
Abstract
Although prior studies indicate that approximately 6 percent of the population will engage in racial identification switching (RIS), no prior research has explored the potential relation between RIS and health outcomes. Using the California birth cohort file from 2005 to 2015, the authors examine RIS among mothers identifying as non-Hispanic (NH) white or NH Black and with at least two live births over the test period (n = 449,008). Using a sibling-control design, the authors compared perinatal health and sociodemographic characteristics of mothers with RIS over time against those without RIS. The authors also conducted logistic regression analyses predicting maternal race at the second birth after controlling for characteristics of the second birth. In sibling-control univariate results, mothers who switched from NH white to NH Black over time were more likely to deliver a low-weight infant, use public programs (e.g., Medicaid), and have less than a high school education relative to NH white mothers who did not change racial identity over time. Logistic regression results further indicate several socioeconomic (e.g., Medicaid) and health (e.g., low birth weight) factors related to RIS. The pattern of results indicate that health disparity research should carefully consider racial identity as a fluid construct which often varies with socioeconomic and health status.
Racial identification derives from one’s understanding of their social circumstances in relation to expectations set by society (Helms 1990; Islam 2014; Pickett, Saperstein, and Penner 2019). These expectations by society may be described as social norms situated in time and place (Davenport 2020; Pickett et al. 2019). Historical context, politics, and social norms determine the extent to which individuals approach their racial identification as flexible and dynamic (Agadjanian and Lacy 2021; Davenport 2020; Liebler et al. 2017; Pickett et al. 2019; Porter, Liebler, and Noon 2016). In various studies, an average of 8 percent of people change their racial identities at some point in their lives (Agadjanian 2022; Agadjanian and Lacy 2021; Liebler et al. 2017; Saperstein and Penner 2014).
These findings of racial identification switching (RIS) reside within a larger scientific literature which views race as a societal construct (Agadjanian 2022; Omi and Winant 2014; Penner and Saperstein 2008; Pickett et al. 2019). As such, this approach to race leaves many attractive avenues open to inquiry about causes and consequences of RIS. For public health researchers, to whom the social determinants of health remain of primary interest, RIS provides a novel avenue to examine racial/ethnic health disparities. Here, we broaden previous research by Penner and Saperstein (2008) to an epidemiologic forum. We investigate the relation between RIS among non-Hispanic (NH) white and NH Black mothers and maternal and infant health outcomes through use of the California birth cohort file (BCF).
Social identity theory (Islam 2014) and racial identity theory (Helms 1990) provide a fundamental framework for RIS. Social identity theory contends that individuals identify with a group (e.g., racial, economic) on the basis of its relation to their own social circumstances (Islam 2014). On the other hand, racial identity theory argues that individuals define themselves according to the society’s understanding of their race (Helms 1990). These theories find application to health in studies such as that of Harvey and Afful (2011) that demonstrate certain health behaviors to be perceived as more Black or more white. Therefore, as both theories suggest an alignment between racial identity and individual perception, it seems plausible that cultures which equate white identity with higher social status might display correlations between changing racial identification and health status (López 2006; Omi and Winant 2014; Saperstein and Penner 2012).
Previous studies examined the association between socioeconomic status and health outcomes (Bilgin, Mendonca, and Wolke 2018; Dolin and Kominiarek 2018; Leddy, Power, and Schulkin 2008; Menting et al. 2019), socioeconomic status and RIS (Doyle and Kao 2007; Penner and Saperstein 2008), and racial identification and health (Jones et al. 2008). The efforts by Jones et al. (2008) highlights the relation between socially assigned race, the way others identify a person, and health status. Particularly, someone identified as white by others exhibits a health advantage irrespective of their self-identified race (Jones et al. 2008). Additionally, previous studies highlight the role of low socioeconomic status contributing to the likelihood of an individual switching racial identification over time (Doyle and Kao 2007; Ren, Amick, and Williams 1999; Saperstein and Penner 2012). Given these previous findings, an individual of low socioeconomic status may also exhibit a greater likelihood of adverse health as well as a greater likelihood of RIS. As such, we hypothesize a potential relation among socioeconomic status, health, and RIS.
Identifying as multiracial or with both a racial and ethnic identity influences the likelihood of RIS. Doyle and Kao (2007) examined RIS among multiracial individuals, finding that low socioeconomic status predicts a greater likelihood of RIS. The work of Antman, Duncan, and Trejo (2016) highlights ethnic attrition especially among children of interracial couples. Ethnic attrition relates to Mexican American children identifying as NH (Antman et al. 2016). Furthermore, among ethnic attritors, their health status more closely relates to that of white individuals (Antman et al. 2016). These findings highlight the necessity to differentiate between Hispanic and NH individuals.
Previous literature also suggests stigma (Horan and Austin 1974) and stereotypes (Allen 1996; Donovan and West 2015) may play a role in one’s racial identification. Additionally, theories such as social identification and racial identification highlight different circumstances influencing one’s preference to identify with one group over another. Social identification theory emphasizes that individuals lean toward identification on the basis of shared characteristics (Islam 2014). On the other hand, racial identity theory argues that individuals mold their behaviors to adhere to social expectations (Helms 1990). Within these theories, stigmas or stereotypes related to low socioeconomic status or poor health may deem a minoritized race as expectation. The work of Saperstein and Penner (2012) suggests a greater likelihood of identifying as Black after experiencing low socioeconomic status via unemployment or poverty. Additionally, Allen (1996) suggested that Europeans tend to be stereotyped as educated or rich, while African Americans tend to be stereotyped as poor. These stereotypes may inherently carry a positive or negative connotation potentially influencing one’s opportunities in life. For example, Jones et al. (2008) found that individuals classified as white by others exhibit better health than other racial/ethnic groups even if the individual does not self-identify as white. As such, the perception of an individual by society may influence not only life opportunities but also health status.
The examination of racial identification and RIS in more recent work relates to historical context, politics, and social expectations. For instance, Bratter and O’Connell (2017) examined the role of law in racial classification. The authors found that place-specific historical context (i.e., country or state history) and politics influence one’s racial identity. Likewise, Davenport (2020) contrasted racial fluidity within the United States and Latin America suggesting that place-specific social expectations affect one’s racial classification. As such, these findings highlight the complexities of racial identity.
Furthermore, U.S. census data demonstrate that RIS occurs within 4 percent to 8 percent of the population (Liebler et al. 2017; Singer and Ennis 2003; U.S. Census Bureau 1993). Work examining various panel surveys shows RIS occurring within 5 percent to 12 percent of the population (Agadjanian 2022). Whereas these studies suggest a higher level of RIS pervasiveness than intuitively expected, Penner and Saperstein (2008) found that these numbers exceed simple data error, which seems to occur in other variables about 2 percent of the time. Subsequently, researchers have investigated this pattern in different social contexts including presidential elections, incarceration, and employment (Agadjanian and Lacy 2021; Liebler et al. 2017; Penner and Saperstein 2008). Although the literature supports both the prevalence of RIS and its association with social circumstance, we know of no work that examines health as a correlate of racial identification through RIS.
Current scientific literature demonstrates a correlation between both racial/ethnic identity and socioeconomic standing with poorer health over the life course (Grollman 2014; Williams and Sternthal 2010). For instance, preterm birth and low birth weight correlate with a decreased likelihood of higher educational attainment and increased likelihood of receiving social benefits (Bilgin et al. 2018). Additionally, maternal obesity, heavily linked to lower socioeconomic status, also serves as a strong predictor of adverse perinatal outcomes such as increasing the likelihood of pregnancy complications (Dolin and Kominiarek 2018; Leddy et al. 2008; Menting et al. 2019). These health outcomes occur at higher rates among Black mothers and their births (Catov et al. 2016; Culhane and Goldenberg 2011; Dolin and Kominiarek 2018). Given that lower socioeconomic status varies with worse health outcomes and that a certain portion of the population switches racial identification in concert with changes in social status (Penner and Saperstein 2008; Saperstein and Penner 2012), racial reidentification may precede, or arise from, changes in health or economic circumstances.
Health-promoting programs such as the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) and Medicaid (Medi-Cal in California) target lower socioeconomic families. As such, use of these programs may induce a feeling of stigma upon the mother (Horan and Austin 1974) and thus lead to identification with an underprivileged group. On the other hand, as racial identity theory suggests, an individual who changes their racial identification for nonhealth or economic reasons (e.g., new spouse) may display new economic or health outcomes, behavioral scripts apropos to their new identity (Wilkinson and Dunlop 2022). To consider these theories, we use data in California of more than 490,000 sibling-linked births, from 2005 to 2015, to quantify the prevalence and predictors of RIS and identifying with one race over another among NH white and NH Black mothers only given the largest perinatal health disparities exist between these two groups.
Although our observational data cannot inform causes of RIS, we do attempt to locate relevant relations among RIS and health. Characterizing whether, and to what extent, RIS correlates with perinatal and maternal health could hold two main implications. First, positive associations between adverse health and switching racial identification from NH white to NH Black would provide novel support of the importance of considering both racial fluidity and socioeconomic factors when studying health disparities. Second, if RIS occurs frequently among NH white and NH Black mothers, then such information may urge health scholars to incorporate race identification at multiple time points or with multirace codes.
Methods
Data and Variables
The California Department of Public Health BCF for 2005 to 2015 comprises our study data. This dataset contains nearly 100 percent of all births in California and contains socioeconomic and health information of the parents coupled with the birth information of their child. To verify the process of obtaining the mother’s race variable, we contacted the 10 California hospitals with the highest volumes of NH Black births. On the basis of these discussions, we found that the mother, not the health care provider, identifies both their own race and the father’s race. As such, we assume that the race/ethnicity information contained in the BCF accurately reflects the mother’s self-reported race.
For this study the mother’s self-reported race serves as our dependent variable. We restricted our dataset to include only mothers who identified as NH white or NH Black and who had at least two live births over the test period (n = 449,008). We used the first race code as a measure of the primary race identity of the mother. Although mothers may select up to three race codes, we cannot be certain that a mother missing a second or third race code does not identify as multiracial. Because of this ambiguity, we restrict to only mothers identifying as white or Black for the first race code. We then used the Hispanic origin code to identify mothers as NH white or NH Black race/ethnicity. We excluded mothers of Hispanic origin because of their different patterns of perinatal outcomes relative to NH white and NH Black births (MacDorman and Gregory 2013).
Birth outcomes of the infant, which serve as independent variables, included preterm birth and low birth weight. We defined preterm birth as less than 37 completed weeks at delivery (yes or no) and low birth weight as less than 2,500 g (yes or no). We also examined obese pre-pregnancy body mass index (BMI) (yes/no) for the mother as a measure of maternal health given its documented relation with an increased risk for adverse health both for the mother and for the live birth (Liu et al. 2016). Consistent with national guidelines, we determined obesity as a BMI of 30.0 kg/m2 or higher (Weir and Jan 2022).
Sociodemographic characteristics serving as binary predictor variables include Medi-Cal health insurance (1 = yes, 0 = no) and receipt of WIC (1 = yes, 0 = no). Medi-Cal and WIC serve as health-promoting programs for individuals meeting low-income threshold eligibility requirements. As such, we use Medi-Cal and WIC as proxy measures for socioeconomic status when used as predictor variables. Additionally, in our logistic regression analyses we included maternal age (categorized as ≤17, 18–24, 25–29, 30–34, and ≥35 years), education level (less than high school, high school graduate, or greater than high school), and Medi-Cal as covariates given their relation to perinatal health.
Additionally, we created a categorical variable for the father’s race (1 = white, 2 = Black, 3 = other race, refused to state, or not reported). We used the race code provided for the non-birthing parent on the birth certificate. For our sibling-linked design, we did not have a Hispanic origin code for the non-birthing parent, so we could not differentiate between fathers with and without a Hispanic origin. The institutional review boards at the California Department of Public Health (13-06-1251) and the University of California, Irvine (20139716), approved the use of these data for our study.
Sibling Linkage Strategy
Consistent with previous literature (Gailey et al. 2021; Putnam-Hornstein et al. 2013), we used Link Plus version 3.0, a linkage program developed by the Division of Cancer Prevention within the Centers for Disease Control and Prevention, to identify consecutive singleton live births of the same mother. Link Plus uses a probabilistic record linkage algorithm developed by Fellegi and Sunter (1969). The program “blocks” records matching on the basis of a set of decision rules providing a match rate score from 0 to 25. Births were linked on maternal date of birth, maternal first name, maternal last name, and paternal date of birth. The date of last delivery for a subsequent birth was used to ensure true matches between the first birth and the second and third (if applicable) birth. We refer the reader to prior literature which details the full process of creating our sibling-linked data (Gailey et al. 2021).
Analysis
Our data include two time points per mother, that is, the first sibling birth (time 1) and second sibling birth (time 2) of the sibling pair. These sibling births may not correspond to birth orders one and two as time 1 and time 2 births relate to their order during the data years available using the sibling linkage. Our first analysis compares the sociodemographic and health factors, at time 2, of mothers with RIS between times 1 and 2 with mothers without RIS between times 1 and 2. The second sibling birth (i.e., time 2) allows us to discern whether RIS occurred from NH white to NH Black or from NH Black to NH white. We compared mothers who switched from NH white to NH Black with mothers who consistently self-identified as NH white. Similarly, we compared mothers with RIS from NH Black to NH white with mothers consistently self-identified as NH Black. We plotted the differences of these proportions.
Next, we used logistic regression to assess whether identifying as a NH white or NH Black mother relates to poor perinatal health, poor maternal health, and low socioeconomic status. We separate our data into two panels: mothers who identify as NH white at the first birth and mothers who identify as NH Black at the first birth. For each panel, we conduct analyses using low birth weight, preterm birth, obese maternal BMI, WIC receipt, Medi-Cal receipt, and less than high school maternal educational attainment at the second birth as exposures. When examining the association between low birth weight, preterm birth, or obese maternal BMI and maternal race at the second birth (or RIS), we include categorical covariates for father’s race, maternal age, maternal education, and health insurance type of the second birth. Then, when examining the association between WIC receipt or Medi-Cal receipt and maternal race at the second birth, we include categorical covariates for father’s race, maternal age, and maternal educational attainment at the second birth. Last, to examine the relation between maternal race at time 2 as a function of less than high school maternal education at time 2, we control for father’s race, maternal age, and health insurance type at time 2. For the panel in which mothers start as NH white, we assess RIS by using NH Black race as the outcome. Conversely, for the panel where mothers start as NH Black, we assess RIS by using NH white race as the outcome.
Results
The sibling linkage and data restriction strategy provided a sample of 449,008 NH white and NH Black mothers in California with two singleton live births between 2005 and 2015. Overall, RIS among mothers occurred much less frequently—that is, in fewer than 1 percent of births (2,818 of 449,008)—than did RIS as reported in other populations (Penner and Saperstein 2008) (Table 1). The frequency of RIS from NH white to NH Black is similar to the RIS frequency from NH Black to NH white. Table 1 depicts the characteristics of mothers and their second live-born infants by RIS status. Mothers with RIS (vs. no RIS) are more likely to have Medi-Cal insurance, attain less than a high school education, receive WIC, and show an obese pre-pregnancy BMI (p < .0001 for all). The maternal age distribution, moreover, of RIS mothers skews much younger than for those without RIS across births. In addition, NH Black race of the father is much more frequent among RIS mothers than among those without RIS. Regarding perinatal outcomes, RIS mothers show greater risk for preterm (p < .0001) and/or low weight birth (p = .02) relative to non-RIS mothers.
Sociodemographic Characteristics and Race/Ethnicity Identity Switching at the Second Birth among NH White and NH Black Mothers with at Least Two Live Singleton Births in California from 2005 to 2015.
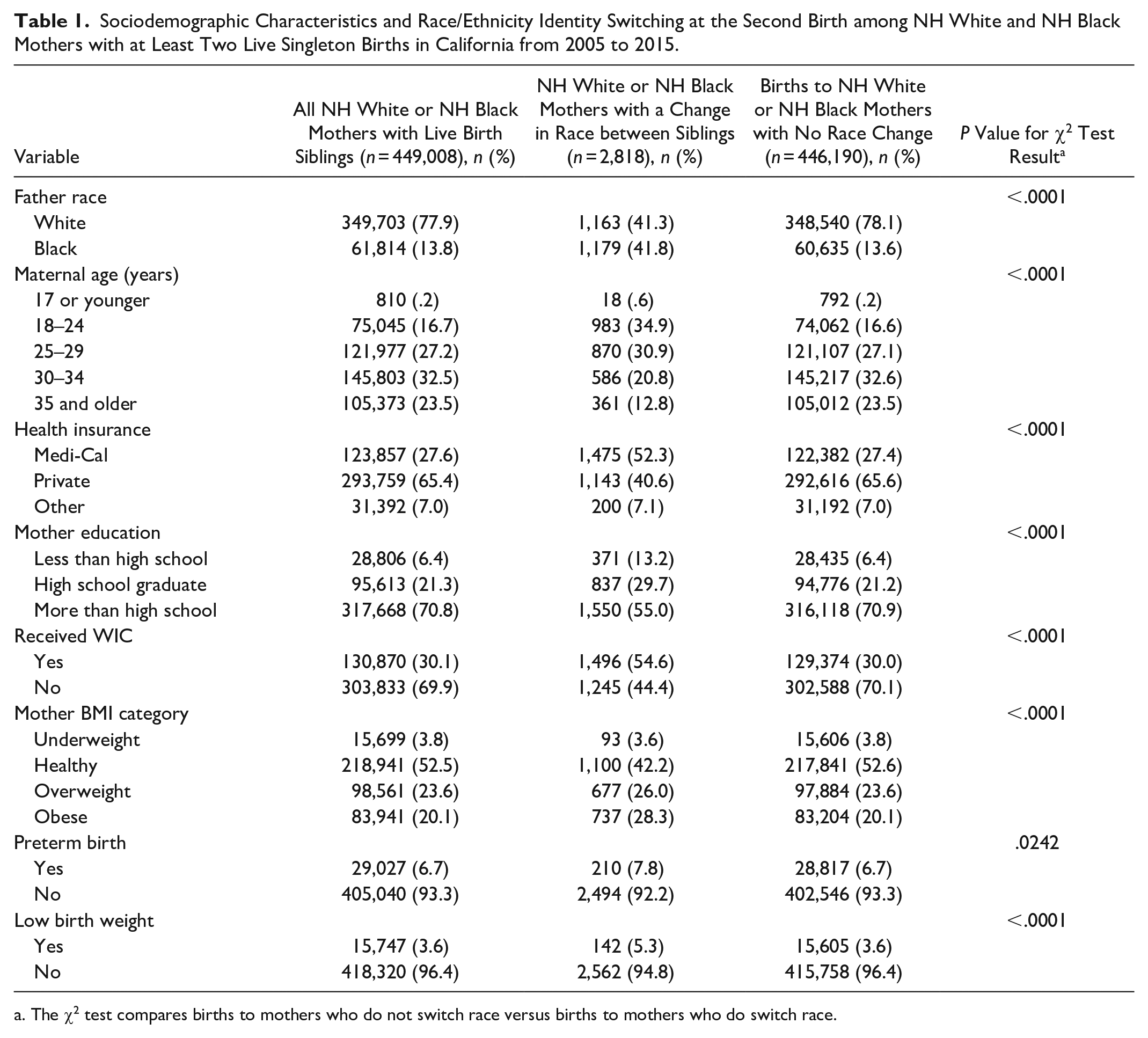
The χ2 test compares births to mothers who do not switch race versus births to mothers who do switch race.
Figure 1 compares sociodemographic and health characteristics of RIS and non-RIS mothers according to their race/ethnicity identification at time 1. Figure 1A describes mothers who identified as NH Black at time 1. The blue bars in Figure 1A show that RIS mothers from NH Black to NH white are less likely than non-RIS NH Black mothers (i.e., orange bars) at time 2 to deliver a preterm or low-weight infant, be obese, have WIC and Medi-Cal benefits, and report a NH Black father (p < .05 for all). Put another way, RIS from NH Black to NH white correlates with having relatively improved perinatal and maternal health and higher socioeconomic status at time 2 compared with NH Black mothers with no RIS.

Mother’s racial classification by social status and birth outcome of second siblings born in California from 2005 to 2015.
Figure 1B describes mothers who identified as NH white at time 1. Results generally cohere with those in Figure 1A, but in the obverse direction. RIS from NH white to NH Black correlates with having relatively greater risk for obesity, low weight birth, and lower socioeconomic status at time 2 compared with NH white mothers with no RIS (p < .05 for all). Consistently for both Figures 1A and 1B, race/ethnicity of the father at time 2 also strongly varies with the probability of RIS (p < .0001).
Results from the logistic regression analyses, in which we examine each variable’s contribution to RIS while adjusting for a set of additional socioeconomic and demographic variables, appear in Table 2. For mothers who start as NH white, WIC and Medi-Cal receipt predicts an increased odds of RIS to NH Black. For mothers who start as NH Black, however, low birth weight, preterm birth, and WIC receipt predict a decreased odds of RIS to NH white. In addition, for mothers first identifying as NH white, low birth weight, and obese maternal BMI may suggest an increased odds of RIS to NH Black, albeit not to traditional levels of statistical detection. Similarly, for mothers first identifying as NH Black, less than a high school educational attainment among mothers may suggest a decreased odds of RIS to NH white, albeit not to traditional levels of statistical detection. The set of results indicate that perinatal health and socioeconomic characteristics correlate with RIS in a subsequent pregnancy.
ORs and 95 Percent CIs of Logistic Regression Models Predicting Mothers Who Switched Identifying as NH White or NH Black at the First Birth and NH Black or NH White at the Second Birth as a Function of Perinatal Health, Maternal Health, and Socioeconomic Status during the Second Sibling a Birth among 449,008 Mothers with at Least Two Live Births in California between 2005 and 2015.

Note: BMI = body mass index; CI = confidence interval; HS = high school; NH = non-Hispanic; OR = odds ratio; WIC = Special Supplemental Nutrition Program for Women, Infants, and Children.
The order of sibling birth refers to whether it is the first identifiable birth or second identifiable birth among mothers giving birth between 2005 and 2015. This may not conform to the actual birth order of a mother’s births.
Controls for father’s race, maternal age, maternal educational attainment, and receipt of Medi-Cal health insurance.
Controls for father’s race, maternal age, and maternal educational attainment.
Controls for father’s race, maternal age, and receipt of Medi-Cal health insurance.
p < .1. **p < .05. ****p < .0001.
To assess the robustness of our findings, we also use time 1 covariates and predictors to examine the relation between sociodemographic characteristics and birth outcomes among mothers switching from NH white to NH Black or NH Black to NH white at the second birth (see Table 3). By doing so, we can assess temporal order between the socioeconomic status or health status of the mother and their birth prior to the switch in racial identity in a mother’s time 2 birth. We find our association for low birth weight and WIC to follow the same directions whether using time 1 or time 2 covariates. Results for preterm birth, Medi-Cal, and less than a high school education further support the notion that poor health or socioeconomic status may contribute to RIS.
ORs and 95 Percent CIs of Logistic Regression Models Predicting Mothers Who Switched Identifying as NH White or NH Black at the First Birth and NH Black or NH White at the Second Birth as a Function of Perinatal Health, Maternal Health, and Socioeconomic Status during the First Sibling a Birth among 449,008 Mothers with at Least Two Live Births in California between 2005 and 2015.
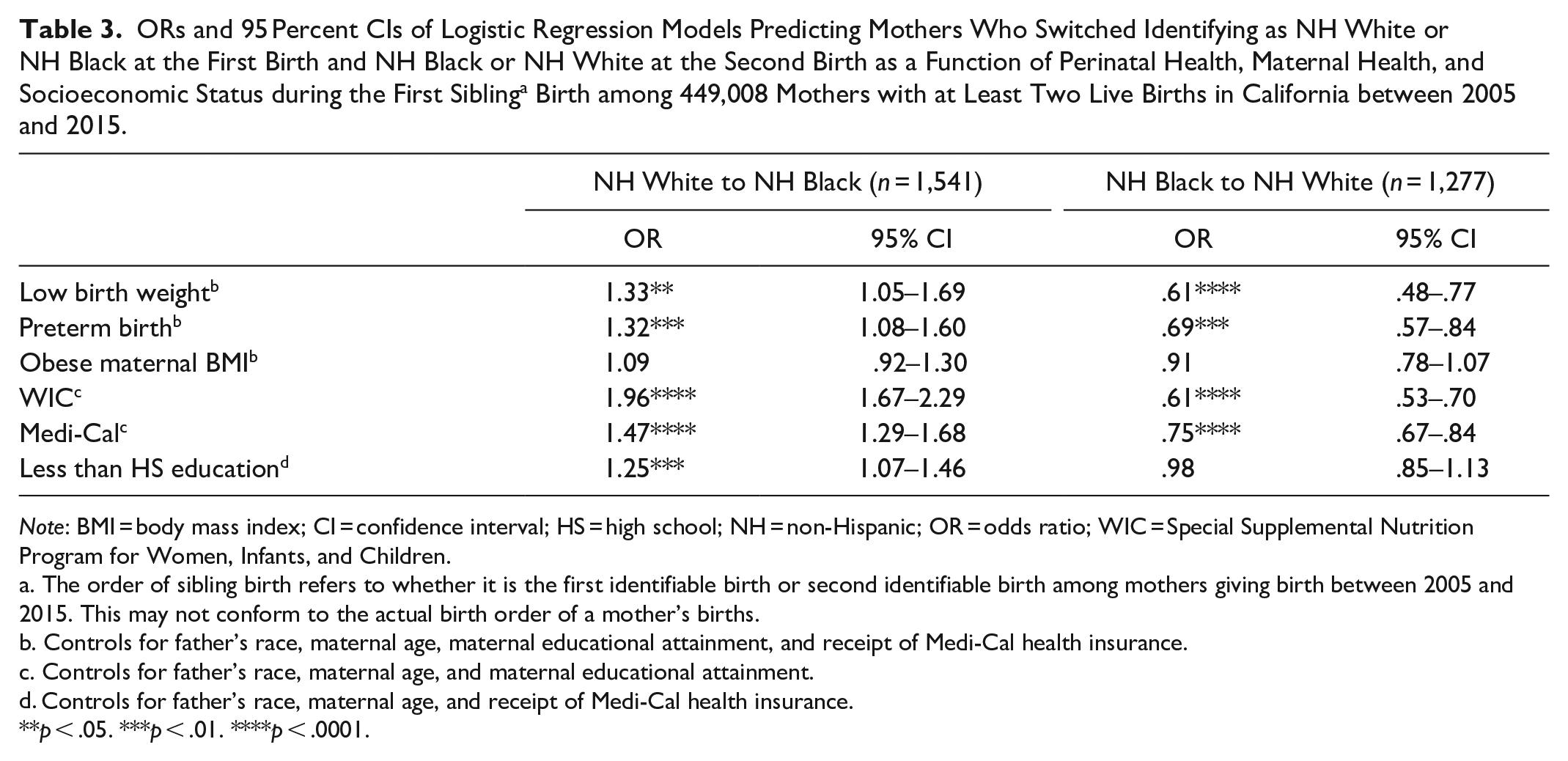
Note: BMI = body mass index; CI = confidence interval; HS = high school; NH = non-Hispanic; OR = odds ratio; WIC = Special Supplemental Nutrition Program for Women, Infants, and Children.
The order of sibling birth refers to whether it is the first identifiable birth or second identifiable birth among mothers giving birth between 2005 and 2015. This may not conform to the actual birth order of a mother’s births.
Controls for father’s race, maternal age, maternal educational attainment, and receipt of Medi-Cal health insurance.
Controls for father’s race, maternal age, and maternal educational attainment.
Controls for father’s race, maternal age, and receipt of Medi-Cal health insurance.
p < .05. ***p < .01. ****p < .0001.
Discussion
Whereas much theory describes the possible motivations for RIS (Davenport 2020; Islam 2014; Omi and Winant 2014), we know of no work that empirically examines RIS and health. We use a unique sibling-linked dataset in California and find that RIS correlates with maternal and perinatal health outcomes. Mothers who switch from NH white to NH Black over time were more likely to be obese, deliver a low weight infant, to use WIC and Medi-Cal insurance, and to have less than a high school education at their second birth than were NH white mothers who do not change racial identity over time. Conversely, RIS mothers who switched from NH Black to NH white were less likely to be on WIC, to have Medi-Cal insurance, to have less than a high school education, to have lower obesity prevalence, and showed lower frequency of low-weight birth at their second birth than persons who self-identified consistently as NH Black. When controlling for sociodemographic factors (e.g., father’s race), several of the univariate findings remained statistically significant. Our findings related to socioeconomic conditions such as the use of Medi-Cal or obtaining less than a high school education aligns with the previous literature. These results underscore, as in prior work, the influence of socioeconomic status on one’s decision to identify as one racial or ethnic group over another (Doyle and Kao 2007; Penner and Saperstein 2008; Ren et al. 1999). Our study, moreover, adds the novel finding of an association between switching one’s racial identity over time and markers of one’s health status.
The overall prevalence of RIS among NH white and NH Black mothers in our study was lower than in previous reports of RIS using other datasets. We suspect that this low prevalence arises for two reasons. First, much of RIS occurs among Hispanic and Asian persons (Alba, Insolera, and Lindeman 2016), which we excluded because of our focus on well-documented disparities between NH Black and NH white mothers in perinatal health. Second, the birth file solicits racial identity via a checklist rather than through open-ended questions. The checklist might induce less nuanced responses that lead to fewer changes over time in the classification of racial identity.
Despite finding only a modest subset of mothers switching race between subsequent births, our work holds implications for our understanding of health disparities. Previous work highlights the need to examine health disparities among multiracial individuals (Grilo et al. 2023; Rizzo and Kintner 2013). Other work focusing on Mexican Americans highlights ethnic attrition as contributing to our understanding of health disparities when considering parental intermarriage status and generation status (Antman et al. 2016). When situating our work within this literature, the implications of our findings may suggest an underestimation of health disparities between NH Black and NH white persons if researchers do not consider racial identity over time. This underestimation may especially hold relevance for multiracial or multiethnic families or individuals who may identify as one group over another depending on their social position, health status, or partner’s race/ethnicity. Given the social construction of race, health disparities research should incorporate markers of social status in addition to stratification by race, ideally using longitudinal measurements, to address potential interventions.
The ability to measure racial self-identification and social circumstances at two time points offers a methodological measurement advantage in our research relative to prior work. Although we suspect that changes in racial identification may reflect health and economic circumstance, and our tests treat racial switching as the dependent variable, we note that the associations we report should not be interpreted as causal relations. However, we view our analysis as reflecting correlations and therefore caution against making any causal interpretations. We base this caution upon both the using of a singular race code and the limited extent to which maternal socioeconomic circumstances are captured in the BCF at the time of birth. Given that we use father’s date of birth to match sibling births, we could not examine single mothers as a subset of all mothers. We encourage future work to examine single mothers given the large association we find with father’s race and RIS.
Our investigation of birth certificate data in California both supports and extends the previously explored phenomenon of racial fluidity in administrative records such as census data, political party affiliation, and the labor market (Agadjanian and Lacy 2021; Liebler et al. 2017; Penner and Saperstein 2008). The low prevalence of RIS that we observe suggests that our findings may be better suited for further demographically oriented work than for public health interventions. If applied to public health research, future work should consider capturing race at multiple time points to assess whether RIS influences estimates of health disparities especially among racial and ethnic groups exhibiting greater RIS in previous sociological work.
Supplemental Material
sj-docx-1-srd-10.1177_23780231251323717 – Supplemental material for Racial Identification Switching and Health among Mothers in California
Supplemental material, sj-docx-1-srd-10.1177_23780231251323717 for Racial Identification Switching and Health among Mothers in California by Brenda Bustos, Jason Bonham and Tim A. Bruckner in Socius
Supplemental Material
sj-docx-2-srd-10.1177_23780231251323717 – Supplemental material for Racial Identification Switching and Health among Mothers in California
Supplemental material, sj-docx-2-srd-10.1177_23780231251323717 for Racial Identification Switching and Health among Mothers in California by Brenda Bustos, Jason Bonham and Tim A. Bruckner in Socius
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (grant R01 HD103736, Tim A. Bruckner, principal investigator).
Data Availability Statement
Restrictions apply to the availability of the data because of the inclusion of personal identifiable information as needed for the sibling linkage.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.