
Abstract
Using longitudinal data from the Midlife in the United States (MIDUS) study, we computed the extent to which the quality of friendships, familial relationships, and intimate partnerships predict one’s risk of dying at any given point in time. The results suggest that experiencing low support or high strain from friends or families can reduce lifespan and that policies to facilitate high-quality relationships among adults could potentially improve well-being and extend longevity.
Decades of research have demonstrated a robust link between social well-being and longevity.1,2 The association between satisfaction with one’s relationships and survival persists even when investigators control for potentially confounding variables such as physical health and habits. Yet little research has focused on how the quality of specific kinds of relationships might affect lifespan.
To address this gap, we examined the association between people’s longevity and the perceived quality of their relationships with friends, intimate partners, and family members (other than spouses), using data from the Midlife in the United States (MIDUS) survey. MIDUS queried a sample of U.S. adults who were 25–74 years of age in 1995 about their well-being and health at multiple points in their lives. 3 Although our methodology did not establish causation, we found that having poor-quality relationships was associated with reduced lifespan, particularly in the case of friendships and, to a lesser degree, familial relationships. We further found that, although a perceived lack of support and high strain were each associated with reduced lifespan, strained relationships were more closely associated with early death than unsupportive relationships were.
Research into how relationships affect longevity is particularly relevant in the United States today because of a long history of lower life expectancy here compared with other developed nations. Given that the 21st-century economy is becoming increasingly dependent on older workers, policymakers must seriously consider investing in strategies that increase constituents’ healthy, productive lifespans. 4 Our findings suggest that policies and programs that promote healthy relationships—particularly friendships—may extend longevity. The United States lags behind other countries in investing in programs to combat loneliness and enhance interpersonal and community connections, but it has made some investments in familial and marital relationships. Our findings imply that policymakers would be wise to supplement those programs with ones designed specifically to support positive friendships.
Past Research on Relationships, Health, & Longevity
Theoretical Work
We grounded our study in a vast body of research greatly inspired by George L. Engel, 1 who proposed in 1977 that people’s relationships with others affect their physical and mental health. We asked how relationship quality might affect health and longevity.
One leading group of theories, known as direct-effects models, posits that strong relationships help by giving meaning to life and providing the self-esteem, motivation, and encouragement to engage in healthy behaviors and that loneliness diminishes self-esteem and increases risky behavior.2,4 Another major class of theories, known as stress-related models, views good social relationships as improving health and longevity by reducing the likelihood of experiencing stressful situations and of perceiving stressful situations as overly distressing. 4 Stress, if persistent, can impair health in part by causing chronic elevations of cortisol and other stress hormones, which can contribute to such ills as inflammation, high blood pressure, and heart disease. In this article, we contribute to the literature on both models by exploring whether one’s self-evaluation of relationship support and strain is associated with longevity. Examples of relationship support can include feeling cared about and understood by others and able to rely on them for material or emotional help. Examples of feeling strain can include perceiving that others make too many demands or are often critical, annoying, or unreliable.
Empirical Findings
The Importance of Social Connections for Health & Longevity
A growing body of literature illustrates the link between social connections, health, and longevity. One notable finding is that loneliness is strongly associated with depression, stress, and poor physical health.5 –7 For example, studies have shown that adults who live alone have a higher probability of reporting poor physical health, 8 and women who are lonely face an elevated risk for coronary heart disease. 9 In contrast, social connectedness is associated with fewer functional limitations in old age. 10
Further, feelings of loneliness and objective social isolation have been linked to an increase in mortality. 11 This association holds when investigators look at specific demographic groups. Among women with breast cancer, for example, those who are socially isolated face a greater risk of dying at any given point in time than do those with strong social networks. 12 Also, African Americans who participate in group or religious activities face a lower mortality risk than socially isolated African Americans do. 13
Links Between Social Support & Health & Longevity
Empirical research typically finds an association between social support and physical health.4,14 –16 For example, higher levels of social support generally correlate with lower risk for cardiovascular events (heart attack, heart failure, or stroke) and mortality.17 –20 Supportive social interactions have also been shown to improve immune, endocrine, and cardiovascular system functioning.4,19
In line with these findings, individuals who have higher levels of nonspousal family support are less likely to develop heart problems later in life. 21 Moreover, in the MIDUS cohort, researchers found that individuals with supportive marriages had better cardiovascular health than those with unsupportive marriages.22,23
In addition to enhanced physical health, social support is associated with improved mental health outcomes. For example, lack of social support is a risk factor for suicidal ideation, 24 whereas higher levels of social support link to greater well-being and less loneliness. 25 This association between social support and improved mental health holds when studies focus on specific relationship types, such as with a spouse, other family members, or friends. For example, greater spousal or familial support in midlife has been related to fewer depressive symptoms and lower levels of loneliness,25,26 although findings on the relationship between support from friends and loneliness are not as distinct.25,27
Social support levels vary across demographic groups. Individuals with higher education and socioeconomic status levels tend to have stronger social support systems, and people with low socioeconomic status tend to be less able to mobilize assistance from support systems during times of need—a problem that may stem, in part, from having too little time to seek assistance while also managing family responsibilities such as arranging for childcare while working. 28 Within socioeconomic groups, social well-being levels also vary across races. Among men who are unemployed or out of the labor force for other reasons, racial minorities report higher well-being than their White counterparts do. This trend may reflect stronger social networks among these communities. 29
With respect to longevity, people who report higher than average levels of emotional- and health-related support expect to live longer than do people who report less support. 30 And they do live longer. 11
Links Between Social Strain & Health
Some researchers have found that negative social interactions have a greater effect on mental health than supportive interactions do, 31 but this finding is not universal.16,32 Nevertheless, higher levels of social strain in any type of relationship have been associated with more intense loneliness. 25 Strained social interactions have also been linked to increased inflammation and chronic pain.33,34 Among married individuals, increases in marital strain have been associated with decreases in cardiovascular health. 22 And, family strain has been linked to chronic pain. 34 Researchers are investigating this link to pain. So far, the data suggest that high biological reactivity to negative emotions and an accumulation of biological consequences from chronic stress (allostatic load) may contribute to such pain. An evolving body of research is focusing on the causal channels driving this relationship. Current findings suggest that high reactivity to negative emotions and allostatic load may both contribute to emotional strain that then manifests as physical pain.35,36
Differences Across Relationship Types
Few researchers have investigated the association between the quality of specific relationships and health or longevity. Beyond those previously mentioned, a handful of others warrant mention.
Using the same MIDUS dataset we employed in the study discussed in this article, one group 37 examined correlations between family or intimate partner strain and support and people’s health over time. They found that variations in the quality of the relationship with family correlated more strongly with health as people aged than did variations in the quality of the relationship with an intimate partner. 37
Also using the MIDUS data, a different team 38 studied the connection between the quality of romantic relationships and physical health using systemic inflammation as their measure of physical health. They found that the quality of intimate partnerships was not a statistically significant predictor of systemic inflammation. In other work, investigators examined the link between strained relationships and allostatic load. 39 Findings showed that the accumulated physiological consequences of the body’s response to chronic emotional stress increased with negative ratings of family interactions but not with negative ratings of intimate partner interactions, again highlighting the relative importance of the quality of family relationships over the quality of intimate partnerships. 39
Few studies have considered the role of friendships in health and longevity. In two notable exceptions, researchers used MIDUS data to analyze the relationships between support or strain at the family, friend, and intimate partner level and health 16 and longevity. 40 In work focusing on gender differences and longevity, for instance, investigators found that social support from partners, family, and friends reduced mortality risk for both men and women. In addition, social strain (particularly from friends and spouses) increased mortality risk more significantly for women, who also appear to benefit more than men do from the buffering that supportive relationships provide against negative social interactions. Our study expands on the longevity research by incorporating five additional years of mortality data and a more robust set of controls.
Hypothesis & Methods
On the basis of the research summarized above, we hypothesized that peoples’ perceptions of the quality of their relationships would correlate with their lifespan if we held constant other social and demographic factors that influence health. In particular, we predicted that people who had satisfying relationships with friends, families, or intimate partners would live longer than those who did not.
As noted earlier, we drew our data from the long-running MIDUS survey. 3 MIDUS researchers initially interviewed participants about their health and well-being in 1995 or 1996. They then had participants fill out an extensive self-administered questionnaire addressing these issues and repeated the questionnaire in 2004–2006 and 2013–2014. Deaths were recorded through 2020.41,42
We used a national representative cohort and included only participants who had at least answered the first questionnaire. Participants also had to have either completed a second- or third-wave survey or passed away. We did not use data from the second and third surveys in our analyses, but the requirement for completing one of those surveys ensured that our sample was representative of the MIDUS population and that response rates were consistent in at least two survey rounds.
The resulting sample included 2,256 individuals. Of them, 928 had died by the end of 2020. Six-hundred-seventy survey respondents reported not having an intimate partner relationship. Thus, when we examined the link between relationships with partners and longevity, we had a population size of 1,586. See Table S1 in the Supplemental Material for participant demographic details.
To assess the perceived quality of relationships, we used the MIDUS measures of support, strain, and solidarity. Solidarity is an overall measure of the combined positive and negative feelings one holds about a relationship 43 and is generated by averaging the measures of support and strain after scaling them so that higher scores indicate more positive perceptions (that is, strong support and low strain). All three concepts are much studied by psychologists. Evaluating solidarity in addition to support and strain allowed us to evaluate whether high support might offset high strain, or vice versa. Usually in psychological research, support and strain are negatively correlated: Low support correlates with high strain, and high support correlates with low strain. 16 We speak of support, strain, and solidarity as “predictor” variables because their levels are potentially predictive of longevity, our outcome variable.
In the MIDUS surveys, respondents indicated their feelings of support or strain by answering four to six relevant questions on a 4-point scale; these answers were then averaged to generate a single support or strain score.16,21,44 In our study, we used these single averaged scores as well. For instance, to obtain a score for perceived strain in familial relationships, the MIDUS investigators averaged participants ratings of how often family members “make too many demands on you,” “criticize you,” “let you down when you are counting on them,” and “get on your nerves.” For support, they averaged ratings of how much “do they really care about you” and “understand the way you feel about things” and how much can you “rely on them for help if you have a serious problem” and “open up to them if you need to talk about your worries.”
We assessed the association between relationship quality and longevity by applying a Cox proportional hazards survival regression analysis. Cox regressions predict the likelihood that an event of interest, such as death, will occur earlier when one or more factors (such as relationship support or strain) are present. The analysis yielded a hazard ratio (HR): one group’s risk of dying at any given time relative to that of another group. An HR greater than 1 indicates that a predictor variable is associated with an elevated relative risk of dying, whereas a ratio smaller than 1 indicates a reduced risk.
In addition to examining the association between support, strain, or solidarity and longevity, we also analyzed whether other potential predictors of longevity, such as age or income, altered the associations found in our main analyses. For instance, low income might itself increase the risk of death, so we wanted to take that effect into account. The factors, or covariates, we examined were selected through an approach known as the lasso technique and included respondent’s age during the first wave of the MIDUS survey, race (White or non-White), gender (male or female), education level, self-evaluated mental health, self-evaluated physical health, income, and assessment of whether they had enough money for daily expenses. In some analyses, we controlled for all the covariates selected by the lasso technique for a given relationship type; in other analyses, or specifications, we used other mixtures.
We also ran simplified regression analyses that confirmed the validity of the Cox regression results. See the Supplemental Material for more detail on methods and statistical analyses.
Results
Overall, the perceived quality of friendships correlated strongly with longevity. The association between the quality of familial relationships and longevity was weaker but still statistically significant. Interestingly, however, the quality of intimate partnerships was not associated with longevity.
Table 1 shows the data from our primary analyses relating to support, indicating a statistically significant HR of 0.82. Because a ratio less than 1 indicates a reduced risk of dying, this result shows that more supportive friendships were associated with longer lifespans.
Cox proportional hazards regression results for social support
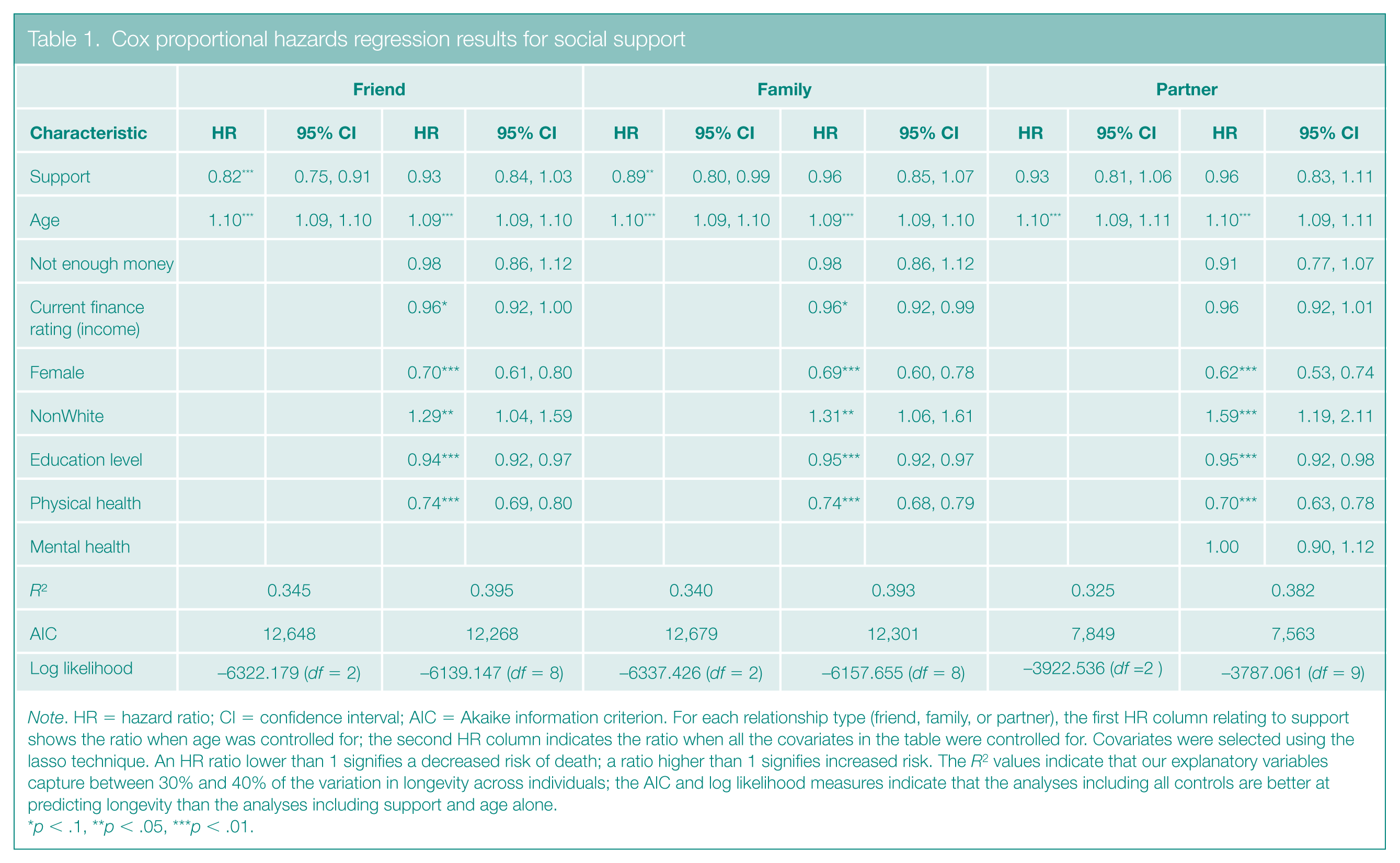
Note. HR = hazard ratio; CI = confidence interval; AIC = Akaike information criterion. For each relationship type (friend, family, or partner), the first HR column relating to support shows the ratio when age was controlled for; the second HR column indicates the ratio when all the covariates in the table were controlled for. Covariates were selected using the lasso technique. An HR ratio lower than 1 signifies a decreased risk of death; a ratio higher than 1 signifies increased risk. The R2 values indicate that our explanatory variables capture between 30% and 40% of the variation in longevity across individuals; the AIC and log likelihood measures indicate that the analyses including all controls are better at predicting longevity than the analyses including support and age alone.
p < .1, **p < .05, ***p < .01.
Regarding how to interpret the HRs: In Tables 1–3, the first HR given for a relationship-quality measure (support, strain, or solidarity) under the Friend, Family, or Partner heading indicates the ratio calculated when relationship quality is considered without controlling for the full set of covariates selected by the lasso technique but still controlling for age (because of age’s potentially powerful confounding effect on one’s likelihood of dying). The second HR column shows the ratio when we controlled for all covariates selected by the lasso technique for each relationship type. In each case, the HR indicates the relative risk of dying when the variable measure increased by one unit. Imagine, for example, that every respondent could select a number from 1 to 4 to indicate the level of support they felt in a relationship sphere. For every one-unit increase (say, from 1 to 2 or from 3 to 4) respondents would be X% less likely to die at a given point in time.
In Table 1, the HR of 0.82 for friend support therefore means that people who indicated a support level one unit higher than that of another group faced 82% of the risk faced by the group reporting the lower support level. In other words, the higher scorers had an 18% decrease (100% minus 82%) in risk. If the HR were smaller, say 0.62, the decrease in risk between the groups would be even greater (38%).
According to additional analyses not shown in Table 1, the positive association between friend support and longevity persisted when we controlled for education level, race, income, physical health, and, in the case of intimate partner relationships, mental health. See Tables S10 and S14 in the Supplemental Material.
When we controlled for gender in those additional analyses, however, the association between friend support and lifespan was no longer statistically significant, indicating that gender was associated both with longevity and friend support. In the MIDUS sample, women reported higher levels of friend support than men did (see Figure S4 in the Supplemental Material), although it is unclear whether women truly have more supportive friendships, appreciate support from friends more, or have more friendships than men. The nature of the association between gender, friend support, and longevity requires further study by policymakers interested in promoting supportive friendships for adults.
Supportive familial relationships were also associated with longer lifespans (HR = 0.89), although this relationship was less robust than the association between supportive friendships and longevity. We did not find a statistically significant association between intimate partner support and longer life.
As Table 2 shows, higher strain in friendships was associated with shorter lifespan (HR = 1.24), and this pattern held when all the potential influences identified by the lasso technique were controlled for (HR = 1.18). Strained familial relationships were also associated with shorter lifespan (HR = 1.19). Stressful intimate partner relationships were not associated with shorter lifespan.
Cox proportional hazards regression results for social strain
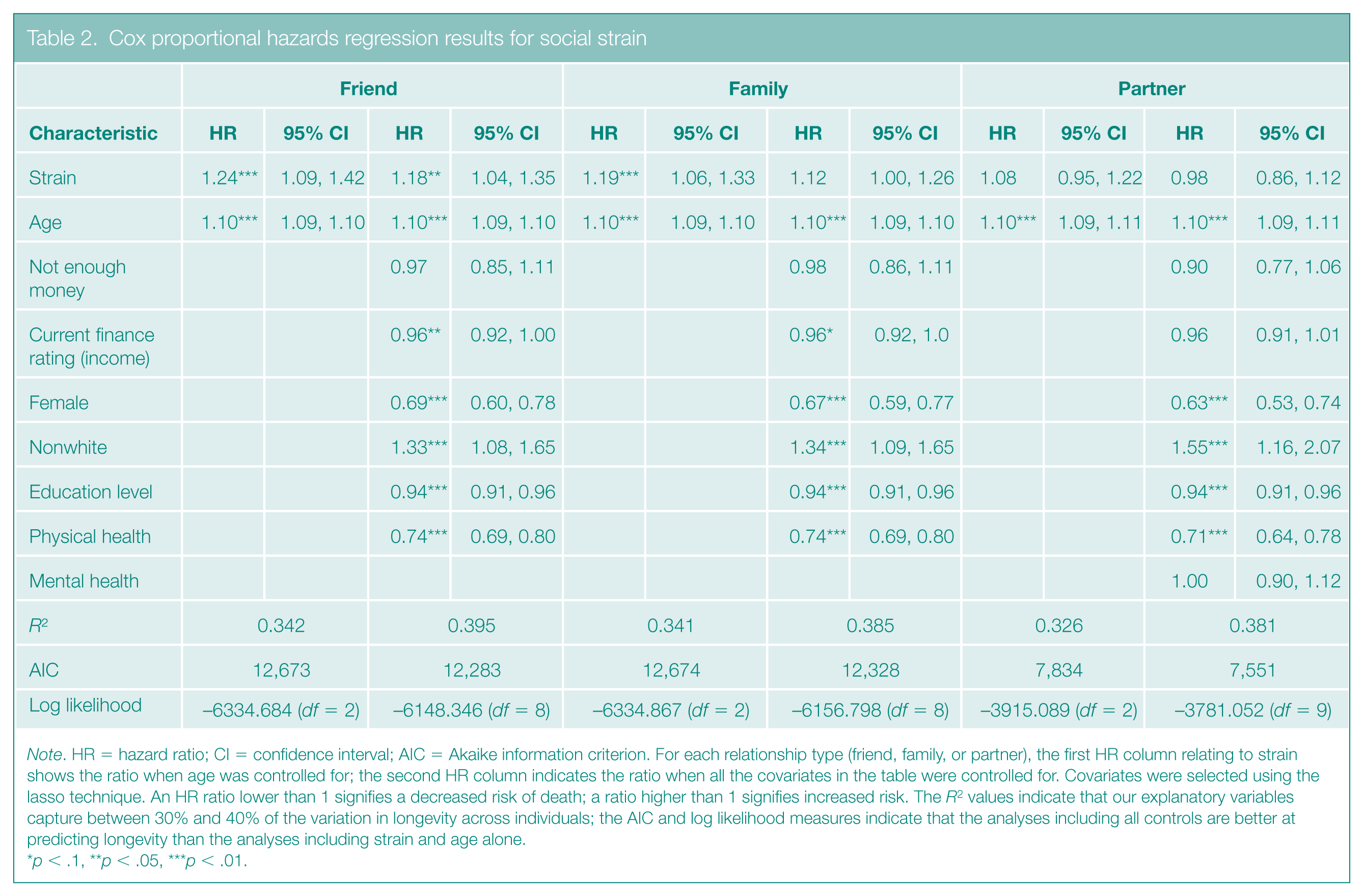
Note. HR = hazard ratio; CI = confidence interval; AIC = Akaike information criterion. For each relationship type (friend, family, or partner), the first HR column relating to strain shows the ratio when age was controlled for; the second HR column indicates the ratio when all the covariates in the table were controlled for. Covariates were selected using the lasso technique. An HR ratio lower than 1 signifies a decreased risk of death; a ratio higher than 1 signifies increased risk. The R2 values indicate that our explanatory variables capture between 30% and 40% of the variation in longevity across individuals; the AIC and log likelihood measures indicate that the analyses including all controls are better at predicting longevity than the analyses including strain and age alone.
p < .1, **p < .05, ***p < .01.
Recall that measures of solidarity reflect the combination of stress and strain in relationships. A person who reported high support and low strain, for instance, would end up with a high solidarity score. As is shown in Table 3, the HR for the variable friendship solidarity was 0.82 when all the covariates were controlled for, indicating that a higher friendship solidarity score was associated with a decreased likelihood of dying sooner than people who report lower friendship solidarity. When all covariates are controlled for, the effect of solidarity was greater than the effect of support or strain alone, indicating that the combining of high support and low strain or low support and high strain may have synergistic effects.
Cox proportional hazards regression results for social solidarity
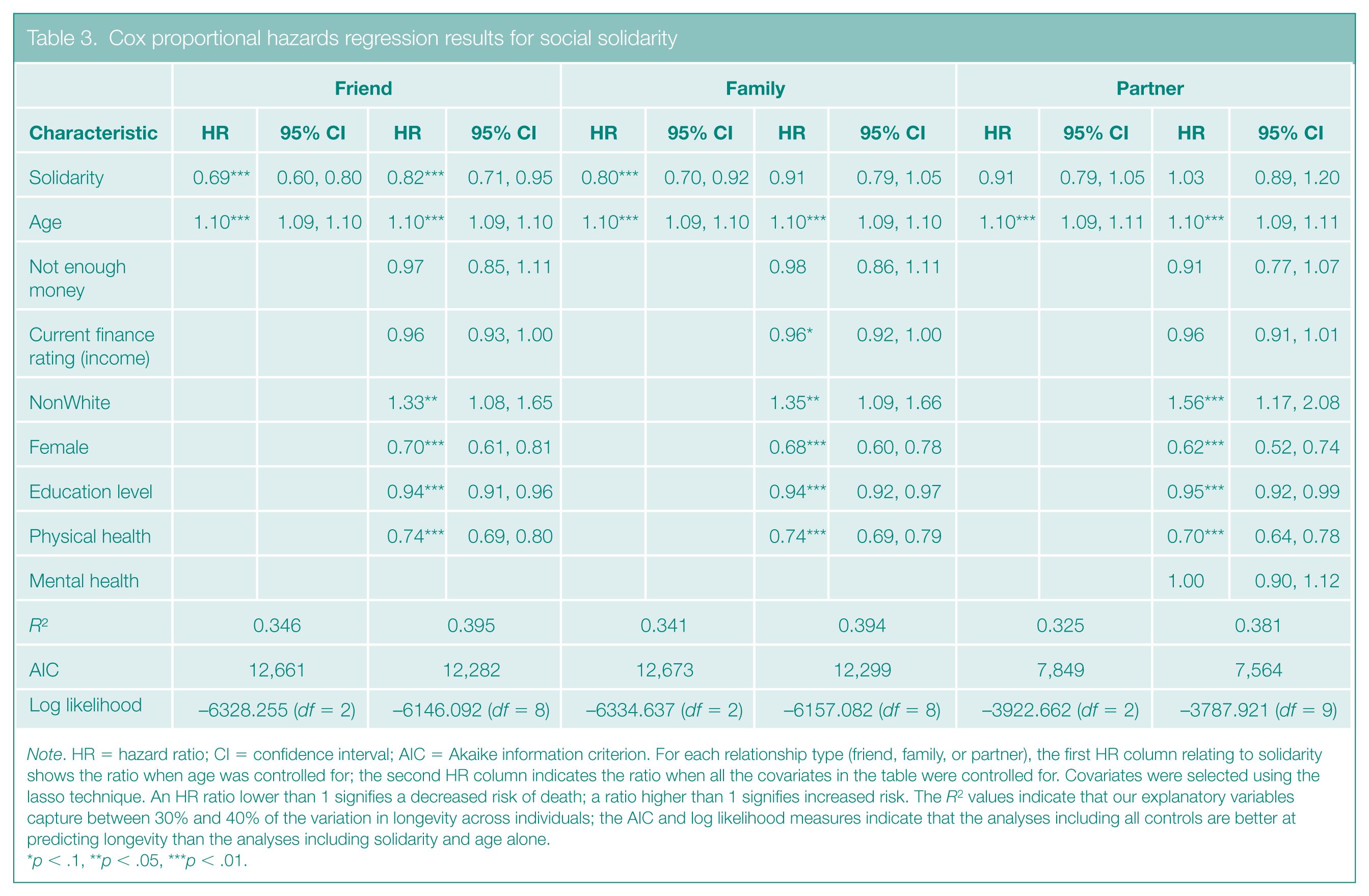
Note. HR = hazard ratio; CI = confidence interval; AIC = Akaike information criterion. For each relationship type (friend, family, or partner), the first HR column relating to solidarity shows the ratio when age was controlled for; the second HR column indicates the ratio when all the covariates in the table were controlled for. Covariates were selected using the lasso technique. An HR ratio lower than 1 signifies a decreased risk of death; a ratio higher than 1 signifies increased risk. The R2 values indicate that our explanatory variables capture between 30% and 40% of the variation in longevity across individuals; the AIC and log likelihood measures indicate that the analyses including all controls are better at predicting longevity than the analyses including solidarity and age alone.
p < .1, **p < .05, ***p < .01.
A word about our finding of no association between longevity and support, strain, or solidarity in relationships with intimate partners: It is possible that another influence on longevity is so strong that it renders insignificant any effects of relationship quality. Specifically, people who have an intimate partner generally live longer than those who do not. The buffering effect of having a partner at all may counteract the ill effects of having a poor-quality partner. In addition, because not all participants had intimate partners, we had fewer participants in this group than in our analyses of friend and family relations; the smaller size makes the conclusion less certain.
Although our primary analysis considered the quality of different relationship types in isolation, in reality, many relationships are experienced simultaneously and to differing extents. In Table 4, we included all six relationship-quality dimensions (family support, family strain, friend support, friend strain, partner support, and partner strain) in the Cox regression analysis at once. The only predictor variable that had a statistically significant influence on longevity was friend support. That is, when we controlled for one’s perceived level of support and strain from family and intimate partners, only supportive friendships were strongly associated with longer lifespans, and they reduced the risk of death by about 20% (HR = 0.80). It is likely that relationships with one group of people can affect the health and longevity effects of relationships with another group. Having supportive friendships might reduce the negative effects of strained relationships in family members or an intimate partner.
Cox proportional hazards regression results for friend versus family versus partner
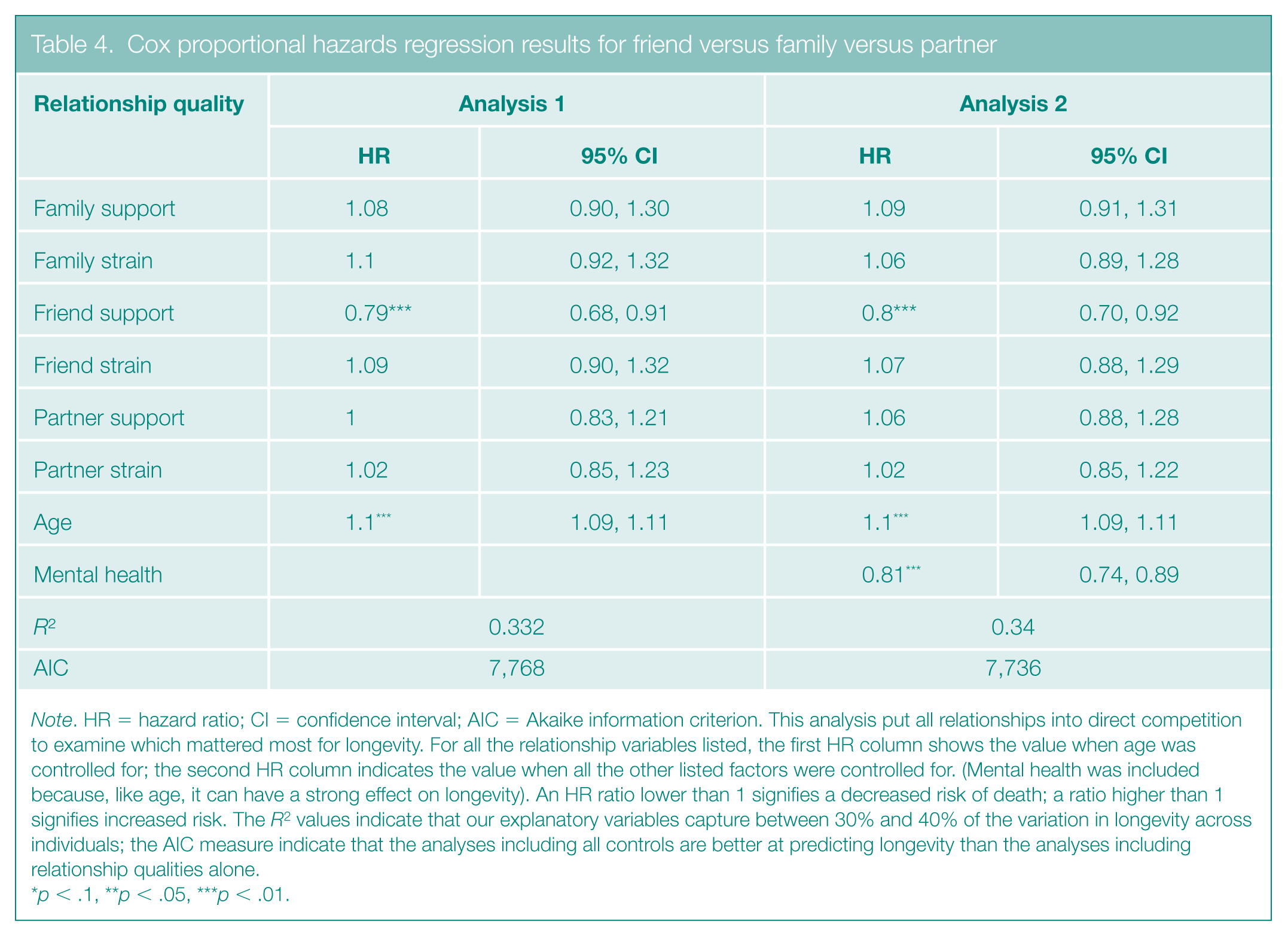
Note. HR = hazard ratio; CI = confidence interval; AIC = Akaike information criterion. This analysis put all relationships into direct competition to examine which mattered most for longevity. For all the relationship variables listed, the first HR column shows the value when age was controlled for; the second HR column indicates the value when all the other listed factors were controlled for. (Mental health was included because, like age, it can have a strong effect on longevity). An HR ratio lower than 1 signifies a decreased risk of death; a ratio higher than 1 signifies increased risk. The R2 values indicate that our explanatory variables capture between 30% and 40% of the variation in longevity across individuals; the AIC measure indicate that the analyses including all controls are better at predicting longevity than the analyses including relationship qualities alone.
p < .1, **p < .05, ***p < .01.
See Figures S5 and S6 in the Supplemental Material for survival curves relating to support and strain in friend, familial, and intimate partner relationships.
Discussion & Policy Implications
Scientific Implications
Our analysis of MIDUS participants found that perceived support and strain from friends and family, although not from intimate partners, was associated with longevity. Participants with the most strained relationships faced the shortest lifespans. The quality of friendships was more strongly related to longevity than was the quality of relationships with family members. People with poor-quality friendships faced a higher risk of dying than those who did not have poor-quality friendships. In addition, supportive friendships appeared to be protective when we controlled for variations in the quality of other relationship types. That is, supportive friendships were strongly associated with longer lifespans even in the presence of other relationships that were strained.
The data raise the possibility that friendship offers something unique. Although it might be obvious that supportive friendships are beneficial when other relationships are strained, our results imply that even when one has a loving spouse and supportive family, having good friends still adds an extra layer of protection for health and longevity. What is more, the protective effect of friendship may work through pathways that go beyond improving psychological well-being; we think so because we found, as Table 4 shows, a statistically significant effect for friend support even when we controlled for all other relationships and mental health at once.
The voluntary nature of friendships—in contrast to familial relationships and romantic partnerships (in which complex emotional and often legal commitments can be difficult to break)—may in part explain why friend support demonstrated unique protective effects. A person can choose friends who will provide support while the individual disengages from others who generate stress.45,46
Our data analyses are subject to limitations. Confounding factors such as mental illness, employment status, and unhealthy habits (such as smoking and alcohol consumption) can affect social relationships, physical health, and longevity. Future research should further explore how these factors relate to support and strain from relationships, in particular, friendships. In addition, suffering from depression and other factors we did not consider, such as anxiety, could conceivably color perceptions across all relationship types, which in theory could have somewhat impaired our efforts to distinguish the association of these relationships with longevity. We explored this possibility, however, and found little or no correlation in support or strain across friend family, and partner relationships.
Apart from our main analysis, we identified certain groups more likely to experience poor-quality relationships than others and who may thus face a higher risk of dying. Notably, individuals with poor finances were more likely to have unsupportive and strained relationships than people with good finances. Our results suggest that poor-quality relationships in low-income individuals may help to account for a robust body of research linking low socioeconomic status with mortality. For certain low-income groups in the United States, for instance, a trend of decreasing life spans is often attributed to deaths of despair (suicides, alcohol-related deaths, and overdoses).47 –49 It is conceivable that unhappy relationships could be contributing to this despair. Educational attainment, which is highly correlated with income level, is also known to be an important determinant of longevity, and we, too, found this effect. Anne Case and August Deaton recently found an eight-year gap in the life expectancy of those with and without four-year college degrees, which they attributed to differences in the prevalence of deaths of despair as well as heart disease and cancer—diseases that are exacerbated and/or heightened by stress. 50 Our findings suggest that policymakers might improve the outcomes for high-risk groups by fostering supportive friendships—for example, by investing in community spaces in low-income communities as well as providing services that support low-income individuals’ efforts to manage time and financial constraints, which make socialization much more difficult.
Policy Considerations
With respect to broader policy implications of our study, the finding that supportive friendships and familial relationships in the MIDUS cohort were associated with longer life and that strained friendships and familial relationships were associated with shorter life suggests that policymakers interested in promoting long and healthy lives should direct attention to increasing adults’ perceived social support and decreasing perceived social strain. In locales where mental health care is limited, mobilizing community support could be an effective way to decrease disparities in longevity.
Examples to emulate abound. For instance, many countries have made community well-being a policy priority. The United Kingdom’s Loneliness Strategy (which grew out of the Cox Commission on Loneliness and is the first of its kind in the world) and the Campaign to End Loneliness provide practical examples of strategies to alleviate loneliness and build stronger social relationships.51,52 These initiatives deliver a range of interventions targeted at individuals and communities, including providing resources for therapy, training in developing emotional and social skills, and social activities in community-based settings. These are generally low-cost programs that have been shown to have positive effects.
In Brazil, integrative community therapy (ICT) has become a cornerstone of mental health services and is gaining traction in communities across the globe. Developed by Adalberto de Paula Barreto, this therapeutic approach assumes people will heal most successfully when treatment includes interacting locally in community spaces with others who face similar problems. 53 Studies on ICT have found generally positive effects and provided evidence suggesting that engaging in ICT may help individuals resolve issues without receiving formal mental health interventions.53,54
As a nation, the United States, too, has given attention to the importance of community. The U.S. Surgeon General released a 2023 report on loneliness noting that social isolation is significantly associated with early mortality. 55 In addition, the report laid out a national strategy to advance social connection, which included several new steps that governmental and nongovernmental organizations could take to address the loneliness epidemic. In particular, it called for investments in social infrastructure to design environments that foster community and social connection. 55
In the United States, community well-being initiatives have been driven by nonprofit organizations operating on a local scale. Efforts such as The Confess Project take mental health services to community spaces.56,57 A related example is the Visible Hands Collaborative, based in Pittsburgh, Pennsylvania, that develops peer support for community participants in need of mental health services. 58 These programs provide models for delivering mental health and well-being services to underresourced communities while leveraging the positive effects of social relationships on well-being. Although these efforts provide essential services and support, they are, however, localized and underresourced themselves.
At the federal level, the U.S. government makes significant investments in supporting marriage and two-parent households. For example, the Healthy Marriage and Responsible Fatherhood program disburses $150 million annually in grants aimed at strengthening families. But few comparable programs exist that strengthen nonfamilial relationships, as the Surgeon General’s report on loneliness made clear.
Our finding that friendship is significantly associated with longevity suggests that the United States should consider supplementing existing investments in familial and marital relationships with programs designed to promote positive friendships. Policies supporting adult friendship formation represent an underutilized health promotion avenue.
We end with additional advice particularly relevant to the United States. Recent research shows that loneliness is increasing and is more prevalent in the United States than in Europe. 59 It is critical that the United States catch up with other developed nations by making community well-being a policy priority. Innovative approaches such as ICT are promising for addressing community well-being, but their efficacy and impact are not yet well understood. Beyond investing in social support and community well-being programs, policymakers should fund empirical research on their impact. These programs provide a model for leveraging the positive well-being effects of social relationships to deliver mental health services to underresourced communities. Their relatively low cost and broad scope may make them an effective approach for improving well-being and extending lifespans.
Supplemental Material
sj-docx-1-bsx-10.1177_23794607251388787 – Supplemental material for Relationship quality & longevity: Do support & strain from friends, families, & intimate partners predict lifespan?
Supplemental material, sj-docx-1-bsx-10.1177_23794607251388787 for Relationship quality & longevity: Do support & strain from friends, families, & intimate partners predict lifespan? by Kasey Vangelov, Emily Dobson and Carol Graham in Behavioral Science & Policy
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.