
Abstract
Introduction:
Despite being acknowledged as the second global burden of oral disease, periodontal disease has few epidemiologic studies in the literature, particularly for developing countries. Many previous studies have assessed the relationship between periodontal disease and oral health–related quality of life (OHRQoL), with patients attending dental clinic or hospitals rather than a general population. This study attempted to fill the knowledge gap in limited information about periodontal disease and OHRQoL, with reference to a general population in a developing country.
Objectives:
To investigate the relationship between OHRQoL and periodontal diseases in an older population in Indonesia.
Methods:
We invited 582 older people from community health centers. The 369 (63.4%) older people who agreed to participate consented to an oral health examination and a questionnaire capturing demographic, socioeconomic, behavioral, and Oral Health Impact Profile–14 (OHIP-14) data.
Results:
Almost 75% of the older people had generalized periodontitis; 3% had healthy periodontal status; and around 22% had localized periodontitis. There was a lack of statistical evidence for an association between periodontal disease status and OHRQoL. This result was based on the appraisal of the prevalence of the impact (Odds ratio [OR], 0.95 [95% CI, 0.54 to 1.59]; P = 0.77), difference in mean severities (0.07 [95% CI, –1.66 to 1.80]; P = 0.94), and extent of the impact (P = 0.996). However, we found evidence for a relationship between tooth mobility and OHRQoL for all of the OHIP assessments, including prevalence of the impact (OR, 1.87 [95% CI, 1.16 to 3.01]; P = 0.009), difference in mean severities (–2.98 [95% CI, –4.50 to –1.45]; P < 0.001), and extent of the impact (P = 0.001).
Conclusion:
There was a lack of statistical evidence for a relationship between periodontal disease status and OHRQoL in this society. However, we found evidence that tooth mobility, as a sign of periodontal disease progression, is related to OHRQoL.
Knowledge Transfer Statement:
The present study can be used by dentists, community health workers, and policy makers in Indonesia to understand the prevalence, severity, and extent of the negative impacts of periodontal disease on older people’s quality of life. In addition, this study provides information about factors that might considerably affect the oral health–related quality of life in this society, such as brushing habits, dental visit, family income, DMF-T status, and subjective appraisal toward dental health.
Keywords
Introduction
Improvements in health prevention and treatment of diseases have contributed to a steadily increasing life expectancy. Correspondingly, the proportion of older people has been rising around the world (United Nations 2017). This longer life expectancy is associated with challenges for global public health in relation to the burden of chronic noncommunicable diseases, which often reduce older people’s oral health–related quality of life (OHRQoL; Newman et al. 2019).
Periodontal disease has been acknowledged as the second-most important global oral disease burden after dental caries (Petersen and Ogawa 2012). Moreover, periodontal disease was the seventh-most prevalent noncommunicable disease worldwide (Vos et al. 2017).
Alongside dental caries, chronic periodontitis is the leading cause of tooth loss for adults globally (Pihlstrom et al. 2005; Jin et al. 2011; Jin et al. 2016). Individuals with advanced progression of periodontal disease are estimated to have a higher risk of losing multiple teeth, which may lead to problems with masticatory function, social interactions, and self-esteem. This disease may also introduce burdens in socioeconomic impacts and oral health care costs (Petersen and Ogawa 2012; Chapple 2014; Jin et al. 2016; Tonetti et al. 2017).
Previous periodontal disease studies have mainly focused on objective evaluations based on clinical and radiographic examinations. There has been limited exploration regarding subjective evaluations of the impact of periodontal disease on OHRQoL (Ferreira et al. 2017). Few previous studies have assessed the relationship between periodontal disease and OHRQoL in a population setting, as many of these studies performed data collection with patients attending dental clinic or hospitals. Also, these studies were mainly conducted in high- and upper-middle–income countries. Thus, there is a need to investigate the relationship between periodontal disease and OHRQoL with lower-middle– and low-income countries as research backgrounds (Masood et al. 2019). Another important gap is that the evaluation of the relationship between periodontal disease and OHRQoL did not often take into account other oral health diseases and systemic diseases that might affect this relationship (Haag et al. 2017). Finally, the FDI World Dental Federation emphasizes the importance of socioeconomic aspects and demographic factors in OHRQoL assessment (Hescot 2017).
Indonesia has a developing economy and is the fourth-most populous country in the world. As with many other developing countries in Asia, Indonesia has witnessed an aging population and a growing number of older people. Up to the present time, there is limited information regarding periodontal disease in Indonesia (Badan Penelitian dan Pengembangan Kesehatan 2019).
This study attempted to fill the gap of knowledge about the relationship between OHRQoL and periodontal disease with Indonesia as a research background.
Methods
Approval for this study was obtained from the Ethics Committee of Faculty Dentistry, Universitas Indonesia (138/Ethical Approval/FKGUI/XI/2017). All participants provided written informed consent.
This study followed the STROBE guidelines (Strengthening the Reporting of Observational Studies in Epidemiology) for a cross-sectional study. This research focuses on an urban older population in 3 districts of Depok, Indonesia (Beji, Pancoran Mas, and Sukmajaya). Prior to the data collection of this study (February to May 2018), there was no published prevalence of periodontal disease in Indonesia (Badan Penelitian dan Pengembangan Kesehatan 2019). Thus, this study used the probability of periodontitis in the age group ≥65 y in Malaysia as an estimation for sample size calculation, which was 63% (probing depth ≥4 mm; World Health Organization 2010). Based on the simplified sample size calculation for a sample survey, this study needed to obtained data from at least 359 participants (if P = 0.63, confidence level = 95%, and relative precision = 5%).
The community health workers invited 582 older people (63.2% women, 36.8% men) registered with 12 elderly community health centers (posbindu). The participation response rate of this study was 63.4%, which means that 369 people (68.6% women, 31.4% men) agreed to participate. There was a smaller proportion of men in the study than in the reference population, possibly because some of them were still working and did not have time to participate.
From the 369 participants, 6 were excluded from the analysis because of edentulism. Participants were accepted if they met the following inclusion criteria: native Indonesian of age ≥51 y, able to provide consent, and had at least 1 natural tooth in mouth.
A questionnaire and oral health examination were used as the data collection instruments. The questionnaire asked about participants’ background, smoking and tobacco use status, diabetes status, oral health behavior, pattern of dental attendance, and perception regarding their oral health. In addition, the Oral Health Impact Profile–14 (OHIP-14) was included to assess OHRQoL.
Participants were asked how frequently they had experienced a negative impact of their oral health problems on their well-being within a period of 12 months. Participants were required to give an answer for each impact in 7 OHIP dimensions—functional limitation, physical pain, psychological discomfort, physical disability, psychological disability, social disability, and handicap—based on a 5-point Likert scale: never = 0, hardly ever = 1, occasionally = 2, fairly often = 3, very often = 4 (Slade 1997).
In calculating the scoring formats of the OHIP as the primary outcomes, 3 estimations were calculated: prevalence, extent, and severity of the impact (Tsakos et al. 2012). The details of the primary outcomes are presented in the Appendix. The minimal important difference (MID) for the OHIP-14 severity scores assessment is described as 5 scale points (Locker et al. 2004).
The Basic Periodontal Examination (BPE) to signify participants’ periodontal disease was divided into 2 groups: participants who did and did not have generalized periodontitis. The threshold for generalized periodontitis was defined as participants who had ≥30% of their remaining teeth affected by periodontitis (probing depth ≥3.5 mm; British Society of Periodontology and Implant Dentistry 2018).
Other intraoral health examination scales included the DMF-T index (decayed, missing, and filled teeth; World Health Organization 2013), Simplified Oral Hygiene Index (OHI-S; World Health Organization 2013), tooth mobility status (Scottish Dental Clinical Effectiveness Programme 2014), and furcation involvement status (Newman et al. 2019). The details about calibration of dental examiners, the oral examinations, and categorizations used in this study are presented in the Appendix.
Statistical Methodology
Descriptive statistics were calculated to estimate the characteristics of the study population and the outcome variables: prevalence, severity, and extent of the impact based on the OHIP-14 data. For exploration of continuous data (the severity of the impact), normality testing included examination of histograms and Q-Q plots and the Shapiro-Wilk and Kolmogorov-Smirnov tests, while the Levene test was used to assess equality of variances.
The independent samples t test and the one-way analysis of variance (ANOVA) or Kruskal-Wallis test were used to analyze the severity of impact according to the predictor variables: demographics, socioeconomics, behavior, systemic disease, subjective appraisal about oral health, and oral health condition. The independent t test was performed where there were 2 groups of independent variables. Dependent variable residuals normality in each group of independent variables was checked before the one-way ANOVA or Kruskal-Wallis test. An ANOVA test was performed when there were >2 groups of independent variables, evidence of the residuals normality distribution, and no evidence of a violation to homogeneity of variance assumptions. A Kruskal-Wallis test was performed when there were >2 groups and there was evidence of a violation to the residual normality distribution.
To examine the relationship between prevalence of impact and 1) periodontal condition (periodontal status, mobility status, and furcation status) and 2) each of the 7 domains of OHIP, the Pearson chi-square test or Fisher exact test was performed and a corresponding odds ratio and 95% CI calculated. A Fisher exact test was used when cells had expected frequencies <5.
For exploration of extent of impact, general assumptions of the nonparametric tests were checked before performing the nonparametric tests. The Mann-Whitney U test and Kruskal-Wallis test were used to analyze the extent of impact score according to the predictor variables. The Mann-Whitney U test was performed to test for differences in the extent of impact score between 2 groups of a categorical variable. The Kruskal-Wallis test was performed to test for differences of the extent of impact score among ≥3 groups of categorical variable.
In addition, a Jonckheere-Terpstra test for ordered alternatives was conducted to determine if there was a statistically significant trend between the independent variables and the extent of impact score. For nonparametric testing, we used the effect size proposed by a Rosenthal calculation (Rosenthal’s r) for the Mann-Whitney U test and an eta-squared calculation for the Kruskal-Wallis test. The interpretation of this effect size was based on Cohen’s work for nonparametric tests: r ≤ 0.1, small effect size; 0.1 < r ≤ 0.3, small to medium effect size; 0.3 < r ≤ 0.5, medium to large effect size; r > 0.5, large effect size (Pallant 2016).
Robust regression was carried out to determine the adjusted effect of each predictor variable on the total OHIP-14 scores (severity of the impact) as our data violated the assumption of normality and homoscedasticity. Model 1 examined the strength of the relationship between periodontal condition variables (periodontal status, mobility status, and furcation status) and the OHIP-14 scores. Model 2 included model 1 and adjusted for age, sex, marital status, education, income, smoking status, brushing habits, pattern of dental visit, diabetes status, diabetes time duration, and subjective appraisal of dental health. Finally, model 3 was additionally controlled for other oral health assessments (DMF-T score and OHI-S). Collinearity diagnostics were performed before running the regression model. The bootstrapped confidence intervals and significance values were reported, as they did not rely on assumptions of normality and homoscedasticity.
Results
Our study found that almost 75% of the older people had generalized periodontitis. Of the remaining participants, around 22% had localized periodontitis, and almost 3% had a healthy periodontal condition. The mean number of teeth present in the sample was 19.36 (SD = 7.02).
Summary data of the characteristics of the sample are presented in Table 1. The characteristics of the prevalence, severity, and extent of the impacts for each OHIP-14 dimension are presented in Appendix Table 1.
Characteristics of the sample.
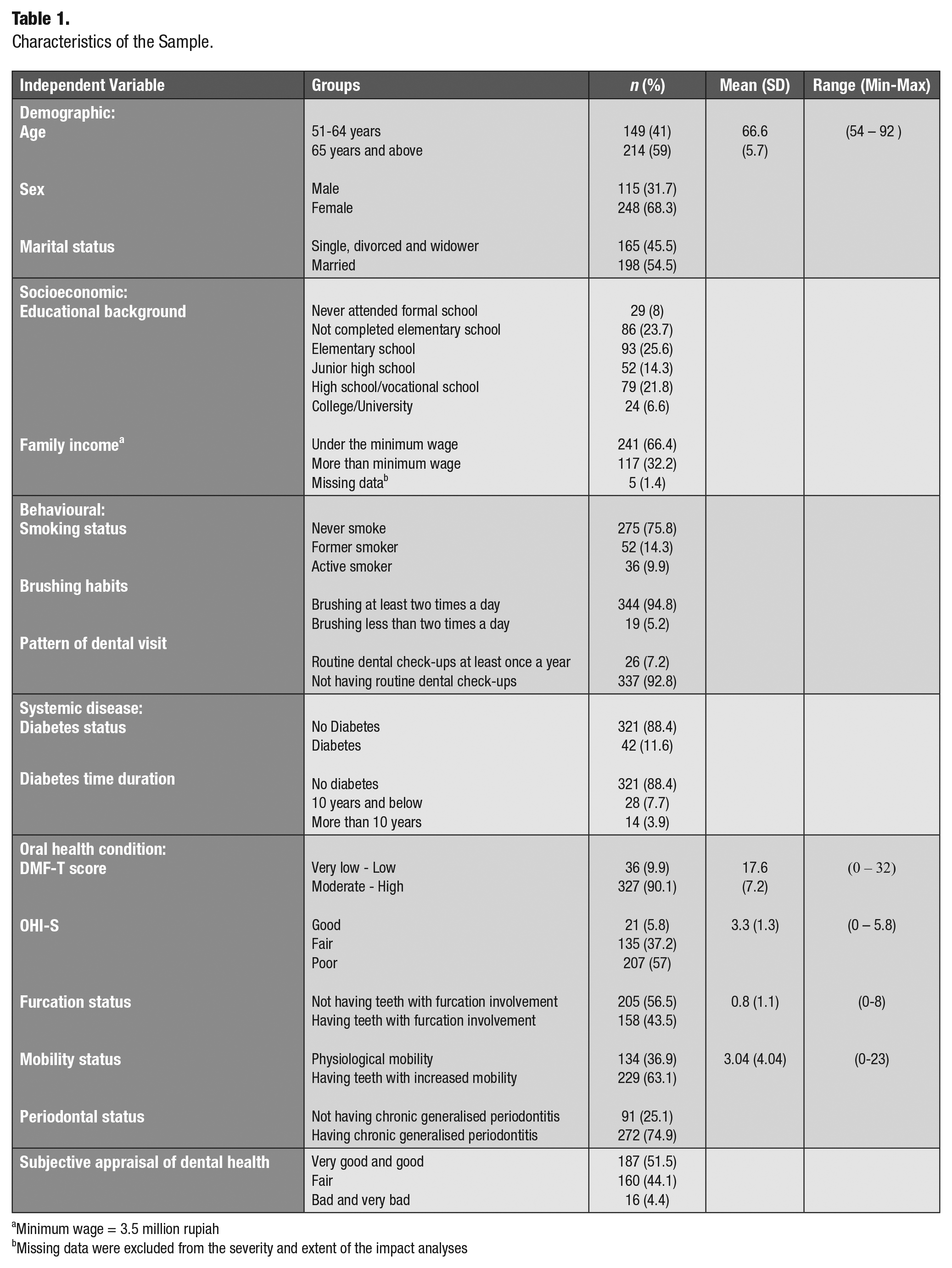
Minimum wage = 3.5 million rupiah
Missing data were excluded from the severity and extent of the impact analyses
Periodontal Disease and Prevalence of the Impact
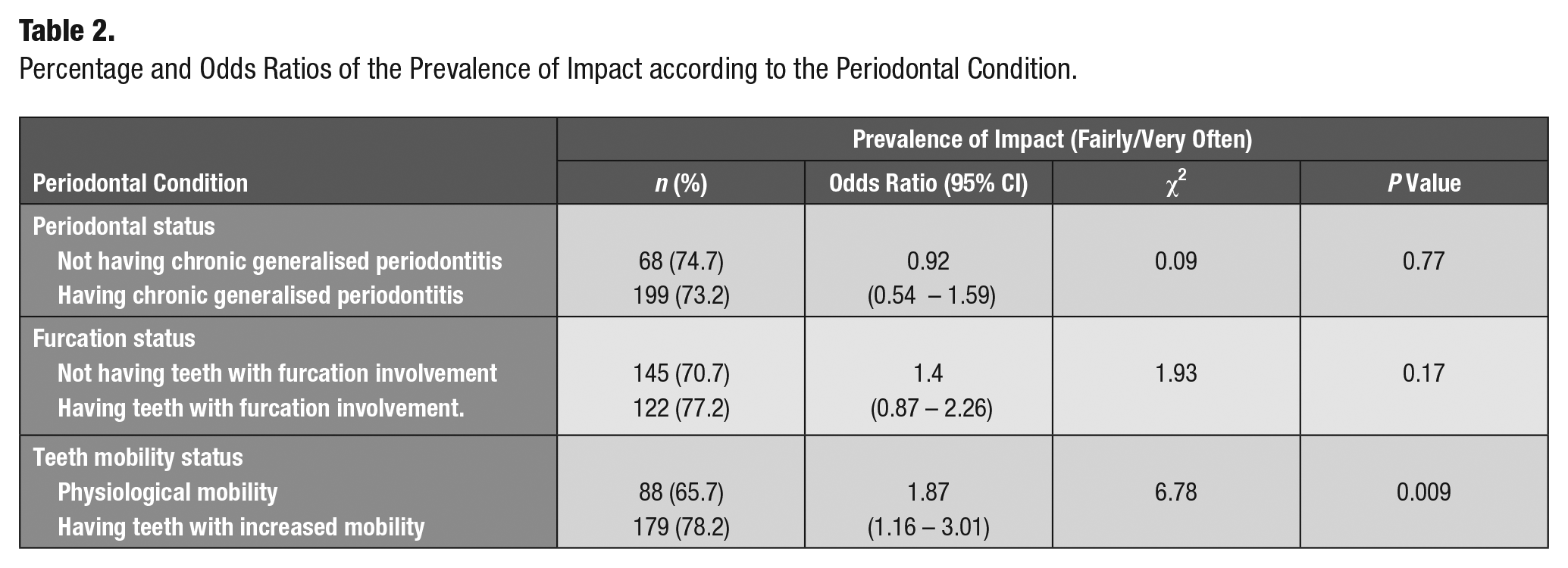
While prevalence of impact was not significantly associated with periodontal disease and furcation status, it was significantly associated with teeth mobility status, which is a recognized periodontal disease manifestation. Older people who had teeth with increased mobility were more likely to experience an impact on their OHRQoL, with the odds ratio being almost 2 times that of older people who did not have any teeth with increased mobility (Table 2). This result is explained further by 5 domains of the OHIP that were significantly associated with teeth mobility status: functional limitations, physical pain, psychological discomfort, physical disability, and handicap (Appendix Table 2).
Percentage and odds ratios of the prevalence of impact according to the periodontal condition.
Severity of the Impact
The severity of the impact differed significantly according to brushing habits, DMF-T, teeth mobility, and subjective appraisal of dental health (Table 3).
Severity of the impact according to the predictor variables.
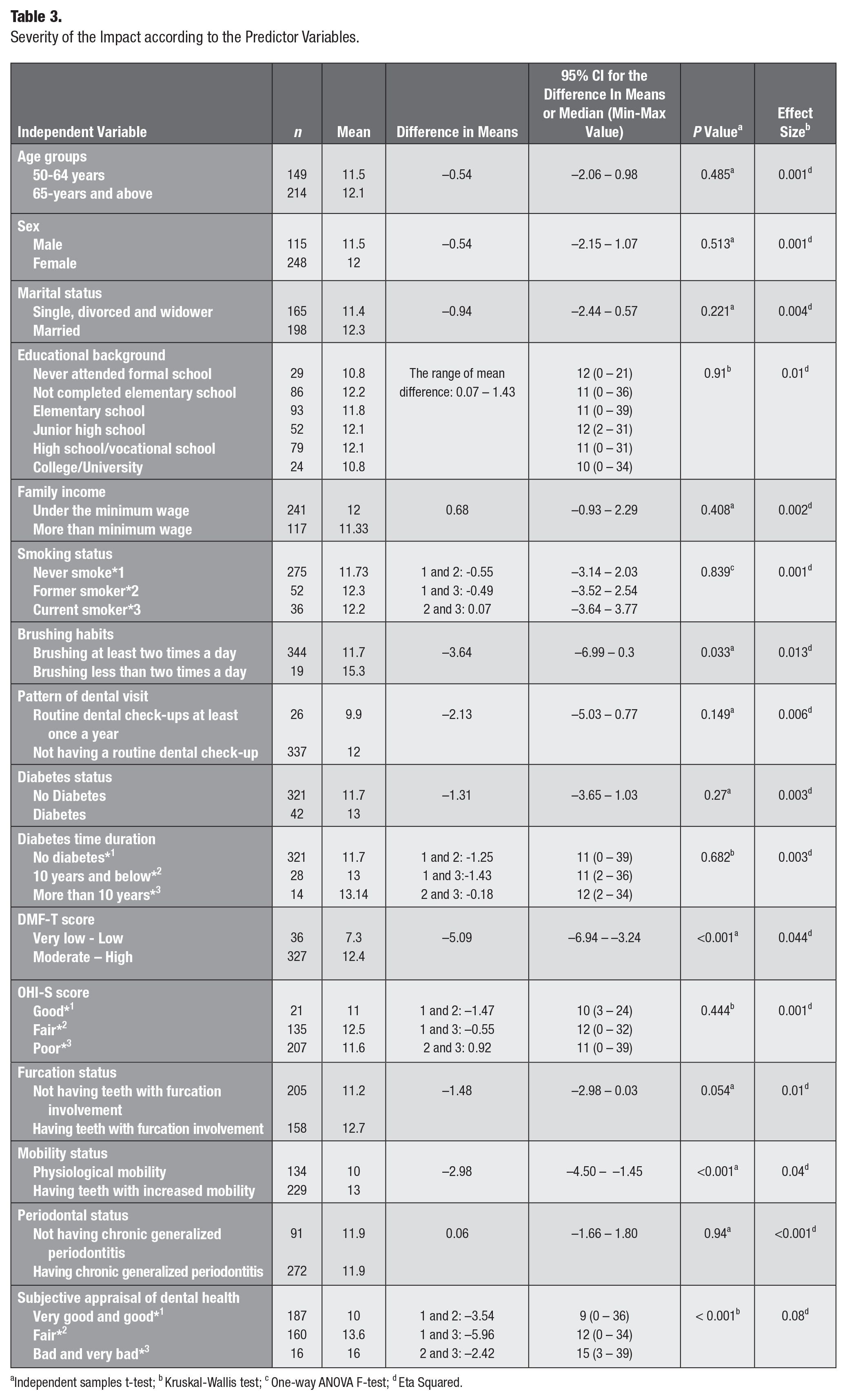
Independent samples t-test; b Kruskal-Wallis test; c One-way ANOVA F-test; d Eta Squared
Pairwise comparisons between categories of the subjective appraisal of dental health variable with Bonferroni corrections for multiple tests showed a statistically significant difference between those participants categorized as “very good and good” and “fair” (P < 0.001, r = −0.29) and between those categorized as “very good and good” and “bad and very bad” (P = 0.034, r = −0.18).
A Jonckheere-Terpstra test for ordered alternatives showed a statistically significant increasing trend in severity of impact score with worse levels of subjective appraisal of dental condition (P < 0.001).
Extent of the Impact
The extent of impact differed significantly according to family income, brushing habits, pattern of dental visit, subjective appraisal of dental health, DMF-T, furcation involvement, and mobility status (Table 4).
Extent of the impact according to the predictor variables.
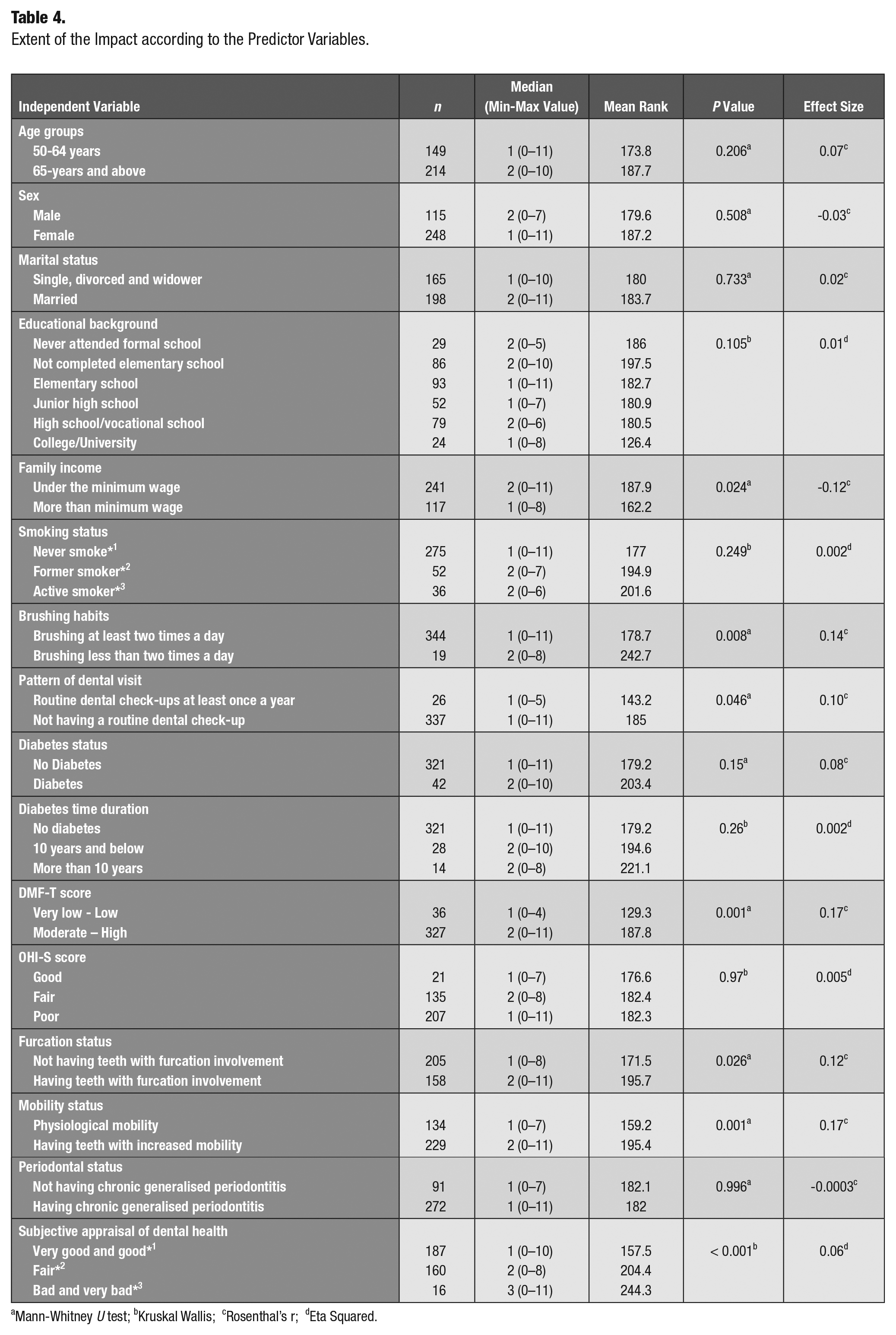
Mann-Whitney U test; b Kruskal Wallis ; c Rosenthal’s r; dEta Squared
Pairwise comparison between categories of subjective appraisal of dental condition showed a statistically significant difference of the extent of impact score between the categories “very good and good” and “fair” (P < 0.001) and between “very good and good” and “bad and very bad” (P = 0.004).
A Jonckheere-Terpstra test for ordered alternatives showed a statistically significant increasing trend in extent of impact scores with worse levels of subjective appraisal of dental condition (P < 0.001).
Multiple Regression Models of Predictors Variables on the Total OHIP-14 Score
The results from the multiple regression model (Table 5) show that the severity of the impact was significantly associated with teeth mobility status, DMF-T, and subjective appraisal in the fully adjusted model. The model explained 16.4% variability of the severity of the impact (R2 = 0.164). Teeth mobility status, as one of periodontal condition variables, showed a significant association with the severity of the impact. This relationship was attenuated but remained significant after adjustment for demographic, socioeconomic, behavioral, systemic disease, subjective appraisal about oral health, and other oral health assessment (P = 0.002, model 1; P = 0.005, model 2; P = 0.01, model 3). Collinearity diagnostics indicates that there is no collinearity issue within our data.
Multiple Regression Models of Predictors Variables on the Total OHIP-14 Scores (Severity of the Impact) With Bias-Corrected and Accelerated 95% CIs.
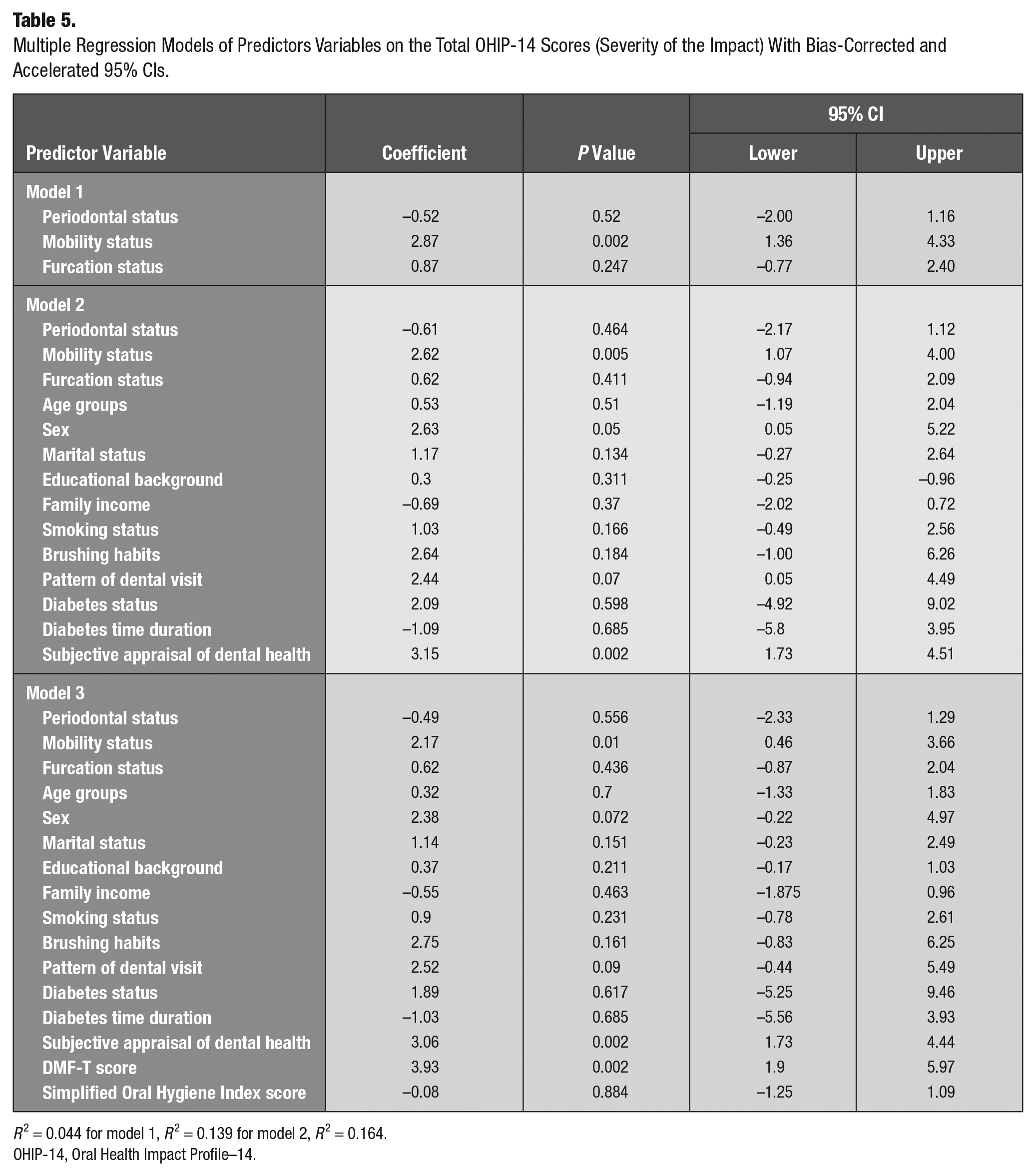
Note: R2 = 0.044 for model 1; R2 = 0.139 for model 2; R2 = 0.16
Discussion
In this study, the 4 dimensions of the OHIP that most commonly fell under the highest prevalence of impact were psychological discomfort (57.3%), functional limitation (37.2%), physical pain (28.7%), and physical disability (26.4%). This is consistent with a national survey of the Canadian adult population, where psychological discomfort (11.3%), physical pain (9.3%), psychological disability (6.1%), and physical disability (5.4%) were the 4 most reported dimensions that affected OHRQoL (Locker and Quiñonez 2009). By comparison, a cross-sectional study of 20- to 64-y-olds in Brazil found psychological discomfort (35.8%), physical pain (19.6%), psychological disability (19.4%), and physical disability (17.0%) as the most reported impacts (Batista et al. 2014). A birth cohort study of 32 y conducted in New Zealand accounted physical disability (10.7%) and psychological disability (10.3%) as the most reported OHIP dimensions (Lawrence et al. 2008). Interestingly, our findings of the most reported impacts of OHIP’s dimensions are considerably high in comparison with the previous studies. Another difference from the earlier studies is that our findings marked functional limitation as one of the dimensions with a high prevalence. These discrepancies might be due to differences in sample characteristics, including age ranges. This study focuses on older people of age ≥50 y. For this age group, oral health problems and high numbers of missing teeth may be more prevalent, leading to more oral health functional problems.
This study and a number of previous studies found a discrepancy between periodontal clinical findings and OHRQoL assessed through the OHIP-14 (Mariño et al. 2008; Montero-Martin et al. 2009; Khalifa et al. 2013; Lawal et al. 2014; Sanadhya et al. 2015; Kato et al. 2018). Some of the comparable previous studies focused on developing countries (India, Nigeria, and Sudan) and some others on developed countries (Sweden, Spain, and Australia). Most of the previous studies that confirmed an association between periodontal disease and OHRQoL focused on developed countries—Sweden (Jansson et al. 2014), Germany (Brauchle et al. 2013), and the United Kingdom (Jowett et al. 2009; Bernabé and Marcenes 2010; White et al. 2012)—with an exception being a Brazilian study (Palma et al. 2013). The differences in study findings might be influenced by differing subjective perceptions, expectations, preferences, income social, psychological state, and psychological support (Tsakos et al. 2006).
Another consideration is the periodontal disease categorization used in this study. Almost all of the participants in the study presented teeth affected by periodontitis; 97% of the participants had ≥1 teeth with probing pocket depth ≥3.5 mm. The high prevalence of periodontal disease might be due to the BPE as a sole indication to determine the periodontal disease. For comparative purposes, we divided respondents into 2 groups according to presence or absence of chronic generalized periodontitis. Based on this classification, some of the participants might have had missing teeth due to generalized periodontitis in the past, which was not accounted for in our study. Consequently, through focusing on existing rather than historical periodontal data for participants, we may have underestimated the extent of chronic periodontitis in the past in some cases and, in turn, a potential association between periodontal disease status and OHRQoL. Another point of interest was the higher prevalence of periodontal disease in this study (97%) versus the national prevalence in those aged ≥45 y (77.8%), which may affect the true relationship between periodontal disease and OHRQoL (Badan Penelitian dan Pengembangan Kesehatan 2019). This high prevalence of periodontal disease in the sample has introduced an unequal sample distribution between older people who did not have generalized periodontitis and those who did (ratio 1:3), which may have reduced statistical power on comparing across groups.
While we did not identify a significant association between periodontal disease status and OHRQoL, we found a significant relationship between tooth mobility and OHRQoL. For all 3 estimates of OHIP, there was a highly significant relationship between tooth mobility and OHRQoL.
While there was a highly significant difference in the severity of impact according to tooth mobility status, the difference did not reach the MID threshold. However, we need to highlight that the MID threshold was based on the longitudinal study, while our study is a cross-sectional study. None of the previous works reported the MID for a cross-sectional study with a nonnormal distribution of the OHIP scores up to the present time. Nevertheless, there was strong evidence of the relationship shown by the prevalence and extent of the impacts assessments. In this case, older people with increased teeth mobility were 1.87 times more likely to experience negative impacts on their OHRQoL as compared with those who did not have teeth with increased mobility. The multiple regression model also confirms a significant relationship between teeth mobility and severity of the impact on OHRQoL after adjustment for other predictors.
The discrepancy of the association between periodontal disease and OHRQoL may be understood by the nature of periodontal disease as a chronic disease. This chronic disease may not show significant symptoms until it progresses to a later stage and creates obvious symptoms, such as tooth mobility (Petersen and Ogawa 2012).
There was no statistically significant relationship between the furcation status and prevalence of impacts. The P value for the difference in mean severity of impact on the OHRQoL according to furcation status was slightly above the statistical significance level (P = 0.054). However, there was a statistically significant difference in the extent of impact according to the furcation status. To compare this study’s findings with the previous studies, a literature search was done regarding the association between furcation involvement and OHRQoL through the MEDLINE database with keywords “furcation” and “quality of life.” There were no previous studies that assessed this relationship up until data accessed on January 11, 2021.
This study attempted to assess the relationship between OHRQoL and other predictors. The assessment was based on OHIP severity and extent of impact as outcome measurements.
None of the demographic variables and systemic disease variables showed a significant relationship with the OHRQoL. A previous study reported that periodontal disease is significantly associated with type 2 diabetes (Chapple 2014). Although poorly controlled diabetes mellitus has been established as one of the important factors related to periodontal health, the diabetes status and diabetes time duration variables in this study did not show any significant relationship with OHRQoL.
The behavioral variables in this study comprised brushing habits, smoking status, and pattern of dental visits. Severity of impact was significantly different according to brushing habit, while extent of impact was significantly different according to each brushing habit and pattern of visit. These results were expected as better oral health maintenance can help people maintain oral health.
Previous studies demonstrated that the prevalence of pocket depth, attachment loss, and alveolar bone loss was higher in smokers as compared with nonsmokers (Johnson and Hill 2004; Johnson and Guthmiller 2007). Surprisingly, while smoking status is recognized as one of the important risk factors for periodontal disease, no significant difference was found in severity or extent of impact according to smoking status. The proportions of former and current smokers in our sample were quite low, approximately 14% and 10%, respectively, which may have reduced statistical power on comparing across groups. As might be expected, the mean score of the severity of the impact was higher in former smokers and current smokers as compared with those who had never smoked. However, the differences were small and did not achieve statistical significance.
Older people who had a routine dental check-up at least once a year reported being affected by fewer OHRQoL dimensions than those who did not have any routine dental check-up. Regular dental visits should allow dentists to detect oral health problems earlier and treat diseases before they progress to an advanced stage, which may affect OHRQoL.
Socioeconomic factors examined in this study included educational background and family income. The severity and extent of the impact did not differ significantly according to educational background. A significant difference emerged for the extent of impact according to family income.
This study assessed the relationship between OHRQoL and other oral health predictors, including DMF-T and OHI-S. For each of severity and extent of impact, there was a highly significant difference according to DMF-T.
Neither severity nor extent of impact assessment was statistically significant according to the OHI-S score. The OHI-S score was calculated as the mean of the debris and calculus scores from the present teeth. In the event that a participant did not have molars or incisors for ≥1 of the 6 segments measured for the OHI-S score, those segments were excluded from the calculation. Such participants might have experienced impacts on their OHRQoL due to tooth loss, and their OHI-S score could had been relatively low, given that the missing teeth were not reflected in this score. This may help to explain why we did not find a significant relationship between OHI-S and OHRQoL. This possibility is supported by our data. Participants with better oral hygiene had more missing teeth, on average: good hygiene, 15.1 missing teeth; fair hygiene, 12.41; and poor hygiene, 12.23.
Subjective appraisal of dental health was associated with quality of life. The better dental health subjectively appraised by the participants reflected the lower score of both severity and extent of the impacts.
In conclusion, although our research did not show a significant relationship between periodontal disease status and OHRQoL, we found a substantial relationship between teeth mobility and OHRQoL. This finding was confirmed through the prevalence, severity, and extent of impact as measures of OHRQoL and the multiple regression model. Our findings also revealed a significant relationship between tooth furcation and extent of impact on older people’s OHRQoL. Thus, we underline the potential negative impact of advanced progression of chronic periodontitis on OHRQoL, such as increased tooth mobility and furcation involvement.
This study has some limitations. First it mainly focused on periodontal disease screening through the BPE. Specifically, it did not perform further examinations to establish a diagnosis of periodontal disease, such as clinical attachment loss and radiographic assessment, mainly due to a time limitation in data collection. Furthermore, as a nature of cross-sectional study, ours cannot assess the causality relationship between periodontal disease (including other predictor variables) and OHRQoL. Thus, a longitudinal study is needed to provide a better understanding of the causality relationship between the predictors and OHRQoL.
To the best of our knowledge, this is the first study to assess the relationship between periodontal disease and OHRQoL in older people in Indonesia delivered at the population level. The other strength is that the study includes the assessment of participants’ characteristics as predictors of the OHRQoL: demographics, socioeconomics, behavior, systemic disease, and subjective appraisal of dental health.
Author Contributions
M. Hijryana, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; M. MacDougall, A.W.G. Walls, contributed to conception, design, and data interpretation, critically revised the manuscript; N. Ariani, P. Saksono, contributed to data acquisition, critically revised the manuscript; L.S. Kusdhany, contributed to data interpretation, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jct-10.1177_23800844211021391 – Supplemental material for Periodontal Disease and Oral Health–Related Quality of Life in the Older Population in Indonesia
Supplemental material, sj-docx-1-jct-10.1177_23800844211021391 for Periodontal Disease and Oral Health–Related Quality of Life in the Older Population in Indonesia by M. Hijryana, M. MacDougall, N. Ariani, P. Saksono, L.S. Kusdhany and A.W.G. Walls in JDR Clinical & Translational Research
Footnotes
Acknowledgements
The authors thank the Principal’s Career Development PhD Scholarships and the Edinburgh Global Research Scholarship from the University of Edinburgh for supporting the PhD study of M. Hijryana.
A supplemental appendix to this article is available online.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors thank the Principal’s Career Development PhD Scholarships and the Edinburgh Global Research Scholarship from the University of Edinburgh for supporting the PhD study of M. Hijryana.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.