
Abstract
Many pregnant women do not seek or receive maternal health care, endangering their health and that of their unborn babies. This problem is especially acute in low- and lower-middle-income nations, where rates of maternal mortality and morbidity are high. Incentives and digitally delivered communication can encourage women to use maternal services, thereby improving maternal health outcomes. However, behavioral evidence to support the most effective combination of components for these interventions is limited. We tested the impact of a nondigital incentivized intervention against a digital nonincentivized behavior change communication intervention (interactive voice messaging) on the uptake of antenatal services and the use of a skilled birth attendant (a midwife, nurse, or doctor who is trained to deliver babies) in parts of Nigeria, a lower-middle-income country. We randomized 845 participants to receive one of the two interventions or no intervention. We found that the nondigital incentivized intervention increased the probability that women would use antenatal care and a skilled birth attendant significantly more than the digital messaging.
Primary health care is the backbone of a productive economy 1 and crucial for providing inclusive and cost-effective medical care. Primary health care centers deliver a range of basic services, including maternal care, which encompasses antenatal care, skilled delivery, and postnatal care. These services are critical for safeguarding women’s lives during and after pregnancy and ensuring newborn survival. 2 Yet in many countries, access to and delivery of primary health care is inconsistent, leading to high rates of infant and maternal death and disability.
The authors of this article include officials who work for government organizations that deliver primary health care services in Nigeria, private sector researchers, and behavioral scientists. Uptake of maternal health care services is low in Nigeria. In the last quarter of 2021, the Nigerian National Primary Health Care Development Agency reported that only approximately 50% of pregnant women across Nigeria had at least four antenatal care (that is, pregnancy care) visits (Gombe State 54%, Niger State 37%), and roughly 34% of mothers had used a skilled birth attendant to deliver their baby (Gombe State 45%, Niger State 33%). 3
In large part because of this care gap, Nigeria has one of the highest maternal and child mortality rates worldwide, accounting for 12% of global maternal and neonatal deaths and stillbirths. 4 Preventing these deaths would therefore make a sizable impact on infant and maternal death rates globally. Because of these statistics, we believe Nigeria is an appropriate testing ground for determining how best to increase demand for primary health care in nations with high maternal and child mortality rates in sub-Saharan Africa.
Preventing these deaths is largely a matter of improving access to and uptake of available maternal care.5,6 Doing so requires overcoming two kinds of challenges. In one, infrastructure barriers and lack of resources mean long distances to health facilities, unaffordable service costs, poor-quality care, and unreliable electricity and water supplies.7–9 In addition, behavioral and psychosocial factors depress the use of maternal care services. These factors include confidence among women that they will have good maternal outcomes without regular maternal health checks (a form of optimism bias), often because they have friends or family members who gave birth successfully at home, 10 and a preference for traditional birth attendants (community members who assist with childbirth at home).11–13
In this article, we report on a pilot study we conducted. It was designed to supply the Nigerian National Primary Health Care Development Agency with preliminary insights on the best ways to overcome these barriers and motivate women to seek maternal health care as preparation for a larger, longer-term study. We compared the effects of two interventions on the uptake of antenatal care and intention to use a skilled birth attendant at a public health facility. One intervention included an incentive, as incentives are commonly used in Africa to promote behavior change, but required no technology to implement. The other required mobile phones, a potentially more scalable solution, but did not involve an incentive.
Methods
Location
We conducted our study in two northern states in Nigeria (Gombe and Niger) because of the prevalence of poor maternal outcomes in these regions. 14 We aimed to provide evidence for the best way to allocate limited public health resources there and in similar locales. In each of these states, we homed in on two local government areas—Yamaltu/Deba and Dukku in Gombe State, and Katcha and Chanchaga in Niger State—that local health care authorities suggested were most in need of ways to connect women to maternal health care.
Participant Demographics
In Gombe State, 62% of participants resided in Dukku, a predominantly rural local governmental area, while 38% were from the more urban Yamaltu/Deba area. In Niger State, 76% of the sample came from urban Chachanga, with 24% from the Katcha area, which is a mixture of rural and peri-urban (urban transition zone) landscapes. Most participants in both states had attained secondary education. Gombe State had a higher percentage (45%) of participants with no formal education compared to Niger State (16%). Additionally, most of the sample reported low income levels, with 79% in Gombe State and 74% in Niger State indicating a monthly income estimated between 0 and 50,000 Naira (approximately $0–$70 as at the time of this study). See the Supplemental Material for a detailed demographic breakdown.
Participant Recruitment
Community health volunteers recruited pregnant women 18 years or older and their spouses who lived in the selected study locations and who had functional and reachable mobile devices. Additional details on the enrollment process can be found in the Supplemental Material.
Basic Study Design
Our study was a field experiment consisting of two intervention arms and one control group. Pregnant women were randomly assigned to one of the three groups. As explained below, we tested two variables per treatment: incentive versus no incentive and digital versus nondigital alternatives.
The digital, nonincentivized intervention consisted of a motivational audio message voiced by respected regional traditional leaders. 15 The message encouraged women to visit a health care center at least eight times during their pregnancy to avoid problems with the pregnancy and to deliver at a health care center so that the baby is born safely. It provided information about practical matters such as the cost and location of these important health care services and was framed in accordance with the community’s social norms.16,17 It also encouraged expectant mothers to seek maternal care by emphasizing the exemplary practices of other local women (see Figure 1).
Voice message intervention
The voice messages were delivered to pregnant women via their personal phone or their spouse’s phone. Spouses were included because we learned that some women in the region do not have their own phone for social or economic reasons and often shared a phone with their spouse.
The audio messages were sent in the evenings near the beginning and near the end of each week for four weeks. When a pregnant woman or her spouse answered the call, they were instructed to press a number to receive the message. At the end of the automated message, the listener could also press a number to repeat the message. In addition to these calls, the women and their spouses received periodic SMS reminders of the location of the nearest health care center.
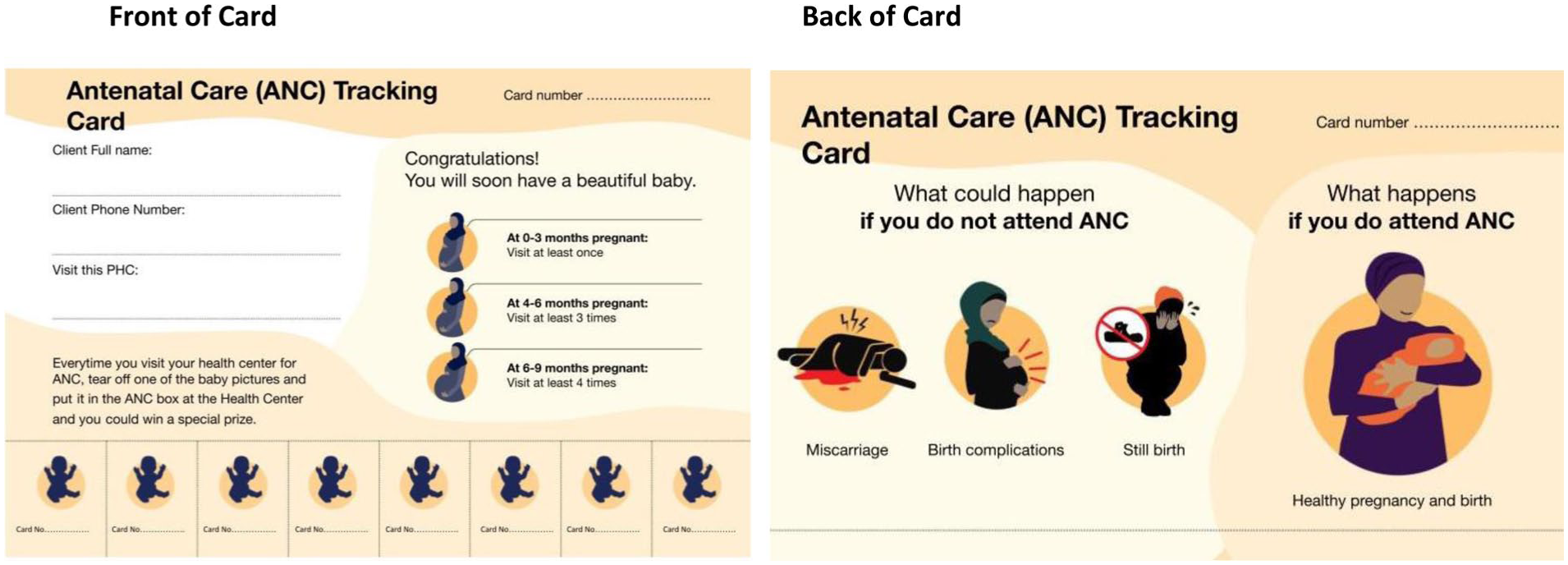
The incentivized, nondigital intervention featured a laminated paper card designed to motivate women to seek care.18,19 The front of the card reminded women about the recommended number of maternal care visits. 8 The back of the card displayed infographics highlighting the consequences of neglecting maternal care. Each card included eight detachable tickets, one for each recommended antenatal care visit (see Figure 2).
Card intervention
After each visit, a woman could deposit a ticket in designated collection boxes at the health clinic. These tickets were entered into a raffle for a chance to win prizes such as diapers, bottles, and clothing. A gamified incentive like this is more cost effective than providing cash to every compliant individual because it rewards only a subset of the women who engage with the health care system. We chose maternal supplies such as nappies and bottles instead of digital payments because earlier stakeholder interviews revealed a preference for these items, and digital payments through mobile apps were not commonplace in the study locations. 20
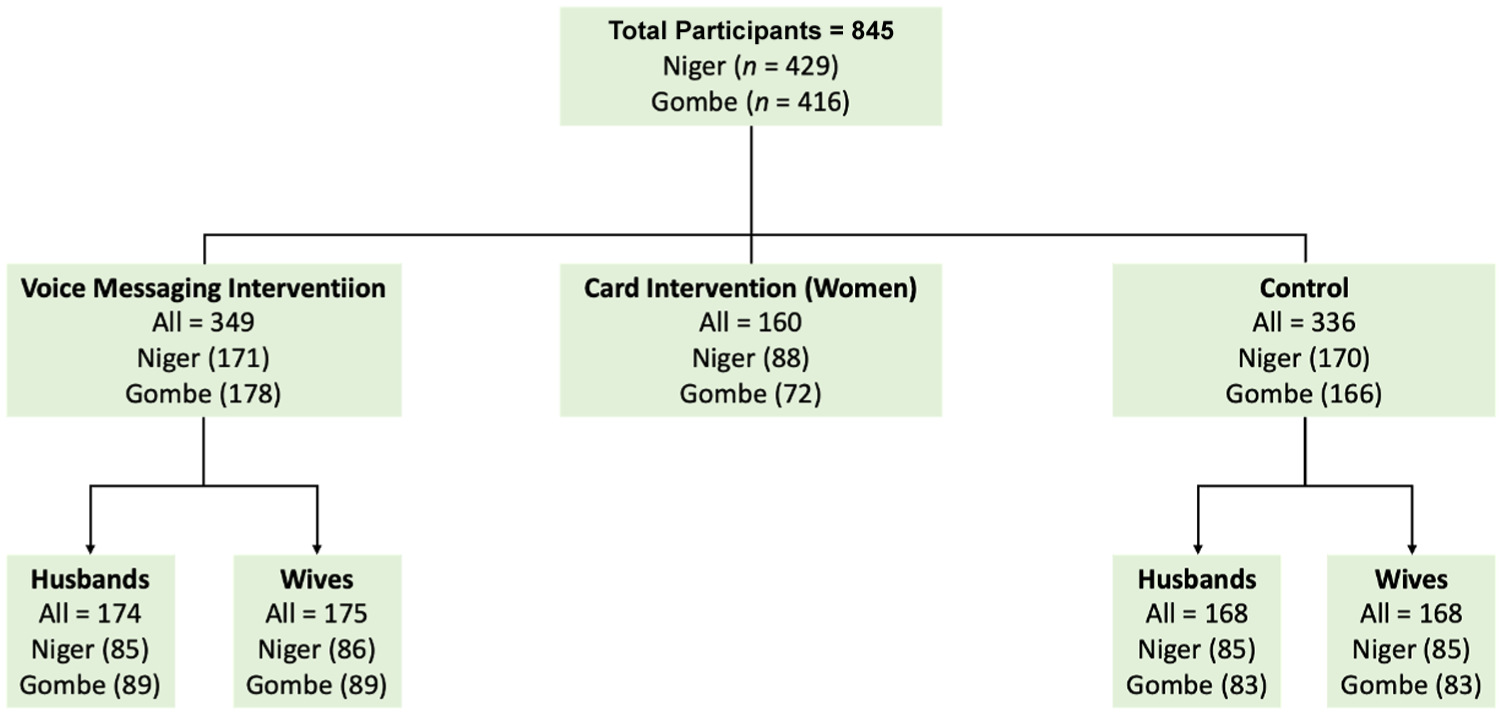
Cards were available in both English and Hausa, the predominant local language. A control group of pregnant women and their spouses were followed for the four-week study but did not receive any intervention. (See Figure 3 for a breakdown of the number of participants across arms of the study.)
Distribution of participants in the arms of the study
Study Design Rationale
Policymakers in sub-Saharan Africa and international agencies have long sought to boost health care use by balancing the advantages of mobile health solutions (scale and cost) 21 with those of incentives (rapid results). 22 Previously, policymakers23,24 have favored incentive-based interventions, which mostly take the form of cash25,26 or access to free transportation to medical facilities, 25 free maternal care, or free health insurance.27–29 Despite the inconsistent and fragmented nature of primary health funding, 30 in-kind and cash-based incentives are more practical than digital payments in sub-Saharan Africa, 31 particularly for low-income households that struggle to afford health care. Digital financial literacy—the awareness and usage of mobile banking or mobile money service providers—is far from universal among people from the study locations and neighboring regions.32,33
Incentives generally do increase desired health-related behaviors, especially when engagement in a desired behavior is very low.21,24,34 For instance, incentives have been shown to improve attendance at antenatal care visits and increase the number of women who return to a health facility after birth for postpartum care. 35 However, they can present a considerable cost burden for lower-middle-income countries such as Nigeria 30 if every individual who meets a specified goal is eligible to receive a reward.
Non-incentive-based maternal care interventions in rural and peri-urban settings in Nigeria have traditionally consisted of interpersonal interactions such as one-on-one or group-based counseling with community health workers, community volunteers, or local influencers such as village heads 36 who encourage women to use primary health care. These practices work but are notoriously hard to scale due to the cost and shortage of trained human counselors.
Mobile-based health solutions provide a scalable alternative, enabling health care communications to reach many women and households. A growing body of research supports delivering voice messages to mobile phones as a way of promoting healthy behaviors. In lower-middle-income countries, these messages usually consist of automated reminders of health care appointments and communications with health support workers or personnel.37–40 This strategy has increased women’s attendance at these appointments in Nigeria, Ghana, and Rwanda. 37
The combined effects of mobile health interventions and incentives 41 seem to be even greater, but little to no experimental research compares nondigital incentive-based approaches directly against mobile health interventions in a lower-middle-income country such as Nigeria. Such research is needed to determine the most effective combination of components.
We aimed to supply evidence for the relative merits of a nonincentivized voice-based mobile health intervention, on the one hand, and an analog information card coupled with a gamified incentive on the other. Emerging evidence supports using digital-based interventions 42 and gamified incentives as a way of promoting positive health outcomes, mostly through mobile health apps. 43 Although our raffle-based payout system is neither digital nor as advanced as those found in the current literature, it may be more cost effective and accessible to the population we are intending to reach.
Data Collection
To assess the results of our interventions, we measured antenatal maternal service uptake at 137 primary health care centers: 66 in Gombe and 71 in Niger. These health care centers all met the minimum standards of infrastructure, staffing, equipment, supplies, and service quality, as defined by Nigeria’s National Primary Health Care Development Agency. 44 Health care staff at participating centers were trained to record the names and numbers of women who came in for antenatal care or registered for skilled birth attendant delivery services at the center during the four-week study period. We collected these records weekly.
Outcome Variables
The number of expectant mothers who attended at least one antenatal care visit at one of the designated health care centers was the study’s primary outcome measure. The secondary outcome measure was the number of women who registered to use a skilled birth attendant during delivery.
Statistical Analysis
We used a linear probability model to estimate the effect of each intervention relative to a control condition. The model estimated the probability that a woman receiving the intervention visited a health center for antenatal care, registered for skilled delivery, or completed all recommended antenatal care visits, relative to no intervention. Results are presented as percentage point differences. They were calculated by comparing the share of women in the intervention group achieving one of the outcomes to that in the control group. The model adjusted for baseline variables such as age and education that may influence health services usage.
Results
Descriptive Results
Of the 503 women in our sample, 183 (36%) visited a primary health care center at least once during the study period. Among these visits, 63% were made by women who received the tracking card involving incentives, 23% by women who received a voice recording, and 14% by women in the control group, indicating that the tracking card was the most effective intervention.
Effects of the Interventions in Niger State
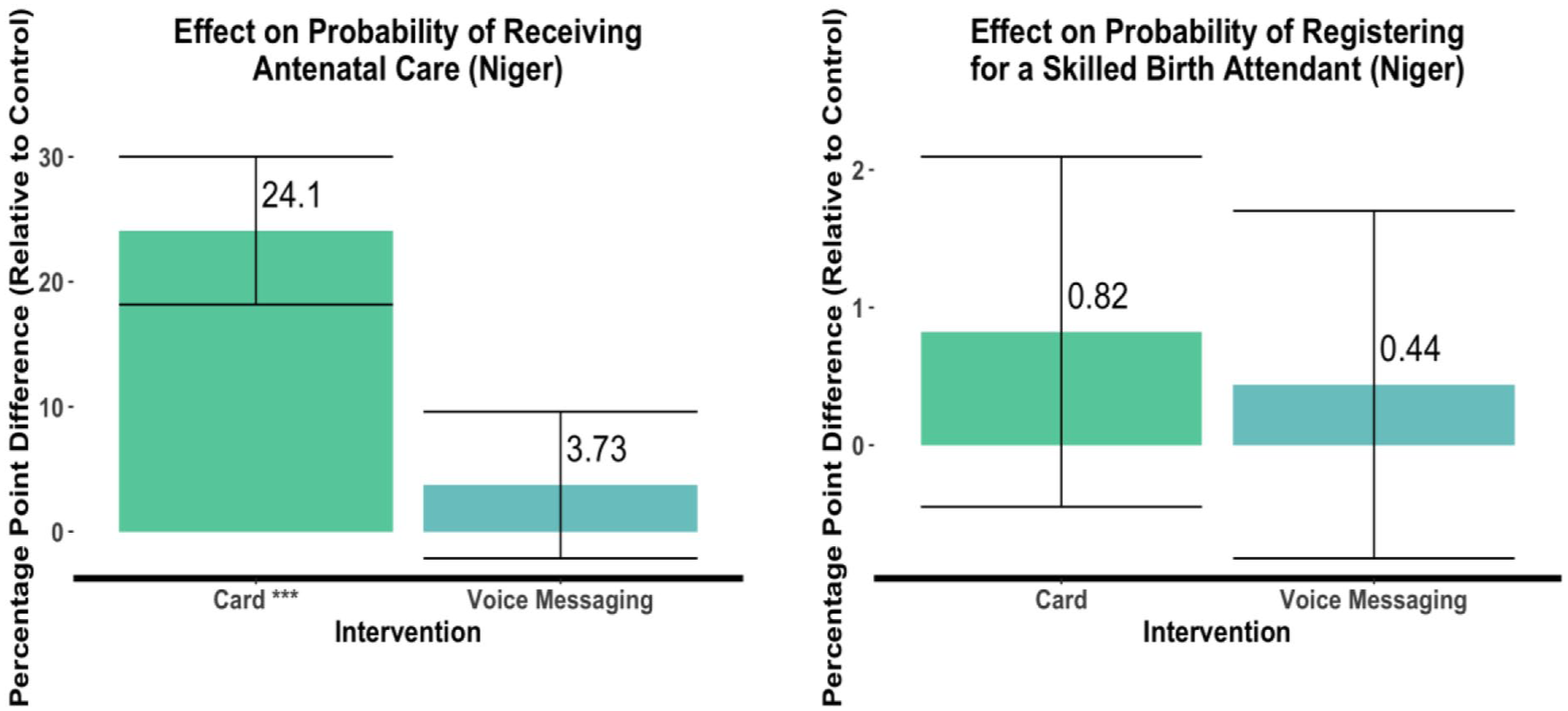
In Niger State, the incentivized visit-tracking card increased the probability of a woman attending at least one antenatal care visit by 24.10 percentage points relative to the probability found in the control group, a statistically significant effect (p < .01). (See Note A for a discussion of the statistical terms used in this article.) The effect of the voice messaging was minimal and not statistically significant, with a 3.73 percentage point difference with respect to the control group. The number of women registering for a skilled birth attendant or skilled delivery services was similarly low, and neither intervention showed a statistically significant effect on this outcome: Compared to the control group, registration for a skilled birth attendant was 0.82 percentage points higher for the card recipients and 0.44 percentage points higher for the women who were sent the voice recording. See Figure 4.
Effects of the interventions in Niger State
Effects of the Interventions in Gombe State
In Gombe State, the incentivized visit-tracking card also made a statistically significant impact on the number of women receiving antenatal care: The women who received the card were 18.17 percentage points more likely to attend antenatal health care visits than women in the control group (p < .01). Unlike its effects in Niger, the card made a small (5.45 percentage points), but statistically significant (p < .01) difference in the probability of engagement with skilled delivery services in Gombe. But similar to the results in Niger, the voice messages had no, or even a slightly negative effect, on boosting the probability of an antenatal visit. However, the messages did increase the probability of registering for skilled birth attendant services by 2.68 percentage points (p < .1). See Figure 5.

Effects of the interventions in Gombe State
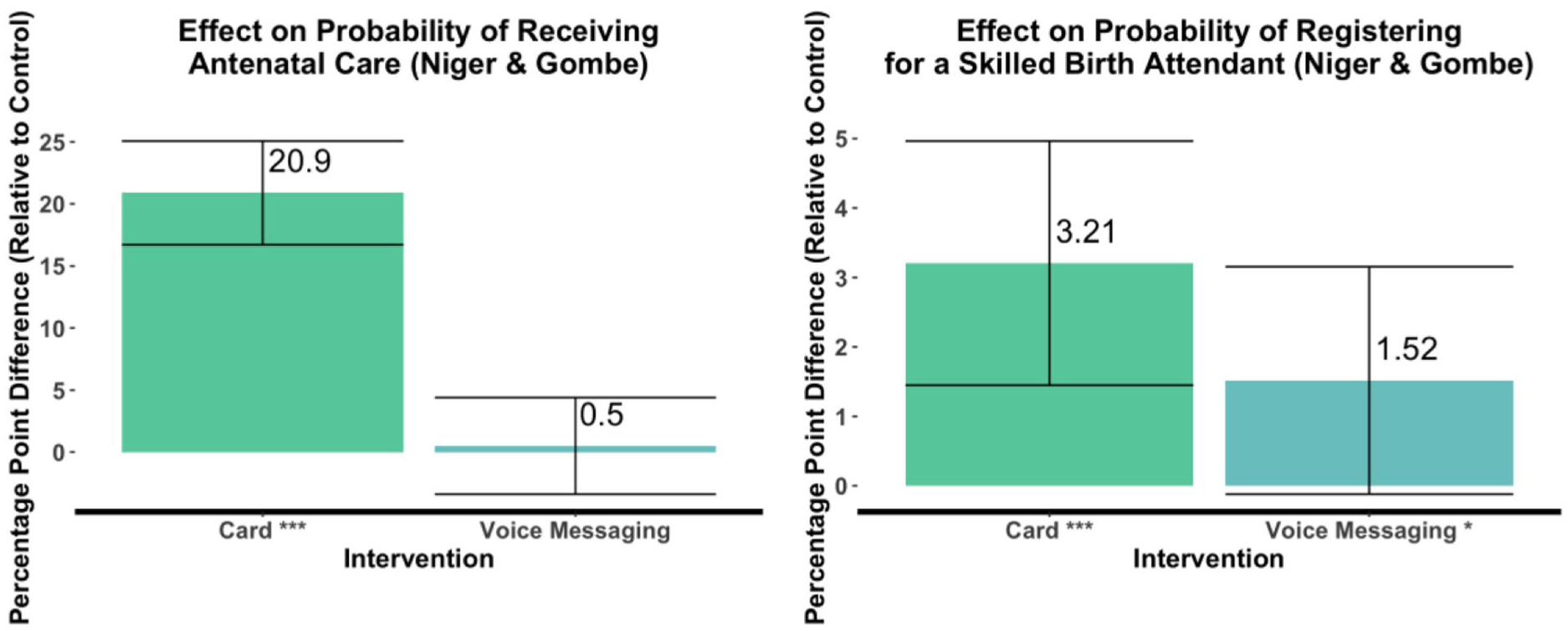
Combined Results
Merging the data for both states showed an advantage for the card on the probability of antenatal care uptake of about 20.90 percentage points (p < .01). By contrast, the voice recordings had no significant effect on this outcome. The card intervention also increased the probability of skilled birth attendant registration by 3.21 percentage points (p < .01) compared to 1.52 percentage points for the voice recordings (p < .1). See Figure 6.
Combined effects of interventions in both states
For the voice recordings, we did a separate calculation across both states for expectant mothers in their third trimester. For these women, the voice recordings had a slightly greater impact on registration for skilled delivery services, boosting these registrations by 4.40 percentage points relative to the control group.
Discussion
Policymakers in Nigeria and across the developing world face mounting pressure to meet the targets for health and well-being listed among the United Nations Sustainable Development Goals 45 (see https://sdgs.un.org/goals for these goals). To meet these targets, policymakers need more data on the relative efficacy of interventions aimed at boosting compliance with health-related recommendations. In this study, we compared the effects of an incentivized visit-tracking card with that of a voice messaging intervention on the probability of uptake of antenatal care services and registration for a skilled birth attendant among pregnant women in two northern states in Nigeria.
Impact of Incentivized Visit-Tracking Card
The success of the incentivized visit-tracking card on both antenatal care uptake and the intention to use a skilled birth attendant suggests that an infographic card combined with a gamified incentive could encourage pregnant women in sub-Saharan Africa to heed health care guidelines. We suspect that both components of the intervention contributed to its success. The gamified incentive likely motivated mothers to visit a health care center, and the images on the card reminded the women of these appointments and of their importance.46–48 In another study, 49 similar “commitment devices,” tools that help women consistently complete tasks or work toward a goal, increased usage of skilled delivery care at a health facility.
An incentivized visit-tracking card such as the one we used may be more scalable than approaches that rely on the limited supply of skilled health care workers in sub-Saharan Africa 46 as it requires minimal human input. Our gamified incentive was also designed with limited resources in mind, as the reward was given to only a small fraction of individuals exhibiting the desired behavior instead of to every person who did. The reduced probability of reward did not seem to significantly lower women’s motivation to seek health care, indicating the power of a perceived incentive50,51 and of potential rewards to motivate behavior.
Personal financial incentives are most effective at driving behavior change in the first few weeks to months after they are introduced, with effects typically fading within three months of their removal. 52 The impact of incentives on behavior often declines once the incentive is removed. 53 Incentives last only as long as there are resources to sustain them and policymakers are still aiming to meet their targets for behavior change. Nonetheless, gamified performance-based incentives like the one we tested could kickstart maternal care demand, especially in places where baseline uptake of maternal services is very low, as was the case in our study region.
Impact of Interactive Voice Messages
The interactive voice messages were less successful in encouraging women to attend antenatal care visits than the card was in both study locations. The voice intervention had a positive effect only in Gombe and only on the probability that a woman registered for a skilled birth attendant. This finding suggests that under some circumstances, voice messaging might encourage the use of skilled delivery services. We do not know what circumstances are most conducive to this outcome, though they may lie in cultural factors unique to each region.
The limited success of this intervention was somewhat surprising, given the proven effectiveness of mobile-based health interventions in improving maternal outcomes in Tanzania, Kenya, Ethiopia, and Ghana.41, 54–60 However, there was at least one key difference between the most successful of these interventions 57 and our voice messaging strategy. The most successful messaging included interactive features that allowed patients to communicate with health care staff and to receive referrals or to access prerecorded maternal and sexual health counseling. So, expanding the number of interactive components could strengthen the impact of our intervention. In addition, the literature suggests that positive maternal outcomes from mobile health interventions are most likely to be seen when interventions last between six and twelve months.59,61 Our pilot study might also have been too short to fully assess the benefit of each intervention.
But location may matter too, due to the varying reliability of electrical grids and mobile networks across some parts of sub-Saharan Africa. Mobile-based interventions alone may not work well in northern Nigeria, where electrification is incomplete and mobile network connectivity is unpredictable, limiting the ability of those who have mobile phones to receive calls. The instances of mobile phone sharing in Niger state may both reflect some of these issues and compound them, depressing the efficacy of voice messaging for the target audience—for instance, if a spouse is either unwilling or unable to give his wife the phone when a call arrives.
One overall limitation of the study is that it only assessed maternal visits to the small number of well-functioning primary health care centers within the designated study region. Our results might undercount such visits if any of the women in the study sought care from better equipped health care facilities outside the study region because of our messaging.
Recommendations
As the sidebar “Key Policy Points” indicates, to boost the use of antenatal services by pregnant women in Nigeria and similar locales, health care policymakers and practitioners should consider strategies such as our incentivized cards with infographics that remind women of the consequences of neglecting to see a health care provider and that help women track their health care visits. Supplementing practical information and reminders with incentives 62 and gamification through raffles may provide a cost-effective solution to bolster behavior change in the short term. However, more evidence is needed on how long gamified incentives can motivate women in Northern Nigeria to use maternal health care.
We are intrigued by the finding that the voice messaging intervention, whose only benefit was to marginally raise the probability of engagement with a skilled birth attendant, seemed to have the greatest impact on women in their third trimester of pregnancy. This outcome suggests that mobile health interventions may yield the most benefit if implemented toward the end of gestation. However, more evidence is needed to support the efficacy of digitized behavioral messaging at different stages of pregnancy. Regardless of that timing, health care decision-makers should thoroughly investigate the feasibility of mobile interventions by assessing patterns of mobile use, such as device sharing, and how these patterns could affect intervention delivery.
Implications for Future Research
As this study was a pilot, its results will be useful in guiding the design of a more expansive trial. Experimental data from a larger cohort of women from the start to the end of their pregnancy could reveal how health-seeking behavior changes over time in response to nondigitized and digitized behavioral messaging and incentives. A larger sample size would also allow for a nested experimental design that explores how a tracking card with infographics would perform without a gamified incentive as well as the efficacy of mobile phone messages coupled with a gamified incentive.
In addition, employing other statistical methods to analyze the data may uncover the layers of factors that affect the uptake of maternal care in sub-Saharan Africa. For example, survival analysis, which involves calculating the time to an event, could factor in how long it takes pregnant women to attend antenatal care and the social and environmental factors that delay attendance. A better understanding of why so few expectant mothers in certain countries get this care could pave the way to improved survival of mothers and their babies around the world.
Key Policy Points
Uptake of primary health care is inconsistent in many African nations, contributing to high rates of infant and maternal death and disability.
Nigeria has one of the highest maternal and child mortality rates worldwide, accounting for 12% of maternal and neonatal deaths and stillbirths globally.
Uptake of maternal health care services is low in Nigeria. In 2021, a survey conducted by the Nigerian National Primary Health Care Development Agency revealed that about half of pregnant women in Nigeria attended the then-recommended minimum of four (now eight) antenatal care visits and used a skilled birth attendant to deliver their baby.
To encourage women in developing nations to seek the recommended maternity care, our results suggest that policymakers should consider designing behavioral interventions with the following elements:
Nondigital reminders such as cards displaying infographics that show the recommended number of antenatal care visits for each trimester and that aid women in tracking their visits.
These cards should also indicate the potential consequences of neglecting to see a health care provider during pregnancy.
A cost-effective, gamified incentive for attending appointments, such as a raffle for maternal care prizes, should also be included.
Voice messages that stress the importance and practicality of antenatal visits seem to be less effective than an incentivized reminder. In our study, the voice messages sent to encourage use of antenatal and skilled birth services slightly increased women’s use of a skilled birth attendant, particularly during the third trimester of pregnancy.
Before administering any mobile health strategy, policymakers must ensure that mobile network coverage is stable, that women in the area have access to mobile phones, and that no cultural or practical barriers prevent their use.
Supplemental Material
sj-docx-1-bsx-10.1177_23794607251382993 – Supplemental material for Applying behavioral science to increase use of maternal care services: Findings from a field experiment in northern Nigeria
Supplemental material, sj-docx-1-bsx-10.1177_23794607251382993 for Applying behavioral science to increase use of maternal care services: Findings from a field experiment in northern Nigeria by Mohammed M Alhaji, Maryam Anike Yusuf, Laila Umar, Robert Nyaga, Arizechukwu Okafor, Francis Meyo, Zarah Haruna Shayau, Yakubu Ozohu-Suleiman, Zainab Ibrahim Isah, Aisha Mukhtar Dodo, Maryam Abubakar, Aisha Isa Umar, Halimatu Abubakar, Hauwa Nnatako Kolo and Usman S. Adamu in Behavioral Science & Policy
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Gates Foundation. The funder has no role in the study design, data collection, analysis, interpretation, writing, or publication decisions.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.