
Abstract
Introduction:
An established body of literature highlights a higher prevalence of oral health concerns among Indigenous Australians including untreated dental caries and periodontal disease. In South Australia, access to and provision of culturally safe oral health care for these communities remains a challenge in dental services, and less is known around what culturally safe dental care means for Indigenous communities.
Objectives:
This study explored (1) the barriers to accessing culturally safe oral health care for Indigenous Australians and (2) the enablers to promote and support culturally safe oral health care.
Methods:
This qualitative study involved semi-structured interviews with 136 Indigenous South Australian adults who participated in a dental care intervention involving oral epidemiological examinations at baseline and 12-mo follow-up (after receiving formal dental care) and health assessments. Reflexive thematic analysis was used to analyze qualitative data on participants’ oral health care experiences more broadly, the dental care received as part of the study, and their perspectives on improving dental care for Indigenous communities, including culturally safe care.
Results:
Participants reported a range of experiences in formal dental care settings including discrimination, fear, and limited access to dental care due to cost or location. Various enablers to improve culturally safe dental care were highlighted, including continuity of care, Indigenous-led dental services, mobile services and at-home care, trauma-informed clinics, early intervention, oral health promotion, and improving accessibility through free or low-cost dental care.
Conclusion:
Overall, this study emphasized the need for further action to ensure cultural safety in Australian dental services.
Knowledge Transfer Statement:
This study found that Indigenous Australians’ access to culturally safe oral health care is limited. Culturally safe care was affected by discrimination and distressing experiences in dental care settings. Dental care remains costly and regional areas remain underserviced, affecting access. Mobile services, continuity of care, early intervention, and Indigenous-led care can improve access. Findings from this study may shape health services planning regarding models of care that are family-centered, affordable, accessible, and prioritize cultural safety.
Keywords
Introduction
There are estimated to be more than 476 million Indigenous people across 90 countries (United Nations 2021). Although diverse, these groups share historical continuity and strong ties to their lands and regions, including in Western-settler colonial countries such as Australia, New Zealand, Canada, and the United States (United Nations 2021). Globally, the effects of colonization, assimilation policies, and systemic discrimination have contributed to Indigenous communities experiencing poorer well-being and greater health inequities compared with non-Indigenous groups (Satur and Carrington 2022). Among Indigenous communities worldwide, outcomes are particularly pronounced in relation to oral health status (Schuch et al 2017), with Indigenous groups experiencing a higher prevalence of tooth decay (ie, dental caries; Nath et al 2021) and periodontal (gum) disease (Nath et al 2022).
In Australia, 3.8% of the national population identify as Aboriginal and/or Torres Strait Islander (hereafter, respectfully referred to as Indigenous Australians; Australian Bureau of Statistics [ABS] 2023). Health disparities between Indigenous Australians and the non-Indigenous population are well-established and are known as the “health gap.” The incidence for various chronic noncommunicable diseases such as cancer, cardiovascular disease, and musculoskeletal conditions is reported to be higher in Indigenous Australians compared with non-Indigenous Australians (Australian Institute of Health and Welfare [AIHW] 2022). In Australia, within the overall health gap is an oral health gap, with Indigenous Australians experiencing increased incidence and severity of untreated dental caries and periodontal disease (Schuch et al 2017; AIHW 2022) and higher hospitalizations for dental problems (Australian Medical Association [AMA] 2019). This is of concern, as previous research suggests potential links between poor oral health and several chronic diseases including diabetes, cardiovascular disease, and mental health (Botelho et al 2022; Satur and Carrington 2022). Access to timely, comprehensive dental care can prevent these issues and may improve systemic health (COAG Health Council 2015). However, Indigenous Australians face several barriers in accessing oral health care.
Emerging research has identified various structural barriers for Indigenous Australians in accessing oral health care, including a lack of oral health promotion, high cost of services, and discrimination in dental services (Durey et al 2016; Butten et al 2019; Krichauff et al 2020). Mistrust and fear of dental care are major barriers, with a previous qualitative study suggesting that Indigenous Australian patients often experience painful and invasive procedures or anticipate these experiences, with little concern or empathy from dental practitioners (Krichauff et al 2020). In addition, feelings of inferiority due to interpersonal racism in clinical settings may result in increased apprehension and avoidance of services by Indigenous Australian patients (Durey et al 2016; Ali et al 2021). These issues are often associated with long-standing colonial practices by Western institutions; for example, until the 1990s, dental providers were entitled to extract remaining teeth from Indigenous Australians as a requirement to receiving heart disease surgery (AMA 2019; Jamieson et al 2023). Similarly, as described by Aboriginal Health Workers in Western Australia, Indigenous caregivers may often fear their children could be taken from them if dental practitioners perceived caregivers were inadequately caring for their child’s teeth, stemming from experiences of transgenerational forcible child removals (Durey et al 2016). These barriers highlight the need for culturally safe dental care for Indigenous Australians in closing the health gap.
Culturally Safe Care
“Cultural safety” is a concept introduced by Ma¯ori nurse and scholar Irihapeti Ramsden to address health inequity in New Zealand in relation to nursing and midwifery practice (Papps and Ramsden 1996). The term applies to health care more broadly and requires practitioners to “provide care within the framework of recognizing and respecting the difference of any individual. … It empowers users of the service to express degrees of felt risk or safety” (Papps and Ramsden 1996, p 494). A culturally safe environment is one that is emotionally and physically safe and is determined by the people receiving the care (Papps and Ramsden 1996; Satur and Carrington 2022). Culturally safe care requires accountability from practitioners in acknowledging their personal biases, attitudes, and stereotypes and requires understanding of how factors such as colonization, systemic racism, and power imbalances affect individual and community health (Satur and Carrington 2022). An aspect of cultural safety includes trauma-informed care—a strengths-based approach that ensures the physical and emotional safety of clients, considers Indigenous perspectives on health, experiences of racism, historical and cultural trauma, and stories of resilience and survival (Tujague and Ryan 2021). As aforementioned, barriers remain regarding access to culturally safe, trauma-informed dental care for Indigenous Australians, and inequities persist in terms of oral health, warranting specific exploration around Indigenous perspectives on culturally safe dental care.
Dental Care Provision in Australia
Australia’s federal government subsidizes most primary health care through Medicare, a universal public health insurance scheme providing free or low-cost services to citizens and permanent residents in Australia (Services Australia 2025). Currently, dental services are not included on Medicare and are provided via 2 pathways, including publicly and privately funded services (Schuch et al 2017). Publicly funded dental care is means tested, may have lengthy waiting times, and may require co-payment from patients. Free or subsidized treatment from public dental clinics is also available to people with Health Care cards (ie, those who receive specific payments from the government; Services Australia 2023). For privately funded services, patients pay out of pocket, with approximately half the Australian population paying for dental care using private health insurance (Schuch et al 2017).
For Indigenous Australians, health care may be provided through nationally funded Aboriginal Community Controlled Health Organisations (ACCHOs). The number of ACCHOs providing dental care is limited (approximately one-third), with some requiring a small out-of-pocket cost, making access to Indigenous-led care challenging (AMA 2019; Jamieson et al 2020). In addition, government initiatives such as Closing the Gap (CTG) aim to address health inequities between Indigenous and non-Indigenous Australians (National Indigenous Australians Agency [NIAA] 2025). Under CTG, practitioners may support Indigenous Australians in accessing lower-cost or free medications (already subsidized by the Australian government through the Pharmaceutical Benefits Scheme [PBS]; Services Australia 2024). Some services offered under the CTG initiative may provide health checks and follow-up services in which Indigenous Australian patients are not required to pay any out-of-pocket costs (NIAA 2025). However, free or low-cost dental services are not included under the CTG agreement despite the initiative’s aims to reduce disparities in Indigenous health.
Current Study
Provision of care that is free of racism, whereby clients’ identities are not denied nor challenged (ie, culturally safe care), remains limited in oral health care settings, exacerbating poor health outcomes for Indigenous groups (Satur and Carrington 2022). As such, the current study aimed to explore the experiences of Indigenous South Australians—a proud group that continues to experience marginalization and inequity regarding oral health care—and their perceptions of and experiences with dental services, as well as enablers for culturally safe dental care. The current study was guided by 2 research questions: (1) What are the barriers to accessing culturally safe oral health care for Indigenous South Australians? and (2) What are the enablers to providing culturally safe oral health care for Indigenous South Australians?
Method
Study Design
This qualitative study was part of a broader mixed-methods study involving 2 components (see Jamieson et al 2023 for the study protocol). The first component was a single-arm intervention in which 273 Indigenous South Australians (n = 187 adults, n = 86 children) participated in oral epidemiological examinations at both baseline and 12-mo follow-up (after receiving dental care). After baseline examinations and prior to the 12-mo follow-up, participants were referred for dental treatment at private or public clinics (based on health care card ownership) at no cost. In centering cultural safety, the research team supported with booking participant appointments with dental clinics, conducted baseline and follow-up examinations at a location of the participant’s choosing (eg, at home), supported with organizing transportation to and from clinics, and prioritized trust building in supporting long-term relationships with communities. The second component of the study involved qualitative, semi-structured interviews at 12-mo follow-up with consenting participants. Participants involved in the study at both baseline and 12-mo follow-up were eligible to participate in an interview. Interviews explored Indigenous South Australians’ experiences with dental care more broadly and as part of the intervention, with the findings from these interviews reported in the current study.
Participants
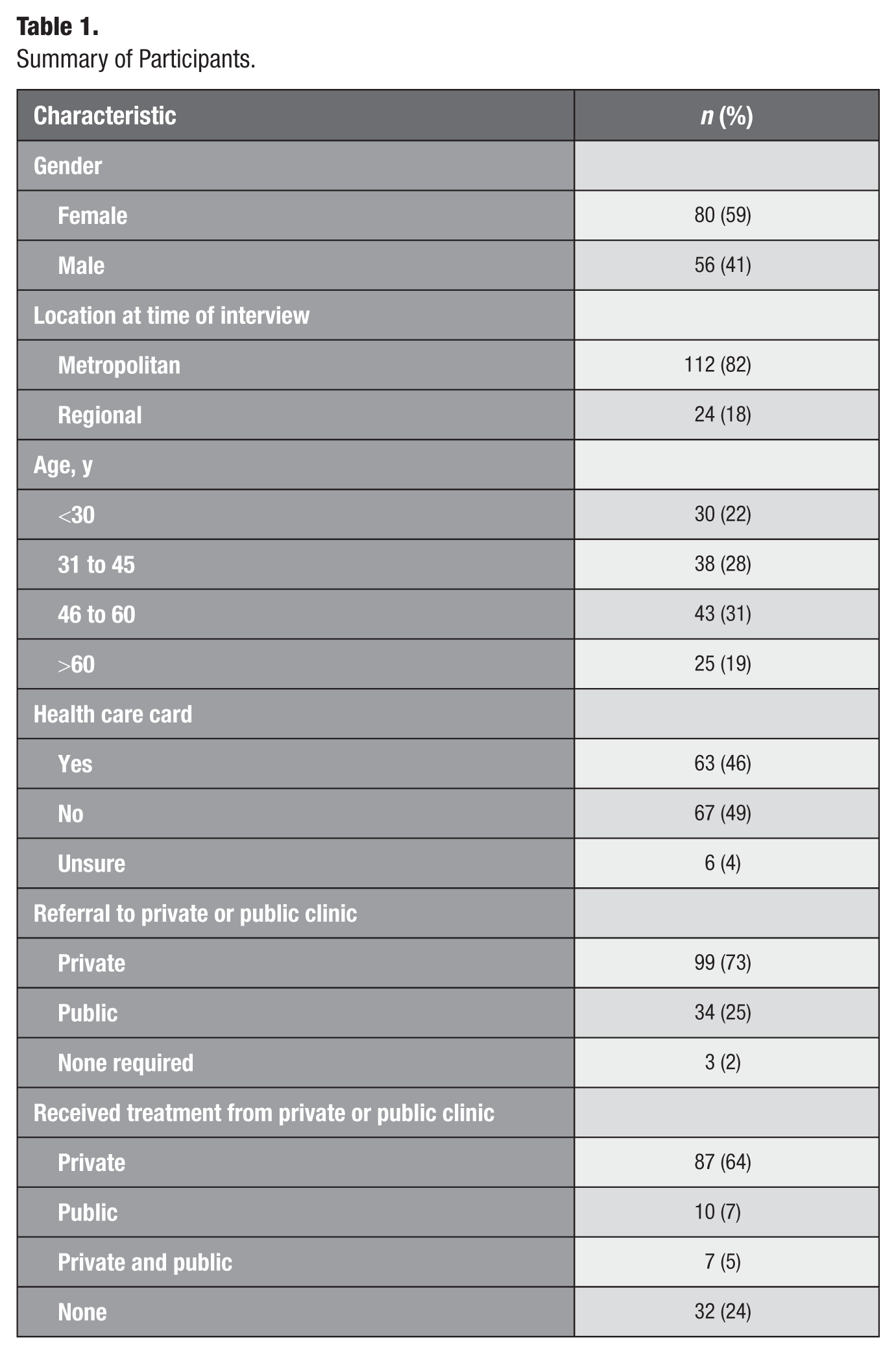
Interviews were conducted with 136 Indigenous South Australian adults (n = 80 female, n = 56 male). Participants ranged in age from 18 to 80 y (mean = 44.8 y, SD = 14.8 y). At the time of interview, 112 participants resided in metropolitan Adelaide, while 24 resided in regional South Australia (Table 1). Of the 136 participants, most were referred to private clinics as part of the intervention, with about 64% receiving their treatment from private clinics. About 2% of participants did not require treatment, and 24% of participants reported receiving no treatment at all due to various reasons (eg, illness or disability, time constraints, feeling scared or anxious, or personal and cultural commitments).
Summary of Participants.
Procedure
This study took place on the lands of the Kaurna, Adnyamathanha, Nukunu, Barngarla, and Ngarrindjeri Peoples in South Australia. Ethics approval was obtained from the Aboriginal Health Council of South Australia’s Human Research Ethics Committee (approval No. 04-22-990) and the University of Adelaide Human Research Ethics Committee. The overall study was informed by the CONSIDER statement for Indigenous health-reporting guidelines to support the research praxis and promote Indigenous health outcomes (Huria et al 2019). Inclusion criteria for adult participants were (1) aged 18 y or older, (2) identified as being Aboriginal or Torres Strait Islander, and (3) resided in South Australia. Those who were not enrolled in the original recruitment period were not eligible to participate in the 12-mo follow-up.
Study information was circulated via ACCHOs and ACCHO staff through presentations. Study flyers were circulated to communities via local community organizations and social media, and participants were also recruited via snowball sampling. Participants involved in the 12-mo follow-up were offered an opportunity to provide further feedback through an interview. The 12-mo follow-up and interview were conducted in a location of the participant’s choosing (eg, their home, community center, a research facility at the university). Interview questions related to participants’ experiences with the dental care intervention, experiences with private and public dental services more broadly, and thoughts regarding provision of culturally safe dental care for Indigenous communities. Examples of questions included: “Can you tell us about your experiences with the dental care system?” with prompts for positive or negative experiences and, “What changes/improvements would you like to see in the way that dental care is provided for communities to ensure cultural safety?” All participants received a $20 AUD shopping voucher and an oral health pack (toothbrush, toothpaste, dental floss) as recognition of their time. Interviews were audio-recorded and manually transcribed by the first author, and any personally identifying information was removed.
Analysis
Data were analyzed using reflexive thematic analysis as per Braun and Clarke’s (2021) 6 phases. Reflexive thematic analysis involves the development, analysis, and interpretation of patterns across a dataset and recognizes researcher subjectivity as a resource and strength (Braun and Clarke 2021, 2022). This approach was suitable for a large data corpus of qualitative interviews, offering the flexibility for an inductively driven analysis in capturing contextually rich experiences (Braun and Clarke 2021). Reflexive thematic analysis is also compatible with the critical realist ontology and contextualist epistemology underpinning this study, whereby meaning and knowledge were co-produced (by the researchers and participants) during the research process and shaped by context. Therefore, in line with the philosophical underpinnings of this research, findings reflected participants’ perceptions of their reality as influenced by and grounded within their cultural context (Braun and Clarke 2021). Analysis began through data familiarization, whereby the first author transcribed and repeatedly read all interviews. Codes were generated at the semantic level and related to participant experiences with dental care broadly, discrimination, fear in clinical settings, access to dental care, affordability, experiences with the intervention, and enablers for improving access to culturally safe care. The research team subsequently developed and defined themes, with extracts for each theme reviewed by all authors.
The research was guided by Tracy’s (2010) criteria for methodological rigor in qualitative research. In ensuring the overall trustworthiness of the findings, this research considered data generation and analytic approaches that cohere meaningfully with the aims, the study’s qualitative paradigm, and theoretical underpinnings. In addition, positionality was considered in acknowledging researcher influence and assumptions as well as transparency in terms of disclosing these aspects and the limitations of the research.
Reflexivity
Reflexivity is an important aspect of research, encouraging researchers to reflect on the assumptions they bring to their work and the impact these assumptions have on analysis and interpretation (Braun and Clarke 2021). In terms of the present study, the research team have more than 20 y combined experience working with Indigenous communities in the oral health field. As a team of Indigenous and non-Indigenous researchers, academics, and clinicians—both with and without the lived experiences that guided the aims of this study—we engaged in critical reflection of the assumptions we brought to the research. This included reflection on the rights afforded to some of us in accessing dental and health care (eg, in terms of class, citizenship, race) and our privilege in being able to access this health care in the Australian context. The non-Indigenous authors were guided by a senior Indigenous researcher (J.H.) and Indigenous research officers (E.F., T.-M.M., E.W.) in ensuring project implementation was culturally appropriate. Throughout the study, the team were involved in discussions with the senior Indigenous researcher, Indigenous research officers, and Indigenous health care workers, providing opportunities for consideration of positionality and ensuring the research prioritized cultural safety.
Results
Six themes were developed from the interview data (Fig 1). The first 2 themes highlight barriers experienced by Indigenous communities in accessing dental care, including discrimination (anticipated and actual) and lack of access to care due to rurality and/or unaffordability. The final 4 themes describe enablers for culturally safe dental care, including mobile dental care, collaboration and continuity of care, culturally safe clinical spaces, early intervention, and free or low-cost dental services.
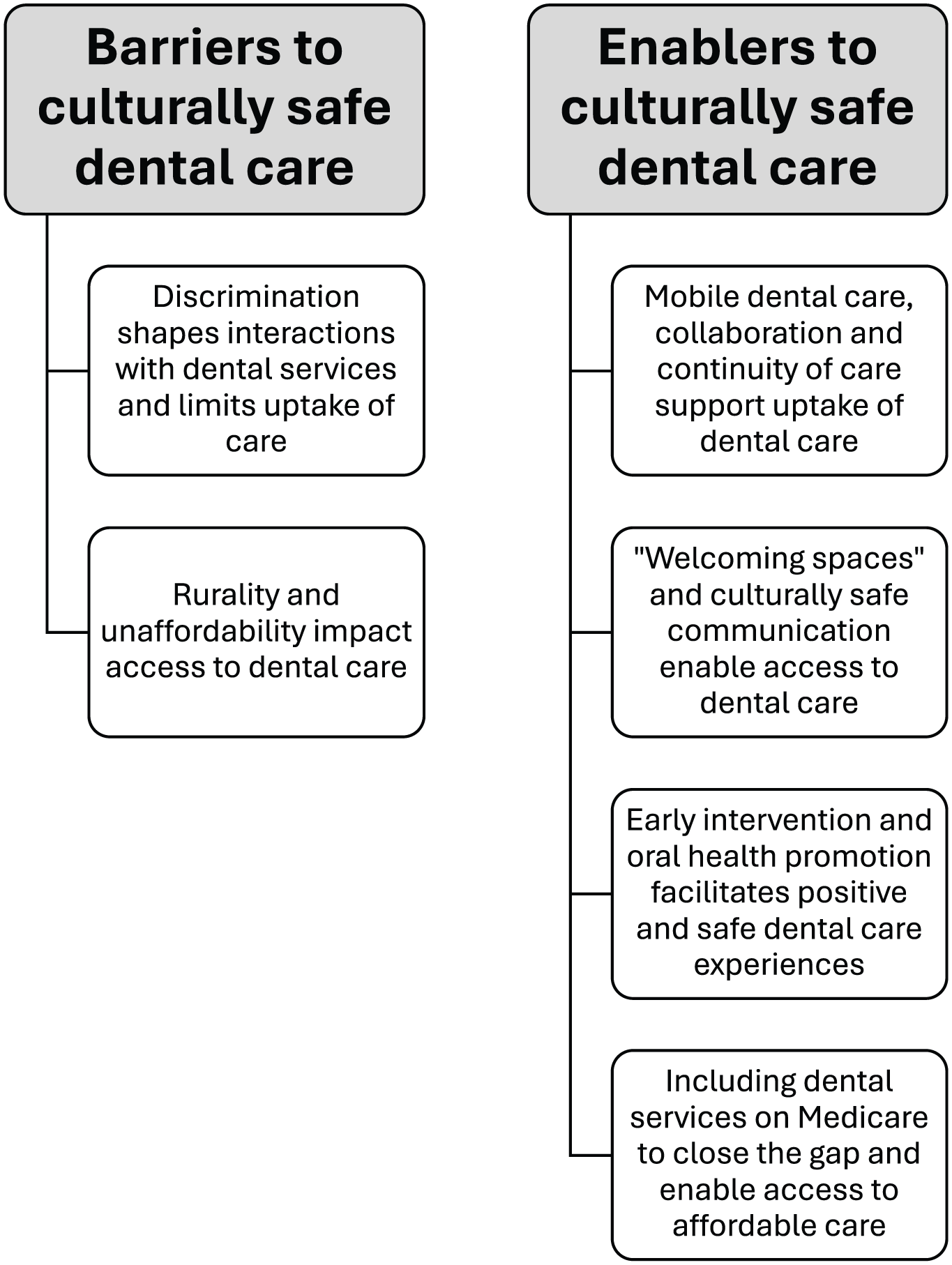
Thematic map.
Theme 1: Discrimination shapes interactions with dental services and limits uptake of care
Some participants anticipated discrimination within dental services due to ongoing discrimination they experienced as a result of racial or cultural differences, speaking of fear in interacting with services. One participant linked these experiences to colonial practices, including control and authority over Indigenous people, as well as the Stolen Generations, which involved the forcible removal of children from their families by Australian authorities spanning the 1890s to 1970s. These events continue to have deep implications for the well-being of Indigenous communities in Australia today: “It’s mainly fearful, people are fearful of doctors, nurses, of authority of any kind. It’s just past hanging on. And the Stolen Generation still lives” (P183). This is further highlighted by one mother, who noted: . . . because my kids are darker than me and look more Aboriginal than me sometimes I can feel [discrimination] more through my kids than myself. And sometimes it’s just a feeling that you get . . . you’re automatically assuming it’s going to happen somewhere because it’s happened all the time. So even if it’s not happening you’re anxious because you think it’s going to happen. (P157)
Similarly, another participant described how prejudicial attitudes may exist within dental services, a key barrier for Indigenous Australians in accessing care: I think, obviously we’re not gonna go [to the dentist] because of that divide. Like there’s still that prejudice against us Aboriginals, and that sucks. So if we can get rid of that stigma, then I think that would be great, you know what I mean? (P370)
While participants anticipated discrimination within dental services, many also experienced it. Distressing experiences often left some fearful and anxious of dentists and dental treatment. Participants spoke about feeling, “treated like a number” (P211), where practitioners were primarily concerned about monetary outcomes and seeing a high volume of patients: “I wasn’t respected at all . . . just taking money, didn’t care about you emotionally, your well-being at all . . . get you out the door as fast as they can, next person in-line” (P49). A power imbalance also underlined interactions between Indigenous Australian patients and practitioners, where patients felt they were not seen or heard: Very negative. I went to the dental clinic and a guy stood over me in a chair, ripped my tooth out, ripped all my gum and exposed the bone and another tooth fell out, and that was very traumatic for me. I ended up with infection and in hospital. They wouldn’t have treated me like that if I was non-Indigenous. (P375)
Another participant described a similar negative experience, linking this to a lack of trauma-informed practice on the part of dental practitioners: I’m a social worker, so this whole idea of trauma-informed practice is very big in my field but it may not be in other people’s fields, and [dentist] put like a rubber shield over my mouth so that I felt like I couldn’t breathe and like it was blocking my nose, my nostrils, it was blocking my entire mouth, and I had no idea that he was even going to do it, I didn’t know what it was. (P435)
Overall, this theme highlights that some participants were fearful around how they would be treated when accessing dental services and that this treatment may be negative due to past experiences and ongoing stigma toward Indigenous people. Due to discrimination experienced across day-to-day interactions and within health care more broadly, some participants deemed dental services potentially culturally unsafe, especially in returning to clinics for ongoing care.
Theme 2: Rurality and unaffordability affect access to dental care
A key barrier discussed by participants in both regional and metropolitan locations were the lack of dental services in regional and remote areas for Indigenous communities. Some participants highlighted the health effects of limited or no access to oral health care based on where people lived: . . . the absence of people on the ground to deliver dental services . . . people there would have horrible abscesses and some of the abscesses are due to a contributing factor of poor nutrition. . . . It’s around quality food, accessibility that then determines health determinants . . . getting services into the rural and remote is very, very difficult. (P390)
One participant noted that if communities in regional areas did have access to a dentist, communities did not receive comprehensive care as a result of dentists’ large workloads. For those experiencing pain, some were said to remove their own teeth due to wait times, fear, and cost: . . . everyone has to travel for [dental care] . . . they’re [regional dentists] flat out busy and you’ll just get it’s mainly a hygienist . . . I’ve seen [community members] sit there and pull their own teeth out. . . . If they’re rotten and stuff, people are spitting teeth out. (P183)
In addition to rurality as a factor affecting access, cost was described as a significant barrier. Given that dental care is not subsidized by Medicare or CTG, one participant shared how this further limited people’s access: I think because the cost is not covered under CTG or anything, so people go, “Oh bugger it, I’m not going,” and let’s face it going to the dentist is quite expensive, and you haven’t got the money, there’s a lot of things you’d rather spend the money on. (P400)
While some Indigenous health care services may offer free dental care to communities in metropolitan areas, getting an appointment proved difficult due to wait times: . . . it would’ve been [Aboriginal health organization] and I had a broken tooth, and even that is not accessible like as an Aboriginal person, actually my understanding is it’s free dental but you can’t get in and that’s really disappointing so that puts you off knowing that your own Aboriginal health organization doesn’t allow you to use their services, or there’s a massive waiting list. (P245)
This theme emphasizes that dental care remains inaccessible for Indigenous communities, especially for those living in regional or remote areas where receiving oral health-related support is a known challenge due to location and underservicing. These barriers have implications for the health and well-being of communities in regional and remote areas. The following themes describe enablers for improving access to dental care and promoting culturally safe care.
Theme 3: Mobile dental care, collaboration, and continuity of care support uptake of dental care
Various factors were shown to affect access to culturally safe dental care for Indigenous communities. This included discrimination, fear, high cost of services, and location of services. In addressing these concerns, participants expressed the need for dental services to show flexibility, much like the intervention this study provided, where dental checkups were completed in a space they were comfortable in—their homes: I mean like this kind of a setting I think is really congenial to Indigenous families and Indigenous culture right? Like it kind of seems a bit personal, and in that sense kind of breaks down a lot of barriers that might be there and prevent people from being forthcoming with important medical information. (P476)
Mobile dental clinics were also described as a culturally safe way to promote dental care in communities, especially for those in regional or remote areas. For example, one participant described the apprehension experienced by people in regional areas who may be required to travel long distances to unfamiliar metropolitan cities for treatment: Boots on the ground out there, talk to people out on their own ground. You’ve lost something straight away as soon as you come here [to metropolitan Adelaide] . . . the apprehension, anxiety straight away, they’re off their ground so their confidence level has gone down to 40%. . . . Lot of the [regional and remote] communities are very welcoming, very welcoming. (P183)
In addition to offering oral epidemiological examinations and health assessments at a location of participants’ choosing, researchers collaborated with dental clinics to provide free treatment to participants. Where possible, participants were referred to a clinic with an Indigenous dentist with whom some community members were familiar and most had positive experiences: So I went to a dental clinic that had an Aboriginal dentist which again felt very culturally safe. I actually found out that we lived in the same area like at separate times but had that in common which was awesome . . . it was really good having someone that it felt like just hanging out with mob. (P4)
Continuity of care and regular engagement with communities outside of clinical environments was also described as important in improving access: Someone that goes out into communities is also really good. Like not as in you know they only go out to do the dental checks but also a person that’s just involved and sort of understands the community in a way I’m thinking of like [Aboriginal health clinic] in South Australia, like I know the people that are in that building because they’re at every event, they’re at every sort of gathering, every NAIDOC week, Reconciliation week, Mabo Day, whatever it may be, they’re there. And I think that that creates more trust in that service because you see them all the time. (P4)
This theme highlights the importance of “being where the people are” in providing culturally safe care in safe spaces. This includes within the home and via mobile units to regional and remote communities, with continuity of care and community engagement a priority in addressing barriers to access.
Theme 4: “Welcoming spaces” and culturally safe communication enable access to dental care
In ensuring oral health care is culturally safe, enablers highlighted by participants included culturally safe communication, with consideration of how trauma may shape experiences with health care. Enablers included ensuring proper consent is obtained from patients, explaining any medical terms used, hearing and understanding patients when they have questions or concerns, and practitioners clearly explaining processes involved: The idea that people will come to you who have, particularly in Aboriginal communities . . . regional or remote communities, will have trauma at some point in their life, and if you are going to their face, and their face is somewhere that’s a really intimate area to be touched, then being informed about every step of what’s happening and why. . . . So a trauma-informed lens would be so beneficial in this. (P435)
Representation in physical environments and clinical spaces was also important to participants: . . . welcoming spaces . . . references to Custodians of the Country, an environment that at least shows some sort of embracement of our Aboriginal culture, its local Aboriginal culture. The more place-based some of that stuff and resources in that environment, the better . . . also, when there’s significant periods to Aboriginal people, be it kind of culturally focused either NAIDOC Week or Reconciliation Week . . . you’d like to think you go into that environment and you see support around that in those environments. (P292)
One participant spoke of the possibility of services incorporating Aboriginal perspectives. This could be achieved through collaborating with people who have cultural authority and specific knowledge related to traditional healing practices—known by many Indigenous communities as “Ngangkari” in Pitjantjatjara language: “. . . if there is potentially a space for that decolonization to kind of happen in collaboration . . . get the perspective of potentially those Ngangkaris [Traditional Healers] . . . they can be involved some way, or their perspective could be involved with this” (P292).
“Welcoming spaces” and culturally safe ways to promote dental care may also be achieved through co-location of dental services (eg, within ACCHOs run by and for Indigenous communities) and with broader community-based health care services specifically for Indigenous families: So when you can sort of bunch things together so a medical service that does a health check and in the same place maybe then they can get a dental check and things like that, I feel are very successful. [Hospital] when they run their Nunga clinic once a week they also have like a little playroom for the kids, they’ve also got a space where people in the community can come and catch up with each other as well. (P349)
Overall, practitioner education and promotion of culturally safe communication underpinned by trauma-informed care may address some of the challenges associated with access to oral health care for Indigenous communities. Participants shared the importance of Indigenous practitioners and Aboriginal perspectives within dental services and co-locating dental services alongside other health care services (that are Indigenous-led) to further address the barriers around accessibility and cultural safety.
Theme 5: Early intervention and oral health promotion facilitates positive and safe dental care experiences
Early intervention was a key facilitator noted by participants in promoting lifelong health for Indigenous communities regarding oral health. This may be important for adults who had negative experiences with dental services and were concerned their children may have similar experiences: Because there are a lot of Aboriginal people that are adults that have been traumatized by the system in dental and things like that, where then they’re hesitant to bring their own children and then it becomes a generational cycle. So knowing where they can go that’s safe and connected, partnering up I guess with other Aboriginal First Nations medical programs as well. . . I find that can be very helpful as well in terms of being inviting. (P349)
This extract further highlights the need for welcoming spaces, collaboration, and co-location in promoting oral health outcomes for Indigenous communities across the lifespan. Participants were also in favor of free dental checkups and preventative care within schools—a government initiative that previously saw 2 to 3 dental chair clinics based on school grounds, which have since been amalgamated into larger community clinics: . . . we used to have the South Australian Dental in schools. It’s a terrible shame they’re not there, because that was probably a really big and very good thing. In hindsight, they should have stayed having dental clinics at the schools, giving the kids a check-up and taking away that childhood fear. (P390)
One participant also noted how children seeing adult family members receive a dental checkup in safe spaces (ie, the home) as per the intervention, as well as practitioners including an educative component on the importance of looking after oral health, can promote positive outcomes: . . .it exposes it to the young people so that they can see their aunties, nannas, uncles, dads, having their treatment done and the importance, so that the fear is removed a little bit, it’s normal to go [to the dentist] . . . everyone was there trying to get into [child’s] mouth and watch as well, it’s that breaking down of fears. Really when you think about it, a dentist appointment is only once or twice a year if you keep on track. So then that’s where the anxiety and that build up because it’s few and far between. (P9)
The importance of culturally safe and accessible care and early intervention in supporting oral health and therefore long-term health was highlighted by participants, with implications for Indigenous children and families.
Theme 6: Including dental services on Medicare to close the gap and enable access to affordable care
In promoting accessible, affordable, and culturally safe oral health care, participants strongly recommended dental care be part of Medicare: “. . . kind of like in the public system like Medicare type of thing would benefit a lot, yeah for sure, and I don’t see why not because it is very important, so that’s the question, ‘Why not?’” (P41). This would ensure most Australians could access low-cost or free dental care and may support closing the gap in terms of existing health inequities: . . . closing the gap, wouldn’t that be the whole point of dental as well? Because obviously as we know, Closing the Gap you can get under Medicare or whatever it is they do . . . even you don’t pay a gap when you go the GP at an Aboriginal Clinic, because of Closing the Gap. Well, wouldn’t that be similar for dental? (P408)
This experience was shared by another participant who similarly noted that CTG could be an avenue for expanding free or low-cost dental care to Indigenous people: Well, it would be amazing if dental care could be included in the close the gap care because we get the PBS medications and stuff and that’s been super helpful. And when you sit with your doctor and go through everything they do ask about your teeth, but there’s nothing they can do about it, so yeah it’d be good if it was included on [CTG] like that. (P459)
As there is clear separation between dental services and the general health care services that are covered under Medicare, some participants suggested that dental care should “be incorporated as part of overall primary health care” (P423) to improve affordability and access, as well as to support well-being. In this final theme, free or low-cost dental care was seen as a key step in committing to providing culturally safe dental care. This is especially important in improving oral and overall health outcomes for Indigenous communities.
Discussion
This study explored the views of Indigenous South Australians involved in a culturally safe dental care intervention with qualitative findings reporting participants’ experiences of dental care and their perspectives of what comprises culturally safe dental care. Key findings suggested participants often anticipated and/or experienced discrimination with dental services, which shaped interactions with services, such that their likelihood to accessing dental care was low. These findings mirror previous research with Indigenous Australians in metropolitan and remote communities, in which participants reported apprehension in accessing health care services generally (Durey et al 2016), with dental fear highlighted as a significant barrier to attending an already inaccessible health care service due to high costs and location (Kong et al 2020; Patel et al 2021).
Prior negative experiences with health care or government services more broadly (eg, assimilation, child removal, land and custom theft, restrictions on Indigenous civil rights, mobility, employment; Hedges et al 2021) may often leave Indigenous clients fearful and result in a “spill-over effect” with other institutions including dental services (Kong et al 2020, p 7). As a result, clients continue to fear contact with institutions and therefore avoid or disengage with services. Minimal cultural safety in these settings strongly affects the decisions of Indigenous clients to access services for fears they may reexperience racial trauma during their interactions with practitioners (Gatwiri et al 2021). Cultural safety must be prioritized in oral health care settings, as regular dental care, including early detection of oral diseases and preventative services, plays a key role in supporting systemic health and improving quality of life (Lee and Somerman 2018). However, closing the gap in Indigenous health outcomes will not progress if such services remain culturally unsafe.
Importantly, the current study found that most participants described clinical spaces as unwelcoming or unsafe, felt they were not seen or heard by practitioners, and some interactions with dental services were described as traumatic. One participant in the current study shared an instance in which she could not breathe due to a shield (dental dam) covering her mouth, a process that was not explained by the dentist prior. These findings reinforce barriers in health care more broadly regarding poor treatment, communication, and failing to ensure informed consent on the part of practitioners, which may exacerbate feelings of fear or trauma as identified in prior work with First Nations and Indigenous communities in Canada (Pilarinos et al 2023) and Ma¯ori peoples in New Zealand (Espiner et al 2021). In addition, some participants felt that practitioners were only concerned about getting Indigenous Australian patients “out the door as fast as they can”, emphasizing that the Western model of care tends to be highly profit driven and lacks cultural safety (Jamieson et al 2023).
These experiences suggest that the social, cultural, and historic context of participants’ lives are not well understood by some dental practitioners and that the care received by Indigenous participants from dental services was not respectful or sensitive to patient needs (Durey et al 2016). Findings from the current study also highlight issues previously identified in the literature regarding dental care as not patient centered and, instead, disease oriented, with clinics using high-technology facilities or equipment while lacking actions such as Indigenous acknowledgement and representation (eg, through Reconciliation Action Plans, statements, or artwork in clinics; Krichauff et al 2020; Jamieson et al 2023).
In addition to experiences of discrimination or lack of trauma-informed care, participants described challenges in accessing culturally safe dental care for families living in regional and remote locations and the effect this lack of access had on oral and overall health. In particular, lower service provision in regional and remote areas, long waiting lists (Dudko et al 2018), lack of access to affordable and nutritious foods, lack of fluoridated water (COAG 2015), and no access to dental care within an hour of travel (Gardiner et al 2020) are all barriers to care identified in the broader literature and reflected by the findings of this study. These barriers may explain the higher rates of potentially preventable hospitalizations and acute disease in regional and remote communities more generally (Gardiner et al 2020).
Affordability was also a major barrier to access, with many participants noting other immediate priorities such as living expenses, which meant that dental care was put on hold. The high cost of dental care is a very common barrier to access identified in previous research among both non-Indigenous and Indigenous groups (Kong et al 2020; Patel et al 2021; Hopcraft and Holden 2025). Some practitioners in Australia blame the lack of universal coverage for widespread disparities in access to care, poor oral health outcomes, and chronic disease burden (Hopcraft and Holden 2025). It is evident that oral health care remains inaccessible and culturally unsafe due to the lack of attention to servicing regional areas and the high cost of receiving care.
Clinical Implications
Participants in the current study suggested various recommendations to facilitate culturally safe dental care and address the barriers they experienced in accessing this care. First, continuity of care with the same dentist (preferably Indigenous dentists and staff) was noted as key in supporting access to care. In previous research with Indigenous communities, continuity of care was described to improve communication, trust, and confidence toward oral health practitioners and reduce the fear in accessing services (Shrivastava et al 2019; Kong et al 2020). Second, integrating dental care into existing Indigenous-led services and collaborating with people who have cultural authority or local input were recommendations in facilitating culturally safe care, reflecting previous evidence (Kong et al 2020; Walker et al 2023).
Third, community-based, family-oriented, and at-home care, much like the care delivered through our intervention, was valued by participants in the current study. Care delivered in this way helped to bridge the gap between communities and formal services, such that fear in accessing dental care was reduced as a result of relationships that were established between the research team and participants. This model allowed time for oral health promotion, which supported awareness within the community around the importance of dental and health care. Models of care that center outreach such as mobile or at-home dental services may be favored by people who have had negative experiences with dental care while supporting trusting relationships between services and communities (Kong et al 2020; Patel et al 2021).
Fourth, participants emphasized the need for early intervention for Indigenous children and communities. This is of importance, as dental disease in childhood can have long-term effects and persist into adulthood, with caregivers having a significant influence on child oral hygiene practices (Ha et al 2019), suggesting that health promotion could be targeted toward children and in family settings. Fifth, the provision of free or heavily subsidized dental care within schools for children was described as an important enabler to access for Indigenous families. Previous research suggests schools may also be a hub to support broader community and family health (Patel et al 2021; Walker et al 2023). Bringing dental care to settings such as the home or school may provide additional holistic options for access in cases in which ACCHOs or public dental services have long wait times or limited staffing. The current study also highlighted intergenerational aspects of health care, for example, ideas around what good or bad health care constitutes and the level of trust that families may place in dental practitioners. Early intervention with families in ways that foster trust (eg, community engagement, outreach) is therefore important. In terms of those living in regional areas, mobile clinics that offer flexibility including walk-in appointments can address structural barriers in access to dental care and support those in underserviced locations (Patel et al 2021).
Sixth, those who attended formal dental clinics in the current study noted the need for improvements in representation and the physical environment of these spaces. “Welcoming spaces” and “an environment that at least shows some sort of embracement of our Aboriginal culture” were described as important in promoting culturally safe care. The idea of “welcoming spaces” is reinforced in previous research with Canadian Indigenous patients in health care settings (Pilarinos et al 2023, p 409), reflecting the need to consider ways in which clinics may support clients’ well-being and in becoming representative and inclusive for Indigenous families.
To participants, cultural safety included culturally safe communication (eg, processes explained clearly by practitioners, all questions answered, consent obtained) and practitioner awareness around important aspects of Indigenous culture and community, with a trauma-informed lens noted as important. Tujague and Ryan (2021) note that while important, cultural safety training may not be sufficient alone in considering the effects of intergenerational or other traumas on clients. As such, a trauma-informed approach that centers the effects trauma may have on clients can prevent the reexperience of racial trauma in clinical settings (Tujague and Ryan 2021). In addition, dental practitioners’ interactions with their clients may be influenced by their personal value systems, the systems in which they work, and the education or training they received. Any training or education within services should therefore require practitioners to critically reflect on their personal, professional, or cultural assumptions in recognizing how their views and any implicit biases may influence their practice. In addition to this critical inward focus among individual providers, a focus on health care systems as a whole is required (eg, through evaluating organizational policies around provision of culturally safe care) to address cultural safety at the institutional level.
Lastly, in alleviating the financial burden of dental care, participants described the importance of providing free or low-cost dental care under Medicare. A recent study with dental practitioners in Australia found that many supported subsidized diagnostic and preventative care, with means-tested and capped schemes for periodontal and restorative treatments as possible options to explore in improving access (Hopcraft and Holden 2025). Participants in the current study also recommended that subsidized dental care become part of CTG policy in ensuring Indigenous families across Australia can access dental care, therefore improving health outcomes and addressing the health gap.
Limitations and Future Research
While the current study included perspectives from those living in regional areas, this was less than one-fifth of our sample. Maldistribution of dental services in regional and remote areas, where major cities have approximately 65.1 dentists per 100,000 people, reducing to 27.7 in remote and very remote areas, may contribute to poorer oral health in these communities (KBC Australia 2022). Future research should explore the experiences of Indigenous communities in regional and remote areas and their perspectives regarding culturally safe dental care. This would expand understandings around their needs and concerns in relation to mobile dental care, specifically in the South Australian context, for which very little research exists. In addition, the current study did not explore the views of service providers (eg, dentists, oral health practitioners, Aboriginal health workers) who could provide perspectives into system- and institutional-level factors that may affect oral health care experiences for Indigenous South Australians. Additional research could target service provider perspectives in further understanding levels of support or training that providers receive and their knowledge and experience of providing culturally safe care to Indigenous communities.
Conclusion
This study explored the experiences of Indigenous South Australians and their perspectives of and experiences with oral health care and promoting culturally safe care. Findings from this study may shape health services planning regarding models of care that are family-centered, affordable, accessible, and prioritize continuity of care and outreach. Indigenous South Australians favored and highlighted the importance of early intervention in promoting lifelong health and well-being as well as focusing oral health promotion efforts in underserviced, nonmetropolitan areas in reducing rates of avoidable and preventable oral health problems. The experiences shared by Indigenous South Australians are a call to action to reevaluate the way dental care is currently delivered and to promote oral health care that is culturally safe, trauma informed, and equitable.
Author Contributions
R. Aiyar, contributed to design, data acquisition, analysis and interpretation, drafted and critically revised the manuscript; S. Nath, J. Hedges, G.L. Guzzo, K. Kapellas, contributed to conception and design, data acquisition, analysis and interpretation, critically revised the manuscript; E. Flanagan, T.-M. Mastrosavas, E. Wallace, contributed to data acquisition, analysis and interpretation, critically revised the manuscript; L. Jamieson, contributed to conception and design, data analysis and interpretation, critically revised the manuscript. All authors gave their final approval and agree to be accountable for all aspects of work.
Footnotes
Acknowledgements
The authors acknowledge the Kaurna, Adnyamathanha, Nukunu, Barngarla, and Ngarrindjeri Peoples of South Australia, Traditional Custodians of the land on which this research was undertaken. We pay our respects to Elders past, present, and emerging. We would like to thank Madison Cachagee and Alexander Pham for their ongoing support with this project. We are sincerely thankful to the ACCHOs and service providers that supported this work. Importantly, we are extremely grateful to the participants for sharing their stories and for their time and contributions to research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this research was funded by a National Health and Medical Research Council project grant (APP1120215). L.J. is supported by an NHMRC Research Fellowship (APP1102587).