
Abstract
School suspension has been linked to numerous adverse social outcomes in adolescence and adulthood. While research continues to highlight the deleterious consequences tied to suspension, less is known about how exposure to suspension influences health over the life course. Drawing from panel data, we address this gap by investigating whether school suspension is associated with self-rated health from adolescence to midlife. Compared to youth with no history of suspension, suspended youth were more likely to report poorer health in adolescence. Findings also demonstrate that school suspension plays a significant role in self-rated health patterns over time. Specifically, we find suspended youth experience a persistent health gap in excellent health from adolescence to midlife and a more rapid acceleration of fair and poor health from their late 20s to midlife. Taken together, this study provides new evidence of the role of exclusionary discipline in shaping health disparities from adolescence to midlife.
Exclusionary discipline, the practice of removing students from their typical learning environments through suspension or expulsion, has become a commonly used punishment tool in U.S. schools (Losen and Haynes 2016; Losen and Skiba 2010). Due to the use of “zero-tolerance” and “get tough” policies that mandate predetermined punishments for certain student code of conduct violations, exclusionary discipline increased by roughly 50 percent from the early 1970s to 2010 (Hirschfield 2008; McCombs, Scott, and Losen 2022). Although this school punishment practice has slightly declined in recent years, approximately 60 percent of U.S. schools continue to mandate suspension or expulsion for code of conduct violations (Perera and Diliberti 2023). Consequently, an estimated 5 million youth are exposed to exclusionary discipline each year (U.S. Department of Education, Office for Civil Rights 2022).
Despite the widespread use of this form of punishment, exclusionary discipline policies have been shown to be ineffective at dissuading school-age children from engaging in conduct violations. For instance, greater use of exclusionary discipline has been shown not to deter classroom disruptions or student misbehavior or improve school climate (Perry and Morris 2014; Raffaele Mendez 2003; Skiba 2000). Moreover, removing students from their learning environments through exclusionary discipline has been associated with a range of adverse academic outcomes, such as a reduction in standardized test scores, graduation rates, educational matriculation, and postsecondary enrollment (Balfanz, Byrnes, and Fox 2015; Christle, Jolivette, and Nelson 2007; Fabelo et al. 2011; Kinsler 2013; Morris and Perry 2016; Raffaele Mendez 2003).
Exclusionary discipline also limits youths’ ability to develop and maintain prosocial peer relationships. For instance, school suspension has been linked to greater friendship discontinuity and involvement with substance-using peers (Jacobsen 2020). Scholars also demonstrate that the widespread use of exclusionary discipline practices contributes to the “school-to-prison pipeline,” a system that pushes suspended and/or expelled youth into the U.S. criminal legal system (Hirschfield 2008; Kang-Brown et al. 2013; Monahan et al. 2014). Specifically, studies find that exposure to exclusionary discipline can serve as a turning point toward offending, arrest, and incarceration both as a juvenile and adult (Fabelo et al. 2011; Gerlinger et al. 2021; Hemez, Brent, and Mowen 2020; Mittleman 2018; Skiba, Arredondo, and Williams 2014; Wolf and Kupchik 2017). Finally, although exclusionary discipline has been shown to negatively shape social and academic outcomes for those exposed to this type of school punishment, it is important to note that in some cases, removing students from the classroom for disruptive behavior is associated with improvement in academic achievement outcomes for nonsuspended students, particularly historically marginalized groups (Figlio 2007; Hwang and Domina 2021).
Due to the range of deleterious social and academic harms associated with exclusionary discipline, an emerging body of scholarship has placed attention on understanding the broader health consequences associated with exposure to school suspension and expulsion. Focusing mostly on mental and behavioral health, studies find a history of exclusionary discipline increases the risk for tobacco use (Hemphill et al. 2012) and in some cases, depression and anxiety (So, Freese, and Barnes 2024). Despite the significant downstream consequences of school suspension—such as exclusion from peers, increased criminal legal contact, and school failure—this commonly used disciplinary tool remains underexplored as a potential driver of health disparities across the life course (American Psychological Association Zero Tolerance Task Force 2008; Duxbury and Haynie 2020).
Drawing from nationally representative panel data and guided by stress process theory and the life course perspective, we address this gap by examining whether and how school suspension determines life course patterning of self-rated health from adolescence to midlife. Despite the increased availability of biomarker and anthropometric measures that can be linked to survey data, self-rated health continues to be shown to be a valid and reliable indicator of general health status (Bailis, Segall, and Chipperfield 2003; Chandola and Jenkinson 2000) and a key determinant of early death (Idler and Benyamini 1997; Jylhä 2009).
Background
Exclusionary Discipline as a Stressor
To better understand how exclusionary discipline is potentially associated with self-rated health from adolescence to midlife, we draw on the core principles of stress process theory and the life course perspective. Although stress process theory and the life course perspective have distinctive features, both recognize the importance of stress in shaping health disparities. Stress process theory posits that repeated stress exposures and/or major life events heighten the risk of poor health and well-being by negatively impacting various life domains, such as work, family, and school (Aneshensel and Avison 2015; Aneshensel and Mitchell 2014; McLeod 2012; Pearlin 1989; Turner 2010).
Guided by extant literature on exclusionary discipline, we argue that there is substantial evidence to suggest that school suspension is a stressor that potentially plays a role in health disparities. Contemporary U.S. education operates under the premise that all have equal access to the education necessary to lead a meaningful and productive life. A robust literature, however, finds schools play a central role in legitimating and reinforcing social inequality (Baumert, Nagy, and Lehmann 2012; DiPrete and Eirich 2006; Fryer and Levitt 2006; Potter and Morris 2017).
From the time students enter the U.S. educational system, schools engage in practices that categorize and sort students based on age, grades, ability, instructional tracks, behavior, and existing racialized, gendered, and class-based hierarchies. Sorting within schools often dictates the allocation of resources, support, and incentives available to students (Domina, Penner, and Penner 2017). In addition to obstructing access to education and upward mobility, schools are powerful institutions that shape and regulate social identities (Ferguson 2000; Ochoa 2013; Ray 2022; Vasquez-Tokos, and Norton-Smith 2017). Disciplinary practices, particularly those that involve school-imposed labeling, can significantly shape students’ sense of self by affecting their emotional well-being, performance of gender, and educational attainment (Ferguson 2000).
With respect to exclusionary discipline, scholarship consistently finds that schools sort suspended and/or expelled youth into academic and social pathways that can be a source of stress. For example, punitively removing students from their learning environments is associated with a reduction in instructional days, diminished student-teacher relationships, and increased likelihood of dropping out of school or failing to attend and graduate from college (Chu and Ready 2018; Noltemeyer, Ward, and Mcloughlin 2015). Exclusionary discipline also stresses essential social relationships. Suspended and expelled youth frequently receive stigmatizing labels within and outside of schools (Anyon, Zhang, and Hazel 2016; Davies and Tanner 2003; Novak 2019; Rios 2011), which has been linked to the loss of peer relationships and increased association with peers who use illicit substances (Novak and Krohn 2021). The repercussions of exclusionary discipline also extend to the family. The removal of young people from educational settings disrupts parent work schedules, leads to stigmatization of families, and exacerbates tensions between parents and punished youth (Dunning-Lozano 2018; Kupchik 2016).
Youth who have been removed from schools through exclusionary discipline are also more likely to be exposed to the U.S. criminal legal system, which is also widely recognized as a form of stress that shapes health (Boen 2020; Del Toro et al. 2019; Niño et al. 2023). For instance, suspended youth are at greater risk of arrest within the first 12 months of disciplinary action (Monahan et al. 2014) and are nearly three times more likely to have contact with the juvenile justice system (Sedlak and McPherson 2010). Importantly, scholarship on the school-to-prison pipeline also finds exposure to exclusionary discipline increases the risk of criminal legal contact in later life. For example, several studies find that suspended youth are more likely to report a history of incarceration in adulthood (Hemez et al. 2020; Novak 2019; Wolf and Kupchik 2017).
Although stress process theory is a useful framework for understanding how exclusionary discipline, as a stressor, plays a role in health patterning, other frameworks may be better positioned to explain how the timing of this type of stress exposure may determine the shape and direction of health patterns throughout the life course. For instance, the life course perspective is a prominent framework used to understand how early life conditions impact health patterns over time (Corna 2013; Elder and Giele 2009; Jones et al. 2019; Pavalko and Caputo 2013; Pearlin et al. 2005). In the next section, we provide an overview of the life course perspective and the general frameworks used when investigating health patterns over time.
The Life Course Perspective, Exclusionary Discipline, and Health over Time
The life course perspective posits that health changes as people age and that individual age-graded trajectories of health are often determined by the unequal distribution of and exposure to chronic stressors that accumulate over time. Using this framework, a large body of scholarship continues to underscore the profound impact of early life conditions on long-term health (Corna 2013; Elo 2009; Pearlin et al. 2005). For instance, studies find being exposed to and having to cope with stressors such as adverse familial experiences and/or socioeconomic disadvantages in childhood significantly shape health and mortality trajectories in adulthood (Austin 2018; Bellis et al. 2019; Gruenewald et al. 2012; Haas 2008; Montez and Hayward 2014). Although most scholarship on the early foundations of health and mortality continues to highlight the importance of family and socioeconomic conditions, questions concerning how school-related events and/or conditions are related to long-term health remain unanswered.
Although there is broad agreement that health patterning over the life course is a function of age and that the magnitude and direction of patterns between groups are driven by social exposures, there are varying perspectives on how and why health patterns change throughout the life course. Currently, three hypotheses are commonly used to explain age-based health patterns: (1) the aging-as-leveler hypothesis, (2) the persistent inequality hypothesis, and (3) the cumulative disadvantage/advantage hypothesis. The aging-as-leveler hypothesis argues that aging reduces the gap in health observed by a range of socioeconomic differences over time. More specifically, health differences between disadvantaged and advantaged groups diminish or converge over time due to age-related declines in physiological reserves and resilience (Ferraro and Farmer 1996). In contrast, the persistent inequality hypothesis suggests that health disparities remain constant throughout the life course. According to this hypothesis, the sociodemographic mechanisms that underpin health disparities in the United States are stable over time. As such, we should expect health disparities between groups to persist across the life span, challenging the notion that age could act as a leveler (Brown, O’Rand, and Adkins 2012; Ferraro and Farmer 1996; Henretta and Campbell 1976).
Lastly, the cumulative disadvantage/advantage hypothesis asserts that health disparities between more and less advantaged populations widen with age. According to this hypothesis, advantaged groups accumulate more social, economic, and political resources as they age, which supports better health outcomes. Meanwhile, less advantaged groups accumulate more disadvantages over time, leading to deteriorating health patterns (DiPrete and Eirich 2006; Ferraro and Shippee 2009; O’Rand 1996). Taken as a whole, the cumulative disadvantage/advantage hypothesis emphasizes the role of accumulated resources or their absence in shaping health disparities over the life course.
Gaps in the Literature
Despite growing attention on the potential health consequences associated with exclusionary discipline, several gaps remain. First, this understudied area of scholarship focuses predominately on mental health and health behaviors, and findings are often mixed (Hemphill et al. 2012; So et al. 2024; Sutherland and Shepherd 2001; Wolf and Kupchik 2017). For instance, some scholars find school suspension does not significantly increase the risk of depression or anxiety (Wolf and Kupchik 2017), whereas others find significant associations between exclusionary discipline and current depression and anxiety (So et al., 2024). The limited health behavior scholarship focuses mostly on tobacco use and finds significant associations between a history of school suspension and tobacco use (Hemphill et al. 2012; Sutherland and Shepherd 2001). Although this body of scholarship provides evidence suggesting exclusionary discipline plays a role in certain health-related outcomes, questions concerning the broader health consequences of exclusionary discipline remain unanswered. Guided by stress process theory and the existing literature highlighting the deleterious consequences associated with exclusionary discipline, it is plausible that youth who have a history of being exposed to school suspension may perceive their health to be worse than those who have not been exposed to this form of school punishment. To our knowledge, however, scholars have yet to test this assertion.
Second, although emerging evidence highlights disparities in health by exposure to school suspension, most focus primarily on one period of the life course, adolescence. Although exposure to this form of punishment typically occurs during adolescence, only focusing on the potential health consequences during this stage of the life course restricts our understanding of how disparities in health by history of school suspension may vary over time. The core tenants of the life course perspective suggest that exposure to punitive school disciplinary practices—which are often connected to the accumulation of other negative social, criminal legal, and economic consequences—has the potential to play a role in disparities in health throughout the life course. Yet questions about whether and how exclusionary discipline is associated with age-graded health patterns remain unanswered.
Present Study
Using nationally representative panel data and drawing from stress process theory and the life course perspective, the present study fills these gaps in the literature by examining whether and how exclusionary discipline determines individual-level age trajectories of health. Specifically, using five waves of data from the National Longitudinal Study of Adolescent to Adult Health (Add Health) and mixed-effects growth curve ordinal models, we examine how exposure to school suspension plays a role in self-rated health from adolescence to midlife. As such, the present study has two primary research aims: (1) determine whether exposure to school suspension is associated with poorer health in adolescence and (2) assess the role of school suspension on age-graded self-rated health patterns from adolescence to midlife.
Methods
Data
Data were drawn from Waves I through V of Add Health, a sample of approximately 20,000 adolescents in Grades 7 through 12, attending 132 schools in 1994–1995 (Wave I). The school sample is a stratified random sample of all schools in the United States, stratified by region, school size and type, racial/ethnic composition, grade level, and curriculum. Wave I incorporated an in-school survey administered to every student in participating schools (N = 90,118), followed by an in-home interview (N = 20,745) of randomly selected students from the in-school survey. Baseline interviews from the in-home interviews were followed by three additional in-home interviews in 1996 (Wave II), 2002–2003 (Wave III), 2007–2008 (Wave IV), and 2016–2018 (Wave V), with a response rate ranging from 72 percent to 88 percent across all five Add Health waves (Harris et al. 2019).
Measures
Self-rated health
Self-rated health was measured at each wave and was derived from a question asking respondents to rate their health as excellent, very good, good, fair, or poor. For each wave, measures were coded as 1 for excellent health and 5 for poor health. As mentioned earlier, self-rated health is a reliable and valid indicator of general health status and is highly correlated with morbidity.
School suspension
School suspension serves as the primary independent variable for this study. School suspension captured whether the respondent had been suspended from school at or before the Wave I interview.
Time
Time was represented by the age of the Add Health respondent. Age was calculated as the difference between interview month and year and year and month of birth. Age was repeated across Waves I through V and centered on the individual mean age of the participant.
Controls
We also account for several individual and family measures that are likely to be associated with school suspension and/or self-rated health. These factors include racial and ethnic background, gender, immigrant generation, family structure, parents’ education, governmental assistance, school belongingness, family relations, and parent self-rated health. All control measures were captured at Wave I. Race and ethnicity was measured using a respondent’s self-reported racial and ethnic background and includes categories for White, Latinx, and Black Americans. Gender was measured using a dummy variable with male as the reference. Immigrant generation was measured using the respondent’s and the respondent’s parent’s country of birth and includes three categories: first generation (foreign-born), second generation (children of immigrants), and third generation-plus. Respondents categorized as first generation were born outside the United States to at least one parent born outside the United States. Second-generation respondents were born in the United States to at least one parent born outside the United States. Respondents were considered third generation-plus if they were born in the United States to U.S.-born parents. Family structure assessed whether respondents were living in a two-parent household. Governmental assistance captured whether parents reported receiving governmental assistance, such as welfare. Parent’s education was measured using three dummy variables: less than high school, high school graduate, and more than high school diploma.
School belongingness was assessed using five indicators that focus on students’ perceptions of school security, comfort, happiness, and prejudice. These items were assessed using a 5-point Likert scale, where 1 signified strongly agree and 5 signified strongly disagree. All items were reverse-recoded. The school belonging index represents the mean of the five items, with higher scores representing a stronger sense of school belongingness (Cronbach’s α = .76). Family relations was assessed using six items that gauged respondent’s levels of satisfaction with multiple aspects of their familial relationships. These items captured perceptions of parental care, familial understanding, attention from family, and feelings of closeness to both the mother and father. The family relations index represents the average of the six items, with higher scores representing more positive family relations (Cronbach’s α = .74). Similar to the outcome measure, parent self-rated health was derived from a question asking a parent to rate their health as excellent, very good, good, fair, or poor. The final measure for parent self-rated health was coded as 1 for excellent health and 5 for poor health.
Analytic Strategy
We begin by providing descriptive statistics for the total sample and across exposure to school suspension. To assess whether there were significant differences in our key measures by school discipline, we estimated tests for differences, as indicated in Table 1. We then use mixed-effects growth curve models to estimate the longitudinal associations between school suspension and self-rated health from adolescence to midlife. Mixed-effects growth curve models are well suited for examining individual change over time because the models generate individual trajectories that are determined by person-specific intercepts (initial value) and slope (rate of change) estimates that demonstrate changes in health patterns as a function of age (Raudenbush and Bryk 2002).
Descriptives for the Overall Sample and by School Suspension.

p < .001.
In all models, observations were nested within individuals, and a random intercept was included at the individual level. Given that self-rated health is an ordinal outcome, we used mixed-effects growth curve ordinal logit models. These models have an established history in empirical research using repeated measure ordinal data (Hedeker and Gibbons 1994).
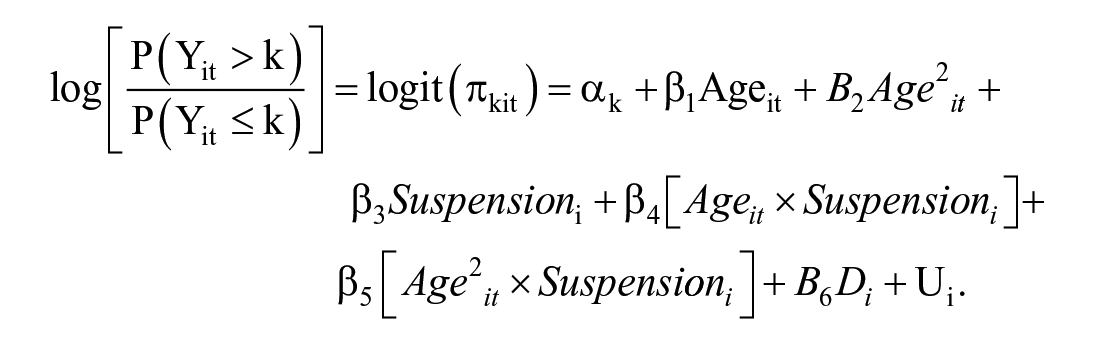
For self-rated health categories k = 1, 2, 3, 4, 5, c – 1, the mixed-effect ordinal logit model can be specified as follows:

where
To test whether the relationships between school suspension and self-rated health vary from adolescence to midlife, we include interactions between exposure to school suspension and age. The following equation describes the basic structure of the interaction model:
To avoid potentially biased estimates resulting from incomplete data, we utilized full information maximum likelihood (FIML) estimation to account for missing data under the assumption that nonresponses were missing at random. FIML estimation allowed respondents with at least one valid measure of self-rated health across Wave I through V, including those who dropped across the observation period, to remain in the analyses. SAS Version 9.4 was used for data management, and STATA Version 16 was used for all analysis.
Results
Table 1 presents a summary of the descriptives statistics for all measures by exposure to school suspension. Results reveal more than a quarter of respondents (26 percent) reported a history of school suspension at or before the Wave I interview. Table 1 also shows most of the sample were White (60 percent), third generation-plus (83 percent), female (53 percent), and living in a two-parent household (52 percent) and had parents with more than a high diploma at Wave I (58 percent). We also observe that the average self-rated health scores slightly decline from the baseline interview to Wave III but increase in Waves IV and V.
Shifting to patterns by exposure to school suspension, we find that compared to respondents who report no exposure to exclusionary discipline, respondents with a history of school suspension had significantly higher average self-rated health scores, indicating poorer health, across all five Add Health waves. Consistent with prior literature, we also find Black and Latinx respondents were more likely to experience school suspension compared to their White counterparts. Results from Table 1 also indicate that compared to males, females were less likely to report school suspension. Finally, a greater sense of school belongingness and family relations decreased the likelihood of school suspension.
We present estimates from the mixed-effects growth curve ordinal logit models in Table 2. To provide a baseline understanding of general self-rated health patterns from adolescence to midlife, we begin by providing estimates of the initial level and rate of change for self-rated health net of controls. Results indicate that the negative fixed linear growth component and positive quadratic term were statistically significant, demonstrating that the average population rate of change is nonlinear. More specifically, the negative coefficient for age (−.06, p < .001) and the positive coefficient for age2 (.001, p < .001) demonstrates that the overall rate of change for self-rated health is decreasing at an increasing rate.
Poorer Self-Rated Health from Adolescence to Midlife.

p < .05. **p < .01. ***p < .001.
Although unstandardized coefficients and odds ratios from the ordinal logit model provide scholars with a general direction of associations, they are not intuitive. To better illustrate individual-level age-aged self-rated health trajectories, we plotted predicted probabilities for excellent, fair, and poor self-rated health in Figure 1. Results demonstrate that as youth age into later stages of the life course (i.e., young adulthood and midlife), the probability of reporting excellent health decreases, whereas the probability of reporting fair and poor health decreases from adolescence to midlife. Importantly, patterns from Figure 1 indicate that notable changes in self-rated health emerge in the late 20s and early 30s, suggesting this may be a critical turning point for health from adolescence to midlife. Results from Model 1 in Table 2 also show that exposure to school suspension is significantly related to self-rated health. Specifically, compared to respondents with no history of school suspension, suspended respondents were more likely to report poorer health (.24, p < .001) at baseline.

Age trajectories of excellent, fair, and poor self-rated health.
Model 1 assumes self-rated health patterns from adolescence to midlife are the same for suspended and nonsuspended youth. In Model 2, we relax this assumption by including age and suspension interactions. Results from Model 2 demonstrate that intercepts and slopes significantly vary by exposure to school suspension. To ease in the interpretation of results, Figure 2 illustrates the shape and direction of individual-level self-rated health trajectories for each response category by history of school suspension net of controls. Compared to respondents with no history of suspension, Figure 2 illustrates that suspended respondents exhibit a lower probability of reporting excellent health from adolescence to midlife. Finally, Figure 2 shows that suspended youth are more likely to report a higher probability of fair and poor health in adolescence, with the disparity between suspended and nonsuspended youth expanding over time.

Age trajectories of excellent, fair, and poor self-rated health by school suspension.
Discussion and Conclusion
The impact of exclusionary discipline on health disparities over the life course remains largely unexplored. Using nationally representative panel data and guided by stress process theory and the life course perspective, we begin to address this gap in knowledge by examining whether and how exposure to school suspension is related to self-rated health patterns from adolescence to midlife. In doing so, this study advances understanding of the dynamics of school suspension and health across the life course.
This study offers two contributions to the literature. First, results from our mixed-effects growth curve ordinal models reveal that exposure to exclusionary discipline plays a significant role in self-rated health patterning in adolescence. Specifically, when compared to youth with no history of school suspension, our results indicate that respondents with a history of school suspension were more likely to report poorer health during this critical developmental period. This finding provides evidence that exposure to exclusionary discipline actions, such as school suspension, can act as a source of stress that can negatively impact perceptions of health in adolescence. Moreover, this finding contributes to an increasingly important area of research that explores the role of school policy and practice on adolescent health (Bonell et al. 2019; Leurent et al. 2021). While most adverse childhood experience literature focuses on the family (Petruccelli, Davis, and Berman 2019), this finding underscores how adverse school-related mechanisms have the potential to negatively impact health patterns in adolescence.
Second, results from this study reveal that the effect of school suspension on self-rated health varies with age, contributing to the robust body of literature on age patterning of health disparities. Results from our analysis indicate that compared to respondents with no history of school suspension, respondents with a history of school suspension were more likely to report poorer health from adolescence to midlife. More specifically, we find that compared to individuals with no history of school suspension, the likelihood of reporting excellent health from adolescence to midlife was lower for individuals with a history of school suspension. The average excellent health trajectory for suspended youth can be characterized as one of persistent inequality. Rather than excellent health trajectories diverging between suspended and nonsuspended youth, the gap between the two groups remained relatively stable. On the other end of the self-rated health spectrum, compared to nonsuspended youth, those with a history of suspension were more likely to report fair and poor health from adolescence to midlife, with the gap growing substantially into midlife. In contrast to the average excellent health trajectories, the fair and poor health age patterns can be characterized as an acceleration of poorer perceptions of health for suspended youth. Suspended youth, who had slightly higher probabilities of reporting fair and poor health in adolescence, experienced a more rapid perception of fair and poor health from their late 20s into midlife.
Taken as a whole, our growth curve estimates provide support for both the persistent inequality (Brown et al. 2012; Ferraro and Farmer 1996; Henretta and Campbell 1976) and cumulative disadvantage/advantage hypotheses (DiPrete and Eirich 2006; Ferraro and Shippee 2009; O’Rand 1996). Although the mechanisms behind the age-graded self-rated health patterns observed in this study remain unclear, they may be linked to other stress exposures tied to exclusionary discipline. These exposures include but are not limited to interactions with the criminal legal system and reduced economic opportunities (Monahan et al. 2014; Novak 2019; Wolf and Kupchik 2017). Although this study establishes important linkages between school suspension and self-rated health inequalities over the life course, the investigation into whether and how other stressors, such as criminal legal contact or socioeconomic challenges, play a role in exclusionary discipline self-rated health relationships is beyond the scope of this study. As such, future studies should investigate how other stressors related to this form of school punishment are associated with school suspension-health relationships. Focusing on the potential role of other stressors will enhance our understanding of how various forms of stress exposure tied to exclusionary discipline contribute to health disparities throughout the life span.
This study has several limitations. First, although self-rated health is a widely used health indicator (Bailis et al. 2003; Chandola and Jenkinson 2000), it represents one of several health measures used in contemporary survey research. It is plausible that depending on the type of health outcome, we may observe individual-level age trajectories that do not align with patterns observed in this study. As a result, scholars should include a range of health indicators in future research to assess whether individual-level age trajectories are consistent across outcomes for youth with a history of school suspension. Second, due to data limitations, we were unable to account for the frequency and duration of school suspension in adolescence. Additionally, although we were able to capture exposure to school suspension, we were unable to assess other types of exclusionary discipline, such as in-school suspension and expulsion. To better assess the long-term health consequences tied to exclusionary discipline, survey instruments designed to capture school experiences should not only incorporate more robust measures of school punishment but also assess the frequency, duration, and severity of various exclusionary discipline practices. Similarly, due to design constraints, we were unable to incorporate important time-variant measures, such as family income, that have been shown to play a role in health patterning over the life course (Kim and Durden 2007).
Although the Add Health has fairly high response rates across all five waves (Harris et al. 2019), sample attrition and missing data due to nonresponses should also be taken into consideration when interpreting results. Research finds that among men, those who are younger, have lower socioeconomic statuses, and consume alcohol were more likely to be nonrespondents, whereas older women are more likely to be nonrespondents in panel studies (Caetano, Ramisetty-Mikler, and McGrath 2003). Given that demographic differences in nonresponse patterns can impact outcome and predictor variables, future studies should attempt to replicate the findings presented in this study.
Although this study uses repeated measures for self-rated health, it is also challenging to disentangle whether poorer self-rated health patterns over time are a direct consequence of suspension or whether youth with preexisting health issues were more likely to be suspended. This ambiguity could potentially be addressed in future research with causal inference techniques, such as propensity score matching or instrumental variable approaches, to better establish the directionality of relationships. Finally, findings from this study may not be generalizable to other educational contexts where exclusionary discipline practices and their consequences might differ. Future research should explore whether similar patterns are observed in other countries with different disciplinary practices and educational systems.
Despite these limitations, this study contributes to the extant literature on age patterning of health disparities by elucidating how school suspension is associated with self-rated health patterns from adolescence to midlife. Our findings—which partially support the persistent inequality (Brown et al. 2012; Ferraro and Farmer 1996; Henretta and Campbell 1976) and the cumulative disadvantage/advantage hypothesis (DiPrete and Eirich 2006; Ferraro and Shippee 2009; O’Rand 1996)—reveal that compared to youth with no history of school suspension, suspended youth experience (1) poorer health in adolescence, (2) a persistent health gap in excellent health from adolescence to midlife, and (3) a more rapid acceleration of fair and poor health from their late 20s to midlife. Overall, findings from this study not only highlight the immediate health repercussions of school suspension for adolescents but also underscore the long-lasting influence of punitive school punishment practices on health into midlife.