
Abstract
Individuals with disabilities are likely to be doubly disadvantaged, as they tend to earn less but require more financial resources than individuals without disabilities to maintain an average standard of life. Exploring the links between early-life disabilities and income attainment in adulthood requires high-quality data that allow accounting for selection into disability as well as a comprehensive list of predictors of income attainment. The authors harness the power of Norwegian register-based data and inverse-probability weighting regression adjustment estimators to examine whether individuals born with or who acquire disabilities in early life have lower income attainment at age 32 than individuals in the general population of the country. The results are robust to alternative estimation specifications and suggest that early-life chronic health conditions, such as asthma and diabetes, and impairments, such as sensory loss and physical impairment, are associated with significantly lower income attainment even when individuals’ actual working hours are accounted for among those employed.
Studies from across countries and disciplines consistently demonstrate that disabilities are linked to poorer life outcomes, such as lower educational attainment, reduced employment prospects, limited intergenerational mobility, and diminished life satisfaction (Chatzitheochari, Velthuis, and Connelly 2022; Gugushvili et al. 2024; Heymann, Wong, and Waisath 2022). Many individuals experience congenital disabilities, such as chronic health conditions or impairments, or acquire them in early life, and these conditions, shaped by socioeconomic origins, can profoundly influence their later life trajectories (Bowen and González 2010; Chatzitheochari et al. 2022; Cohen et al. 2010; Emerson and Llewellyn 2021; Simkiss et al. 2011). The theory of social determinants of health highlights this interplay, suggesting that socioeconomic position in childhood affects the likelihood of early-life disability, which in turn affects adult outcomes such as income (Krokstad and Westin 2004; Leinonen, Martikainen, and Lahelma 2012; Marmot and Bell 2019). Analyzing these relationships requires accounting for the nonrandom distribution of disability, where parental socioeconomic disadvantages increase the probability of childhood disability, alongside social barriers like stigma, inadequate institutional support, and discrimination that further exacerbate inequalities (Bunbury 2019; Østerud 2023).
Even if educational, occupational, and income disparities were eliminated, evidence from the United States and Europe indicates that households with a disabled adult need approximately 30 percent more income to offset disability-related costs (Morris et al. 2022; Morris and Zaidi 2020). Yet far from earning more, individuals with disabilities typically face labor market disadvantages, including lower employment rates, prolonged unemployment, poorer job quality, and reduced working hours, resulting in lower earnings than their nondisabled peers (Amin et al. 2023; Banks, Kuper, and Polack 2017; Maroto and Pettinicchio 2014; Meyer and Mok 2019; Saatcioglu and Skrtic 2019). This dual burden, earning less while needing more, positions individuals with disabilities as doubly disadvantaged, raising critical questions about economic equity and the adequacy of support systems in modern societies.
Such persistent disparities challenge the effectiveness of welfare states in reducing disability-based inequalities, particularly in income attainment. Research on low- and middle-income countries links disability and poverty to inadequate welfare provisions (Banks et al. 2017; Rudra 2007), but more research in this regard is also required about advanced welfare states in the Global North. Social-democratic nations such as those in northern Europe, including Norway, prioritize labor market integration through early health interventions, inclusive education, antidiscrimination regulations, disability-friendly employment opportunities, occupational rehabilitation, and adapted infrastructure (Movahed 2023; O’Brien 2015). These measures aim to equalize opportunities and outcomes, yet evidence of their success in narrowing income gaps remains scarce (Ballo 2023; Gugushvili et al. 2024), especially when accounting for early-life disabilities’ long-term effects. This gap is particularly puzzling in Norway, a welfare state with equitable income distribution but notable health disparities, dubbed the health inequality paradox (Mackenbach 2012).
Despite robust welfare frameworks, prior studies fall short in rigorously assessing whether early-life disabilities, such as sensory loss or physical impairments, independently reduce income attainment in adulthood. Survey-based research often lacks sufficient samples of rare conditions (e.g., the low prevalence of cerebral palsy among newborns), provides unreliable income data (Brewer, Etheridge, and O’Dea 2017), and rarely adjusts for selection into disability due to socioeconomic origins. Our study fills this void by asking, how do early-life disabilities affect income attainment in adulthood in Norway, net of selection and key predictors such as education and work intensity? Using high-quality Norwegian register data and inverse-probability weighting regression adjustment (IPWRA), we examine this question, offering a novel test of welfare state efficacy in a context designed to maximize equality of opportunity (Mackenbach 2019).
Framework
Conceptualizing Disability
Disability is a complex concept, interpreted through diverse theoretical lenses that shape how it is studied and understood. Since the nineteenth century, the default model of most industrialized societies has arguably been a “medical model” which explains disability as the consequence of individual health conditions or impairments (i.e., a biological deficit that is best remedied through diagnosis, treatment, or accommodation) (Oliver 1990; Oliver and Barnes 2012; Retief and Letšosa 2018; Stiker 2019). From the 1980s onward, however, interdisciplinary research on disability has explored the significance of societal barriers, such as inaccessible environments, discriminatory attitudes, or exclusionary policies, as well as other cultural and psychological-relational factors that contribute to disablement (Shakespeare 2013; Thomas 2004).
To the extent that there is a consensus, disability is recognized to be a multicausal, multidimensional phenomenon that Shakespeare (2013) termed a “predicament.” Consequently, a hybrid approach was adopted, wherein the tangible reality of impairments is acknowledged along with the social contexts that amplify their effects, offering a nuanced understanding of disability as both embodied and socially constructed (Anastasiou and Kauffman 2013). Furthermore, it is important to recognize that what constitutes an “impairment” is, in part, a question that is informed by diagnostic systems and conventions.
This study adopts such a hybrid perspective, recognizing the predicament of disability as the result of the interplay between individual conditions and the broader societal landscape. Rather than isolating disability as a purely medical phenomenon, we consider how social structures, such as economic opportunities, institutional support, and cultural norms, interact with physical or chronic conditions to influence life outcomes (Zaks 2024). This approach acknowledges that although impairments may originate in biology, their consequences are mediated by external factors like access to resources, stigma, or systemic inequities. It also recognizes that although disablement consistently correlates with impairment, the degree of disablement and marginalization is, in principle, highly variable. By blending these models, we aim to capture the dual nature of disability: a personal experience shaped by tangible limitations and a social phenomenon influenced by the environment.
In line with this perspective, we consider both early-life chronic health conditions (such as asthma and type 1 diabetes) and impairments (such as sensory loss and physical disabilities) under the broad category of disability. Although chronic health conditions and impairments are distinct in terms of their medical classification, both can impose long-term limitations on individuals’ educational and occupational trajectories, leading to comparable socioeconomic disadvantages. To reflect this conceptual overlap, we interchangeably refer to these conditions as early-life chronic health conditions and impairments or simply disabilities throughout this article. This framing aligns with disability studies’ call to examine both the lived realities of individuals and the structural forces that shape their opportunities, providing a foundation for exploring economic inequalities in a welfare state context (Goodley 2024).
A Welfare State and Disability-Based Inequalities
Welfare state theories suggest that comprehensive social-democratic systems, such as those in Scandinavia, should be particularly effective in equalizing life opportunities for individuals with disabilities (Dominko and Verbič 2021; Hadjar and Kotitschke 2021). Esping-Andersen’s (1990) path-breaking typology of welfare regimes laid the foundation for understanding cross-national differences in social protection, classifying welfare states into liberal, conservative-corporatist, and social-democratic models on the basis of their redistributive capacity and decommodification levels. His work sparked extensive scholarly debate, with subsequent research exploring the extent to which these welfare regimes mitigate social inequalities, including those related to disability (Arts and Gelissen 2002; Ferragina and Seeleib-Kaiser 2011; van der Zwan and de Beer 2021).
Although social-democratic states are expected to provide stronger safety nets and labor market inclusion measures, critiques have highlighted that their universalistic policies may insufficiently address the distinct barriers faced by individuals with disabilities (Böheim and Leoni 2016; OECD 2010; Scharle, Váradi, and Samu 2015). Moreover, empirical evidence suggests that Scandinavian welfare states do not necessarily outperform other European countries in reducing disability-based disparities in income and labor market participation (Gugushvili et al. 2023). These findings challenge the assumption that generous welfare provisions alone are sufficient to equalize opportunities in life, emphasizing the need for more targeted policies to address the structural disadvantages experienced by individuals with disabilities. Furthermore, the long-established social-democratic policy goal of participation in society, echoed by the more recent United Nations Convention on the Rights of People with Disabilities, is ambiguous in that it is arguably directed at a minimum of participation rather than equality in valued outcomes (Grue 2019).
One area of policy that should equalize conditions for individuals with and without disabilities, including income attainment, is the widespread adoption of legal provisions against disability-based discrimination, reflecting the general shift toward a human rights model of disability (Degener 2016). The 2008 Anti-Discrimination and Accessibility Act of Norway strengthened protections in employment and education, accompanied by increased investments in inclusive education and vocational training. However, despite these commitments, evidence suggests that disability-based inequalities and perceived discrimination persist (Gugushvili and Grue 2025). Research indicates that Norwegian employers are 48 percent less likely to respond to job applications from individuals who use wheelchairs (Bjørnshagen and Ugreninov 2021). Comparative studies further show that Norway does not consistently outperform other European countries in securing better employment outcomes for individuals with disabilities (Gugushvili et al. 2023).
A central feature of Norway’s welfare state is its two-tiered system of disability-related benefits, which includes both income replacement and compensatory support. The Work Assessment Allowance and the Disability Pension (Uføretrygd) provide financial assistance for those unable to work because of long-term health conditions, ensuring basic income security (Bråten and Sten-Gahmberg 2022). Additionally, the Basic Benefit (Grunnstønad) and the Attendance Benefit (Hjelpestønad) offer compensation for additional costs related to disabilities, such as medical expenses, assistive devices, and personal assistance (Kristensen et al. 2021; Weber 2018). Beyond financial support, Norway has activation policies aimed at integrating people with disabilities into the workforce. Programs such as Work Preparation Training (Arbeidsforberedende Trening) and Permanently Adapted Work (Varig Tilrettelagt Arbeid) provide vocational training and subsidized employment (Gjertsen 2021; Nossen 2023).
Despite the described disability-related provisions, a recent study using Norwegian register data highlights that individuals with early-life disabilities are significantly less likely to experience intergenerational upward mobility, as measured by income tertiles (Gugushvili et al. 2024). However, the latter study does not clarify the observed inequality and does not elaborate on what the contributing factors of the disability gap in income attainment are. To provide answers to the latter questions, it is important to account for the nonrandom distribution of individuals in disability categories, as individuals’ initial socioeconomic position might be a significant predictor of whether they have or do not have disabilities (Cummings et al. 2018; Delobel-Ayoub et al. 2022; Van Kerschaver et al. 2013). On the other hand, conventional explanations of income attainment in adulthood, such as individuals’ social origins, educational attainment, type of employment, working hours, and the contextual characteristics of a place of residence, should be accounted for. In the present study, using high-quality register data from Norway, we explicitly consider selection into disability, on the one hand, and also account for various factors why individuals with disabilities might be disadvantaged in income attainment in their adult lives, on the other hand.
The Role of Socioeconomic Selection in Disability
One of the reasons why individuals with disabilities in early life can have lower incomes in adulthood is that their socioeconomic position already in early life could have been worse than the socioeconomic position of individuals without disabilities (Bowen 2009; Emerson and Llewellyn 2021). Early life socioeconomic position, in turn, is directly linked with later life educational, occupational, and income attainment (Andrade and Thomsen 2018; Mulder et al. 2009) and with the likelihood of having worse health outcomes and the risk for becoming disabled (Cohen et al. 2010; Laditka, Laditka, and Hoyle 2021). The latter implies that both early-life disabilities and later life outcomes could be affected by characteristics from individuals’ initial years of life.
There is compelling evidence on the role of initial socioeconomic position in specific childhood disability outcomes. For instance, an association was demonstrated between various measures of parental socioeconomic position and hearing impairment of newborns in Belgium (Van Kerschaver et al. 2013). The overall cumulative incidence of visual impairment was higher among British children with parents in the lowest quintile of socioeconomic status (Teoh et al. 2021). The analysis of Canadian data suggests that families’ socioeconomic marginalization was linked to children’s adverse outcomes related to type 1 diabetes mellitus (Cummings et al. 2018). Another study from France showed that the prevalence of children with cerebral palsy was significantly higher in the most deprived tertile of residence, while children with cerebral palsy and preterm birth history had more severe forms of motor impairment if they lived in the most deprived areas of the country (Delobel-Ayoub et al. 2022).
But what are the mechanisms behind the association between early life socioeconomic position and disability conditions? The greater resources of more advantaged families can mitigate the risk for disability development or reduce the severity of disability conditions if children inherit or acquire them in the first years of life. The specific channels linking socioeconomic position and disability outcomes among children are not dissimilar to the predictions of the fundamental cause theory of health inequalities, in general (Phelan, Link, and Tehranifar 2010), and their comprehensive illustration through type 1 diabetes treatment regimens among advantaged and disadvantaged individuals in the United States, in particular (Lutfey and Freese 2005). In addition to significant links between socioeconomic origin and disability-related outcomes among children, origin socioeconomic conditions also have a direct effect on outcomes in adulthood in relation to, among other aspects of life, educational, occupational, and income attainment (Ballarino, Cantalini, and Panichella 2020; Gugushvili et al. 2017). The latter is the reason why both the selection into disability and origin socioeconomic characteristics should also be accounted for when estimating later life outcomes, such as income attainment.
Determinants of Income among Individuals with Disabilities
Incomes among individuals with disabilities can be disaggregated by labor market earnings and other types of income, such as disability benefits. For the majority of individuals, labor market earnings are the most important component of their incomes. In turn, according to the human capital model, earnings from the labor market are significantly affected by individuals’ education and experience (Arcidiacono, Bayer, and Hizmo 2010). The latter suggests that if individuals with disabilities attain lower levels of education or accumulate less work experience, as shown in numerous studies (Ballo 2020; Laditka and Laditka 2016), the level of their earnings will be lower than what is observed in the general population.
In addition to potentially lower levels of educational attainment and accumulated experience, individuals with disabilities also have a lower likelihood and intensity of market work (Ballo 2023; Shandra 2018). The existing estimates suggest that across European societies, the gap in the levels of employment between individuals with and without disabilities varies between 10 and 42 percentage points, with some of the highest inequalities observed in Denmark, the Netherlands, and Austria for women and Sweden, the Netherlands, and Denmark for men (van der Zwan and de Beer 2021). If labor market earnings are not supplemented with other types of income, such as welfare and disability benefits, then individuals with disabilities are expected to have lower incomes. In addition, lower intensity of market work also implies that even when they are employed, individuals with disabilities are more likely to have part-time jobs and work shorter hours than individuals in the general population (Barnay 2016).
For instance, in the United States, the analysis of data on people with visual impairments suggests that they were more likely than people without visual impairments to work part-time (McDonnall, Cmar, and McKnight 2022). Another study from the same country indicates that men and women with disabilities reported spending 321 and 289 fewer minutes on work daily than those in the general population (Anand and Ben-Shalom 2014). In addition to human capital and work intensity perspectives, the direct effect of social origins should also be accounted for in estimating the income attainment of individuals with disabilities. Having children with disabilities over prolonged periods of time might reduce the parents’ incomes, which, in turn, through various channels, can negatively affect individuals’ position in the income hierarchy (Wondemu et al. 2022). Early-life disabilities can also have an important effect on individuals’ family life, for instance, in relation to their marital status, which in turn can affect income outcomes (Brown and Clark 2017). Furthermore, the type of settlement where individuals reside can provide different opportunities for income attainment (Sage et al. 2019), and therefore, it should be accounted for in empirical estimations of disability-related income inequality.
To reiterate, the main goal of the study is to test if individuals with early-life disabilities are disadvantaged in income attainment in adult life even when nonrandom allocation in disabilities and a comprehensive list of predictors of income attainment are accounted for.
Methods
Data
To explore the income of individuals with early-life disabilities in Norway, we study those born from 1977 to 1995 who had at the time of birth or acquired the conditions described later by age 15 and who were alive by the time data were accessed in 2021 (4,316 individuals with fully available information). We compare the latter individuals’ outcomes with a randomly drawn sample of the country’s general population, 13,198 born in the same period. Among individuals with disabilities, we differentiate between those with chronic health conditions, such as asthma and type 1 diabetes mellitus, and impairments, such as sensory loss in vision and hearing, and physical impairments (e.g., cerebral palsy). Because of the small number of individuals with vision loss in our sample, with about 3 percent of all cases, we combined this condition with individuals who had hearing loss and referred to this disability category as sensory loss.
The individuals with the listed early-life chronic health conditions and impairments have been identified through the register of the Norwegian Labour and Welfare Administration of disability benefits recipient families who had a child with one of the considered conditions. In the country’s welfare system, family members may apply for benefits to compensate for the extra care needed and/or expenses related to a child’s disability. Having a disability in this context refers to individuals’ medical conditions related to a permanent injury, illness, or functional impairment that individuals experience. The level of benefits depends on the extent of extra care or assistance the child needs or the additional expenses the families have due to existing chronic conditions and disabilities. The level of the family’s income and wealth is not taken into account when disability benefits are granted to individuals.
The data we accessed do not cover all early-life disabilities that might affect individuals’ later life income attainment. The main reason why we concentrate on the described chronic health conditions and impairments is that the procedures for qualifying for disability benefits have largely remained constant for the considered disabilities, while the procedures for other types of conditions and impairments, especially those related to individual mental health, have been changing over time. Therefore, we focus on individuals’ chronic health conditions and impairments diagnosed in early life that did not experience major changes over time regarding qualifying conditions for disability benefits. These conditions also represent some of the most prevalent disabilities found in the Global North, including in Norway.
Selection into Disabilities
On the basis of insights from research on socioeconomic determinants of health and disability among children (Hunter and Flores 2021), we explicitly account for selection into chronic health conditions and impairments by considering parental characteristics that could be linked to a higher risk for children having these disabilities (Alfaro Hudak et al. 2023; Holst et al. 2020; Jahan et al. 2021; Mönkemöller et al. 2019; Zhang et al. 2024). Considering the process of selection is important because the same factors that potentially affect children’s disabilities might also influence their latter-life socioeconomic outcomes, including income attainment (Bulczak et al. 2024; Chatzitheochari et al. 2022; Gugushvili et al. 2021). Therefore, we account for parental socioeconomic characteristics in the first years of individuals’ lives, specifically at age 4. We mainly use parental characteristics at age 4 because 1981 is the first year information about important parental characteristics becomes available in the accessed register data.
On the basis of the insights from social learning theory on gendered intergenerational transmission of various inequalities, it is important to consider mothers’ characteristics separately from fathers’ characteristics (Beller 2009; Hout 2018; Wainwright and Watts 2021). We first account for separately fathers’ and mothers’ educational attainment. The latter are the categorical variables operationalized with four distinct levels of attainment: (1) primary and lower secondary, (2) upper and postsecondary, (3) tertiary, and (2) postgraduate education. We also consider separately individuals’ fathers’ and mothers’ income as predictors of children’s risk for having chronic health conditions and impairments. More specifically, we divide fathers and mothers into income deciles and observe the relative paternal and maternal standing compared with other men and women. This procedure gives us information for everyone in the diagnosed and general population groups about an income decile to which their parents belonged.
Income Attainment in Deciles
We use a relative measure of income attainment as the main outcome variable in this study. For each individual in our analytical sample, we divide men’s and women’s incomes at age 32 into deciles and observe their relative standing compared with other men and women at age 32. We acknowledge that age 32 is a relatively early stage in the life course to measure lifetime income attainment, yet measuring income later significantly reduces the number of individuals available for our analysis.
We operationalize income attainment using deciles rather than the log of income for several reasons. First, income deciles provide a relative measure of socioeconomic positioning, allowing meaningful comparisons between individuals with and those without early-life disabilities within the overall income distribution. Second, this approach reduces the influence of income outliers, which are particularly prevalent in administrative earnings data, while ensuring greater interpretability in the context of policy research. Third, given that we account for selection into disability using parental socioeconomic characteristics (also measured in income deciles), this choice maintains conceptual and methodological consistency throughout our analysis. As our focus is on inequality rather than absolute differences in income, income deciles provide an appropriate and policy-relevant metric for evaluating disability-based disparities in economic attainment.
Predictors of Income Attainment
Apart from individuals’ early-life chronic conditions and disabilities, which we regard as treatments that affect the level of income in adulthood, there are a number of important predictors of income attainment that we account for in our estimation strategy (Bick, Fuchs-Schündeln, and Lagakos 2018; Cheng and Song 2019; Pensiero and Barone 2023; Bulczak and Gugushvili 2022). To mitigate the concerns related to reverse causation (i.e., outcome measure affecting explanatory variables), all considered characteristics for explaining variation in income attainment at age 32 derive from earlier stages in individuals’ life course. First, parental variables are measured at the individuals’ age of 15 because this is close to the period when adolescents in Norway complete mandatory primary and lower secondary education and make consequential transitions to upper secondary education by competing for a place in their preferred study program on the basis of their grade point average or alternatively exit the educational system (Haugan, Frostad, and Mjaavatn 2019). As for individuals’ own predictors of income attainment, we measure their characteristics at the individuals’ age of 30, 2 years earlier in the life course, when the decile position in the income hierarchy is estimated.
For parents, we account for four separate variables: fathers’ education and mothers’ education, both measured with the attainment of primary and lower secondary, upper and postsecondary, tertiary, and postgraduate education; and fathers’ income and mothers’ income, both measured in deciles in relation to other men and women. These social background characteristics are important predictors of individuals’ income attainment in adulthood, as shown in, for instance, the analysis of high-quality register data from Sweden and Denmark (Harding and Munk 2020; Thaning 2021).
For individuals’ own characteristics, we consider their education level measured similarly to their parents with the attainment of primary and lower secondary, upper and postsecondary, tertiary, and postgraduate education. By age 30, for most individuals, educational attainment is complete. We also account for marital status as a predictor variable of the outcome because of, among other mechanisms, income pooling within a joint household that could raise risk-averse individuals’ reservation wages (Pilossoph and Wee 2021). We also account for the potential effects of contextual characteristics on income attainment by including the centrality of the municipality of individuals’ residences in our outcome models. The latter is a categorical variable, with level 1 indicating the residence in most central communities of Norway.
For the employment-related characteristics, we account for labor market status, which includes the following four categories: being out of the labor market, being employed, self-employed, or unemployed. Considering the capacity for work intensity of individuals with chronic conditions and disabilities, we should also account for the length of work performed by individuals to estimate actual income attainment. However, given that the recorded hours of employment are unknown among those who are self-employed, we analyze the subsample of only employed individuals and test if actual working hours explain inequalities in income attainment between individuals with and without chronic health conditions and impairments. Descriptive statistics of variables used in the treatment and outcome models are shown in the supplementary materials (Table S1).
IPWRA Approach
To explore the links between early-life disabilities and income attainment in adulthood, we use an IPWRA approach (Smith et al. 2022). IPWRA estimators rely on probability weights to obtain outcome regression parameters that account for the problem of missing data. The latter issue arises from the fact that each individual is observed in only one of the potential outcomes: being in the general population sample or having one of the considered chronic health conditions and impairments.
IPWRA uses adjusted outcome regression parameters to compute averages of treatment-level predicted outcomes, where the weights are the estimated inverse probabilities of treatment, in our case, having one out of four chronic conditions and impairments in early life. The contrasts of these averages between the general population (non-treated individuals) and individuals with chronic health conditions and impairments (treated individuals) estimate the treatment effects. The main advantage of IPWRA over using only inverse-probability weighting (treatment inverse-probability weighting model) or regression adjustment (outcome regression adjustment model) approaches is that IPWRA estimators have the double-robust property, which implies that only one of the two (treatment and outcome) models must be correctly specified for the IPWRA estimator to be consistent (Słoczyński and Wooldridge 2018).
Deriving treatment effects from IPWRA estimators involves three stages. First, we compute inverse-probability weights by estimating the parameters of the treatment model, in our case, parental education and income accounted separately for fathers and mothers. Second, on the basis of the estimated inverse-probability weights from the first stage, we fit weighted regression models of the outcome for each treatment level and obtain the treatment-specific predicted outcomes for each individual in the analytical sample. Third, we estimate the means of the treatment-specific predicted outcomes, and by contrasting these means, we derive the estimates of the average treatment effects (ATEs). On the basis of the described three-step approach within IPWRA, we can derive consistent estimates of the effect parameters because it is assumed that the selection into treatment (having one of the chronic health conditions and impairments) is independent of the potential outcomes (income attainment) after conditioning on the covariates (Forsman et al. 2016).
Results
Income Attainment and Over-Time Changes
In Figure 1, we present the mean levels of income attainment measured in deciles at age 32 and changes over time in these mean estimates. We see that the most advantaged individuals, as expected, are those belonging to the general population, and the estimates of income are slightly lower for women (5.79, 95 percent confidence interval [CI] = 5.73–5.85) than men (5.92, 95 percent CI = 5.87–5.98). The mean income decile attainment, both for men and women, among those with type 1 diabetes mellitus and asthma are close to each other. Income outcomes for these chronic health conditions and impairment categories come close to the mean estimates for the general population, especially among men with asthma. The mean level of income attainment among those with sensory loss is 4.44 (95 percent CI = 4.18–4.70) decile among women and 4.24 (95 percent CI = 4.02–4.46) decile among men. The most disadvantaged individuals in terms of income attainment at age 32 are those with physical impairments, with a mean level of income attainment of 3.09 (95 percent CI = 2.93–3.25) decile among men and slightly higher among women at 3.52 (95 percent CI = 3.33–3.71) decile. Nonetheless, individuals with physical impairments are the only ones who have experienced more than one decile improvement in mean income attainment between the birth years of 1977 and 1978 (2.24, 95 percent CI = 1.83–2.65) to 1987 and 1988 (3.47, 95 percent CI = 3.12–3.82).
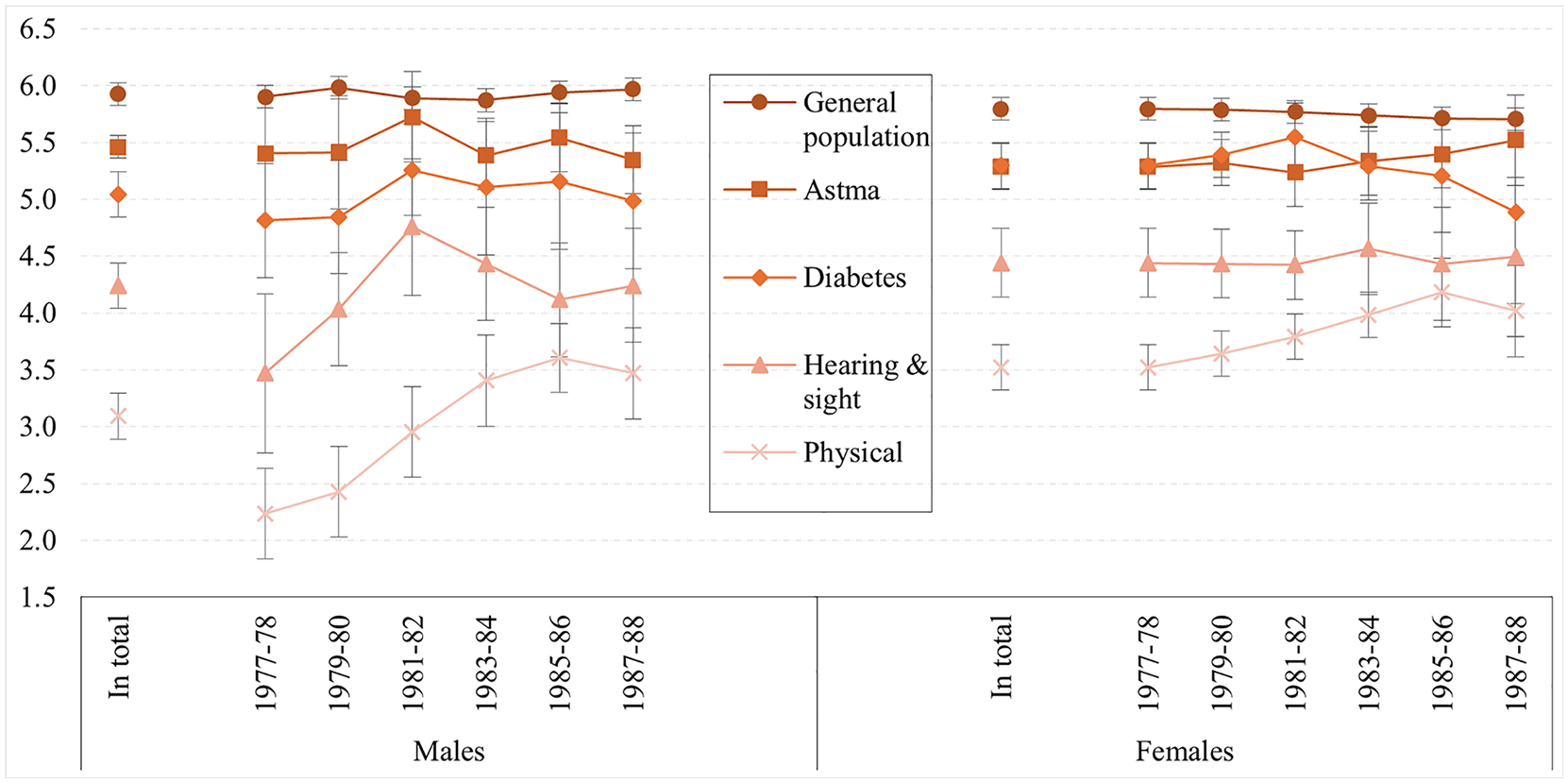
Mean decile attainment and over-time changes in the general population and disability groups.
After observing that there are major inequalities in income attainment according to chronic health conditions and impairments by age 32 and that there has been modest over-time change, Figure S1 in the supplementary materials, depicts the exact distribution of individuals by deciles in the general population and across disability groups. Individuals in the general population are overrepresented in fifth and higher income deciles, both among men and women. Individuals with asthma are more equally distributed across income deciles than individuals with type 1 diabetes mellitus, who are also underrepresented in the eighth decile and above. Lower income attainment is pronounced among men and women with sensory loss. For this disability category, a significant share of individuals is in the bottom four income deciles. The most pronounced inequality in income attainment is observed in the group of physically impaired individuals, among whom up to 70 percent of men fall within the bottom three deciles of income attainment.
Overlap Assumption and Treatment Selection
The central assumption when using the IPWRA approach is the overlap assumption, which requires that every individual in the analytical sample has a positive probability of receiving each treatment, in our case, being in the general population sample or having one of the considered chronic health conditions or impairments. In the supplementary materials (Figure S2), we show the estimated densities of the probability of being in control and treatment groups. The depicted plots suggest that most men across groups have a likelihood of being in the considered treatment categories with propensity scores of 0.60 to 0.85, while women’s propensity scores vary between 0.70 and 0.90. We conclude that there is no evidence that the overlap assumption is violated, which means we can estimate ATEs from IPWRA. Control and treatment groups largely overlap across propensity score distribution among women and men.
Table 1 presents diagnostic statistics that allow us to check for covariate balance over four treatment groups in our IPWRA estimation strategy. The results suggest that our weighting strategy balanced the covariates for mothers’ and fathers’ education and mothers’ and fathers’ income. The variance ratios between raw and weighted estimates are all close to one, as shown in Table 1, while all the standardized differences between raw and weighted estimates are also close to zero, as shown in the supplementary materials (Table S2). The described inference from the diagnostic results is informal because the variance ratio calculation procedure does not produce standard errors for these statistics. Yet we see that the major improvement takes place in the weighted parameters, especially for fathers’ and mothers’ educational attainment.
Variance Ratio between Raw and Weighted Covariates across Disability Conditions.

Note: Variance ratios close to 1 indicate achieved balance for specific variables. Number of individuals = 17,515.
Outcome Model Estimates
Tables 2 and 3 present results from outcome models used to estimate the means of the treatment-specific predicted outcomes and derive ATEs for the considered disability conditions by contrasting these outcomes. For the income of the general population, we see that the attained level of education at age 30 is a strong predictor of the position in the income hierarchy at age 32, with a postgraduate degree increasing income by 2.7 (95 percent CI = 2.5–2.9) and 3.7 (95 percent CI = 3.4–3.9) deciles for, respectively, men and women compared with individuals with only primary and lower secondary education. Both fathers and mothers’ income attainment when individuals were age 15 matter for their income decile position at age 32, with the father’s income demonstrating the strongest effect (0.9, 95 percent CI = 0.06–0.11). Among both men and women, labor market position at age 30 is a significant predictor of income attainment at age 32, with those who are employed having 3.2 (95 percent CI = 3.0–3.4) and 2.3 (95 percent CI = 2.1–2.4) deciles higher position in income distribution than those who are out of labor market and do not look for employment.
Outcome Model Estimates for Income Decile Attainment at Age 32 among Men.

Note: Number of individuals = 9,388.
p < .05. **p < .01. ***p < .001
Outcome Model Estimates for Income Decile Attainment at Age 32 among Women.
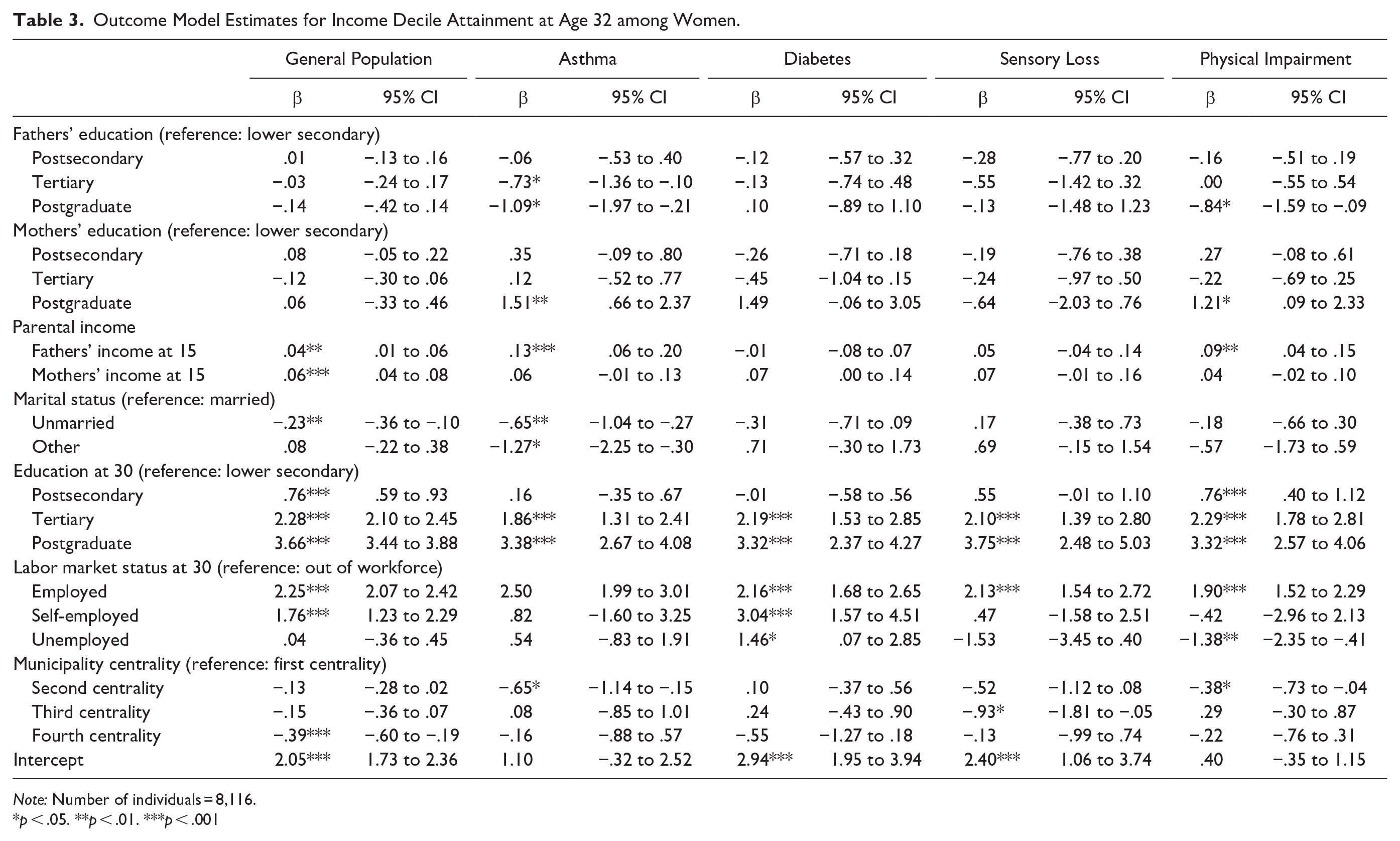
Note: Number of individuals = 8,116.
p < .05. **p < .01. ***p < .001
Predictors of income among individuals with disabilities, in turn, vary by specific chronic health conditions, impairments, and gender. For instance, a postgraduate degree, in comparison with the reference educational category, matters more for men with diabetes (3.8, 95 percent CI = 3.1–4.5) and for women with sensory loss (3.8, 95 percent CI = 2.5–5.0). Fathers’ income matters for women with asthma (0.13, 95 percent CI = 0.06–0.20) and physical impairment (0.09, 95 percent CI = 0.04–0.15) and for men with diabetes (0.09, 95 percent CI = 0.02–0.17). For all chronic health conditions and impairments, being employed is associated with a significantly higher position in the income decile distribution, but this effect is, as a rule, weaker than the one we observed for the general population. Women with asthma, sensory loss, and physical impairment have higher incomes in more central municipalities in comparison with less central municipalities.
By including the birth years of individuals, shown in the supplementary materials (Table S3), we observe that the position in the income hierarchy of individuals with disabilities has not changed over time, apart from one disability category. Having physical impairments among men is the only considered early-life disability for which incomes at 32 were higher among those born from 1981 to 1988 than those born before this period from 1977 to 1980, even after other predictors of income are accounted for.
ATEs for Chronic Health Conditions and Impairments
In Figure 2, we present ATE estimates from our IPWRA outcome models. Two sets of estimates per gender show ATEs, both without and with controlling for individuals’ labor market status. The results suggest that individuals with the considered chronic health conditions and impairments diagnosed during their childhood, compared with the sample of the general population without these early-life disabilities, are significantly disadvantaged in terms of income attainment at age 32. The inequalities are most prominently manifested among men with physical impairments who, on average, attain −1.95 (95 percent CI = −2.19 to −1.71) deciles lower position in income distribution, while for men with sensory loss, this effect is −1.16 (95 percent CI = −1.42 to −0.90) decile. The effect sizes for these disabilities are reduced when individuals’ labor market status is accounted for, but significant inequalities remain for all chronic health conditions and impairments, including for those men who were diagnosed with asthma in early life (−0.18, 95 percent CI = −0.36 to −0.01). After labor market status is accounted for, physically impaired men still have −1.44 (95 percent CI = −1.66 to −1.21) lower attainment in income decile distribution.

Average treatment effect estimates from the inverse-probability weighting regression adjustment approach from models without and with accounting for individuals’ employment status.
We observe the same patterns of inequalities for women as for men, but these inequalities are less pronounced. In the estimates that do not account for labor market status, physical impairment has the strongest negative effect on income attainment at age 32 with −1.14 (95 percent CI = −1.39 to −0.89) decile of lower position in income hierarchy. This effect is reduced to a −0.73 (95 percent CI = −0.97 to −0.49) decile in estimates when the labor market status is controlled. Sensory loss among women in IPWRA estimates, adjusted for labor market status, also maintains a significant negative association with the effects size of −0.35 (95 percent CI = −0.62 to −0.08) decile. The confidence intervals for asthma and diabetes mellitus ATE estimates do not reach conventional statistical significance when women’s employment status is included in the outcome model estimates.
Accounting for Working Hours
In Table 4, we conduct a subsample analysis of only individuals who were employed at age 30 and for whom information on actual working hours per week was available in our dataset. Before describing ATEs for chronic health conditions and impairments, in supplementary materials (Table S4), we see that one additional working hour is associated with improved income decile position for the general population sample as well as for all considered early-life chronic health conditions and impairments, both among men and women with effects sizes varying between 0.4 to 0.11 decile for each additional hour worked per week. In other words, working 10 hours more on a weekly basis, for instance, among physically impaired men, would be associated with 1 decile higher position in the income hierarchy.
The Potential Outcome Means and ATE Estimates from the IPWRA Approach for Income Decile Attainment at Age 32.

Note: Number of individuals = 17,515. ATE = average treatment effect; IPWRA = inverse-probability weighting regression adjustment.
In Table 4, we present potential outcome means and ATE estimates for the general population sample and for individuals with early-life chronic health conditions and impairments. This analysis is limited to only those individuals who were employed at age 30. Among men, for each treatment group, we observe a lower mean decile position than what we see for the general population sample, the strongest effect being among those with physical impairment (−1.07, 95 percent CI = −1.35 to −0.79) and sensory loss (−0.87, 95 percent CI = −1.13 to −0.60). ATE estimates are smaller, but they are also statistically significant for those women with early-life type 1 diabetes mellitus and physical impairment. To illustrate the effect size of these inequalities, we can take the absolute values of income of individuals in 2019 and apply the estimate of decile differences to them. These calculations suggest that, for instance, men with sensory loss were expected to have up to 65,000 Norwegian kroner less income (~$6,000), while for women with physical impairments, this effect size would be about 31,000 Norwegian kroner.
Additional Checks
We conducted additional analysis with various specifications to test how robust the results described above are. In the supplementary materials (Table S5), we reestimate the main results when parental characteristics are measured at the year when individuals were born, but as parental educational variables become available only in 1981, our analytical sample is severely reduced. Table S6 presents the results from the analysis using additional data on parents receiving social assistance as an indicator of selection into disability, but this variable became only available in the registers in 1986, which is the reason why this part of the analysis is conducted with a significantly reduced sample size. Table S7 reports the main ATE estimates for income attainment measured in deciles at age 35 as the outcome measure. Table S8 shows the results when we account for the detailed educational attainment of individuals for 49 specific types of formal educational qualifications according to the Norwegian Standard Classification of Education. With all these new estimates, we observe similar patterns as in the main analyses, which confirms our central finding on the sizable inequalities in income attainment between individuals with early-life chronic health conditions and impairments and the general population of Norway.
Discussion
Widespread inequality based on individuals’ early-life chronic health conditions and impairments is an important social challenge in modern welfare democracies. Despite conducted reforms toward, among other areas, inclusive education, the disability-friendly environment in employment, and disability-related antidiscrimination legislation, the wide gap in various valued life outcomes between individuals with and without disabilities remains across European societies. The existing studies on the considered inequalities have explored many aspects of life, such as educational attainment, labor market characteristics, political participation, and life satisfaction. However, in this stream of literature (see Ballo 2023; Maroto and Pettinicchio 2014), there is limited research analyzing early-life disabilities and subsequent income attainment that also accounts for selection into disabilities. This is particularly relevant for equality considerations because individuals with disabilities and their families often require significantly more resources to maintain the same standards of living as the general population. Some of the reasons why extra costs are needed for these households is that people with chronic health conditions and impairments require goods and services that the general public does not have a need for, such as, among other things, costs related to adjusting apartments for individuals with physical impairments.
Despite being doubly disadvantaged and this issue being of high social relevance, there are several challenges to investigating the consequences of early-life chronic health conditions and disabilities. First, in conventional sources of data such as surveys, cohort studies, or longitudinal panels, it is often impossible to capture sufficiently big sample sizes of individuals with relatively rare conditions such as vision loss or cerebral palsy. Second, even if individuals with disabilities in the data are accounted for, unbiased information about their parents and own income is difficult to derive unless this information stems from official registers. Despite large evidence suggesting that socioeconomic conditions are related to early-life chronic health conditions and impairments, most existing studies on the consequences of disabilities on later life outcomes do not explicitly consider the process of selection into disability. To estimate inequalities in income attainment, it is also important to account for conventional explanations of income, primarily through earnings on the labor market. It is particularly important to control the work intensity of individuals with disabilities as they are more limited in terms of work availability because of alternative needs such as treatment-related routines and procedures (Lutfey and Freese 2005).
To address some of the main methodological shortcomings in this area of research, we have used high-quality national registers from Norway. This source of data allowed us to identify a sufficiently large sample of individuals with relatively rare chronic health conditions and impairments. In addition, register data can account for unbiased information about parental and individual characteristics, such as income attainment. The high-quality and reliable information from the data allowed us to consider selection into early-life chronic health conditions and impairments. This is important because existing evidence indicates that all considered chronic conditions and impairments and their negative consequences are more prevalent among those who are born in less affluent families. The IPWRA approach used in this study is particularly suited to account for the nonrandom distribution of early-life conditions and individuals’ later life characteristics that predict income attainment.
Using treatment models and appropriate weights, we have identified that selection into chronic health conditions and impairments in early life indeed takes place and is an important factor in the potential negative consequences of later life income attainment. Our weighting strategy adjusted for the unequal distribution of parental education between individuals in the general population and those with chronic health conditions and impairments. Additionally, after considering individuals’ labor market characteristics, we identify significant disability-based inequalities, especially among men, which aligns broadly with previous research on gendered disability earnings inequality in Norway and the United States (Ballo 2023; Pettinicchio and Maroto 2017). We showed that those with physical impairments and sensory loss attain up to 1 decile lower position at age 32 than individuals without chronic conditions and impairments. Inequality is also substantial among women with diabetes and physical impairments who, after accounting for actual working hours, have at least one-third of income decile lower attainment than women in the general population.
Overall, we see that the two most disadvantaged groups of individuals are those with sensory loss and physical impairment. These are severe conditions, and they may have more life-altering implications than diabetes mellitus and asthma. It is an unanswered question, however, what are specific channels leading to lower income attainment among individuals with disabilities compared with the general population, even if they have the same social origin characteristics, educational attainment, and work intensity in the labor market? Among other explanations, individuals with considered disabilities might be directly or indirectly discriminated against even after being employed by an organization, might not be given the same opportunities for taking up positions within companies as other employees, might be perceived as less productive employees, and overlooked in promotion decisions and salary raises.
Our findings reveal a persistent gap between Norway’s disability policies and their effectiveness in reducing income disparities. Despite income replacement benefits (e.g., Disability Pension, Work Assessment Allowance) and labor market activation measures (e.g., Varig Tilrettelagt Arbeid), individuals with early-life disabilities remain significantly disadvantaged in income attainment. Although these policies provide financial security, they do not fully address barriers to career mobility, workplace inclusion, and long-term labor market participation. Broader welfare provisions may reduce economic inequality in the general population, but they are not always designed to compensate for the cumulative disadvantages associated with early-life disabilities. Individuals with disabilities often experience disruptions in education, limited access to career progression, and structural labor market exclusion, which are not easily mitigated by financial support alone. Although universal policies promote social inclusion, they may not fully account for the specific needs and barriers that disabled individuals encounter when navigating the labor market. Our findings suggest that stronger targeted interventions are needed, including better enforcement of workplace accommodations, proactive employment support programs, and policies that ensure greater stability and career progression for individuals with disabilities.
Norway, perhaps more than other European societies, has formally committed to promoting equal opportunities and participation for individuals with and without disabilities across various life domains, implementing policies such as the disability-specific antidiscrimination law adopted in 2008 to support this aim. Nonetheless, the evidence presented in this study does not show that the situation has substantially improved for individuals with the considered early-life chronic health conditions and impairments. However, one exception in our analysis is the group of physically impaired men. For those physically impaired men born between 1977–1978 and 1987–1988, the mean level of income attainment at age 32 improved by up to 1 decile, but it still remains at a much lower level than what we observe for the general population.
Our study has its limitations. First, despite comprehensively covering the considered disabilities by including in the analysis all of those who were alive at the time of accessing the data, this also implies that our results do not capture those who died between their birth year (from 1977 to 1995) and 2021. As the mortality levels are higher among those who have early-life chronic health conditions and impairments than in the general population (Blair et al. 2019; Morgan et al. 2015), we assume that those who were alive in 2021 were positively selected, which, in turn, might suggest that the described results are conservative estimates.
Second, there is no mechanism in place to guarantee that a child with a severe condition becomes a recipient of the benefit. Access to benefits may be influenced by a number of factors not related to the child’s condition (Finnvold 2009). The possible bias related to these inequalities may also underestimate the extent of inequalities in our results.
Third, the register data we used provide unbiased estimates of individuals’ parental education and income, but this source of data cannot consider other potentially important characteristics affecting the selection into disabilities and later life outcomes, such as parental cultural capital, health behaviors, or genetic predisposition to certain chronic conditions and impairments.
Last, in the accessed data, we did not have information about individuals’ occupations, which could be an important factor in explaining disability-based inequality in income attainment. However, we accounted for fine-grained educational categories in the supplementary materials, which did not influence observed disability-based inequalities.
Conclusion
With the present study, we document disability-based inequality in income attainment at age 32 in one of the most advanced welfare states in the world, Norway. We show that the selection into disability and the conventional predictors of income do not explain why individuals with early-life disabilities earn less than individuals in the general population of the country. We did not observe meaningful over-time change in income attainment for most considered early-life chronic health conditions and impairments, while men with physical impairment remain the most disadvantaged category of individuals. Much more research is needed to understand the specific mechanisms behind income inequality in adulthood of individuals with early-life chronic conditions and impairments, which could be potentially helpful for policymakers to implement effective reforms and improve the quality of life of these disadvantaged groups of individuals.
Supplemental Material
sj-docx-1-srd-10.1177_23780231251335191 – Supplemental material for A Register-Based Study of Early-Life Disabilities and Income Attainment in Adulthood
Supplemental material, sj-docx-1-srd-10.1177_23780231251335191 for A Register-Based Study of Early-Life Disabilities and Income Attainment in Adulthood by Alexi Gugushvili, Jon Erik Finnvold, Therese Dokken and Jan Grue in Socius
Footnotes
Funding
This work was supported by the Research Council of Norway (grant 312650). The sponsor did not play any role in the study design; in the analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Data Availability Statement
Access to the Norwegian register data is restricted by Statistics Norway. Within our project, we have requested access to register data through our formal procedures under certain strict conditions related to handling, storage, and regulating data use. Our application was evaluated and approved by the Norwegian Centre for Research Data, which mandates that it is illegal to share these data. The data are only on “loan” to research projects for a certain amount of time and need to be deleted by the end of the project period within which access to data was requested.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.