
Abstract
Disability is predominantly understood as a medical problem. Since the 1980s, disability scholars have critiqued the medicalization of disability to illuminate disability’s social and political dimensions. Building on this tradition, the present article analyzes the Paralympic movement to call sociological attention to how medicalization affects disabled social movements, cultural production, and cultural practices. The author draws from interviews with Paralympic athletes and coaches alongside primary historical sources to identify and evaluate medicalization’s effects on the Paralympic movement. Findings show that medicalization both enabled and constrained the Paralympic movement. The medicalization of spinal cord injuries developed lifesaving treatments and mobilized disability sport as rehabilitative treatment to mold patients into healthy, productive “taxpayers.” Framing disability sport as rehabilitation catalyzed the medicalization of the Paralympic movement, as the medical profession facilitated the formation and maintenance of the movement. This understanding of disability sport reflected the clinical nature of medicine and rehabilitation’s approach to disability. However, the clinical approach to Paralympic sport conflicted with Paralympians’ desire for high-performance disability sport and recognition as elite athletes. Medical governance subsequently marginalized Paralympians within Paralympic organizations and limited Paralympians’ ability to develop their sports beyond mere rehabilitation. These findings are consistent with Mauldin’s conceptualization of medicalization as “ambivalent.”
Within sociology, theoretical approaches to disability broadly fall into two contrasting camps. The first camp, established by medical sociology and the sociology of health and illness, primarily theorizes disability through the lens of social deviance as abnormal or biologically deficient (Thomas 2004, 2007). Such examples include the classic works of Parsons (1951), Foucault (1965), Goffman (1968), and Strauss and Glaser (1975) among many others. The second camp originated within disability studies in the 1980s and theorizes disability through the lens of social oppression. Influenced by materialist thought, these scholars critiqued the medical model of disability and initially coalesced around the social model of disability, which distinguished between impairment (a biological difference) and disability (social oppression built upon impairment) (e.g., Abberley 1987; Finkelstein 1980; Oliver 1990). Building on this critical theoretical foundation, scholars have developed a rich array of sociopolitical theories of disability inspired by Oliver’s original social model—what Shakespeare (2014) called “the family of social approaches” (p. 47). A multitude of empirical analyses have mobilized these social approaches to examine the structural inequalities that disabled people face in a number of arenas, including but not limited to civil rights (Pettinicchio 2019), labor (Ruppel 2024), and education (Dolmage 2017). Yet the broader discipline of sociology has yet to fully engage with disability studies’ theoretical frameworks, and a rift persists between how disability is studied among sociological subfields, that is, medical sociology and the sociology of health and illness versus the sociology of disability (Mauldin and Brown 2021).
The history of the Paralympic movement vividly illustrates tension between medical and social models of disability in action. Medical and rehabilitative professionals mobilized disability sport as rehabilitation for patients, but Paralympians eventually engaged in disability sport as elite athletes pursuing high-performance sport, not medical treatment. Gérard, Legg, and Zintz (2017) correlated the rehabilitative and sport logics of Paralympic sport with the medical and social models of disability, respectively. At its core, the social model of disability can be understood as a critique of how the medical model medicalizes disability (Mauldin and Brown 2021). The purpose of this study is to analyze the effects of medicalization within the Paralympic movement. Although the rehabilitation subspecialty’s focus on restoring abilities and returning individuals to work is distinct from broader medicine’s traditional focus on diagnosing and treating pathologies (Hunt 1956), both converge in their clinical approach to disability. Consequently, I examine rehabilitation as a type of medicalization.
Furthermore, Paralympic history demonstrates how practical consequences arise from conflict between the medical and social models, particularly when the medical model is institutionalized. The findings presented in this article show that medicalization had an ambivalent effect on the Paralympic movement. Although medicalization produced lifesaving treatments and built the Paralympic movement, clinicians’ medicalized model of Paralympic sport clashed with Paralympians’ approach to Paralympic sport over concrete issues regarding governance and practice. Medicalization subjected Paralympians to medical management and ideology. Furthermore, medicalization impeded Paralympians’ efforts to expand Paralympic eligibility to include broader segments of the disabled population and hampered the development of wheelchairs as specialized sporting equipment.
Despite emerging from a therapeutic regime to become one of the world’s most visible disability events and largest sporting events, the Paralympic movement has received insufficient attention from the medical social sciences in terms of its historical development. The Paralympic Games are consistently one of the world’s largest sporting events by number of competitors (Brittain 2010), featuring 4,400 Paralympians at the most recent 2024 Summer Games in Paris (International Olympic Committee 2024). Not to be confused with the Special Olympics, which organizes sport under a participation model exclusively for intellectually impaired athletes (Brittain 2010), the Paralympic Games are the Olympic equivalent for elite, nondeaf 1 disabled athletes. 2 Through its global platform, the Paralympics influences global perceptions of disability, though scholars debate whether the Games do so for better or for worse (Bartsch et al. 2018; Brittain and Beacom 2016; de Souza and Brittain 2020). Despite the Paralympics’ international prominence, many are unaware that the Games emerged out of rehabilitative therapy for World War II veterans with spinal cord injuries (SCIs) (Goodman 1986; Scruton 1998). Existing literature on Paralympic history frequently omits the voices and perspectives of Paralympians (Peers 2009). This research addresses this critical empirical gap by centering Paralympians’ firsthand experiences with medicalization as reported in interviews.
The medical profession played a leading role in founding the Paralympic movement and governing the organizational predecessors to the International Paralympic Committee (IPC), but the mixed consequences of medical control of the Games have received insufficient examination (Brady 2023 and Peers 2018 are two notable exceptions). Although Paralympic scholars describe the Games’ medical origins and governance, few critically investigate the Paralympics in relation to theories of medicalization. Instead, those who do examine the role of medicine in the Paralympics approached the subject through the lens of institutional theory, examining how the Paralympics gradually shifted its focus from rehabilitative therapy to elite disability sport 3 (Brittain 2012; Gérard, Brittain, and De Vita 2025; Gérard et al. 2017; Legg and Steadward 2011). Given the fraught relationship between medicine and disabled people (Barnes 2019; Brisenden 1986; Conrad 1992; Oliver 1990; Shakespeare 2010), especially before the deinstitutionalization and disability rights movements, the effects of what I term Paralympic medicalization warrant further interrogation.
I take a multimethod approach to understand how medicalization affected the progression of the Paralympic movement. First, I conducted 49 semistructured interviews with 40 retired Paralympic actors, including retired Paralympians and Paralympic coaches. Results from interviews then guided archival analysis of primary historical documents from three organizational predecessors to the IPC. I find that medical professionals played crucial roles both in providing lifesaving treatment as well as establishing and sustaining the Paralympic movement. At the same time, medical control disempowered Paralympians within the movement and hindered their ability to advance Paralympic sport beyond rehabilitative activity. These findings advance an ambivalent understanding of medicalization’s effects (Blum 2015; Mauldin 2016; Reissman 1983) and point to medicalization’s influence over disabled social movements, cultural production, and cultural practices.
Paralympic Medicalization
Several scholars, among them retired Paralympians and Paralympic coaches (Howe 2008; Labanowich and Thiboutot 2011; Peers 2009, 2012a, 2012b; Strohkendl 1996), called attention to the role of medical control within the Paralympic movement. However, the Paralympic movement has seldom been analyzed as a case of medicalization (Peers 2018 is one exception). Other scholars have analyzed medical framings of Paralympic sport through the lens of institutional logics (Gérard et al. 2017). In this study, I examine the early Paralympic movement through the lens of medicalization theory to center the social construction of disability sport as medical in nature and emphasize hierarchical medical power relations within Paralympic organizations.
Conrad (1992) identified medicalization as a definitional process: Medicalization consists of defining a problem in medical terms, using medical language to describe a problem, adopting a medical framework to understand a problem, or using a medical intervention to “treat” it. This is a sociocultural process that may or may not involve the medical profession, lead to medical social control or medical treatment, or be the result of intentional expansion by the medical profession. (p. 211)
I use Conrad’s definition to capture how medical professionals created the Paralympic movement by mobilizing disability sport as therapeutic treatment for disabled people. Drawing from Halfmann (2011), I investigated Paralympic history searching for biomedical discourses, practices, technologies, identities, and actors as characteristic of medicalization. Throughout this article, I use the term Paralympic medicalization to capture several dimensions of the medicalization of the Paralympic movement: the dominance of the medical profession in Paralympic leadership, the rehabilitative framing of disability sport, and the application of medical logics to Paralympic governance. As I explain in my findings, Paralympic medicalization is inextricably linked to, and an outgrowth of, the medicalization of SCIs. Although medicalization research mainly focuses on the definition of a medical problem, I examine alleged treatment.
Initially, medicalization research emphasized its negative consequences (Ballard and Elston 2005; Busfield 2017). Scholars called attention to the negative effects of pharmaceuticalization (Abraham 2010; Moynihan and Cassels 2005), the proliferation of psychiatric diagnoses and treatments (Conrad 2007; Horwitz and Wakefield 2007), and medical control of seemingly normal aging processes (Bell 1990; Conrad 2007). Moreover, medicalization critiques also proved central to the development of disability studies, as the social model of disability is itself a medicalization critique (Mauldin and Brown 2021). However, medicalization has also yielded many substantial benefits, including lower mortality rates and evidence-based medicine (Conrad, Mackie, and Mehrotra 2010; Gagné-Julien 2021; Kaczmarek 2018). Taking a more balanced approach, Mauldin (2016) coined the term ambivalent medicalization to underscore “that individuals are both empowered by and surrendering to the process of medicalization” (p. 4). This research uses Mauldin’s concept of ambivalent medicalization to outline the simultaneous positive and negative consequences of Paralympic medicalization.
I investigate the effects of medicalization within the Paralympic movement at both the micro- and meso-levels. At the micro-level, I examine disability sport practice and interactions between Paralympians and governing Paralympic officials. At the meso-level, I interrogate how the Paralympics were organized by Paralympic governing bodies. This research elaborates on the implications of expanding medical control as a consequence of medicalization (Conrad 2007). Medical social control has been noted to enforce new behavioral norms (Armstrong 2003), proliferate medical surveillance (Armstrong 1995; Conrad 2000; Klawiter 2002), and expand medical therapies (Conrad and Jacobson 2003; Sullivan 2001). My findings highlight how medicalization intersects with social movements, cultural production, and cultural practices to restrict autonomy from medicine and hinder the development of nonmedical structures, practices, technologies, and identities.
Research Design
This multimethod research integrates findings from Paralympic interviews and primary historical documents from IPC predecessor organizations. I conducted 49 semistructured interviews with 36 retired Paralympians, 2 prominent retired disabled Paralympic coaches, and 2 active veteran Paralympians. I first gathered participants through the U.S. Olympic and Paralympic Museum, which contacted their Paralympian alumni e-mail list on the study’s behalf. Recruitment then continued via snowballing, enabling access to networks of retired Paralympians, veteran Paralympians, and coaches that otherwise would have remained a “hard-to-reach population” (Goodman 2011:350). Interview questions focused on five themes: athletic career history, historical changes within disability sport, medicine in disability sport, the Paralympian community, and the meaning of disability sport.
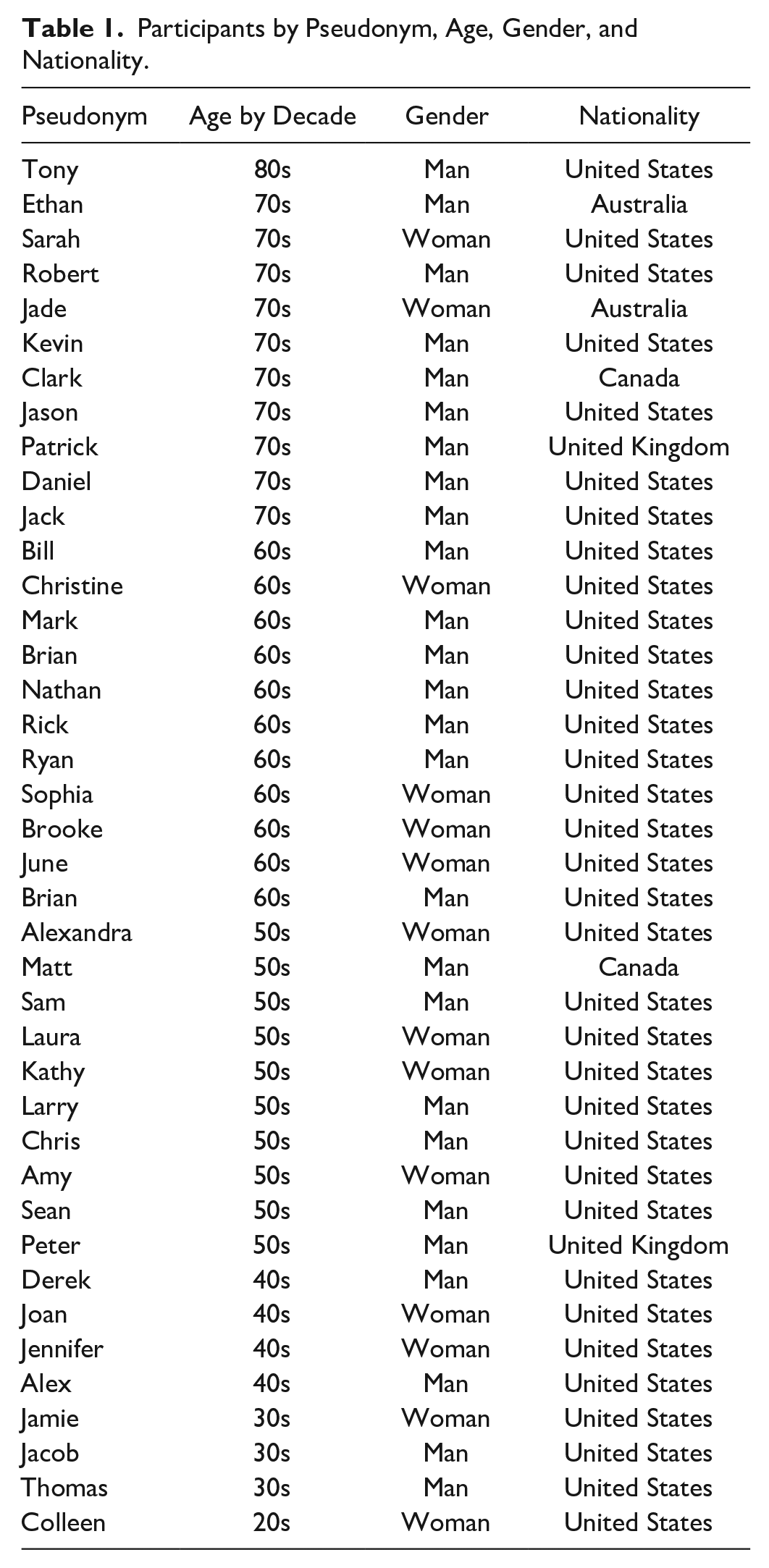
Table 1 includes a list of participants by pseudonym, age, gender, and nationality. Variance in participant age enabled the study to capture 40 years of Paralympic medicalization, beginning with observations of the Games in the 1970s. The sample comprises athletes and coaches from the highest levels of disability sport competition and leadership, including IPC Hall of Fame inductees, national and international governing body officials, and pioneering disability sport innovators. A range of impairment types are represented, including but not limited to paraplegia, quadriplegia, amputations, and blindness. No deaf athletes were represented in the sample, as they have long competed in the Deaflympic Games, a competition autonomous from the Paralympics (DePauw and Gavron 2005). Although athletes with intellectual impairments do compete in the Paralympics under the Games’ elite sport model (Brittain 2010), none were included in this study’s sample. Despite the Paralympic Games’ origins as therapy for injured veterans (Goodman 1986; Scruton 1998), only two participants acquired their impairments from military service. Although the Paralympics are an international competition, hiring translators for interviews was beyond the scope of this project’s available resources. As such, participants are from English-speaking countries.
Participants by Pseudonym, Age, Gender, and Nationality.
One interview was conducted in person, one interview was adapted to written form for accessibility purposes, and the remaining interviews were conducted via Zoom video calls. All nonwritten interviews were audio recorded and automatically transcribed. Interview analysis used a grounded-theory approach to develop novel theoretical categories and themes (Charmaz 2006). Using Dedoose software, I began with open coding (Strauss and Corbin 1990) approximately half of transcripts to identify emergent themes, of which medicine was the most frequent (16.3 percent of codes [n = 155]). Informed by literature that documented the Paralympics’ medicalized origins (Brittain 2010; Goodman 1986; Howe 2008; Scruton 1998), I created this code to capture mention of medical professionals and medical frameworks. The majority of participants (80.5 percent [n = 29]) reported some level of medical involvement within the Paralympics. After writing analytical memos, I continued with thematic analysis (Braun and Clarke 2006) to identify patterns in responses pertaining to Paralympic medicalization. Responses fell within one of three thematic categories: (1) lifesaving treatment and Paralympic movement building, (2) Paralympian marginalization, and (3) limitations to disability sport development. Interview coding subsequently guided archival analysis.
I abductively (Timmermans and Tavory 2012) analyzed more than 1,800 pages of archival primary historical sources in search of the themes, categories, events, discourses, and disputes that emerged from interviews while remaining attentive to alternative patterns that emerged from archival sources. Archival analysis allowed historical verification and contextualization of participant responses. Moreover, interview-guided archival analysis rendered a narrative of the Paralympic movement that maintained the benefits of in-depth interviews: crucial insights into social movements’ internal micro-dynamics and centering social actors’ agency (Blee 2013; della Porta 2014). Archival materials consist of organizational records, including constitutions, minutes, reports, and regulations from three predecessors to the IPC: the International Stoke Mandeville Games Committee (ISMGC), the International Stoke Mandeville Games Federation (ISMGF), and the International Sports Organisation for the Disabled (ISOD).
Lifesaving Treatment and Paralympic Movement Building
Here, I outline the benefits of medicalization within the Paralympic movement. I first show that the medicalization of SCIs generated lifesaving treatments for patients. These medical interventions created new possibilities for disabled athletic participation, enabling SCI patients to become the first athletes of the Paralympic movement. Medicine’s framing of disability sport as rehabilitative treatment for SCIs medicalized the Paralympic movement itself, as medical professionals built, maintained, and governed the movement’s early organizations under this logic. These findings evidence that medicalization created the preconditions for the emergence of the Paralympic movement and catalyzed its organizational formation.
Lifesaving Treatment
Sam is a wheelchair racer whose first Paralympic Games were in the early 1990s. Sam observed that previous breakthroughs in medical care are the reason individuals with SCIs like himself are alive today. Without proper medical intervention and treatment, Sam asserted that a sports movement for paraplegic athletes could not have been possible: Medical advancements allowed for people with disabilities to survive. Having a spinal cord injury, you know, before antibiotics were invented was pretty much a death sentence. So, I mean, in the late ‘30s, early ‘40s, paraplegics just didn’t exist or they were in the back room just waiting to expire. . . Wheelchair sports couldn’t exist before the ‘40s because the population [those with SCIs] didn’t survive. (Sam)
The precursor to the Paralympic Games, the Stoke Mandeville Games for the Paralysed (SMG), originated at the United Kingdom’s Stoke Mandeville Hospital. During World War II, British soldiers with SCIs were sent to Stoke Mandeville for treatment. It was at Stoke Mandeville during the 1940s that Dr. Ludwig Guttmann, the hospital’s director, revolutionized SCI rehabilitative care (Goodman 1986). Guttmann’s revolution in rehabilitation practices for SCIs instigated a fundamental cultural shift in medicine’s conceptions of SCI prognosis, life expectancy, and broader life outcomes including employment and education.
When Guttmann began work at Stoke Mandeville in 1944, an SCI had been long regarded a certain and painful death sentence. Prevailing medical consensus held that patients with SCIs were “hopeless,” and treating them was considered “a waste of time” (Goodman 1986:9). Guttmann’s colleagues at Oxford University did not understand why he accepted a position within a spinal injury unit. At the time, 80 percent of individuals with SCIs died within three years, usually of complications from pressure sores and urinary infections (Goodman 1986:9, 104). Guttmann was displeased with the plight of spinally injured veterans, which he had personally witnessed during World War I and was irate that they were consigned to “the human scrapheap” by both medicine and broader society (Goodman 1986:99). In response, Guttmann instituted a “total care” regimen (Goodman 1986:100).
Under Guttmann’s leadership, Stoke Mandeville Hospital became an experiment to test whether SCI patients could be successfully stabilized and rehabilitated with extensive medical treatment. Guttmann’s regimen required medical staff to care for patients around the clock, rotating patients every two hours, catheterizing with aseptic technique upon admission, avoiding unnecessary surgery, and eventually sport participation (Goodman 1986:100–107). It was unknown whether SCI patients could be adequately stabilized for survival, and Guttmann described the medical profession’s “indoctrinated prejudice” against treating SCIs, including among his own staff, as a barrier to overcome (Goodman 1986:103). Ultimately, mortality rates decreased significantly, and Guttmann’s experiment proved a massive medical success (Guttmann 1945, 1954; Guttmann and Frankel 1966). Stoke Mandeville, and the games held there, became a rehabilitative epicenter through which Guttmann disseminated his therapeutic practices to clinicians around the world (Goodman 1986; Scruton 1998). Today, Guttmann is recognized as a pioneer in rehabilitation (Schültke 2010; Silver 2012; Stahnisch and Tynedal 2012). Although stabilizing SCI patients’ physical health was crucial, Guttmann’s ultimate goal was his patients’ complete reintegration into society. To that end, disability sport proved an integral rehabilitative tool for Guttmann.
Paralympic Movement Building
Ensuring SCI patients’ physical health during hospitalization was only half the battle. Guttmann’s patients faced significant challenges after hospitalization regarding mental health, gaining and maintaining employment, and adjusting to everyday life in a wheelchair (Guttmann 1948). Congruent with prevailing liberal values, Guttmann firmly held that work and recreation treated his patients physically and mentally. In his search to exhaustively identify effective rehabilitative modalities, Guttmann investigated the therapeutic potential of sport. As early as 1944, Guttmann introduced his patients to archery, netball, and table tennis (Goodman 1986). Guttmann asserted that disability sport would “transform a hopeless and helpless spinally paralysed individual into a tax-payer” (Goodman 1986:165). In fact, Guttmann wrote that sport was more important to his patients’ rehabilitation than traditional physiotherapy because of its recreational value (Goodman 1986). However, Michael Oliver, who himself participated in sport at Stoke Mandeville, wrote that the rehabilitative value of disability sport was “over-stated” (Oliver 1996:11).
As sport participation grew among patients, Guttmann organized competitions between other hospitals at Stoke Mandeville. The inaugural SMG consisted of an archery competition with 16 athletes held on the hospital lawns in 1948, the same day as the opening of the London Olympics (“Bus and Bowmen at Stoke Mandeville” 1948; Goodman 1986). The Paralympic movement was born. The SMG were held annually and became international in 1952 with the addition of a Dutch team. As the SMG expanded throughout the 1950s with the addition of other countries and new sports, the need for a governing body to organize, administer, and fund the Games became clear (Scruton 1998).
The ISMGC was formed in 1960 to fulfill these growing needs (Buckinghamshire Archives 1960b). When possible in Olympic years, the Games were held in the Olympic Games’ host city. Beginning in 1960, the Games that coincided with Olympic years are now retroactively recognized as the first Paralympic Games. During the 1960s, other organizations emerged to provide sporting opportunities to disabled people with non-SCI impairments. Notably, ISOD was formed in 1964 (Brittain 2012). In 1972, the ISMGC reconstituted itself as the ISMGF (Buckinghamshire Archives 1972). ISOD and ISMGF collaborated to organize the 1976 and 1980 Paralympic Games. The IPC was established in 1989 but did not become responsible for organizing the Games until after the 1992 Games (Brittain 2010).
These early Paralympic organizations were largely governed by medical and rehabilitation professionals. Notably, Guttmann was the founder and president of the ISMGC, ISMGF, and ISOD. Voting committee members were often other medical or rehabilitation professionals, and his assistant Joan Scruton was often secretary. Medical leadership persisted after Guttmann’s death, as Dr. Robert Jackson succeeded Guttmann as ISMGF president and was later followed by Dr. John Grant. Furthermore, Guttmann, his hospital staff, and appointed medical officials established relationships with funders to finance the Games, cultivated a relationship with the British monarchy and government for support, circulated literature to guide rehabilitative organizations around the world in creating disability sports programs, constructed physical infrastructure for the Games to be held on the hospital’s grounds, and initiated a working relationship with the International Olympic Committee that continues today (Goodman 1986; Scruton 1998). Crucially, medicine was also responsible for creating the Games’ classification system, which refers to a system of rules that determines whether athletes meet minimal disability eligibility for Paralympic sport and subsequently groups particular athletes together to promote fair competition (IPC n.d.). Altogether, rehabilitative medicine created necessary formal organizations and procedures, raised funds, and articulated the movement’s lofty goals. In addition to institutional entrepreneurship, interview participants frequently described medical professionals volunteering in a number of roles necessary for the day-to-day operations of the Games and its teams, including classifiers, events staff, team assistants, and antidoping scientists.
Some interview participants named medical leaders as assets to the development of a sport logic (Gérard et al. 2017), while others were identified as obstacles. Tony is a disabled coach whose Paralympic teams competed in the 1980s. Tony named several doctors whom he claimed were allies to disabled athletes and the development of disability sport. However, Tony also drew attention to medical professionals who posed challenges to the development of disability sport because of their belief that sport endangered their patients’ health. Some rehabilitation professionals aided the development of Paralympic sport beyond its original rehabilitative orientation to a high-performance athletic model. In 1976, Strohkendl (1996) collaborated with athletes to develop a functional, rather than medical, system of athlete classification for wheelchair basketball. As I outline in my final empirical section, early medical classification rules relied on medical knowledge and diagnostic criteria, such as level of spinal injury, as definitive guidelines for evaluating disabled athletes’ physical capabilities. Meanwhile, functional classification systems categorized athletes on the basis of observed athletic abilities. In 1985, Strohkendl lobbied the ISMGF at the Symposium on Wheelchair Sport to implement functional classification and, furthermore, asserted that disabled athletes were the most qualified to determine their sports’ classification systems (Scruton 1998).
In general, participants expressed greater approval when discussing medical professionals serving in roles that were more circumscribed than governing or executive positions. Moreover, participants who held more positive views of medical Paralympic authority tended to be younger athletes who competed in the Games during the 1990s or later. Positive attitudes toward the role of medicine in the Paralympics correlate with diminished medical authority in the later Paralympic movement.
Paralympian Marginalization
Despite substantial benefits, Paralympic medicalization also resulted in adverse consequences. This section traces Paralympian marginalization as one such consequence. The early Paralympics’ medicalized institutional logic and medical governance restricted disabled agency within the early Paralympic Games. In conjunction with the medicalized framing of disability sport as rehabilitative therapy, prevailing medical leadership within Paralympic organizations reproduced hierarchical and often patronizing doctor-patient relationships between medical officials and disabled athletes. Many Paralympian participants reported that they were treated as passive clients, rather than elite athletes, through these roles. Furthermore, Paralympians contrasted medicalized views of Paralympic sport as rehabilitation against their own understandings of their sports as nonmedical, high-performance sport.
Bill competed in both Paralympic wheelchair racing and basketball in the early 1980s. He expressed concern that Paralympic organizational power was concentrated in the hands of medical professionals: Stoke Mandeville was really a top-down operation. The athletes were the recipients of a service. Everything about the sport was really driven by Guttmann and the committees of usually medical personnel. Teams and athletes really weren’t empowered to own the organization. (Bill)
Formal roles within the Paralympics’ governing bodies were predominantly occupied by physicians and other rehabilitative professionals. Three of the ISMGC’s six founding Executive Committee members—Ludwig Guttmann, Antonio Maglio, and Albert Tricot—were doctors, with Joan Scruton, Guttmann’s assistant, serving as secretary. The two remaining members were Michel Boubee of France and Captain Henrik Tjebbes of the Netherlands (Buckinghamshire Archives 1960b). Although individuals who were not medical doctors continued to be added to the Executive, the Presidency continued to be occupied by doctors. Furthermore, the creation of a Medical Committee constituted entirely by physicians in 1967 institutionalized medical influence within the Games (Buckinghamshire Archives 1967). The Executive Committee retained decision-making authority over other committees, while the Medical Committee and Technical Committee functioned as advisory bodies that proposed sport rules and regulations to be approved by the Executive Committee (Buckinghamshire Archives 1982b). The creation of sport subcommittees enabled athletes to make their way to the Technical Committee (Buckinghamshire Archives 1982a), though as I detail in the following section, athletes expressed that their recommendations were not seriously considered by the Executive. Moreover, Paralympians were sometimes punished for publicly speaking out against Paralympic standards. For instance, Guttmann personally issued what was intended to be a lifetime ban against Philip Craven from international competition in 1977 for voicing discontent with “the suitability of coaches” (Strohkendl 1996:22). Interview data suggest that Craven was reinstated in the late 1970s, after missing several international competitions, when Great Britain’s competitive standing declined in Europe, making him eligible for the 1980 Summer Games. Craven would later become the first president of the International Wheelchair Basketball Federation, the current international governing body for the sport, in 1993 as well as the first disabled president of the IPC in 2001 (IPC 2017; International Wheelchair Basketball Federation 2020). It was largely the medical profession, rather than disabled people or athletes, who led the early Paralympic movement. As such, Paralympians were constrained to compete in their nascent but rapidly evolving sports under the structures and regulations designed by medical management on their behalf.
The early Paralympics’ medically led organizational structure and rehabilitation sport logic (Gérard et al. 2017) reproduced the hegemonic doctor-patient roles on which the movement was founded. As previously outlined, medicine founded the Paralympic movement under the notion that sport functioned as rehabilitation for disabled people. Disabled athletes’ physical impairments and, furthermore, their possible welfare dependence were framed by Guttmann and the early Paralympic movement as medical problems (Goodman 1986). The preamble of the ISMGC’s founding constitution declared that the organization “recognises the immense value of sport for the physical and psychological rehabilitation of the paralysed, and above all its importance for the re-integration of disabled people into society” (Buckinghamshire Archives 1960b:1). Across various changes to the organization’s structure, the ISMGF maintained its constitution’s rehabilitative preamble into the 1980s (Buckinghamshire Archives 1982b). The ISMGF’s constitutional preamble was not merely symbolic, as older Paralympians reported treatment as passive clients in their interactions with Paralympic officials.
Matt, another wheelchair basketball player who competed in some of the SMG’s final annual iterations, stated that Paralympic officials governed the Games with a “caretaker mentality” and viewed themselves as “experts over” Paralympians. Similarly, Mark, a wheelchair racer and coach whose first Games were in the early 1980s, reported that medical officials did not always think of Paralympians as elite athletes: This is back in the ‘70s and ‘80s. . . they were always thinking about what was best for the medical treatment and care of the athlete and not “the athlete,” if you know what I mean. They were looking at [wheelchair racing] as therapeutic racing—what we were doing out on the track was therapeutic, and it was going to make our lives better. Yes, it did, but most of us were committed athletes. (Mark)
As Gérard et al. (2025) observed, such interactions made their way into the official organizational record. At ISOD’s 1979 general assembly, a blind Danish delegate asked Guttmann whether ISOD was an organization of disabled people or an organization for disabled people. Citing his historic work for disabled people, Guttmann told the delegate to sit and keep quiet. In a 1981 ISMGF Executive Committee meeting, Joan Scruton claimed that it was the organization’s “task to look after the interests of spinal cord injured people” (Buckinghamshire Archives 1981b:5). In Parsonian terms, Paralympians were expected to adopt the “sick role” and follow medical directives (Parsons 1951). However, Paralympians rejected the sick role and critiqued organizational dynamics that they characterized as fraught with medical paternalism (Chin 2002).
Paralympians contrasted medical leadership’s framing of disability sport as rehabilitative therapy against their own experiences competing in disability sport as high-performance sport. Nathan, a wheelchair rugby player who began his Paralympic career in the early 1980s, contrasted the institutionalized rehabilitation sport logic (Gérard et al. 2017) against his experience competing in the Games: It was fundamentally based on the medical model
4
—that participating in wheelchair sports would promote good health. . . I mean, that goes all the way back to Stoke Mandeville. And then in the ‘70s and into the ‘90s, I helped evolve it into, “These are sports teams. This is an athletic pursuit. These are just athletes, not patients that we’re treating with adaptive sport and recreation.” (Nathan)
Although Paralympic leadership framed disability sports as medical therapy and cast Paralympians as patients, Nathan firmly maintained that Paralympians were elite athletes engaged in high-performance sport. These findings further evidence Brady’s (2023) claim that medical professionals and athletes held divergent interpretations of disability sport. Notably, Nathan’s claim that his athletic career contributed to the shift away from the Paralympics’ rehabilitation sport logic and toward its current sport logic (Gérard et al. 2017) suggests that Paralympian agency aided this institutional transformation.
Paralympic medicalization left little room for Paralympians to lead the Paralympic movement, govern their sports, or be seen as elite athletes. The Games’ formal medical hierarchy marginalized Paralympians, who were framed as patients, or at best passive clients, and subordinated them to medical management. This functioned to restrict disabled athletes’ abilities to self-govern the Paralympic Games. But not all Paralympians disapproved of medical leadership. Ethan, a track and field athlete whose first Games were in the mid-1970s, stated that Guttmann had to act as an autocrat to successfully mobilize the movement. Nonetheless, Ethan felt that Paralympians deserved greater control of the Paralympic Games by the 1970s but did not believe Guttmann envisioned disabled leadership in the movement’s future. Conflicts subsequently arose between Paralympians and medical leadership over athlete classification and wheelchair technology because of these framing differences.
Limitations to Disability Sport Development
Paralympic medicalization also restricted efforts to expand Paralympic sport and advance athletic standards beyond SCI rehabilitation. Following the 1988 Summer Paralympics in Seoul, the Sports Co-ordinating Committee issued the following statement tracing the evolution of the Paralympic Games (Buckinghamshire Archives 1988): In the early history of Stoke Mandeville Wheelchair Games when just a few sports were offered for competition, there was little attention paid to the exact rules of sport. The main idea was to encourage rehabilitation through recreational activities and later through a greater appreciation of competitive sports. . . However, as the athletes desired greater similarity with the non-disabled Sports Federations, many problems over the rules developed. (p. 13)
As the Paralympic movement progressed, a group of entrepreneurial athletes and their allies sought to advance Paralympic sport beyond mere therapeutic activity reserved for SCI patients. Specifically, these institutional actors desired to alter sport regulations to expand Paralympic eligibility to a wider range of impairment groups and tailor equipment for improved athletic performance. Regular conflict arose between athletes and governing Paralympic officials regarding athlete classification and wheelchair design. Athlete classification proved especially contentious for wheelchair basketball, while wheelchair design disputes tended to play out in wheelchair racing.
Medical Classification
Medical professionals developed early Paralympic classification based on diagnostic criteria. This medical approach to classification restricted Paralympic eligibility to only certain diagnoses and prevented athletes with different diagnoses from competing in the same events for team sports. Initially, the Paralympic Games organized disability sport exclusively for individuals with SCIs. In 1960, following the Trainers’ Meeting recommendation to exclude athletes with incomplete spinal lesions entirely, Guttmann instead directed the ISMGC Executive Committee to instruct national teams’ doctors and team leaders to prioritize athletes with more severe spinal lesions. (Buckinghamshire Archives 1960a). Athletes held medical identity cards signed by neurological specialists for Paralympic eligibility (Buckinghamshire Archives 1966). All sports classified athletes for competition by level and completeness of SCI (i.e., the location in the spinal column where damage occurred and the extent of said damage) (Buckinghamshire Archives n.d.).
Disabled athletes with other types of impairments were deemed eligible for Paralympic competition in incremental stages (Buckinghamshire Archives 1970b, 1973). Amputee, blind, and visually impaired athletes first competed in the Paralympics at the 1976 Winter Games in Örnsköldsvik, Sweden—the inaugural winter Games, which notably included no athletes with SCIs. Athletes with cerebral palsy joined Paralympic competition at the 1980 Olympics for the Disabled in Arnhem, Netherlands. “Les autres,” a term used to encompass all remaining motor impairments, were finally incorporated in the 1984 Winter Paralympic Games in Innsbruck, Austria (Brittain 2012). However, the inclusion of other impairment groups was marked by repeated medical concern for preserving opportunities for individuals with the most severe SCIs. Guttmann clarified that while other impairment types would be included in the Games, they should not mix with SCIs for competition. As such, amputees would not be included in Paralympic wheelchair basketball, despite their inclusion in national-level wheelchair basketball competition in the United States and other countries (Buckinghamshire Archives 1978).
The exclusion of athletes with non-SCI physical impairments, such as amputations or cerebral palsy, from ISMGF competition continued well into the 1980s. Bill explained that athletes with other impairment types were believed to have “an athletic advantage” over the spinally injured population. This proved especially contentious for wheelchair basketball. At the national level, wheelchair basketball was historically contested by teams composed of athletes across a range of physical impairments (Strohkendl 1996). Although it was understood as ISOD’s responsibility to organize competition for other impairment groups (Buckinghamshire Archives 1970a), the ISMGF maintained firm control over Paralympic wheelchair basketball and excluded non-SCI athletes from competition. The exclusion of certain athletes on the basis of diagnosis hamstrung the growth and development of Paralympic wheelchair basketball.
In 1981, the ISMGF’s Basketball Sub-Committee petitioned the Executive Committee to include other impairment groups in ISMGF wheelchair basketball. Council representatives expressed concern that basketball would open the floodgates for other sports to integrate other impairment groups as well, which they feared would destroy the Games’ integrity and mission (Buckinghamshire Archives 1981a). Despite a nearly unanimous vote of approval from the wheelchair basketball community in Geneva and the support of 20 participating nations (Buckinghamshire Archives 1982a), the petition was unanimously rejected by Stoke Mandeville’s Medical Committee and by a majority of the Technical Committee. Stan Labanowich, the Basketball Sub-Committee’s chair, asserted that “the players and not the medical doctors” should decide their sport’s regulations. Strohkendl followed by presenting his system of “functional classification,” whereby other impairments could be classified along SCIs through a series of functional tests (Buckinghamshire Archives 1982a:18). Despite the Executive’s shifting perspectives on classification and talks of implementing Strohkendl’s functional classification ahead of the 1984 International Games for the Disabled, two factors prevented integration until the 1988 Paralympics: the geographic separation of segregated events by impairment group (Brittain 2012) and a required constitutional amendment (Buckinghamshire Archives 1984). In 1985, the ISMGF acknowledged that their exclusion of non-SCI athletes led to a decline in the standards of Paralympic wheelchair basketball competitions relative to national-level competitions (Buckinghamshire Archives 1985). Even after the 1984 Games, the ISMGF Executive continued to resist the Sport Subcommittees’ desire to alter the organization’s philosophy to integrate classification to include all locomotor impairments (Buckinghamshire Archives 1986).
Wheelchair Regulations
Paralympic medicalization also constrained the evolution of sports wheelchairs from previous rehabilitative designs. Wheelchair designs now vary by sport, but this section focuses on the development of the racing wheelchair. In its first Executive Committee meeting, the ISMGC introduced wheelchair racing as an event to “help the public understand the possibilities of paraplegics for work” and determined that a standard wheelchair was necessary for competition (Buckinghamshire Archives 1960a:2). Wheelchair technology varied widely between participating countries, prompting officials to institute wheelchair regulations out of concern for technological parity and competitive fairness. However, early Paralympic wheelchair regulations were often ill suited for high-performance competition. Paralympians expressed desire for wheelchair modifications to enhance both athletic performance and athlete safety. Yet Paralympians described Paralympic leadership as reluctant to adopt athlete-driven design innovations in preference for standard rehabilitative designs. Because disputes over racing wheelchair design did not appear in archived organizational records, I instead rely on interview data and secondary accounts to construct a historical account.
Paralympic wheelchair regulations largely mimicked existing rehabilitative designs commonly found in the rehabilitation hospitals that teams initially emerged from. For instance, the ISMGF’s 1979 regulations required that wheelchairs have two large wheels and two small wheels, no steering devices, and limited wheel cambering to just 2° (Buckinghamshire Archives 1977). Today, racing wheelchairs have three wheels, a steering compensator, and cambering over 2° (Cooper and De Luigi 2014). The ISMGF’s wheelchair regulations were largely inspired by the folding Everest & Jennings wheelchair, a massively popular rehabilitative design still used in hospitals (Brady 2023). The ISMGF made clear in 1981 that it did not support the perspective that wheelchairs were sports devices. When arguing against the inclusion of amputees in basketball, the Executive Committee protested that “to put people whose disability did not require the use of wheelchairs into wheelchairs just to do sport was making the wheelchair a kind of sports device” (Buckinghamshire Archives 1981b:2). As athletes began racing longer distances and seeking ways to improve their performance, they began to modify the standard Everest & Jennings design.
Paralympians sought to modify their rehabilitation wheelchairs into specialized sports equipment. Some participants reported experimenting with their wheelchair’s design for improved performance, often using hacksaws and blowtorches in their personal garages. Athletes described an extensive list of modifications to wheelchairs for racing, including: three-wheeled T-frames, steering compensators, cambered wheels, rigid lightweight frames, sagged upholstery, smaller wheel push rings, larger front wheels, custom-fitted dimensions, and the removal of unnecessary parts such as push handles and foot plates. Although legal for use in independent road races, including major marathons, and national-level events, the wheelchairs that athletes modified for competition were often prohibited at the Paralympic level.
In particular, the adoption of the steering compensator proved a significant point of contention between American wheelchair racers and ISMGF officials. The compensator is a device used in racing wheelchairs that athletes activate to push their wheels on turns without manually turning their wheelchairs. Developed in the United States, the compensator was widely permitted at American road races but was initially banned in Paralympic competition. Mark described frustration with ISMGF officials over the prohibition of compensators: Prior to 1989, you were not allowed to race with the compensator, or steering. And the ISMGF, in their wisdom, outlawed steering handles because they felt pushing a wheelchair around a turn at 15 miles an hour was a skill activity. It was actually getting people hurt. . . Anyways, that was something that was developed in the US, the compensator. And we were using it at road events, and nobody said anything. And we used it at American events, and it was okay. But when we got over to Europe, it wasn’t allowed. And they fought us tooth and nail on that. (Mark)
Mark felt that medical leadership’s restrictions on racing wheelchairs not only hindered athletic performance but also posed danger to athletes. Throughout interviews, Paralympians contrasted restrictive medicalized rules at Stoke Mandeville against more liberal rules used in the United States. Bill explained that had athletes been in greater positions of power within the Paralympics, regulations on wheelchair specifications would have been updated more quickly. Despite their medical expertise, medical professionals were characterized by older Paralympians as problematic leaders of the early Paralympic movement who did not fully understand the technical aspects of the sports that they governed. However, not all Paralympians who competed in the early Games reported conflict with ISMGF leadership. Although other Paralympians, whom he identified as Americans from wheelchair basketball, regularly fought with Stoke’s Executive Committee, Ethan stated that he was able to codify changes to his sport without conflict. Ethan contrasted his approach to Paralympic “evolution” against the “revolution” advocated for by American basketball players.
Discussion and Conclusion
Multimethod analysis of interviews with Paralympic athletes and coaches and primary historical materials sourced from Paralympic organizations reveals that medicalization both catalyzed and hamstrung the progression of the Paralympic movement. Medicalization enabled the emergence and continuity of the Paralympic movement through lifesaving medical treatment and movement building. Yet medicalization also marginalized Paralympians within Paralympic organizations, restricted Paralympic eligibility for much of the disabled population, and posed challenges to the development of specialized sports wheelchairs from previous rehabilitative designs. This ultimately inhibited athletes’ efforts to pursue nonmedical, elite, competitive sport. These findings demonstrate how medicalization enables medical control beyond individuals’ bodies and behaviors, implicating social movements, cultural production, and cultural practices defined as rehabilitative. These risks may be heightened in contexts where particular groups, such as disabled people, are more easily cast in the sick role (Parsons 1951). These findings also advance an ambivalent understanding of medicalization as a double-edged sword (Blum 2015; Mauldin 2016; Reissman 1983).
Empirical findings contribute to literature on disability sport and Paralympic history. Although scholars frequently note the Paralympics’ medicalized origins in rehabilitative therapy for individuals with SCIs (e.g., Brittain 2012; Gérard et al. 2017, 2025; Legg and Steadward 2011), the effects of Paralympic medicalization have received insufficient empirical attention. Moreover, Paralympic research tends to exclude the perspectives and experiences of Paralympians (Peers 2009). This research fills this critical gap by presenting the effects of Paralympic medicalization as reported by Paralympians. The findings coincide with and expand Paralympian scholars’ autobiographic work that called attention to imbalanced Paralympic power relations (Howe 2008; Labanowich and Thiboutot 2011; Peers 2009). This study incorporates disability sport within broader medicalization research and stimulates inquiry into other underexplored arenas of medicalization.
Interviews with Paralympians also confirm that the Games’ shift away from a rehabilitation sport logic was not only the product of macro-level forces but also a bottom-up process in which disabled athletes’ transformation of sporting practices pushed the institution in novel directions (Gérard et al. 2017). How Paralympians contributed to the displacement of the Paralympics’ founding rehabilitative institutional logic may interest scholars concerned with social movements’ internal power dynamics, institutional change, and tensions between structure and agency.
At the theoretical level, this research advances the sociology of disability by calling sociological attention to the social and political dimensions of disability. Despite significant contributions from disability studies, sociology as a discipline tends to treat disability primarily as socially deviant or biologically deficient (Mauldin and Brown 2021; Thomas 2004, 2007). Additionally, this study illustrates how conflict between the medical and social models of disability unfolds within institutions. Furthermore, this study demonstrates the practical consequences for disabled people that emerge from conflict between contrasting models of disability.
The effects of Paralympic medicalization noted in this article are characteristic of expanding medical control (Conrad 2007). Tracing restricted autonomy within social movements, cultural production, and cultural practices as consequences of medicalization provide useful theoretical perspectives for social work, social movements, sociology of the body, kinesiology, and cultural studies literature. In particular, medicalization’s bodily limitations and restrictions on cultural autonomy may be portable to comparable cases such as conflict between modern and traditional medicine over jurisdictional authority, deafness and sign language, and disabled art. Moreover, findings contribute to key debates within the sociology of professions, particularly discussions of professional dominance and jurisdictional claims (Freidson 1970). The findings also speak to central concerns in the sociology of knowledge regarding the social construction of scientific knowledge and the limitations of expert knowledge in relation to lived experience (Brown et al. 2010; Epstein 1998). More broadly, this study speaks to overarching debates regarding the appropriate level of medical involvement in culture, society, and the lives of individuals.
Footnotes
Acknowledgements
I would like to thank Amanda McGrory and the U.S. Olympic and Paralympic Museum for assisting this study’s recruitment as well as my participants for their commitment and enthusiasm. I also thank Danielle Peers for assistance with interview protocol design. Additionally, I thank Drew Halfmann, Joss Greene, and Nora Groce for their constructive feedback on drafts of this article, as well as my research assistant, Shvata Malhotra, for helping clean automatic transcripts. Lastly, I thank the anonymous reviewers for their highly useful and constructive feedback.
Correction (October 2025):
This article was updated from initial publication to remove a reference that was not ultimately included in the study’s data sample.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the University of California-Davis’ Dean’s Distinguished Graduate Fellowship and Dissertation Year Fellowship.