
Abstract
Introduction:
There has been little research to explore how adults financially value private orthodontic treatment and whether they have preferences for different attributes of treatment. This study used a discrete choice experiment and aimed to determine whether the recognized skill level of the dental professional and the type of orthodontic appliance influence the values that the public places on private adult orthodontic treatment.
Methods:
In total, 206 adult patients or the parents/guardians of children attending general dental practices in the northeast of England were recruited to complete a discrete choice experiment. Three attributes were included: the type of dental professional providing treatment, the type of orthodontic appliance, and cost. Also collected were demographic and orthodontic history characteristics. Results were analyzed with conditional logistic regression and elicited marginal willingness to pay (MWTP).
Results:
Participants value the training and expertise of the dental professional providing private orthodontic treatment greater than the type of orthodontic appliance. MWTP for orthodontic treatment increased in conjunction with the recognized skill level of the dental professional. Participants were willing to pay more for aesthetic appliances over a fixed metal appliance.
Conclusions:
Participants value the training and expertise of the dental professional providing private adult orthodontic treatment greater than the type of orthodontic appliance. These preferences concur with other discrete choice experiments undertaken in medical specialties that included attributes focusing on the qualification, skill, or expertise of the health care professional. MWTP for orthodontic treatment increased in conjunction with the recognized skill level of the dental professional. Participants were willing to pay more for aesthetic appliances than metal fixed appliances. The cost of orthodontics is significant, and adults appreciate the importance of having options and making choices.
Keywords
Introduction
The demand for adult orthodontic treatment is steadily increasing in absolute terms (Keim et al. 2017). The development of aesthetic appliances, wider-reaching advertising and orthodontic awareness, and an increasingly positive attitude toward treatment may have contributed to this rise. Greater availability and accessibility of services, increased disposable income, and improvements in dental health may also explain this (Almuzian and Gardner 2014a, b). Adults’ motives to seek orthodontic treatment are multifactorial. Most patients desire straighter teeth and an improvement in smile aesthetics (Pabari et al. 2011).
Patients appreciate having options and making choices within health care (Dixon et al. 2010). Patients may wish to decide on the type of treatment, the provider, and the timing and location of their appointments. Policy in England has focused on increasing choice around where and when to deliver care (Dixon et al. 2010). Ultimately, the cost of orthodontics is largely based on an individual’s ability to pay, and adults need information and time to consider their options. Informing individuals is important as their preferences and treatment decisions may change (Mulley et al. 2012).
In England, most adults pay for orthodontic treatment under private arrangements, as there is limited scope to receive treatment on the National Health Service (NHS; Cedro et al. 2010). Private orthodontic treatment can address the aesthetic concerns shared by adults. Adults tend to be cautious about accepting fixed metal appliances and instead request more aesthetic appliances (Jeremiah et al. 2011). Transparent aligners have become popular with adults (Meier et al. 2003).
In the United Kingdom, specialist orthodontists, dentists with enhanced skills, and general dental practitioners (GDPs) provide private adult orthodontic treatment. Specialist orthodontists have commonly completed an additional 3 y of comprehensive training and examinations. GDPs are expected to be competent in recognizing and monitoring the developing occlusion, assessing and diagnosing a malocclusion, and referring appropriately to a specialist orthodontist. GDPs should also be competent in treating patients’ oral health before, during, and after orthodontic treatment. Dentists with enhanced skills and experience have gained additional shorter-term training in orthodontics to develop competencies and forward career aspirations. The additional experience and training undertaken vary widely among practitioners. Dentists with enhanced skills and GDPs cannot use the title “specialist,” as they are not eligible for specialist list registration with the General Dental Council (NHS England 2015). While comprehensive orthodontic treatment is likely to remain in the remit of specialist orthodontists, nonspecialists increasingly offer limited treatment orthodontics as a minimally invasive and affordable alternative to improve smile aesthetics (Maini 2013). Debate exists within the dental and orthodontic communities regarding the merits of limited treatment orthodontics (Chate 2013). Concern has been raised by the orthodontic profession and indemnity companies in relation to training (Ireland et al. 2015; Noah et al. 2015). Ultimately, specialists and nonspecialists providing orthodontic treatment should inform patients of their training, experience, and competencies and practice within their remit (General Dental Council 2013).
Economics has specific methods to measure preferences, including revealed methods (where existing behavior determines preference) and stated methods (where respondents state how they would behave). Stated rather than revealed preference methods are suitable to use in this context because this market is imperfect in terms of economics. There are likely to be information asymmetries and externalities that would distort revealed preferences. Willingness to pay (WTP) can elicit the strength of a preference for an intervention or commodity as a whole, as well as for health states. Contingent valuation and discrete choice experiments (DCEs) are the 2 stated preference methods for providing estimates of monetary valuation (Donaldson and Shackley 1997).
A DCE is appropriate when the importance of different characteristics (attributes) of a particular intervention need establishing. DCEs use hypothetical scenarios and ask people to make choices among alternatives. Respondents weigh up and trade off the positive and negative aspects of multiple competing attributes (Barber et al. 2018). The method is firmly rooted in Lancaster’s (1966) economic theory of value and the random utility theory (McFadden 1974). An assumption is made that the utility (value) that participants attach to an intervention is described by the sum of individual attributes of that intervention. DCEs can identify how individuals are willing to trade between attributes, estimate the importance of an attribute in isolation or relative to other attributes, and predict demand for an intervention with given characteristics. DCEs estimate marginal rates of substitution between attributes of a good or service. This expresses how much of an attribute a participant will give up to have more of another attribute. Trade-offs are calculated in terms of waiting time, traveling distance, or cost. Inclusion of cost as an attribute makes it possible to estimate WTP indirectly, which is otherwise termed marginal WTP (MWTP). DCEs are widely advocated in health economics, and their use in dentistry continues to grow (Ryan et al. 2008; Barber et al. 2018).
To date, there is little research exploring how adults value orthodontic treatment or whether they have preferences for different attributes of treatment. This study used a DCE and aimed to determine whether the recognized skill level of the dental professional or the type of orthodontic appliance influences the values that the public places on private adult orthodontic treatment.
Methods
Study Design
A DCE with a self-completing questionnaire was undertaken in 4 NHS general dental practices in the northeast region of England. The study had ethical approval from the Newcastle and North Tyneside 2 Research Ethics Committee (reference 17/NE/0349).
Questionnaire Design
The DCE was part of a larger questionnaire used in a research project exploring how the population financially valued adult orthodontic treatment. Of relevance to this study were 3 out of the 4 sections of the questionnaire: demographic details, orthodontic treatment experiences, and the DCE. Participants completed demographic information about themselves, including age, gender, postcode (for determination of index of multiple deprivation), employment details (for determination of socioeconomic status), income, qualification level, and ethnicity. These questions were based on standardized national questions where possible. Participants were questioned about their previous experience of orthodontic treatment (if any), their child’s experience of orthodontic treatment (if appropriate), and their personal perceived need for treatment.
DCE Design
Potential attributes and their levels (including costs) were discussed by a research team and then a patient and public involvement group. The latter is well established at Newcastle University as contributing to oral and dental research, and group members have been recruited through various means. Three attributes were included in this study: the type of dental professional providing treatment, the type of orthodontic appliance, and cost. The attribute levels associated with the type of dentist and appliance were related to the orthodontic options available in the United Kingdom (NHS England 2015). Attribute levels were as follows:
Type of dentist: (1) specialist orthodontist, (2) dentist with enhanced skills in orthodontics, (3) GDP
Type of orthodontic appliance: (1) metal fixed appliance, (2) tooth-colored fixed appliance, (3) lingual fixed appliance, (4) clear aligners
Cost: (1) £500, (2) £1,000, (3) £,2000, (4) £4,000
While the attribute levels associated with cost may not necessarily reflect the actual cost of treatment, the presence of a continuous variable enables MWTP to be calculated. The cost levels were discussed with the patient and public involvement group.
Forty-eight profiles existed—2 attributes at 4 levels and 1 attribute at 3 levels (42 × 31)—and if all combinations of levels were used, it would result in a full factorial design of 1,128 pairwise choices: (48 × 47) / 2. The full factorial design of 48 profiles was reduced to a fractional factorial design of 16 profiles by using R (R Core Team 2017). A mixed orthogonal array selected 16 choice sets from these 16 profiles. This was D-efficient (Aizaki and Nishimura 2008). Including a choice set where one option was unambiguously dominant over the other enabled a rationality check to be undertaken, which would identify whether participants understood the nature of the experiment conducted.
Participants considered different factors that might influence their choices of private orthodontic treatment in a hypothetical situation. Explanations and pictures informed participants of the main differences between the clinicians and appliances. An example of a choice set illustrates the DCE concept (Figure). Participants selected 1 option from each choice set, forcing trade-offs between the attributes. They could opt out and select no orthodontic treatment instead of the pair of choices presented. This was appropriate given the elective nature of the intervention. Participants completed 8 choice sets chosen at random from the series of 16. Across the whole sample, multiple participants valued each choice set.
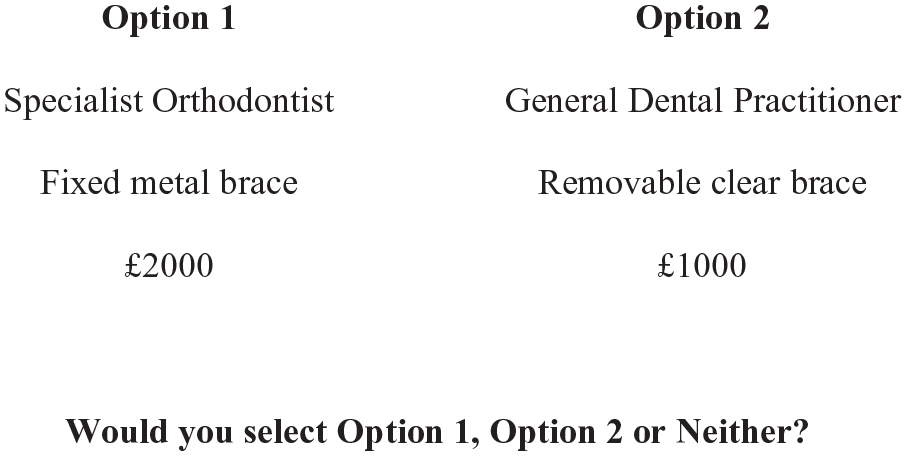
Example of a choice set in discrete choice experiment.
The research team developed the questionnaire, which was refined through the patient and public involvement group. Dental core trainees at Newcastle Dental Hospital / Newcastle University piloted the questionnaire, and minor amendments were made. A word version of the introduction to the choice task is available as an Appendix, although this lacks some of the functionality of the electronic survey.
Sample
The target population was patients or the parents/guardians of children attending dental appointments in the northeast of England. The sample was recruited from 4 NHS general dental practices between January 2018 and February 2018. The practices selected were part of the Northern Dental Practice Based Research Network. They were chosen on the basis of not being orthodontic providers and being willing to participate without a conflict of interest. Participants were considered for inclusion if they were ≥18 y old, had the capacity to consent for participation, and could read/write in English.
For the DCE, a required sample size of 100 was calculated with R (R Core Team 2017). This was based on the following: a significance level (α) of 0.05; a statistical power level (1 – ß) at 80%; a conditional logit model used in the DCE analysis; a DCE design with 8 parameters, 3 alternatives, and 16 choice sets; and estimated coefficient values (de Bekker-Grob et al. 2015). However, a larger sample of 200 participants was ultimately required for another arm of the project, which explored whether the public and profession would value an NHS-funded adult orthodontic service.
Data Collection
Patients attending for routine dental care were approached by research team members and practice receptionists via a convenience sampling method (for practical reasons). The researchers explained the study and provided information sheets in the practice waiting rooms. Those who agreed to participate were enrolled into the study. Informed consent was obtained by participants electronically ticking an opt-in box on a tablet computer provided by the research team. The questionnaire was conducted in a digital format per Qualtrics (2018) and completed on the tablet computer. The questionnaire could also have been conducted face-to-face by a member of the research team if requested by the participant. Participants completed the questionnaire before or after their dental appointments, either way without impinging on the running of the practice. Recruitment procedures and data collection were the same in all 4 centers.
Analysis
Data were analyzed in Stata 15 (StataCorp 2017). Since participants answered 8 choice sets and each choice set had 3 alternatives, there were 24 observations per participant. Dummying of the multilevel categorical variables was required for the regression. Rationality checking validated the inputted data, with irrational and noncorrectable data considered missing.
Descriptive statistics of the final sample were undertaken. A conditional logit model with fixed effects included the 3 main attributes. While the analysis of DCEs remains an area of active debate (Hauber et al. 2016), it is reasonable to assume that the utility function includes unobserved heterogeneity that may be correlated with observed variables, hence the choice of model. Calculating marginal rates of substitution elicited MWTP values.
Results
The final sample recruited 206 adult patients or the parents/guardians of children attending general dental practices. All participants completed the 8 choice sets, resulting in 4,944 observations for the analysis. All participants answering the rationality checking set provided consistent responses (95 participants answered this question: 78 answered this correctly and 17 abstained/chose neither). Tables 1 and 2 show the demographic and orthodontic characteristics of the sample, which included a good representation across levels in all variables except ethnicity. Similar proportions of participants had previously received orthodontic treatment or were keen to seek treatment.
Demographic Status for Sample (N = 206).

GCSE, General Certificate of Secondary Education; NS-SEC, UK National Statistics Socioeconomic Classification.
Orthodontic Status for Sample (N = 206).

Table 3 shows coefficients and confidence intervals from the initial conditional logistic regression model. Overall, participants valued the type of dental professional providing private orthodontic treatment greater than the type of orthodontic appliance worn. Participants preferred a specialist to the other dental professionals. Participants preferred all 3 aesthetic appliances over a metal fixed appliance. A tooth-colored fixed appliance was the most preferred aesthetic option. Cost had a significant effect, with participants more likely to choose orthodontic treatment with a lower cost.
Conditional Logistic Regression Model.

DES, dentist with enhanced skills.
From the MWTP analysis shown in Table 4, the most valued attribute was the type of dental professional, and MWTP increased in conjunction with the recognized skill level. Participants were willing to pay £2,410 more for a specialist to provide private adult orthodontic treatment over a GDP and £980 more for a specialist over a dentist with enhanced skills. Participants were willing to pay £1,800 more for a tooth-colored fixed appliance over a metal fixed appliance.
MWTP Values for Different Attribute Levels.

DES, dentist with enhanced skills; MWTP, marginal willingness to pay.
Discussion
This study showed significant differences in MWTP for private adult orthodontic treatment relative to the recognized skill level of the dental professional and the type of orthodontic appliance. Fees for private orthodontic treatment start at around £2,000 in the region where the study was undertaken but can be higher depending on treatment complexity and the type of appliances used (Vernazza et al. 2018). The MWTP value of £2,410 for orthodontic treatment provided by a specialist over a GDP is greater than the private market rate. As compared with a metal fixed appliance, the MWTP value of £1,800 for a tooth-colored fixed appliance is greater than the private market rate, whereas for a lingual fixed appliance, the MWTP value of £990 is significantly less.
It is surprising that the difference in provider expertise is valued more than the difference in appliance type. This study suggests that participants highly value the expertise of the clinician. These preferences concur with DCEs undertaken in medical specialties, which included attributes focusing on the qualification, skill, or expertise of the health care professional (Kimman et al. 2010; Wong et al. 2016; Meads et al. 2017). Patients’ preferences for more qualified/specialized individuals or services were statistically significant and conformed with the a priori expectations across different specialties, environments, and countries. This is unsurprising given patients’ predisposed understanding of a medical or hospital environment. The health care professional attribute was considered the most important attribute by patients (Kimman et al. 2010; Wong et al. 2016), except in medical situations requiring pain management where the control of side effects and provision of better information and communication were preferred (Meads et al. 2017).
This study suggests that participants were willing to pay more for aesthetic appliances than for metal fixed appliances. Specifically, participants preferred tooth-colored fixed appliances, followed by clear aligners and lingual fixed appliances. Payment scaling methods have investigated the attractiveness, acceptability, and value of orthodontic appliances by measuring WTP directly. A US-based study using a low-to-high payment scale revealed that participants were willing to pay the most for lingual appliances and clear aligners, followed by ceramic brackets (Rosvall et al. 2009). While lingual brackets were deemed the most attractive and metal brackets the least in an Iranian study, their acceptability ratings were reversed (Moshkelgosha et al. 2015). Two international studies do not support the findings of this research. A Brazilian study found that adults were not willing to pay more for aesthetic braces over fixed metal braces (Feu et al. 2012). Clear aligner treatment was preferable in a study based on the bidding method, but no statistically significant difference was identified among the 3 aesthetic appliances (Farronato et al. 2016). However, the importance of these findings relative to other treatment attributes cannot be determined, since contingent valuation considers only a single attribute. Many cultural and health care differences exist between these countries and the United Kingdom. The United Kingdom has a state-funded NHS, and eligible orthodontic patients predominantly receive fixed metal braces since they are effective and comparatively cheap. Conversely, in the United States, most patients fund orthodontic treatment privately, although federally subsidized insurance is available to low-income families. Adults’ perceptions of wearing visible braces will likely vary among cultures, and personal wealth can influence this.
This is the first study employing a DCE to elicit public preferences for private adult orthodontic treatment. Restricting the DCE to 3 attributes was a limitation. A richer set of attributes and choice contexts would elicit further meaningful behavioral responses (Amaya-Amaya et al. 2008). While participants’ unfamiliarity with orthodontics increases cognitive difficulty, Ryan and Gerrard (2003) suggest that DCEs with 4 to 6 attributes are acceptable at maintaining participant efficiency. The research team and patient and public involvement group considered other attributes, such as appointment location and treatment time, but decided to hold these constant by not including them, surmising that values for appointment location had already been elicited. A UK-based study asked participants at 3 orthodontic practices to consider whether they would want more specialized, centrally located services or more personal and familiar local hospital care. Individuals were willing to wait an extra 1.3 mo to have a local clinic for their first appointment and an extra 1.5 mo for their second (Ryan and Farrar 2000). Treatment duration is a concern for adults, with a US-based survey suggesting that patients would prefer shorter treatment between 6 and 12 mo (Uribe et al. 2014). Equally, clinicians and orthodontic companies are keen to improve treatment efficiency. However, it may not be realistically feasible to change the length of treatment without compromising the result. Focus groups or other qualitative research methods would be beneficial for future research to identify missing attributes and enhance the realism and plausibility of the study (Amaya-Amaya et al. 2008; Kimman et al. 2010).
While the sample had good diversity from different demographic and orthodontic experience groups, this may not have represented the proportions found in the regional or national population. Recruiting throughout the United Kingdom would offer greater representation. It would be interesting to investigate whether patient demographics and perceived orthodontic treatment needs affect patient choice. This was not an original aim, and the sample was insufficiently powered to complete further regression modeling.
The study has some limitations, as there was no anchor around the expected outcome. Participants’ preference for a specialist was based on an assumption of similar outcomes and case mixes. A limited number of studies have used outcome measures to compare the quality of fixed or removable orthodontic treatment undertaken by specialists and nonspecialists. The visual analog scale and American Board of Orthodontics index were used to retrospectively compare the orthodontic treatment of specialists and nonspecialists on 255 high school students (Abei et al. 2004). Superior alignment scores were achieved by specialists for all areas of the mouth, statistically significant in the molar regions but not anteriorly. Patients were universally happy with their treatment outcome, and the type of provider did not influence this. The quality of aligner treatment by specialists and nonspecialists has not been compared. Appraising the treatment of mild malocclusions or less complex orthodontic cases is limited from a quantitative perspective. Qualitative research or patient satisfaction may be more appropriate when assessing the alignment of only the anterior teeth. It is plausible to hypothesize that similar outcomes can be achieved for less complex orthodontic cases regardless of provider. DCEs also have general limitations, similar to other stated preference techniques. How participants respond to hypothetical scenarios may not reflect their true preferences or actual choice behaviors (Meads et al. 2017). Participants will not necessarily consider all the attributes when making decisions but instead anchor their choices around existing perceptions, a single attribute, or a subset of attributes. Some participants may disengage and adopt simplifying strategies when presented with unfamiliar tasks (Ryan and Gerard 2003).
The findings from this DCE has implications for patients, clinicians, and policy makers. This research shows that the public is more willing to pay to have orthodontic care provided by different levels of dental service providers. However, patient and public preference is only one aspect of the decisions around levels of service provider available, and there may be other health system or policy advantages to different levels of provider. If a greater skill mix is considered a valuable policy direction to advance the future need and demand of orthodontic services in the United Kingdom, then patient education may be required. Encouraging specialization makes most sense if it leads to higher quality. However, this could be problematic if it mainly leads to higher costs for patients, even if they are willing to pay out of pocket. There is an incentive for clinicians to optimize their knowledge and skills to deliver the high-quality orthodontic treatment that patients are increasingly demanding and willing to pay for. Practices may want to market private orthodontic treatment by emphasizing their clinicians’ expertise and skills in conjunction with the appliances and brands available. In the United Kingdom, any advertising, promotional material, or other information that one produces must comply with the General Dental Council’s (2013) guidance on ethical advertising. While orthodontic specialty training is tailored around fixed metal braces, there is an argument to provide aesthetic appliances for teaching purposes. Aligner companies are starting to approach universities and discount their products so that postgraduate orthodontic students can treat a limited number of patients during their training. National guidance is required for the provision of NHS-funded adult orthodontic treatment to help patients understand what choices are available and to ensure that there is equal access across the country based on need and eligibility. Further research could investigate adult patients’ interest in paying an additional fee for aesthetic alternatives on the NHS. This may be particularly desirable for adults undergoing lengthier courses of treatment.
Conclusions
Participants value the training and expertise of the dental professional providing private adult orthodontic treatment greater than the type of orthodontic appliance. These preferences concur with other DCEs undertaken in medical specialties that included attributes focusing on the qualification, skill, or expertise of the health care professional. MWTP for orthodontic treatment increased in conjunction with the recognized skill level of the dental professional. Participants were willing to pay more for aesthetic appliances than for metal fixed appliances. The cost of orthodontics is significant, and adults appreciate the importance of having options and making choices.
Author Contributions
G.D. Fenton, M.H.M. Cazaly, contributed to conception, design, and data analysis, drafted the manuscript; S.L. Rolland, contributed to conception and design, critically revised the manuscript; C.R. Vernazza, contributed to conception, design, and data analysis, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-pdf-1-jct-10.1177_23800844211012670 – Supplemental material for Eliciting Preferences for Adult Orthodontic Treatment: A Discrete Choice Experiment
Supplemental material, sj-pdf-1-jct-10.1177_23800844211012670 for Eliciting Preferences for Adult Orthodontic Treatment: A Discrete Choice Experiment by G.D. Fenton, M.H.M. Cazaly, S.L. Rolland and C.R. Vernazza in JDR Clinical & Translational Research
Footnotes
Acknowledgements
The authors thank all the participants in the study and the staff in the general dental practices. The authors also wish to thank Kathryn Edwards and Jennifer Rae at Newcastle University for their contribution to the design of the study and data acquisition.
A supplemental appendix to this article is available online.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: C.R. Vernazza was funded by a National Institute for Health Research Clinician Scientist Award during this study. The article details independent research, and the views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research, or the Department of Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.