
Abstract
Power dynamics in social interactions likely affect individuals’ ability to use their preferred contraception, yet research has primarily emphasized financial barriers. Using data from a national survey of people assigned female at birth, we apply a social-ecological framework to assess a broader range of factors shaping nonpreferred use. Over one-quarter of respondents were not using their preferred method; among them, nearly half preferred vasectomy, condoms, or withdrawal. Partner disagreement was the most common reason for nonpreferred use and was associated with experiencing partner contraceptive coercion. Black women, who face structural racism in the health care system, were more likely to attribute their nonpreferred use to a provider’s recommendation. These findings demonstrate how gender and power shape contraceptive use despite the preferences of those at risk of pregnancy, highlighting the need for cultural, policy, and health care shifts to resolve contraceptive preference-use discordance and increase gender equity in the responsibility of pregnancy prevention.
Recent national studies show that one in four individuals capable of pregnancy in the United States is not using their preferred contraceptive method (Frederiksen et al. 2022; Gomez et al. 2024). Using a preferred method is an indicator of reproductive autonomy, or one’s agency over their childbearing and reproductive health decisions (Potter et al. 2019; Shalev 2000). Preferred contraceptive use has additional benefits: those who use the contraception they want are more likely to continue using that method (Beesham et al. 2022; Burke, Thaxton, and Potter 2021; Ela et al. 2022; Pariani, Heer, and Van Arsdol 1991), feel a sense of efficacy in their method use (Chakraborty et al. 2021), and have a lower risk of becoming pregnant when they do not want to (Potter et al. 2016). Particularly in light of the increasingly restrictive abortion access landscape in the United States (Baden and Driver 2023), these consequences underscore the importance of supporting people to use their preferred contraceptive method from human rights and population health perspectives.
Addressing discordant contraceptive use and preferences requires examining a range of factors because sex and contraceptive use are social processes mediated by structural inequalities and interactions laden with power dynamics. To date, research has primarily focused on cost as a barrier to preferred method use, highlighting the role of economic inequality in patterning reproductive autonomy (Burke, Potter, and White 2020; Kavanaugh, Pliskin, and Hussain 2022). Although affordability is a key component of contraceptive access (Holt et al. 2020), the social-ecological model suggests that individuals’ health behaviors and outcomes are embedded in their larger social environments, which include and extend beyond their economic resources (McElroy et al. 1988; Stokols 1996). Important insights from sociological literature have surfaced the gendered power dynamics shaping contraceptive behavior at varying levels of influence, from the development of birth control technology to the interpersonal dynamics with providers and within heterosexual partnerships (Kammen and Oudshoorn 2002; Kimport 2018b; Littlejohn 2021). These perspectives emphasize how social forces, including gender and power, constrain reproductive choices and likely contribute to nonpreferred contraceptive use.
In this article, we build on prior research that has identified the relatively high prevalence of unsatisfied contraceptive preferences in the United States by evaluating a variety of barriers to preferred method use and situating them in their social and structural context. We do so by analyzing data from a new national survey of people assigned female at birth, which enacts recent guidance to broaden the conceptualization of barriers to enacting contraceptive preferences beyond the narrow scope of cost (Burke and Potter 2023) and allows us to look across a range of social-ecological levels of influence on preferred contraceptive use (Holt et al. 2020).
By quantitatively evaluating reasons for nonpreferred use, our findings extend research on contraceptive preferences by highlighting mechanisms through which gender and power contribute to preference-use mismatches. We find that partner disagreement is the most common reason that people are not using their desired method of contraception, followed by cost and accessibility. Reporting partner disagreement as a reason for nonpreferred use is associated with having experienced partner contraceptive coercion. Moreover, nearly half of those not using their preferred method would prefer to use a male-based method, including one-quarter who would prefer vasectomy. We also found that Black women, who have faced historical and ongoing provider bias and coercion as a function of structural racism (Gomez and Wapman 2017; Roberts 1999), are more likely than White women to report not using their preferred contraceptive method due to a provider’s recommendation, highlighting the influence of unequal power dynamics between providers and patients. These findings illustrate how gendered structures and power dynamics shape contraceptive decision-making despite the desires of those at risk of pregnancy.
Background
Evaluating Contraceptive Preferences
In response to ongoing calls to prioritize autonomy in evaluating reproductive health care (Bruce 1990; Potter et al. 2019; Senderowicz 2020), a rapidly growing body of literature examines whether individuals are using their preferred method of contraception (for an overview, see Burke and Potter 2023). This approach is distinct from the traditional focus on contraceptive prevalence, which often uncritically characterizes higher prevalence or more effective contraceptive use as favorable outcomes. For instance, the U.S. Department of Health and Human Services’s public health objectives explicitly call for increasing the use of “effective birth control” among those at risk of unintended pregnancy, irrespective of individual preferences (U.S. Department of Health and Human Services 2020). By contrast, assessing contraceptive preferences and whether they are met aims to capture a dimension of individuals’ autonomy: Do people have the agency to use the contraception they want to and thus exert control over their reproductive outcomes? This perspective acknowledges that using a method does not necessarily mean that an individual’s preferences are satisfied and that various factors can influence reproductive autonomy depending on one’s social context.
Research has primarily highlighted affordability as a barrier to preferred method use. In the context of the United States’s highly stratified health care system, barriers to contraceptive access rooted in economic inequality are extremely salient, and research has consistently identified how cost, affordability, and accessibility shape access to reproductive health services and contraceptive use (Dennis and Grossman 2012; Eisenberg, McNicholas, and Peipert 2013; Fuentes et al. 2023; Kavanaugh, Pleasure, et al. 2022). Consequently, numerous studies have illuminated cost as a significant factor shaping nonpreferred method use (Burke et al. 2020; Chakraborty et al. 2021; Frederiksen, Ranji, and Long 2021; Frederiksen et al. 2022; Frohwirth et al. 2022; Gomez et al. 2024; He et al. 2016; Kavanaugh, Pliskin, and Hussain 2022). Starting in 2015, the National Center for Health Statistics National Survey of Family Growth (NSFG) explicitly highlighted concerns about affordability through their inclusion of a question asking if respondents would prefer to use a(nother) contraceptive method in the absence of cost (National Center for Health Statistics 2018). Using data from the 2015–2017 NSFG, Burke et al. (2020) found that 22 percent of women at risk of unplanned pregnancy were not using their preferred method due to cost; women who were Black and Hispanic, ages 15 to 24, or living on low incomes were more likely to report cost barriers to using their preferred method.
Expanding the Scope of Influence: Gender, Power, and Contraceptive Use
The focus on cost as a barrier to preferred contraceptive use needs to be expanded to recognize that using a contraceptive method involves social interactions with formal and informal health care systems, health care providers, and/or partners. Each of these interactions may be laden with social and structural dynamics that shape whether individuals can use their preferred contraceptive methods. A social-ecological perspective considers how an individual’s health behaviors and outcomes are embedded in and a product of their social environment, spanning micro to macro levels of influence (McElroy et al. 1988; Stokols 1996). Recently, Holt et al. (2020) adapted this multilevel framework to develop a model of contraceptive care, explicitly accounting for community and family; policy and health systems; and historical, social, and political contexts as layers of social-ecological influence on contraceptive behavior. We adopt Holt et al.’s framework, which highlights how contraceptive practices reflect an individual’s social location, to fill a key gap in the literature by broadening the investigation of reasons for nonpreferred contraceptive use and evaluating variation therein.
Sociological literature on contraceptive use underscores gender as a central power structure operating at all levels of the social-ecological continuum through hegemonic masculinity—or dominant understandings of ideal masculine behavior, propped up by both culture and structure, that normalize and perpetuate the subordination of women (Connell and Messerschmidt 2005). Identifying the mechanisms behind nonpreferred method use requires attention to these power dynamics, which result in a gendered division of reproductive labor, mirroring the unequal burden women face in household and emotional labor (Bertotti 2013; Fennell 2011; Kimport 2018a; Littlejohn 2021).
At a historical, social, and political level, the history of the development of contraceptive technologies throughout the late 1900s largely excluded contraceptive use from masculine behavior (Oudshoorn 2004). The development of the pill and subsequent methods of pregnancy prevention have focused on the bodies of people capable of pregnancy, leading to disparate options and ultimately, disparate responsibility by sex. The Affordable Care Act’s contraceptive coverage guarantee also offers a policy enactment of this woman-centric approach by excluding male-based methods, such as condoms and vasectomy, from the options available at no cost to insured individuals (Sonfield 2015). Hegemonic masculinity and gender inequality made manifest in such policies may deter people from using these methods despite their attributes that users may find desirable, such as condoms’ protection against sexually transmitted infections, vasectomies being less invasive than tubal ligations, and both carrying fewer side effects compared to many female-based methods (Jackson et al. 2016; Marshall et al. 2016).
In health systems, hegemonic masculinity and power dynamics seep into patient-provider interactions, often limiting or biasing the information provided about specific methods in such a way that may interfere with people’s ability to use their desired method. The discussion of male-based methods is marginalized in women’s contraceptive counseling, furthering the notion that pregnancy prevention is a woman’s responsibility (Kimport 2018b). In focusing on women’s contraceptive behavior, providers may bring unconscious biases into contraceptive counseling based on their perception of clients’ identities (Gomez and Wapman 2017; Mann, Chen, and Johnson 2022) or explicitly deny or promote certain methods to clients based on specific criteria, such as age or parity guiding the provision of a tubal ligation (Arora, Castleberry, and Schulkin 2018; Lawrence et al. 2011). Meanwhile, men report very low rates of counseling on vasectomy, with fewer than 2 percent of men ages 15 to 44 having discussed vasectomy with their provider in the last year (Borrero et al. 2010).
Furthermore, numerous studies have shown that power dynamics in sexual relationships affect contraceptive behaviors, ranging from subtle to violent. Men may openly reject condoms or vasectomies (Davis et al. 2019; White et al. 2022) or deploy “strategic silence” around the discussion of contraception with their partner (Dalessandro, James-Hawkins, and Sennott 2019), leaving women to initiate the conversation or use methods that do not directly involve their partner (Fennell 2011). In heterosexual relationships, women are more likely than men to privilege their partner’s pleasure and convenience (Armstrong, England, and Fogarty 2012; Higgins and Hirsch 2008), resulting in a deference to men’s implicit or explicit desires around male-based contraception (Littlejohn 2021). Notably, men’s control over contraceptive behaviors can also present as overt violence, such as contraceptive sabotage, which deliberately undermines women’s preferences and agency (Dimenstein et al. 2021; Rowlands and Walker 2019).
Importantly, gendered power intersects with other biases and power dynamics present in health systems, provider interactions, and intimate relationships based on characteristics, including race, age, and sexual orientation, further complicating contraceptive agency for multiply marginalized groups (Eeckhaut and Hara 2023; Gomez and Wapman 2017; Higgins et al. 2019; Higgins, Kramer, and Ryder 2016; Manzer and Bell 2022). Although research has shown how these layers of power in partnerships and care environments influence contraceptive use as an outcome, they also likely influence individuals’ ability to satisfy their contraceptive preferences for reasons beyond cost, resulting in a mismatch between method use and desire (Fay et al. 2022).
Altogether, the influence of hegemonic masculinity across the social-ecological continuum results in what Littlejohn (2021) terms “gendered compulsory birth control,” whereby systems of power discipline individuals capable of pregnancy into being primarily responsible for pregnancy prevention. This dynamic compels women to use contraceptive methods developed for female bodies, which they may not prefer or desire, thereby limiting their reproductive autonomy. The societal relinquishment of men’s responsibility in pregnancy prevention can leave women to navigate a landscape where their contraceptive choices are constrained by the double bind of their method preferences and their desire to avoid pregnancy, all situated in the gendered power structures entrenched in health care systems, policies, and intimate relationships.
Methods
Data
Secondary data for this analysis came from the 2021 Guttmacher Survey of Reproductive Health Experiences, a national online survey conducted in July and August 2021. The survey was conducted in English, and eligible respondents were ages 18 to 49, assigned female at birth, and had ever had penile-vaginal intercourse (PVI). NORC at the University of Chicago managed survey recruitment and fielding using a dual-sampling approach based on both NORC’s AmeriSpeak panel, a nationally representative probability-based panel, and a nonprobability online opt-in sample, which recruited based on enrollment targets for age, race/ethnicity, and education to approximate the U.S. population. The full sample included 6,536 respondents: 3,170 from the probability sample and 3,366 from the nonprobability sample. Combining these samples maximized the sample size, enhancing stability in estimates for smaller subpopulations, such as those not using their preferred contraceptive method. NORC provided sampling weights via their TrueNorth calibration service, which uses small area estimation to minimize bias from the nonprobability sample (NORC at the University of Chicago 2021). 1 These weights were designed to generate estimates representative of the U.S. population ages 18 to 49 who were assigned female at birth and had ever had PVI. Data from this survey are publicly available (Haas and Mueller 2023) and have been used in other research on contraceptive access (Lindberg et al. 2021, 2022). The Guttmacher Institute and NORC institutional review boards approved the original data collection. All respondents provided informed consent to participate.
Given our interest in contraceptive preferences and method use, we limited our analyses to respondents who were not pregnant, not trying to become pregnant, and had PVI in the last 30 days (n = 4,071). We also excluded those who reported hysterectomies (n = 139) and used listwise deletion to remove cases missing information on covariates (n = 111). Our final analytic sample included 3,821 respondents.
Measures
Current contraceptive use
Information on current contraceptive use was ascertained by asking separately about noncoital and coital methods used in the last 30 days, reflecting research indicating this approach increases the accuracy of reporting of noncoital methods (Barber, Kusunoki, and Gatny 2011; Jones, Lindberg, and Higgins 2014). Respondents were first asked, “In the past 30 days, which of the following contraceptive methods have you used, even if you used them for reasons other than pregnancy prevention?” Response options included the pill, patch, ring, shot, implant, IUD, tubal ligation, and none of the above. In a separate question, they were asked to report which coital and/or partner-based method(s) they used at least once in the last 30 days when they had PVI, including withdrawal, condoms, fertility awareness-based methods, the diaphragm, emergency contraception, vasectomy, another method, or none of the above.
Contraceptive preferences
Respondents were asked, “If you could use any contraceptive method that you wanted right now, what method(s) would you use?” They could select as many methods as they wanted, including “I am using the method that I want to use.” Those who were not currently using a form of contraception were offered the additional response option, “I am satisfied not using a method.”
Using preferred method
We compared respondents’ answers to current and preferred method questions to generate our key outcome variable, an indicator of whether they were using their preferred method of contraception. Although both method use and preference questions were asked in a “select all” format, for ease of exposition in this analysis, we compared the most effective method a respondent used during the last 30 days and the most effective method they preferred. We acknowledge that this approach prioritizes efficacy, which may differ from how people construct their preferences (Higgins and Smith 2016; Jackson et al. 2016; Littlejohn 2021; Marshall et al. 2016). Stemming from this concern, we conducted two sensitivity analyses around this analytic decision. First, we used an indicator of whether respondents were using any of their preferred method(s) as our key outcome. In a second sensitivity analysis, we randomly assigned a preferred method among those selected for respondents who chose more than one method to minimize prioritization of highly effective methods, following Hopkins et al. (2023). Both analyses yielded similar substantive patterns as our main results. Consequentially, we maintained our simplified coding scheme and included the distribution of contraceptive use and preferences in their “check all” form in an appendix table.
Reasons for nonuse of preferred methods
Respondents who indicated a preference for a method other than what they were using were asked their reason(s) for not currently using their preferred contraceptive method. Options included: “I can’t afford it,” “It’s too difficult to get,” “My partner doesn’t agree with using it,” “My provider recommended a different method,” and “Other, specify.” Some 300 respondents selected “other” and provided a write-in response. The authors reviewed these responses together and categorized them into existing reasons in addition to inductively generating two additional categories of reasons for nonpreferred method use: side effects (including method attributes, efficacy concerns, and procedure concerns) and low perceived risk of undesired pregnancy (including those who reported that they were unable or unlikely to become pregnant, were open to pregnancy, infrequently sexually active, or otherwise not motivated to pursue their preferred method). Respondents could report more than one reason for nonpreferred use, and these responses were not method-specific for those who selected more than one preferred method.
Psychosocial influences
We considered measures of pregnancy avoidance and contraceptive coercion as psychosocial factors that may be associated with preferred method use and reasons for nonpreferred use. Pregnancy avoidance was assessed by asking respondents, “How important is it to you to AVOID becoming pregnant now?” (capitalization in original survey item). Responses were recorded on a 5-point Likert scale ranging from “very important” to “very unimportant.” We coded this variable such that higher values indicated heightened importance of pregnancy avoidance.
Partner contraceptive coercion was measured by generating an average of six indicators adapted from the Freedom from Coercion subscale of the Reproductive Autonomy Scale (Upadhyay et al. 2014). Respondents reported their rating of each of the following items on a 4-point scale that ranged from strongly disagree to strongly agree: “My partner has stopped me from using a method to prevent pregnancy when I wanted to use one,” “My partner has messed with or made it difficult to use a method to prevent pregnancy when I wanted to use one,” “My partner has made me use a method to prevent pregnancy when I did not want to,” “If I wanted to use a method to prevent pregnancy my partner would stop me,” “My partner has pressured me to become pregnant,” and “I used a contraceptive method without my partner’s knowledge.” In the Guttmacher Survey of Reproductive Health Experiences, these items had a Cronbach’s alpha of .93, indicating high internal consistency around the concept of partner contraceptive coercion.
Sociodemographic characteristics
We also included measures of sociodemographic characteristics identified in prior literature as associated with contraceptive method use, including age (18–24, 25–34, 35–49), race/ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic/Latinx, and non-Hispanic other/multiracial), household income (less than or greater than 200 percent of the federal poverty level), marital status (married, cohabiting, single/separated/divorced/widowed), education (high school degree or less, some college, bachelor’s degree or greater), current health insurance (privately insured, publicly insured, uninsured). Respondents reported their sexual orientation, which we collapsed into an indicator of whether they were straight or LGB+ (lesbian, gay, bisexual, queer, or another orientation). Because of the small number of respondents who identified as trans or nonbinary, we did not include this measure in our analyses. An indicator of whether respondents had previously given birth was derived from one of two questions, which were randomly assigned to respondents and asked either for their lifetime number of pregnancies resulting in live births or whether they had a pregnancy that resulted in a live birth in their lifetime.
Analytic Strategy
We first described the overall sample of people assigned female at birth who had PVI in the last 30 days and were not pregnant or trying to become pregnant according to sociodemographic and psychosocial characteristics. We estimated descriptive statistics on contraceptive method use and preferences for the full sample and contraceptive method use and preferences among those not using their preferred method. We then estimated the overall prevalence of nonpreferred contraceptive use and fit a multivariable logistic regression model predicting the likelihood of nonpreferred method use using sociodemographic and psychosocial characteristics as independent variables. In this and ensuing multivariable regression models, we included an indicator variable for the sample source (probability or opt-in panel) to net out systematic differences between the samples.
For comparability with the NSFG’s estimate of nonpreferred use due to cost, we next estimated the prevalence of nonpreferred use by reason for the sample overall. Our subsequent analyses focused on the subset of respondents who were not using their preferred method. Among those respondents, we estimated the prevalence of nonpreferred use by reason and fit multivariable logistic regression models with each reason for nonpreferred use as a dependent variable and sociodemographic and psychosocial characteristics as independent variables.
Finally, we described reasons for nonpreferred use by preferred method among those with unsatisfied preferences. To produce stable estimates in this final analysis, we limited our presentation to methods that at least 100 respondents preferred. All analyses were conducted in Stata 18 (StataCorp 2023) using sampling weights generated by NORC to account for the complex sample design.
Results
In this sample of individuals ages 18 to 49 who were assigned female at birth, were not pregnant or trying to become pregnant, and had engaged in PVI in the last 30 days, roughly half were ages 35 to 49, non-Hispanic White, and married (Table 1). Most respondents identified as straight, and household income was relatively evenly split between those above and below 200 percent of the federal poverty level. A bachelor’s degree was the most common educational status (42 percent). Nearly all respondents had some form of insurance, and two-thirds had previously given birth. On average, respondents reported a mean of 1.32 on the partner contraceptive coercion scale (minimum = 1, maximum = 4) and a score of 4.14 on pregnancy avoidance (minimum = 1, maximum = 5). Overall, 89 percent of the sample were using a contraceptive method. More than one in four—28 percent—were not using their preferred method of contraception.
Distribution of Sample Characteristics, Guttmacher Survey of Reproductive Health Experiences 2021.
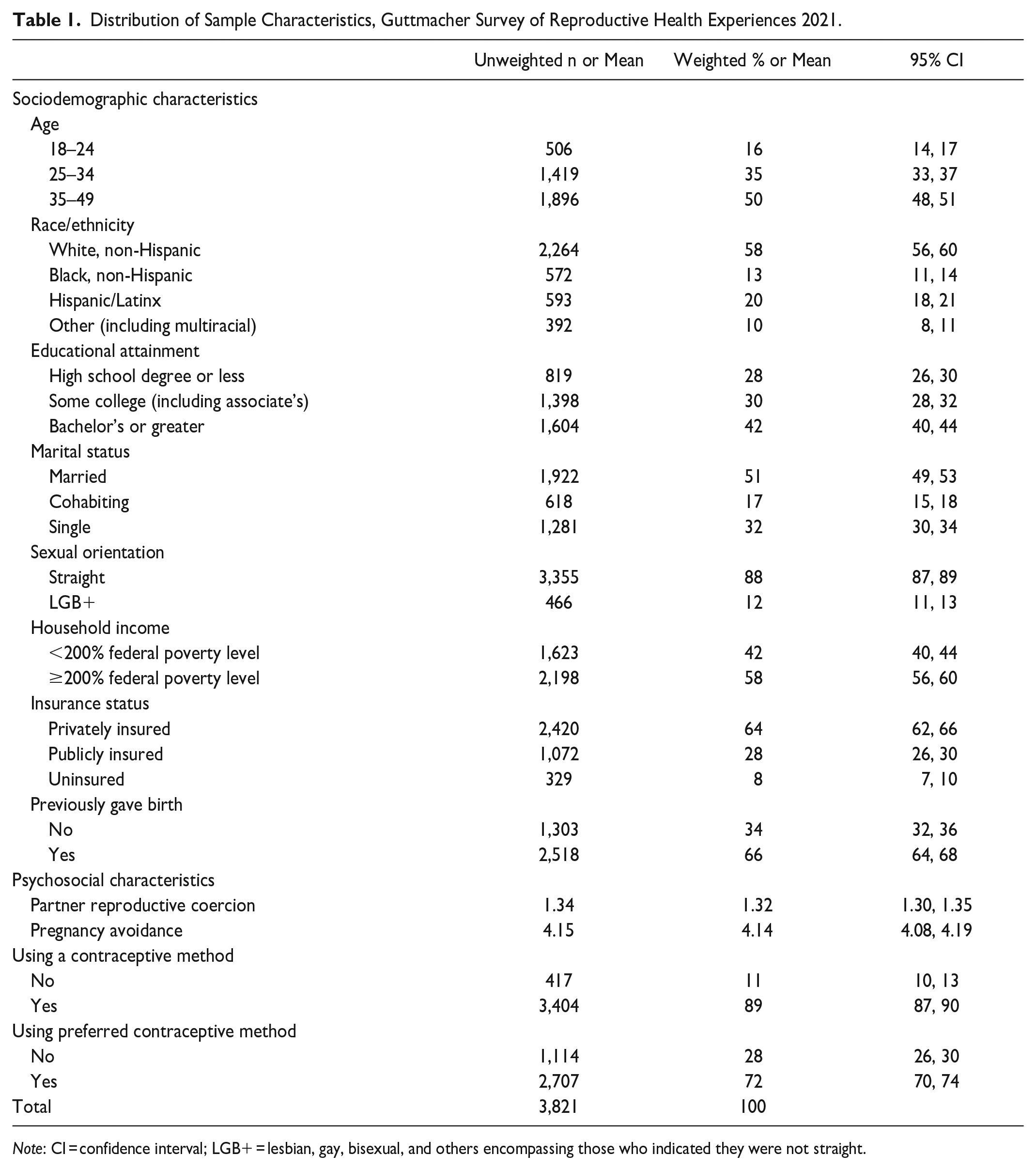
Note: CI = confidence interval; LGB+ = lesbian, gay, bisexual, and others encompassing those who indicated they were not straight.
Figure 1 illustrates the distribution of contraceptive method use and preferences overall and among those with unsatisfied preferences. Overall, the pill (20 percent) and implant or IUD (16 percent) were the most used methods. The pill was also the most preferred method (18 percent), followed by permanent methods (tubal ligation = 16 percent, vasectomy = 16 percent) and the IUD or implant (16 percent). Overall, eight percent of respondents reported that their preference was to use no method.

Distribution of contraceptive method use and preferences overall and among those not using their preferred method, Guttmacher Survey of Reproductive Health Experiences 2021.
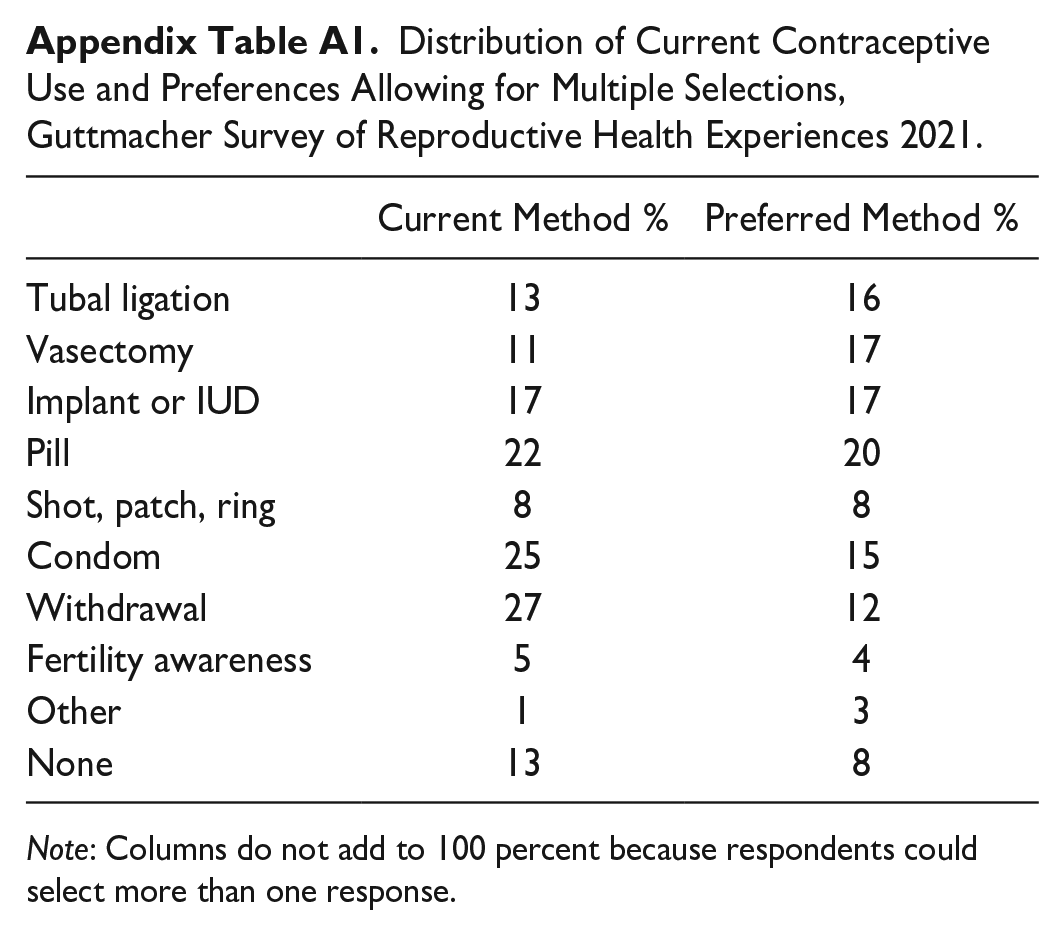
The prevalence of use and preference for certain methods (implant, IUD, shot, patch, or ring) was similar overall and among the subsample who were not using their preferred method. In the overall sample, preferences for tubal ligation and vasectomy were higher than actual use, whereas the opposite was true for condoms, withdrawal, and no contraception. These patterns were more pronounced among those not using their preferred method. Among those with unsatisfied preferences, the most common preference was for vasectomy; one in four respondents in this group wished to use vasectomy for pregnancy prevention. Overall, one-third of the total sample and nearly half of those not using their preferred method expressed a preference for male-based contraception (vasectomy, condom, or withdrawal). In the “check-all” construction of contraceptive preferences (Appendix Table A1), the proportion of the overall sample who preferred male-based contraception rose to 44 percent.
Table 2 presents the distribution of nonpreferred contraceptive use by sociodemographic and psychosocial characteristics. Adjusting for covariates, those ages 18 to 24 were significantly more likely to be using a nonpreferred method than those ages 35 to 49, as were LGB+ respondents compared to those who identified as straight. Respondents using permanent methods or the IUD/implant were more likely to be using their preferred method compared to those using the pill, whereas those using condoms, withdrawal, fertility awareness methods, or no method were less likely. Higher levels of partner reproductive coercion and a stronger desire to avoid pregnancy were also associated with an increased likelihood of nonpreferred method use.
Descriptive Characteristics and Odds Ratios from Multivariable Logistic Regression Analyses Predicting Nonpreferred Contraceptive Use, Guttmacher Survey of Reproductive Health Experiences 2021.
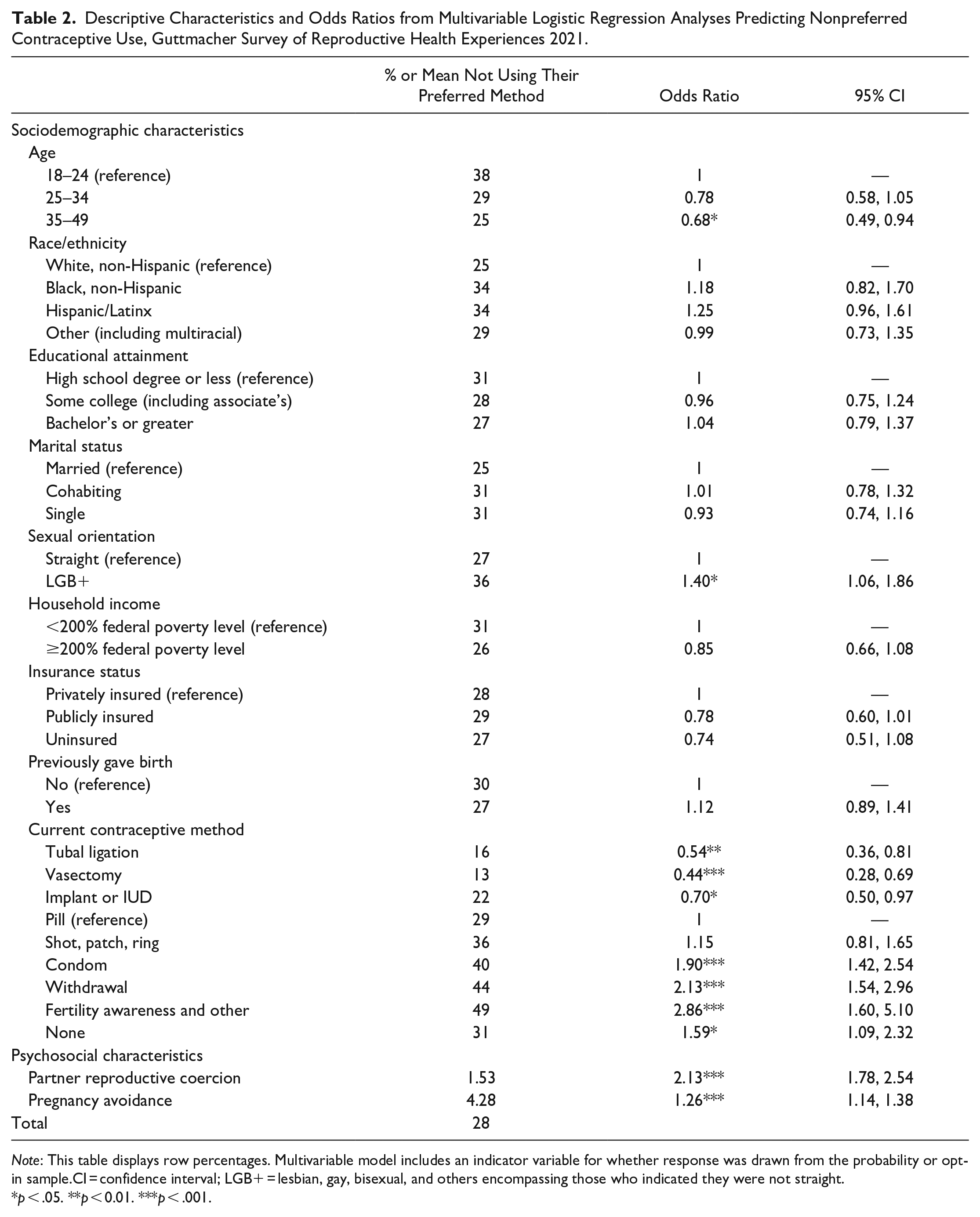
Note: This table displays row percentages. Multivariable model includes an indicator variable for whether response was drawn from the probability or opt-in sample.CI = confidence interval; LGB+ = lesbian, gay, bisexual, and others encompassing those who indicated they were not straight.
p < .05. **p < 0.01. ***p < .001.
The most common reason for nonpreferred method use was partner disagreement (8 percent overall, 28 percent among those not using their preferred method; see Table 3). Providers recommending a method different than what a respondent preferred was a reason for not using their desired method reported by 5 percent of respondents overall and 19 percent of those with unsatisfied preferences. Structural barriers of affordability and accessibility were cited as reasons for nonpreferred use by 5 percent and 6 percent of the overall sample and 17 percent and 21 percent among those not using their preferred method, respectively. Concerns about side effects and low perceived risk of undesired pregnancy were the least commonly reported reasons behind unsatisfied preferences. Among those with unsatisfied preferences, 9 percent chose more than one reason for nonpreferred use.
Descriptive Characteristics and Odds Ratios from Multivariable Logistic Regression Analyses Predicting Nonpreferred Contraceptive Use by Reason among Those Not Using Their Preferred Method Of Contraception, Guttmacher Surve of Reproductive Health Experiences 2021.
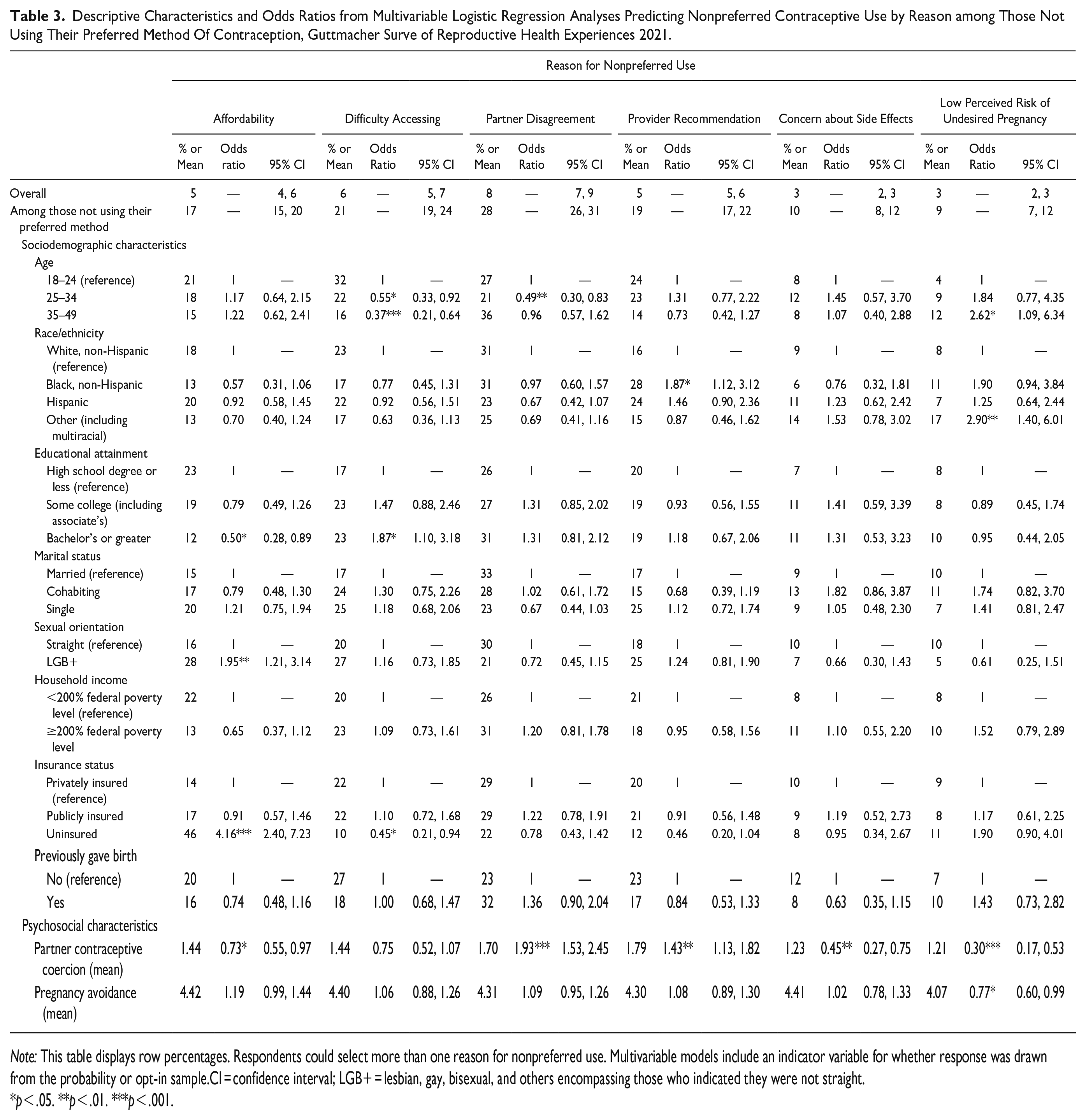
Note: This table displays row percentages. Respondents could select more than one reason for nonpreferred use. Multivariable models include an indicator variable for whether response was drawn from the probability or opt-in sample.CI = confidence interval; LGB+ = lesbian, gay, bisexual, and others encompassing those who indicated they were not straight.
p < .05. **p < .01. ***p < .001.
Focusing exclusively on those not currently using their preferred method, reasons for nonpreferred use varied by sociodemographic and psychosocial characteristics. Net of other characteristics, those with a bachelor’s degree were half as likely as those with a high school degree or less to report affordability as a reason for not using their preferred method. LGB+ respondents were nearly twice as likely as straight respondents and the uninsured were more than 4 times as likely as privately insured respondents to attribute their nonpreferred use to affordability. Affordability was inversely associated with partner contraceptive coercion. Younger respondents were more likely to report accessibility barriers than those over 25.
Attributing nonpreferred method use to partner disagreement was significantly more common among those ages 18 to 24 compared to those ages 25 to 34. Experiences of partner contraceptive coercion were strongly associated with partner disagreement and provider recommendation as reasons for nonpreferred use. We found no statistically significant differences in reporting partner disagreement by marital status, holding other covariates constant. Non-Hispanic Black women were significantly more likely to attribute their nonuse to a provider’s recommendation than non-Hispanic White women.
Reporting side effects as a concern was less common among those with higher levels of partner contraceptive coercion, as was reporting a low perceived risk of undesired pregnancy. Using a nonpreferred method due to low perceived risk of undesired pregnancy was significantly higher among the oldest respondents, those who were not exclusively White, Black, or Hispanic, and those with a lower pregnancy avoidance score.
Reasons for nonpreferred use also varied by respondents’ method preferences (Table 4). Half of those who wanted to use a vasectomy and more than one-third of those who wanted to use condoms reported they were not using these methods because their partner disagreed with using them. Affordability and accessibility were the most common barriers for those who wanted a tubal ligation, implant, or IUD, and more than one-fifth of those who wanted a tubal ligation, an IUD or implant, the pill, or condoms attributed their nonuse to provider recommendations.
Distribution of Reasons for Nonpreferred Method Use among those Not Using Preferred Method Overall and by Method Preference, Guttmacher Survey of Reproductive Health Experiences 2021.
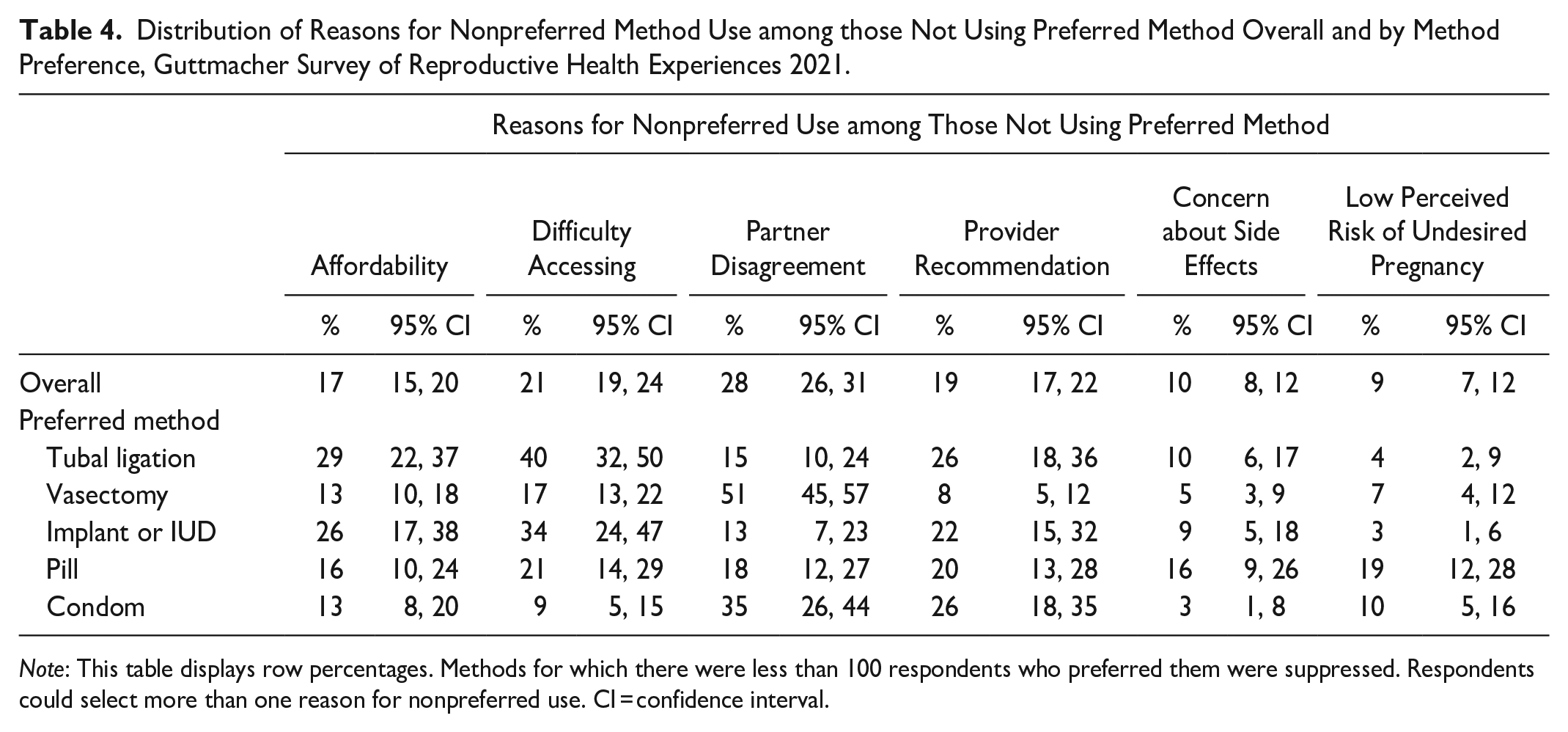
Note: This table displays row percentages. Methods for which there were less than 100 respondents who preferred them were suppressed. Respondents could select more than one reason for nonpreferred use. CI = confidence interval.
Discussion
Building on prior studies of preferred contraceptive use, results from this article highlight the mechanisms by which gender and power shape whether people use their preferred method of contraception, thus deepening our understanding of the social-ecological factors shaping reproductive autonomy. By using data from a national survey of people assigned female at birth and examining a two-item approach that first asked respondents to report on unsatisfied contraceptive preferences and then asked a broad follow-up question about the reasons for nonpreferred use, this study expands the scope of the growing body of literature on contraceptive preferences to consider variation in and correlates of the factors contributing to unsatisfied preferences.
Compared to prior research, we found a slightly higher prevalence of nonpreferred method use overall but similar associations between sociodemographic characteristics and unsatisfied preferences (Burke et al. 2020; Frederiksen et al. 2022; Gomez et al. 2024). However, our findings deviated from previous research concerning reasons for nonpreferred use. In the NSFG, 22 percent were not using their preferred method due specifically to cost (Burke et al. 2020). By contrast, we found that only 5 percent reported affordability as a reason for nonpreferred use when allowed to indicate a range of reasons for nonpreferred method use. Our findings mirror other recent work on reasons for nonpreferred use, which suggest that although cost is not to be ignored as a barrier, a broader array of factors shapes mismatches between contraceptive preferences and use (Frederiksen et al. 2022; Gomez et al. 2024). In the current study, we find that gendered power plays a significant and underexplored role through partner disagreement, elevating the importance of considering the full social-ecological context in which contraceptive behavior occurs (Holt et al. 2020). Provider recommendations and accessibility were also more common obstacles than cost in keeping people from using their desired method.
Our findings draw attention to the power dynamics that shape contraceptive use patterns as key social mechanisms generating preference-use mismatch, echoing scholarship on the role of gendered inequality in reproductive labor (Fennell 2011; Kimport 2018b; Littlejohn 2021). Among those not using their desired method, one-quarter wanted to use vasectomy, and nearly half preferred a male-based method of contraception, yet the most common reason respondents reported for not using their desired method was that their partner disagreed with using it. Furthermore, partner contraceptive coercion, as measured by a validated scale, was associated with not using a preferred method. Coercion appears to work directly through partner preferences, acting as a barrier to women fulfilling their contraceptive preferences, in addition to having an indirect pathway, given that greater exposure to contraceptive coercion was associated with provider-based barriers to the use of preferred contraceptive methods.
Among those not using their preferred method, roughly one in five pointed to the influence of providers on their unsatisfied contraceptive preferences. We found that Black women, a population that has been subject to heightened coercion and control from the health care system (Roberts 1999), more frequently reported that they were not using their desired contraception because their provider recommended another method compared to White women. Although the phrasing of the survey item in the current study does not escalate reports of provider recommendations to the level of coercion, in the context of previous research on biased or coercive care, these findings raise concern (Gomez and Wapman 2017; Manzer and Bell 2022; Rowlands and Walker 2019; Swan et al. 2023).
Although gendered power surfaced as a key factor shaping preferred method use in this study, cost and accessibility remain obstacles, especially to some of the most effective methods. Overall, we found a strong preference for permanent contraceptive methods, with the share of respondents preferring tubal ligation or vasectomy greatly exceeding the share using these methods; among those not using their preferred method, 41 percent preferred a permanent method. Affordability, accessibility, partner disagreement, and provider disagreement were each prominent barriers to using permanent methods among those who preferred them. The high levels of unsatisfied preferences and various barriers to these methods suggest the importance of further research into those who want to but are not using a permanent method, who are likely at a distinct phase of their reproductive life course.
Importantly, this research also highlighted that some individuals prefer not to use a contraceptive method. Although 31 percent of those not currently contracepting would like to use a method, the remaining 69 percent of those not using a method reported that this behavior reflected their contraceptive preferences. This adds to the literature showing that people may choose not to contracept for a variety of reasons that are not rooted in the inability to access contraception (Frederiksen and Ahrens 2020; Littlejohn 2013, 2021; Sedgh and Hussain 2014; Senderowicz and Maloney 2022). If freely chosen, as opposed to a result of barriers to care, lack of information, or coercion, using no method is always a valid contraceptive choice.
Implications
Our findings suggest that meeting people’s contraceptive preferences requires attention to gendered systems of power across the multiple domains of the social-ecological framework that limit women’s reproductive autonomy (Holt et al. 2020). Hegemonic masculinity incorporated into and supported by social norms, interpersonal interactions, the provision of reproductive health care, and public policy reflects this overarching system of power and highlights how efforts to align contraceptive preferences with contraceptive use will necessarily be multifaceted.
Public health campaigns, education, and provider counseling could heighten men’s engagement in reproductive labor by normalizing condom and vasectomy use. Previous research has demonstrated that condom use resistance from a male partner is a common experience (Davis et al. 2019) and that men have normalized this behavior (Dalessandro et al. 2019; Davis et al. 2014). Furthermore, research on men’s contraceptive use has shown how both a lack of knowledge of the procedure (White et al. 2022) and perceptions of the procedure as emasculating can lend to vasectomy resistance (Nicholas et al. 2021; Shih et al. 2013). Increasing knowledge and shifting perceptions through clinical and public education that is attentive to gendered power dynamics could serve to disrupt these norms and undermine the long-standing, unequal gendered division of labor in pregnancy prevention (Kimport 2018b; Littlejohn 2021).
Furthermore, most men ages 15 to 44 are sexually active and seeking to prevent pregnancy, but fewer than one in five access family planning services annually, demonstrating an opportunity for clinical care outreach (Marcell et al. 2016). Opportunities also exist for incorporating men into women’s contraceptive counseling, to the extent that women consent; in a survey of Title X clients, nearly two-thirds of female clients reported that they would be interested in couple-based counseling on birth control or pregnancy planning (Zolna, Frost, and Lindberg 2011). Importantly, any focus on men’s involvement in women’s care needs to be tempered with a heightened awareness of the risk of contraceptive coercion and interference (Kavanaugh, Lindberg, and Frost 2012).
Health care providers have multiple mechanisms for helping to meet the contraceptive preferences of their patients, including counseling patients on partner-based methods of contraception and screening for contraceptive coercion by partners. Furthermore, it is incumbent on providers to increase their awareness of the power dynamics in clinical spaces that lend to their influence on individuals’ contraceptive choices and work to ensure that counseling is centered on patient preferences (Manzer and Bell 2022). Embracing the principles of person-centeredness in contraceptive care by prioritizing patients’ experiences of interpersonal connection, decision support, and receipt of adequate information from their provider (Dehlendorf et al. 2013) can explicitly align the provision of care with what patients want and minimize coercive practices that result in mismatches between contraceptive preferences and use (Senderowicz 2019; Swan et al. 2023).
At a more structural level, undermining patriarchal influences in reproductive health policy, such as amending the exemption of vasectomy from mandated insurance coverage of birth control under the Affordable Care Act, could operate on multiple levels to normalize the procedure, improve access, and increase use among those who desire it. Importantly, the current study focuses on the contraceptive desires of people assigned female at birth (i.e., those who would not be undergoing a vasectomy). To meet the desires of those interested in vasectomy inherently involves another person, entitled to autonomy of their own. The objective of improving access to and normalizing vasectomy is not the infringement of the autonomy of men but instead an avenue to undercut the systematic feminization of reproductive labor and achieve a more equitable starting point from which couples can develop contraceptive strategies that suit their preferences (Kimport 2018b).
Forward-looking efforts to develop new contraceptive technology should also center the desires of those who can become pregnant and consider women’s expressed interest in sharing the burden of pregnancy prevention. Gender inequality has undoubtedly shaped the history of the development and testing of the methods available on the market today (Kammen and Oudshoorn 2002); no reversible medical methods are available for males. Although introducing and promoting a male-based method will involve challenging gendered cultural beliefs about masculinity (Oudshoorn 2004), this challenge is worth facing to expand contraceptive options, promote gender equity, and increase reproductive autonomy.
Finally, on a methodological note, our overall estimate of the prevalence of unsatisfied preferences is more similar to the NSFG’s than our estimate of unsatisfied preferences due specifically to cost. Yet we find similar associations between demographic characteristics and having an unsatisfied preference regardless of reason as the NSFG shows when examining cost alone. We suspect the NSFG survey item is detecting a broader concept than just a desire for a(nother) method in the absence of cost. This variation in estimates with respect to cost underscores the importance of more rigorous evaluation and testing of contraceptive preference survey items, particularly while the literature is nascent. To date, there is substantial variation in how contraceptive preferences have been elicited in survey research (Burke and Potter 2023). Research and scientific dialogue focused on developing and solidifying the construct behind “contraceptive preferences” (as opposed to, for example, ideals) is essential to advancing this person-centered metric with the precision and care that research in the service of equity demands.
Limitations
Although this study offers valuable insights, it is subject to a number of limitations. First, in the questionnaire design, the option to express a preference for not using contraception was only offered to those who reported not currently using a method. Therefore, this survey design can give us insights into how many people who are not using a method do not want to use one, but it does not tell us how many people currently using a method do not want to use one. The decision not to allow those contracepting to express a preference for no method reflects some “upward coercion” incorporated into the questionnaire design (Senderowicz 2019), which future research should address by allowing all respondents the option to prefer no method.
Although the questions in this survey were posed in a way that allowed respondents to select multiple options, we chose to simplify our analyses by focusing on a comparison of the most effective method used and preferred to identify nonpreferred use. This conceptualization of nonpreferred method use privileges efficacy despite prior research showing that people develop personal hierarchies of method preferences based on attributes that may include but are not limited to how well a method prevents pregnancy (Higgins and Smith 2016; Jackson et al. 2016; Littlejohn 2021; Marshall et al. 2016). However, the most effective methods are often those with the most significant structural barriers to obtaining them. Our findings were substantively similar in sensitivity analyses using other coding schemes, including whether respondents were using any of their preferred methods of contraception. A further limitation is that among those who selected multiple preferred methods, we cannot distinguish which reason for nonpreferred use aligns with each preferred method. We encourage future scholarship that continues to fine-tune the operationalization of unsatisfied contraceptive preferences to appropriately balance analytic parsimony with accuracy in representing people’s lived experiences. We note that Gomez et al. (2024) have recently made strides in this area using survey items developed with focus groups and cognitive interviews that directly measure people’s ranking of their preferred methods if they select more than one.
We also note that our reliance, in part, on a nonprobability sample may introduce selection bias that was not addressed by the sampling weights. However, sensitivity analyses excluding the opt-in sample yielded substantively similar results. Compared to other nationally representative samples considering preferred contraceptive use, our sample is older and more educated (Burke et al. 2020; Gomez et al. 2024). This may be due to differences in inclusion criteria compared to other studies: Our data did not include teens, which inherently skewed the age distribution older, and also focused on those who had PVI in the last 30 days, which is associated with age and social advantage (Ueda et al. 2020). These sample differences may underlie some of the high levels of interest in permanent methods.
Finally, our focus on people assigned female at birth poses a limitation, particularly because we highlight substantial interest in male-based methods among this population and seek to challenge the unequal gendered division of reproductive labor. Incorporating males into future research about contraceptive preferences is imperative to explicitly identify gender differences in preferences, the likelihood of using a preferred method, and reasons for nonpreferred use. This research could more comprehensively identify opportunities to improve gender equity in pregnancy prevention.
Conclusion
Evidence from this study of the contraceptive preferences and barriers to preferred method use among a national sample of people assigned female at birth reveals mechanisms through which gender and power play critical roles in shaping reproductive autonomy. These findings expand on previous research that has focused mainly on economic barriers to preferred method use, highlighting the need for a comprehensive assessment of barriers that considers individuals’ full social-ecological context. Beyond expanding the accessibility and affordability of contraception, addressing gender biases in culture, policy, and health care provision is necessary to align contraceptive use with preferences and make the burden of pregnancy prevention more equitable.
Footnotes
Appendix
Distribution of Current Contraceptive Use and Preferences Allowing for Multiple Selections, Guttmacher Survey of Reproductive Health Experiences 2021.
| Current Method % | Preferred Method % | |
|---|---|---|
| Tubal ligation | 13 | 16 |
| Vasectomy | 11 | 17 |
| Implant or IUD | 17 | 17 |
| Pill | 22 | 20 |
| Shot, patch, ring | 8 | 8 |
| Condom | 25 | 15 |
| Withdrawal | 27 | 12 |
| Fertility awareness | 5 | 4 |
| Other | 1 | 3 |
| None | 13 | 8 |
Note: Columns do not add to 100 percent because respondents could select more than one response.
Acknowledgements
The authors thank Alicia VandeVusse for her thoughtful feedback on an earlier draft.
Funding
Kristen Burke received support from the National Science Foundation Graduate Research Fellowship Program (DGE-1610403), the University of Texas Graduate School, and a center grant awarded to the Population Research Center at the University of Texas at Austin by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (P2CHD042849). The Guttmacher Survey of Reproductive Health Experiences was designed by Laura Lindberg, Rachel Jones, Jennifer Mueller, and Madeleine Hass. Data were collected as part of research studies supported by the Eunice Kennedy Shriver National Institute of Child Health & Human Development of the National Institutes of Health under Awards R01HD084473 and R01HD092396. The content is solely the responsibility of the authors and does not necessarily represent the views of the funders.
Data and Code
Data for this analysis are publicly available at: osf.io/mbu6s. Stata code to reproduce these results are available at ![]()