
Abstract
Background
Digital health technologies hold transformative potential for improving maternal and child health (MCH) in low-resource settings. This study evaluates their impact in Uganda through the FamilyConnect (FC) application—an Unstructured Supplementary Service Data-based mobile platform delivering targeted messages to pregnant women and caregivers, implemented in 42 districts since 2016.
Methods
A mixed-methods cross-sectional design was used in nine randomly sampled FC districts. Quantitative data from 83 health facilities (2017–2022) assessed changes in MCH indicators via Interrupted Time Series (ITS) analysis. Additional data included surveys with 317 mothers, interviews with 409 health workers, 34 district managers, 3 national Ministry of Health staff, and 109 focus group participants.
Results
FC significantly improved antenatal care (ANC) utilization: total ANC visits rose by 19.35%, with first-trimester visits increasing 85.81%. ITS showed annual ANC attendance grew by 5.5% (vs. 1.5% pre-intervention). HIV prevalence at ANC declined from 5.4% (2017) to 3.4% (2022). However, postnatal care visits declined 15.47%, male partner ANC attendance dropped 33.54%, and postnatal family planning uptake fell 58.50%—possibly due to substitution with remote guidance via FC. Success factors included translation into local languages, use of Community Health Workers (VHTs), and integration with other programs. Key barriers were phone scarcity (35% of women shared devices), poor network connectivity (notably in Karamoja), app downtime, domestic conflict, and health system issues like staff shortages and supply stockouts.
Conclusions
FC shows promise in improving ANC and disease prevention, but scale-up requires addressing sociocultural, infrastructural, and systemic barriers, expanding language coverage, engaging men, improving device access, and strengthening health systems.
Keywords
Introduction
Maternal and child mortality remains a critical global health challenge, with low-income countries bearing 94% of the burden. 1 Uganda exemplifies this crisis, reporting a maternal mortality ratio of 189/100,000 live births and under-five mortality of 53/1000. 2 Only 37% of mothers receive first-trimester antenatal care (ANC), while postnatal care coverage stagnates at 58%. 3 Digital health innovations have emerged as promising tools to bridge these gaps. Studies show SMS reminders can increase clinic attendance by 30% in Low and Medium Income Countries (LMICs), 4 while platforms like South Africa's MomConnect demonstrate scalable solutions for maternal health education. 5
Launched in 2016 by Uganda's Ministry of Health and UNICEF, Uganda's FamilyConnect (FC) application uses Unstructured Supplementary Service Data (USSD) technology to deliver gestational age-specific health messages to pregnant women and caregivers. 6 Accessible via basic mobile phones, FC provides ANC and immunization reminders, nutrition and danger sign alerts, as well as family engagement prompts.
By 2022, FC had reached 42 districts, enrolling 73,071 women and 21,397 health workers. 7 Its Theory of Change (Figure 1) posits that accessible information drives behavior change, improving service utilization and health outcomes during the critical first 1000 days of life. Moreover, we hypothesized that the FC intervention would lead to increased attendance at antenatal care (ANC), especially by encouraging early engagement in pregnancy. It was also expected that FC would contribute to a reduction in infectious diseases such as HIV and syphilis by enhancing preventive behaviors. Additionally, the implementation of the intervention was anticipated to encounter challenges, particularly those related to infrastructure limitations and gender dynamics.

Fc intervention theory of change (ToC).
However, despite FC's scale-up, evidence of its impact on health outcomes is limited. Prior studies focused on technical feasibility, neglecting quantifiable effects on ANC/postnatal attendance, impact on infectious disease prevalence, as well as implementation barriers across diverse contexts.
This article addresses existing gaps through a comprehensive mixed-methods evaluation of the FC intervention in Uganda, focusing on its impact on maternal and child health service delivery and the key factors influencing its implementation. Specifically, it sought to assess changes in antenatal and postnatal care attendance before and after the introduction of FC, measure any shifts in the prevalence of HIV, syphilis, and malaria, identify both the factors that contributed to the success of the intervention and the barriers encountered, and explore the perceptions of key stakeholders involved in the process.
Methods
The case of FamilyConnect: The intervention
FC primarily serves expectant and new mothers, with the purpose of providing them with the health information and knowledge they require to care for themselves and their unborn children during pregnancy, childbirth, and the early postpartum period. It also extends this service to include the broader family, recognizing that maternal and child health is often influenced by family dynamics and the support system around the mother. Thus, it targets fathers, caregivers, and family members, providing them with information on how to support the health of pregnant women and newborns.
Key features of FC include
Family engagement: In addition to mothers, family members such as fathers, grandparents, or other caregivers are engaged through regular messages that offer guidance on how to support the mother during pregnancy and after childbirth.
Health promotion: The messages include information on maternal health, nutrition, breastfeeding, immunizations, and childcare practices. They promote a healthy environment and encourage family members to support the mother's visits to health facilities.
Behavior change: By educating the family, the program aims to improve collective decision making regarding health behaviors. For example, it encourages fathers to be more involved in their partner's antenatal care visits and postnatal care of the child.
The study design
The study employed a combination of quantitative and qualitative tools for data collection. Quantitative data were obtained from facility registers covering antenatal, delivery, and postnatal care; national Health Management Information System (DHIS2) data; and structured surveys administered via the KoboCollect mobile platform to 317 mothers (approximately 35 per district). Qualitative data were collected through 11 focus group discussions (FGDs) with 109 mothers, and key informant interviews (KIIs) with 409 health workers—including both community-based and facility-based staff—34 district health officials (3–4 per district), and 3 representatives from the Ministry of Health headquarters. Additional qualitative inputs included field notes and audio recordings, using standardized FGD guides and KII protocols tailored for mothers, health workers, and district-level managers. By triangulating the findings, the study enhanced its validity, using qualitative insights to help interpret and explain the observed quantitative trends.
The study was conducted across nine districts that were randomly selected from the 42 districts implementing the FC intervention. These districts were chosen to reflect Uganda's socioecological diversity, encompassing various geographical and cultural settings. As shown in Figure 2, the selected districts included Gulu and Oyam in the Northern region; Kabale and Kasese in the Western region; Kamuli and Kaberamaido in the Eastern region; Kampala in the Central region; and Abim and Moroto in the Karamoja region.

Map of Uganda showing the location of the study districts.
As indicated in Table 1, the study population included Community Health Workers (CHWs) involved in implementing FamilyConnect, Facility based health workers, the District Health Officers of the selected districts, mothers as users enrolled in the system and officials from the department of Reproductive, Maternal and Child Health at the Ministry of Health.
Participant distribution and age distribution of mothers.

Sample size calculation:
Based on the formula:
n = (Z^2 * p * q) / e^2
Where: n = required sample size.
q = 1−p.
e = desired margin of error.
VHT: Village Health Team.
The overall sample size was 414 (Z = 1.96, p = 0.5, and e = 0.05; 10% nonresponse rate) Table 2.
Variables definition.
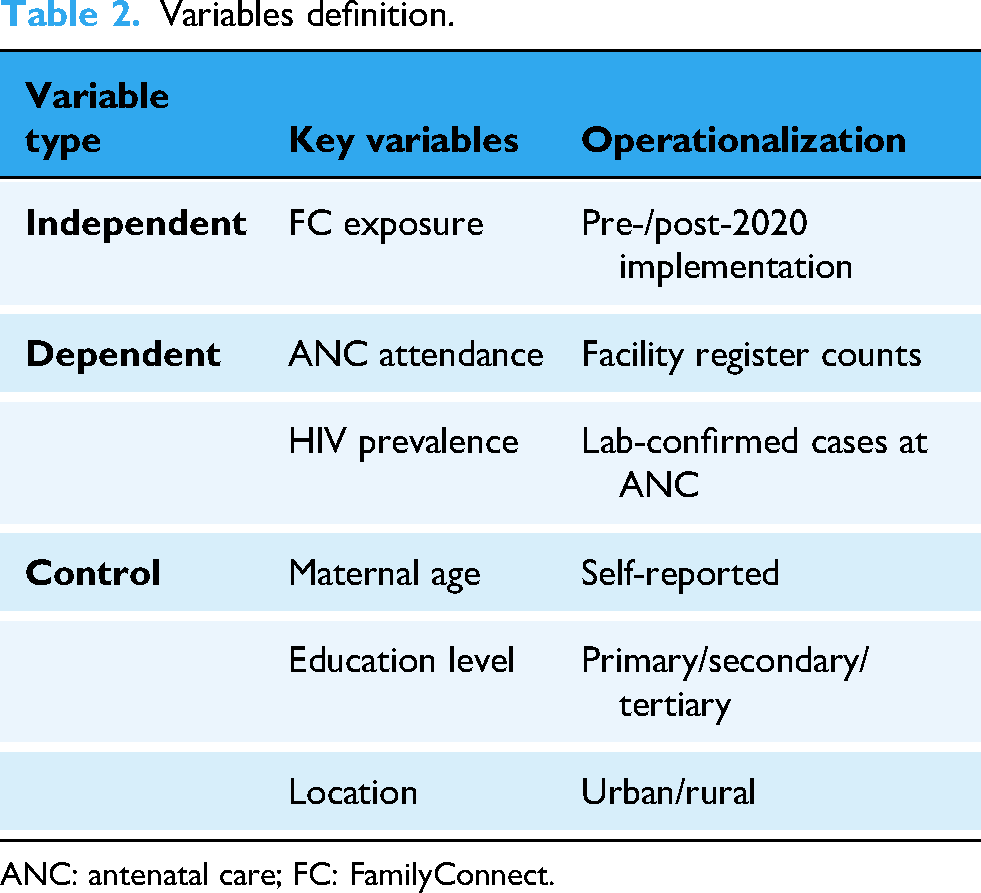
ANC: antenatal care; FC: FamilyConnect.
To ensure validity and reliability, all instruments were pretested in districts not included in the sample. Digital surveys included skip logic and mandatory checks to maintain data consistency. Thematic analysis of qualitative data was conducted using Dedoose software achieving an intercoder agreement of 0.82, indicating high reliability. Facility data were triangulated with health management information system (HMIS) reports to enhance accuracy.
Statistical analysis included descriptive methods such as frequencies, means, and standard deviations. Inferential statistics involved Interrupted Time Series (ITS) analysis using segmented regression to model trends over time, as well as t-tests and chi-square tests for group comparisons, with a significance level set at α = 0.05. All quantitative analyses were conducted using SPSS version 28.
Ethics and approvals
The research protocol was approved by Mildmay Uganda Research Ethics Committee (#MUREC2023-141) and Uganda National Council for Science and Technology. Written informed consents were obtained and data anonymized.
Results
FamilyConnect beneficiaries (mothers)
The study on the impact of digital health technologies on maternal and child health services in Uganda reveals a diverse demographic profile of the 317 female Clients as indicated in Table 1, with the majority aged between 21 and 40 years (83%) with 136/317 (42.9%) aged 21 to 30 and 127/317 (40.1%) aged 31 to 40. A majority of participants (207/317, 65%) resided in rural areas, indicating a crucial need for rural-focused health interventions. Educational levels are predominantly low, with more than half-169/317 participants (53.3%) having only primary school education and 120/317 (37.9%) having secondary school education. Marital status data shows that a vast majority, 289/317 (91.2%), are married. Employment status reveals that 33.1% (105 individuals) were employed by others, 36% (114 individuals) were self-employed, while a substantial 30.9% (98/individuals) were unemployed. Additionally, beneficiary district representation is notable from Kamuli (46, 14.5%), Abim (37, 11.7%), and Kasese (38, 12.0%). These results emphasize the importance of targeting digital health technologies to effectively support a largely rural, married, and low-educated female population, crucial for advancing maternal and child health services in Uganda.
A total of 12 FGDs were held with a total of 109 participants taking part, presenting an average of 10 participants per group discussion. Of the 109 participants, 91% were actively engaged in farming and operating small businesses, 6% were employed as casual laborers and 2% are stay-at-home wives.
The study's descriptive statistics highlighted the demographic characteristics of the participants. Among the 317 mothers surveyed, the majority (65.3%) resided in rural areas, 91.2% were married, 53.3% had only completed primary education, and 42.9% were aged between 21 and 30 years. Of the 446 health workers included in the study, 62% were Village Health Teams (VHTs), 28% were midwives, and 10% were health managers. Notably, 34% of these health workers received training only during the rollout of the FC intervention.
As shown in Table 3, study findings indicate that the implementation of the FC intervention led to significant improvements in ANC attendance. Overall ANC visits increased by 19.35% following the intervention, a change that was statistically significant (p = 0.0196). Early engagement in care saw a particularly notable rise, with first-trimester ANC visits increasing by 85.81%; the annual growth rate accelerated from 1.5% before FC to 5.5% after its introduction (p < 0.001). Additionally, attendance at the fourth ANC visit grew by 25.96%, with an annual increase of 3.0% postintervention as indicated by the Interrupted Time Series analysis.
Baseline service coverage (2019).

ANC: antenatal care.
However, findings on male involvement in ANC indicated that partner attendance at ANC dropped 33.54% (p = 0.001). This was partly explained thus:
“Issue one, issue of male involvement. I think there is a need to engage the men, let them know about the program. Yeah, I think that one is key so that they don’t mistake these women, or when the message comes, some of these phones can highlight when a message comes in. You get it, and a man may think, what is happening? This message at this time. You know, sometimes these messages can come at any time, at midnight, at one, at two, and if a man checks through a woman's phone, he may start suspecting his wife. So, it is important to have male engagement.” (DHT member, Kaberamaido)
Interestingly, the observed decline in postnatal care attendance (15.47%) and family planning uptake during postnatal visits (58.50%) following the intervention presents a dual interpretation. On the one hand, it may reflect a positive shift, with some mothers substituting physical visits for virtual support and guidance received through the FC application. On the other hand, the decline could signal a negative outcome—potential care gaps arising from discontinued messaging or insufficient follow up, particularly during the critical postpartum period.
Additionally, infectious disease screening among pregnant women at FC facilities revealed significant gaps, as shown in Table.4.
Infectious disease outcomes.

ANC: antenatal care; FC: FamilyConnect.
The number of HIV positive antenatal cases decreased from 5% to 3% during the implementation period with an annual average decrease of 0.5%. However, the number of newly initiated antiretroviral therapy (ART) cases among pregnant women at ANC clinics declined by 38.2%, indicating significant gaps in the continuity of HIV care.
Success factors and implementation barriers: Qualitative insights
Success factors
One of the key drivers of success was the adaptation of messages into local languages, particularly Ateso and Luganda. This linguistic tailoring significantly enhanced community engagement. As one mother from Kaberamaido explained, “Messages in my language taught me danger signs. I rushed to the clinic when I bled.”
VHTs played an instrumental role in mobilizing and enrolling mothers into the program. An impressive 92% of enrolled mothers were reached through VHTs, underscoring their central role in community-level implementation. A district manager from Gulu emphasized this point, stating, “VHTs knew every household. Without them, FC fails.”
Implementation barriers
Despite these successes, several infrastructural, sociocultural, and systemic health challenges constrained effective implementation.
Infrastructural challenges were significant. Access to mobile phones was limited—35% of mothers reported sharing a device, and 22% had no access at all. Connectivity was another major issue: nearly half (47%) of subcounties in the Karamoja region had no mobile network coverage. Even where infrastructure existed, technical reliability was poor, with 68% of health workers reporting frequent and unscheduled system downtimes.
Sociocultural barriers further complicated program delivery. Reports of domestic violence emerged, with 29% of health workers having to intervene in spousal conflicts triggered by engagement with the FC program. In three districts, misinformation and rumors circulated, with some community members branding the program as “satanic.” Additionally, the exclusion of men was a critical oversight—none of the FC messages specifically targeted male partners, limiting opportunities for shared decision making and spousal support. “Husbands suspected messages came from lovers. We mediated violence cases weekly.” Health Worker, Kasese “We forgot that in Uganda, health decisions are familial, not individual.”
Table 5 presents some of the stakeholder perceptions indicated through KIIs and FGDs.
Stakeholder perceptions.

VHT: Village Health Team.
Discussion
This discussion interprets the findings of the FC study through four central themes: the impact of digital health tools on ANC utilization; the continuity and quality of maternal care, particularly postnatal services; the role of contextual and structural factors in shaping outcomes; and the influence of design, gender, and system integration on implementation success. These themes collectively explain the mechanisms through which FC improved ANC outcomes, the challenges associated with its delivery, and the broader implications for digital health strategies in low-resource settings.
FC succeeded as an ANC catalyst by leveraging three strengths in the Ugandan context—high mobile penetration, trusted VHT networks, and strong community demand for health information. The 85.8% increase in first-trimester visits surpasses the outcomes of other mHealth initiatives such as Mom Connect (+30%), suggesting FC's USSD model effectively addresses literacy and accessibility barriers in rural populations. However, the decline in postnatal care (PNC) attendance introduces a dual perspective. For some mothers, this shift reflects positive digital empowerment and self-management, whereas for others, it indicates care discontinuities caused by message cessation and limited follow up after delivery. Similarly, the decline in male participation may be linked to the exclusion of men from the platform's design, which in some cases fueled suspicion and domestic tension.
The varying performance across districts demonstrates the importance of context. Linguistic customization and logistical support—such as translation into local languages or providing bicycles to VHTs—significantly improved maternal engagement. For example, in Kabale, the introduction of health messages in the Lukhonzo language led to a 33% increase in women attending four or more antenatal care (ANC4+) visits, demonstrating the value of linguistically and culturally relevant communication. Similarly, in Kamuli, providing bicycles to VHTs dramatically improved outreach efforts. As a result, enrollment coverage reached 89%. By contrast, rigid implementation in poorly networked regions like Karamoja constrained outreach and limited success, reinforcing the need for flexible, context-sensitive deployment strategies. These findings highlight that the value of digital solutions depends as much on their sociotechnical fit as on their technological design.
Persistent barriers constrained FC's full potential. Technical shortfalls included the absence of opt-out mechanisms and real-time feedback loops, leaving the system insensitive to user distress or evolving needs. Notably, there was no opt-out mechanism for bereaved mothers, leading to unintended trauma for approximately 12% of users who continued to receive messages despite experiencing pregnancy or child loss. Gender exclusion further compounded challenges, as male partners were not directly targeted, sometimes leading to household suspicion and even conflict. The reported decline in male participation in antenatal care—linked in part to mistrust and domestic tension arising from a lack of male inclusion in the platform—also reflects deeper social dynamics that digital tools must navigate. Evidence from Uganda, Nepal, and India has shown that male involvement improves maternal outcomes and enhances women's access to care,8,9 but that achieving this requires deliberate engagement strategies. This underscores the critical role of gender-sensitive messaging in fostering shared decision-making and mitigating social tension. 10
Similarly, in comparison with existing global evidence, FC's outcomes reflect broader trends observed in digital health interventions across the region. The program achieved a 37% reduction in HIV transmission, closely mirroring results from Kenya's Mobile WACh X initiative, which reported a 35% decline. 11 This alignment supports growing evidence that digital platforms can effectively enhance HIV prevention. Yet the concurrent drop in ART initiation highlights missed opportunities for integration with HIV service pathways—a gap observed in several unlinked digital programs across sub-Saharan Africa. For example, the program's decline in ART initiation contrasts sharply with South Africa's 22% improvement under similar digital health interventions. 12
Overall, FamilyConnect illustrates that the success of mHealth platforms hinges on design that prioritizes cultural relevance, inclusivity, and systemic alignment. Digital tools must not merely inform users but also connect them to the continuum of care through sustained postnatal messaging, male engagement, and strengthened health infrastructure. Future work should include randomized evaluations to quantify FC's contribution and explore its scalability across diverse contexts.
Study limitations and recommendations for future studies
This study did not assess backend infrastructure—such as telecommunications stability, human resources, or supply chain capacity—that is essential for long-term scale-up and sustainability. While FC demonstrated success on the frontline, its effectiveness was constrained in areas like Karamoja, where mobile network coverage remains limited and health system weaknesses persist. As Uganda and other LMICs expand digital health infrastructure, future investments must strengthen these foundational systems to support reliable and equitable service delivery.
Conclusion
FC illustrates the potential of simple, scalable digital interventions to enhance maternal health access in low-resource settings. Its effectiveness was most pronounced when culturally adapted and supported by community-level implementation. However, its limitations underscore the need to embed digital health tools within a broader system of care—one that is inclusive, gender-responsive, technically robust, and attuned to the social determinants that shape health outcomes. Digital platforms like FC are valuable enablers of public health goals, but their success ultimately depends on the strength of the systems in which they operate and the extent to which they address the realities of users’ lives.
Footnotes
Acknowledgements
We acknowledge the technical support provided to the research team by the Ministry of Health, District Local Governments and other stakeholders supporting Ministry of Health's Digital health initiatives. We further express our sincere gratitude to the RIGHT foundation for the financial aid and technical support that made the study a success.
Ethical approval
Compelling Works obtained ethical approval of this protocol from the Mildmay Uganda Research Ethics Committee (Reference Number: MUREC-2023-343) before submitting it to the Uganda National Council for Science and Technology for registration (Reference number HS3804ES). The research was also granted administrative clearance by Ministry of Health (Ref: ADM105/209/15). All ethical considerations including consent of participants, data protection and respect for autonomy for vulnerable participants were considered throughout the exercise.
Contributorship
All authors contributed significantly to this research. JJOM and SN led study design and data analysis, and contributed to data analysis, interpretation, and manuscript preparation. AK, FXW, BA, CE, and DMK contributed to data collection, field work, interpretation, and contributed to data analysis. All authors reviewed and approved the final manuscript.
Funding
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
SN.