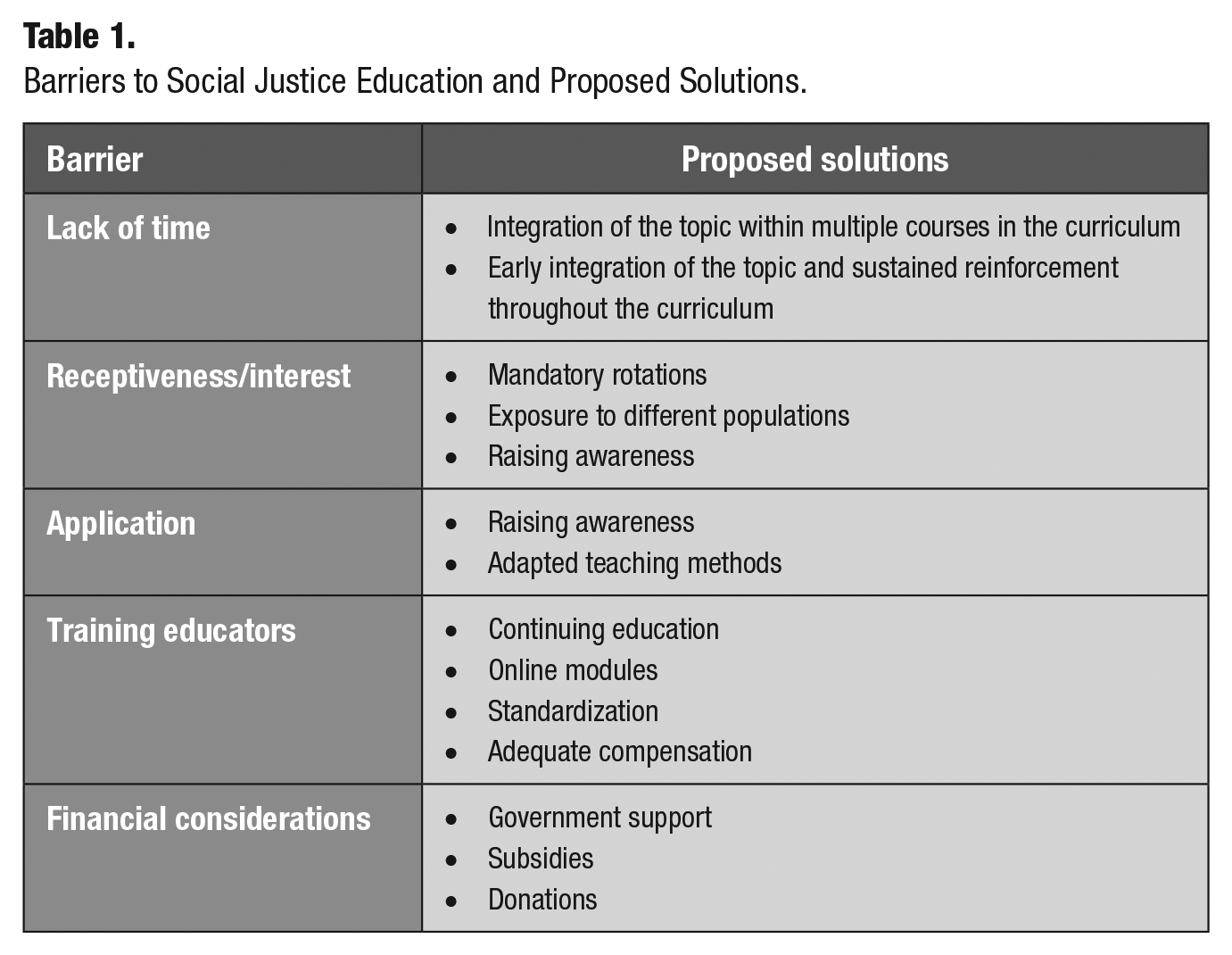
The main barrier to teaching social justice appeared to be a lack of time in the curriculum. Opinions were varied on whether students would be receptive to the idea or not. Some participants felt that it would be a sensitive topic and that discussions may be uncomfortable. It was also mentioned that training educators would be necessary to ensure that the same values were taught throughout the curriculum. Financial barriers included the cost of running a dental office as well as the cost of human resources, such as hiring clinicians to staff outreach clinics. Table 1 outlines the main barriers to SJE and proposed solutions to overcome them.
Barriers to Social Justice Education and Proposed Solutions.
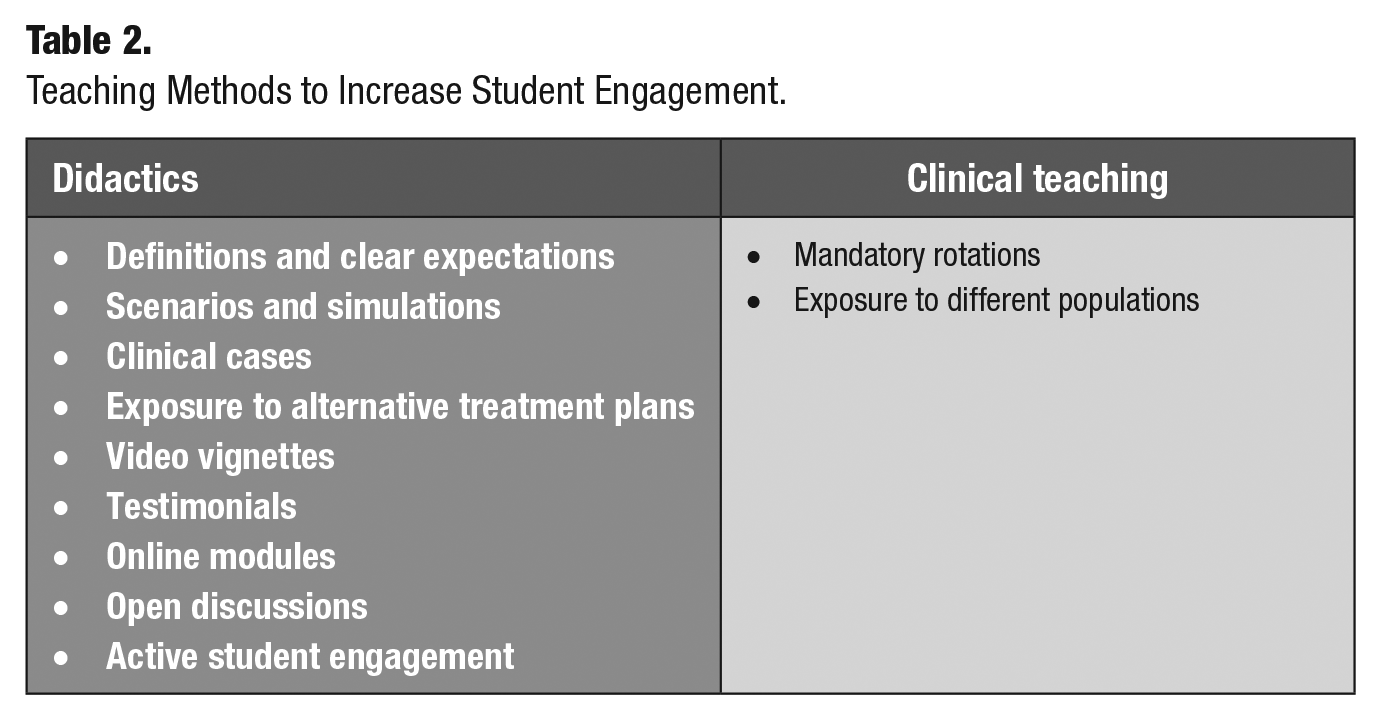
Students and teachers agreed that the ideal SJE program would include increasing awareness through early exposure, integration of the concept in other courses, and sustained teaching throughout the curriculum. Indeed, student awareness was mentioned in the majority of the interviews (16/18). The teaching techniques suggested—in order of frequency—were role-playing, exposure to diverse populations, internships, video vignettes, online modules, testimonials from patients and field workers, and open discussions. Active student engagement appeared to be an important aspect of teaching. In the clinical setting, increasing exposure to diverse populations would help students integrate the concepts they have learned. Students could also be evaluated by how they interact with the patients during their care. Table 2 shows proposed teaching methods to increase student engagement. Finally, clinical exposure to diverse populations should occur throughout the curriculum. Figure 1 presents a schematic representation of the model that we propose.
Teaching Methods to Increase Student Engagement.
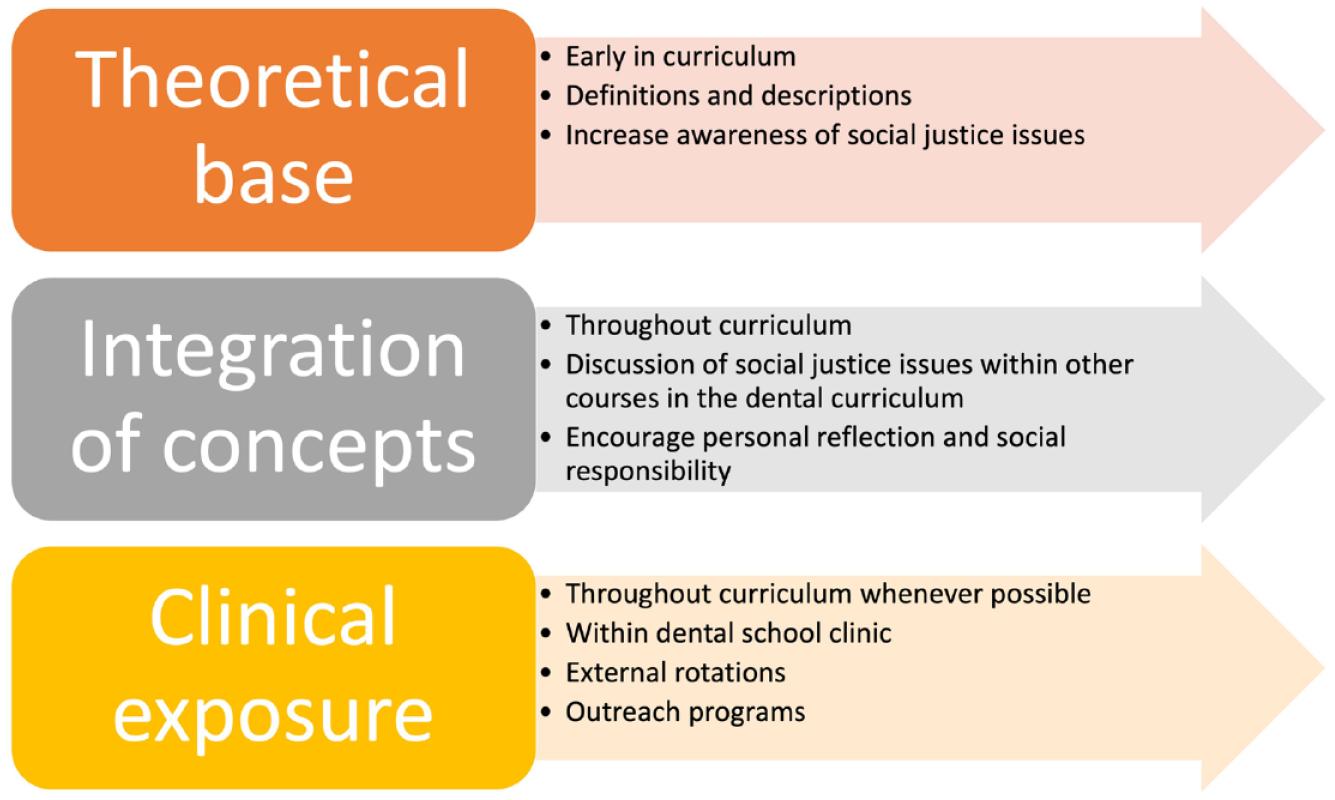
Schematic representation of proposed integration of social justice education in a dental school curriculum.
The goal of SJE is to apply the concepts as a practicing dentist. This translated to being able to provide accessible care, adapted to each patient’s needs, without judgment or discrimination. The principle of equity and absence of discrimination was mentioned in 62% of the interviews (12/18). For the participants in this study, providing accessible care meant providing care that was affordable to the patient. The objective of being able to apply social justice would therefore imply being able to increase the population’s access to health care. In the socioeconomic context of Canada and the province of Quebec, where dental care is covered by the government for a small percentage of the population, financial factors seem to be an important barrier to providing accessible care. In addition, cultural differences and the value placed on oral health are variable, depending on the population. Economic constraints were mentioned more often than societal values. Finally, while social consciousness is associated with the individual, social justice seems to stem from an increased collective social consciousness.
Discussion
Personal values and life experiences have been identified as contributing to the development of social consciousness. Indeed, the voluntary involvement of students in activities promoting social justice was associated with an internal motivation on their part. These results suggest that altruism is an innate characteristic, at least in part. By emphasizing community involvement in the admissions process, dental faculties could recruit a cohort of students who are more likely to be interested in caring for vulnerable populations (Beemsterboer 2006). There is a certain perception at the Université de Montréal that dental students generally come from privileged backgrounds. This perception could exist in other Canadian or North American faculties. This study did not explore participants’ motivations for becoming dentists; however, other reports have suggested that dental students are more motivated by financial security than the altruism associated with the profession (Crossley and Mubarik 2002; Gallagher et al. 2008). A focus on students’ motivations for becoming dentists during the recruitment phase may help to increase the proportion of dentists interested in social justice.
The implicit nature of current SJE was consistently mentioned by students as well as teachers. The topic seemed to have been covered in several courses, but students had no concrete definitions or guidelines on how to apply social justice practically. In clinics, exposure was variable, depending on the clinician teaching and the student’s motivation to become involved in electives in disadvantaged settings. Observed gaps in the curriculum include the fact that many community rotations are optional and that alternative treatment plans that might be better suited to certain populations—particularly those with financial constraints—are not discussed. The lack of exposure to specific populations in the curriculum and the lack of discussion of alternative treatment plans were points mostly brought up by professors and clinical staff. The fact that students do not yet know what is missing from their education before they are exposed to independent practice could explain this phenomenon. Current teaching at the university in which this study was conducted did not seem to prioritize personal reflection. This teaching tool is frequently used to help students think critically and reflect on their experience in the community (Furlini et al. 2018). It appears that by integrating reflection in social justice teaching, students could more easily move from knowledge (being aware that a problem exists) to action—that is, the application of social justice in the community. Lack of time was also identified as a barrier by students, clinicians, and faculty. When it came to student receptiveness, opinions were divided between those who believed that students would be receptive and those who had doubts. This may reflect the influence of students’ personal values on social consciousness. Several studies highlight the importance of teachers’ influence on students (Noushi et al. 2020). Having educators who share values of altruism and a sense of social justice would have a positive influence on students’ perceptions of these topics. Although the strong emotions sometimes provoked by a sensitive topic such as injustice have been reported in other studies (Pilcher et al. 2008), this has not been identified as a significant barrier in our population. It is interesting to note that in this study, monetary considerations were not raised by students, only by professors and clinicians. This could be explained by the fact that students are not involved with the management of finances at the dental school. Professors and clinicians, however, have more of an understanding of how finances can be a barrier to certain treatment plans. Insurance coverage varies by jurisdiction and can significantly affect access to care.
The most frequently mentioned element required for adequate teaching of social justice was student awareness. The importance of this awareness and recognition of the professional’s position in the patient-professional relationship has also been suggested by Stone (2008). Situational exercises to complement theoretical teaching are supported by the literature (Lévesque and Bedos 2011). Beyond awareness, a recognition of one’s placement within systems of inequality and a sense of responsibility are required to effect change (Hackman 2005; Hahn Tapper 2013). Personal reflection is key to achieving this goal. Desirable features of SJE were the introduction of the concept early in the curriculum, integration of the topic into other courses, and, to a lesser degree, sustained teaching throughout the curriculum. An interesting model would be to introduce social justice in a theoretical way, including a clear definition, at the beginning of the undergraduate course. This facilitates the integration of the concept into other courses, particularly in terms of patient approach and treatment plans, and it encourages personal reflection on the dentist’s responsibility to society. This is on par with similar changes proposed in graduate medical education (Siegel et al. 2018). The Association of Canadian Faculties of Dentistry recently published a document detailing 5 competencies that must be acquired for a dental student to graduate. Social justice is part of the competency entitled “health promotion.” To achieve this competency, students must be able to “recognize the determinants of oral health,” “describe the ethical and professional issues inherent in health advocacy, including altruism, social justice, autonomy, integrity, and idealism,” and “describe the role of the dental profession in advocating collectively for health and patient safety” (Charbonneau et al. 2019). Indeed, support from accrediting bodies is necessary to ensure that social justice is being taught in dental schools.
The term “social justice” was often associated with the concept of accessibility to care and care tailored to the needs of a particular population. In terms of care that was adapted, this was very often associated with the patients’ financial situation. SJE is intended to raise awareness and encourage personal reflection so that students can have the tools that they need to provide appropriate and accessible care to a greater number of people. A society’s socioeconomic context also has an impact on the perception of social justice. The two elements raised were financial considerations, i.e., the fact that dental care is not covered by the government and is not always affordable for the general population, and the value that society places on oral health. Quebec’s sociocultural values, where teeth are traditionally perceived as aesthetic and nonmedical and the dentist is often seen as an entrepreneur and not a caregiver, could explain the exclusion of most dental care from the public health care plan. An additional role of education would therefore be to train dentists who are more aware of political and cultural issues and would thus be better able to be active at the government level to promote organizational change (Lévesque and Bedos 2011).
Currently, there are no tools that measure or evaluate SJE in dental schools. There has been increased awareness of the need for such tools in medical education (Batra et al. 2020; Ross et al. 2014). By better understanding where dental schools currently stand with regard to SJE, by identifying the current barriers and proposed improvements, and by sharing knowledge and findings with our colleagues in other health care fields, we can work toward developing such a tool to evaluate and ultimately improve programs that will contribute to reducing inequities in dental health care services.
Theoretical Framework
Students’ individual characteristics as well as their life experiences influence their attitudes toward disadvantaged populations as well as their altruistic behaviors (Davidson et al. 2007; Holtzman and Seirawan 2009; Carreon et al. 2011; Alraqiq et al. 2020). The influence of teaching activities has also been suggested, but the effectiveness of these methods has yet to be validated. We believe that teaching plays an important role and adds to a student’s values and life experience to develop social awareness. A socially competent dentist is better able to act at the societal level by providing appropriate, accessible, and nondiscriminatory care. The professional patient-dentist relationship, with government support and increased public awareness of the importance of oral health, would all be essential for increased social justice in society. Figure 2 represents a conceptual model intended to optimize SJE in dentistry with the goal of training socially competent dentists. It can be used as a tool by dental schools to foster discussion on areas of improvement in the curriculum. It is important to note that recognition of the current shortcomings and freedom for students, faculty, and administrators to discuss these topics without retribution are critical to effect positive change.
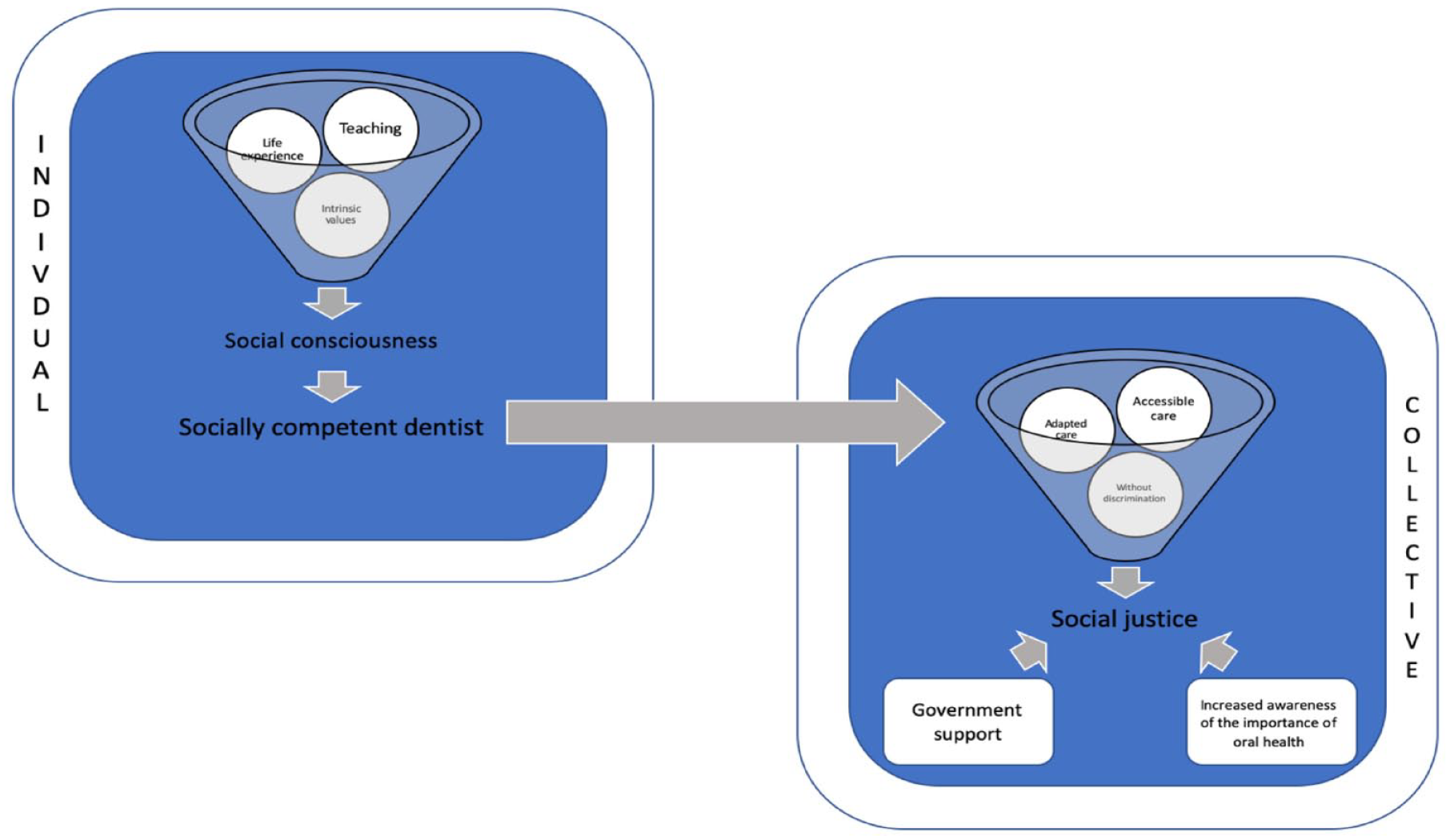
Conceptual framework: social justice education in dentistry.
Limitations
A major limitation of this study is that the recruitment of participants was on a voluntary basis. Thus, it is possible that the participants were already predisposed to being interested in the topic of social justice and having a more developed social conscience. However, many of their comments were about their observations of others as well as their own opinions. An inherent limitation of qualitative studies is that participants are recruited in a single institution and context. Thus, our results may not be generalizable to a global population.
Conclusion
As professionals, dentists have a contract with society to provide just and equitable care. Many factors influence dentists’ altruistic behaviors, such as their individual characteristics and experiences. Undergraduate dental education plays an important role in developing socially competent dentists. Although the majority of dental programs offer some form of social justice curriculum, this curriculum is not consistent, its effectiveness is not well known, and there are significant gaps identified by students and faculty in our study. Improved SJE would include increased student awareness and a variety of teaching methods that involve active student participation, such as role-playing, open discussion, and personal reflection, to help students recognize their positions in a system of inequality, to foster responsibility, and to encourage action to reduce injustices in society. We suggest that these teachings be integrated early into multiple levels of the curriculum and be sustained throughout the entirety of the program.
There are few barriers to these types of teachings, and the solutions are practical and feasible. Improved SJE would promote the development of social consciousness in students and help to produce socially competent dentists. We hope that increasing dentists’ awareness of social injustices will help to solidify dentistry’s position in the health care system and foster interdisciplinarity, reconcile the caregiving and entrepreneurial components of the dental profession, and train dentists to provide patient-centered care and reduce social injustices by improving access to care for all.
Author Contributions
K.L. Kontaxis, contributed to conception, design, data acquisition, analysis, and interpretation, drafted the manuscript; S. Esfandiari, contributed to conception, design, and data interpretation, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Footnotes
Acknowledgements
The authors thank Héléne Labrecque for her help in coordinating this research study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was self-funded.