
Abstract
Emotional support is essential to health outcomes, especially for marginalized communities. The coronavirus disease 2019 pandemic increased the prevalence of mental health issues and thus increased the need for emotional support, particularly for sexual minoritized people. The authors applied minority stress theory and the stress process framework by drawing on a population-based data source of 3,642 respondents, the National Couples’ Health and Time Study, which oversampled sexual minoritized people during the pandemic. The authors examine three sources of emotional support (friends, family, and partners) and their association with three mental health outcomes (depression, anxiety, and loneliness) separately for cisgender men and cisgender women. The authors find that emotional support plays a larger role in the association between sexual identity and mental health for cisgender men than cisgender women. Regardless of gender, bisexual individuals have consistently higher levels of depression, anxiety, and loneliness across all models, and this difference is not attenuated by emotional support.
Emotional support is essential to mental health outcomes especially for members of the lesbian, gay, bisexual, transgender, and/or queer (LGBTQ+) community (Doty et al. 2010). Prior to the pandemic, sexual minoritized persons more often experienced mental health issues than people who identified as heterosexual (Almeida et al. 2009; Borgogna et al. 2019; Plöderl and Tremblay 2015; Ross et al. 2018; Stacey, Reczek, and Spiker 2022). During the coronavirus disease 2019 (COVID-19) pandemic, stress levels (Park et al. 2020; Prowse et al. 2021; Taylor et al. 2020a, 2020b) and the prevalence of mental health issues (Ettman et al. 2020; Hawes et al. 2021) for general population samples substantially increased. Moreover, individuals with LGBTQ+ identities experienced more COVID-19-related stress than heterosexual individuals (Goldbach, Knutson, and Cole Milton 2021; Manning and Kamp Dush 2021; Moore et al. 2021; Salerno et al. 2023). A key strategy to manage stress is via emotional support. For the LGBTQ+ population, it is important to account for sources of emotional support because individuals with sexual minoritized identities report higher levels of emotional support from friends and lower levels of family support (Gustafson et al. 2023; Hsieh and Wong 2020). We examine whether emotional support was especially important for individuals that do not identify as heterosexual during the pandemic, and we examine support from family, friends, and partners.
Women also suffered more mental health issues during the pandemic than men (Almeida et al. 2020; Thibaut and van Wijngaarden-Cremers 2020), similar to prepandemic, when women reported higher levels of depression and anxiety (Afifi 2007; Nolen-Hoeksema 2001; Riecher-Rössler 2017). At the same time, women receive more social support than men (Antonucci and Akiyama 1987; Rueger, Malecki, and Demaray 2008, 2010) and that additional support may be critical during stressful events. Given gender disparities in well-being, studies of well-being during the pandemic require attention to gender-specific analyses of sexual identity.
We apply a minority stress framework to examine the well-being of men and women by their sexual identity. We draw on one of the only population-based data collections initiated during the pandemic, the National Couples’ Health and Time Study (NCHAT) with oversamples of individuals with sexual minoritized identities. These data offer a unique opportunity to explore emotional support of sexual minoritized people at a time when one’s mental and physical health was particularly crucial to their overall well-being. We test separate models for cisgender women and men because of the well-documented gender disparities in levels of mental health well-being and social support (Barnett et al. 2021; McLean et al. 2022). We focus on three sources of emotional support (family, friend, and partner) and we hypothesize that these sources of support may be particularly important for sexual minoritized people as they navigate elevated discrimination and stress in their lives. These findings will provide new insights into the links between emotional support and well-being for a marginalized but growing population during the recent public health crisis.
Background
The stress process model (Pearlin 1999; Pearlin et al. 1981) suggests that there is a process by which people respond to difficult life circumstances such as chronic strains or adverse experiences. Wheaton et al. (2013) defined stress as “a discrete and observable event representing change and thus requiring some social and/or psychological adjustment on the part of the individual” (p. 303). Stress can manifest in terms of mental, emotional, or physical toll, and it causes change and requires adaptation (Meyer 1995, 2003). The stress process model proposes that there are three components of stress, including stressors, buffers, and outcomes. Stressors can affect individuals, leading to a variety of outcomes, while buffers serve to mitigate these effects. Stress has been linked to both mental health outcomes such as depression, anxiety, and suicidality (Meyer 1995, 2003; Mongelli et al. 2019; Wight et al. 2012) and physical health outcomes such as cancer, flu, hypertension, and physical health items from the SF-36 subscale of the RAND Health Survey, including dizziness, aches and pains, headaches, nausea, and others (Frost, Lehavot, and Meyer 2015; Raposa et al. 2014).
The stress process model suggests that at least some of the variation in mental health outcomes can be attributed to differences in individual coping resources (Pearlin 1999). Emotional support is a key coping resource that buffers the effects of stressors on adverse mental health outcomes (Kornblith et al. 2001; Szkody et al. 2021), especially for sexual minoritized people (Clarke 2012; Dakin, Williams, and MacNamara 2020). Emotional support consists of love, caring, trust, listening, discussing personal issues and worries, and other affective behaviors (Frost, Meyer, and Schwartz 2016; House 1987). In this article, we argue that the incorporation of emotional support from partners, friends, and family members will partially mitigate the disparities in mental health issues between sexual minoritized and heterosexual people.
For sexual minoritized people, their stigmatized identity can be a major source of stress (Cyrus 2017; Kelleher 2009), with their unique experiences with stigma and aggressions acting as stressors (Balsam et al. 2011; Munro, Travers, and Woodford 2019). The minority stress theory (MST), as developed by Brooks (1981) and Meyer (1995, 2003) is the most prominent approach used to assess the well-being of sexual minoritized individuals. MST posits that stigma-related stress associated with sexual minoritized status drives increased risk for poor mental and physical health outcomes among LGBT individuals. MST operates under the assumptions that minority stress is (1) unique, (2) chronic, and (3) socially based (Meyer 1995, 2003). Meyer (2003:676) argued that stressors faced by minoritized people are additive to stressors faced by all people, are related to underlying social and cultural structures, and stem from social processes, institutions, and structures. There are four principal components of minority stress: (1) general external pressures (i.e., “don’t say gay” bills and policies) and specific instances of stress (i.e., violence), (2) expected stigma, (3) concealment of one’s sexual orientation or identity, and (4) internalized homophobia (Peleg and Hartman 2019). Each of these components contribute to poorer mental health outcomes among people who identify as sexual minorities (Hoy-Ellis 2023; Ramirez and Paz Galupo 2019). In this study, we examine the role of emotional support in mitigating the harmful effects of minority stress and how emotional support may operate differently according to gender.
Emotional Support
A large body of research has demonstrated the importance of social support for sustaining mental and physical health in marginalized communities (Donev 2005; Heaney and Israel 2008). Social support is a valuable resource and serves to help ameliorate the negative impacts of stress (Kamp Dush et al. 2022). For both men and women, higher social support is associated with better self-rated health and higher life satisfaction (Matud, García, and Fortes 2019). We focus on emotional support, though prior research may refer to such as social support. When discussing the research of others, we will use the authors’ own terminology.
However, there are gender differences in the need for and receipt of emotional support. Women report higher stress levels and slightly more negative life events but also have a larger support network, receive more social support, are more socially connected, and enjoy higher quality social support than men (Dalgard et al. 2006; Henning-Smith et al. 2018; Kneavel 2021). Men have been shown to have consistently smaller support networks, regardless of partnership status (Dykstra and Fokkema 2007) and are less likely to say that they can open up to family or friends (Henning-Smith et al. 2018), which may exacerbate the importance of social support for men. Stronge, Overall, and Sibley (2019) noted a stronger association between men’s relationship status and well-being (self-esteem and life satisfaction), partially due to men’s stronger connection between relationship status and perceived social support. That is, relationship status is a key predictor of men’s perceived social support. Among gender minoritized people, including transgender individuals, high levels of support from family and friends was associated with strikingly lower levels of depression and anxiety (Puckett et al. 2019).
Support from family members has an important and positive influence on mental health (Bouris et al. 2010; Newcomb, Heinz, and Mustanski 2012; Padilla, Crisp, and Rew 2010; Roberts and Christens 2021). Sexual minoritized individuals have more strained family relationships and lower levels of support from parents and family members (Gustafson et al. 2023; McConnell, Birkett, and Mustanski 2016; Needham and Austin 2010; Watson et al. 2019). Thus, other sources of emotional support may be key for LGBTQ+ persons.
Friend support is a central resource and associated with lower levels of mental health problems (Bruce, Harper, and Bauermeister 2015; Gillespie et al. 2015; Tebbe and Moradi 2016). Given the lower levels of family support given to individuals with sexual minoritized identities, friend support may be especially salient. Although friend support was positively associated with life satisfaction for all sexual orientations, the strongest associations were among lesbian women, bisexual men, and bisexual women (Gillespie et al. 2015). This may be due to the tendency for sexual minoritized individuals to be more reliant on their “chosen families” (defined as their non-blood-related friends who come to fill the roles normally filled by family members) as their primary source of social support (Blair and Pukall 2015, 267). Although chosen families come in different forms within different subgroups of society, the rejection by or the lack of support from family members plays a crucial role in the formation of chosen families for LGBs (Dewaele et al. 2011).
A proximal source of support, partner or spouse support, contributes to better mental health (Choi and Ha 2011; Davey-Rothwell 2017; Stapleton et al. 2012) across sexual identities (Kamp Dush et al. 2022). Among older LGBT adults, caregivers assisting friends had lower levels of social support than those assisting partners and thus resulted in higher levels of depressive symptomology for caregivers (Shiu, Muraco, and Fredriksen-Goldsen 2016). Partner support is also linked to relationship satisfaction (Cramer 2004; Lal and Bartle-Haring 2011), which can contribute to lower levels of depression (Leach and Butterworth 2020; Misri et al. 2000), anxiety (Borstelmann et al. 2020; Leach and Butterworth 2020) and loneliness (Eshbaugh 2010; Lee and Goldstein 2016).
Mental Health
Mental health is crucial to one’s overall well-being. As with emotional support, there are significant gender differences in mental health. Women have much higher rates of major depressive disorder and anxiety disorder (Alexander 2007; Zender and Olshansky 2009). The prevalence of mental health disorders differs across sexual and gender identities, as the patterns of risk are different for men and women and for specific sexual minoritized groups (Bostwick et al. 2010). Although there is research linking sexual and gender minoritized identities and racial/ethnic minoritized identities to greater psychological distress and mental health outcomes (Sutter and Perrin 2016; Williams et al. 2007), we focus this work on the intersection of gender and sexual identity.
Women have higher levels of depressive symptoms than men (Botticello 2009; Brown 2000; Kamp Dush et al. 2022; Mirowsky and Ross 1995), and it is well established that sexual minoritized people have greater risk for depression than their heterosexual counterparts (Borgogna et al. 2019; Hatzenbuehler, McLaughlin, and Xuan 2012; Lucassen et al. 2017; Marshal et al. 2011; Safren and Heimberg 1999). Traditionally sexual minoritized individuals are grouped together, but there are distinct differences between individuals with different sexual minoritized identities, particularly among bisexual individuals. Individuals identifying as bisexual most frequently have mental health problems, including depression, anxiety, self-harm, and suicidality compared with gay, lesbian, and heterosexual individuals (Jorm et al. 2002). Among young adults, Li, Pollitt, and Russell (2016) noted individuals identifying as bisexual and “mostly heterosexual” had significantly higher concurrent depression than heterosexual individuals. In Sweden, all sexual minoritized groups had increased risk for depression compared with heterosexual individuals, with bisexual individuals and gay men having the highest likelihood of depression (Björkenstam et al. 2017). Bisexual women are less likely to receive positive responses to their sexual identity, and bisexual men experience more psychological distress than gay men (King et al. 2003). In a meta-analysis by Ross et al. (2018), heterosexual individuals had the lowest rates of depression and anxiety, and bisexual individuals had higher or equivalent rates compared with gay or lesbian individuals. Furthermore, individuals in the emerging sexual and gender minoritized categories (pansexual, demisexual, asexual, queer, questioning, and transgender or gender nonconforming) report significantly higher rates of depression and anxiety compared with cisgender, heterosexual individuals, as well as gay and lesbian individuals (Borgogna et al. 2019).
There are also sexual and gender identity differences in anxiety (Kamp Dush et al. 2022). Sexual minoritized individuals have higher anxiety (Borgogna et al. 2019; Pakula et al. 2016; Ross et al. 2018) than their heterosexual counterparts. For both men and women, bisexual identity and behavior were strongly and persistently associated with heightened risk for mood and anxiety disorders (Bostwick et al. 2010). Bisexual individuals are more likely to report anxiety disorders, mood disorders, and anxiety-mood disorders (Pakula et al. 2016). Women have higher prevalence and severity of social anxiety disorder than men (Asher and Aderka 2018) and have a higher likelihood of affective and anxiety disorders when holding other characteristics and stress exposure constant (Aneshensel, Rutter, and Lachenbruch 1991). Among adolescents, girls had significantly higher prevalence in all mood and anxiety disorders than boys (Kessler et al. 2012).
Loneliness has been identified as a key indicator of health with researchers demonstrating the detrimental effects of social isolation (Umberson, Lin, and Cha 2022). Loneliness varies by sexual and gender identity (Kamp Dush et al. 2022), and those with a sexual minoritized identity have higher levels of loneliness than their heterosexual counterparts. However, there are mixed results when it comes to gender and loneliness. Some studies show that men report more loneliness than women across cultures (in a study spanning 237 countries, islands, and territories) and age (Barreto et al. 2021) and have higher levels of social and emotional loneliness regardless of partnership status (Dykstra and Fokkema 2007). However, a study conducted during the COVID-19 pandemic revealed women to have greater odds of loneliness than men among all age groups (Wickens et al. 2021). Rokach (2018) suggested that women may express, but not necessarily experience, more loneliness than men.
The Present Study
The objective of this study is to apply the stress process framework (Pearlin 1999) and MST (Brooks 1981; Meyer 1995, 2003) to assess the associations between emotional support from family, partners, and friends and three mental health indicators (loneliness, depression, and anxiety) by sexual identity separately for cisgender men and women. In both theories, emotional support is a crucial element driving the mental and physical well-being of sexual minoritized people. We expect that the negative mental health outcomes experienced by diverse sexual identities will be partially mediated with the inclusion of emotional support for partnered cisgender men and women.
A contribution of this study is the ability to include an indicator of minority stress, aggressions, in the model. The models will include indicators that are related to levels of mental health outcomes in prior studies, specifically those focusing on sexual and gender diverse populations (Kamp Dush et al. 2022). The traditional sociodemographic indicators include gender identity (Kendler, Myers, and Prescott 2005), racial/ethnic identity (Wong Santos, and Tobin 2022), age (Bruine De Bruin, Parker, and Strough 2020), education (DeBerard, Spielmans, and Julka 2004), marital status (Marcussen 2005), and parenthood status (Samandari, Speizer, and O’Connell 2010). Furthermore, to contextualize this work in the pandemic, this study includes an indicator of COVID-19 stress to capture the unique experience of the pandemic and potentially a measure of demand for emotional support as well as month of survey to account for variability in experiences during different periods of the pandemic.
Data and Methods
NCHAT is a nationally representative sample of 20- to 60-year-old partnered individuals who are married or cohabiting in the United States. Data were collected using an online survey from September 2020 to April 2021. These data are especially suited for this project because of the breadth of questions, timing of the data collection, and the large, population-based sample of sexual and gender minoritized respondents. To date no data collections, other than NCHAT, were conducted during the pandemic and have large oversamples of sexual minoritized people to address these research questions and are nationally representative. Furthermore, the NCHAT data provide a new opportunity to examine emotional support differences among sexual minoritized people as well as a unique time-specific item, COVID-19 stress. Understanding the correlates of emotional support among sexual minoritized individuals is important for future research on the role of emotional support and well-being amid a global pandemic or a major event such as a climate change shock. The NCHAT data are publicly available for download from the Inter-University Consortium for Political and Social Research at https://www.icpsr.umich.edu/web/DSDR/studies/38417.
The initial sample included 3,642 respondents with valid responses to age and gender. The sample was limited to those who provided responses to the dependent variables (depressive symptoms, anxiety, and loneliness; n = 3,640) and then restricted to those who responded to the support indicators (partner support, family support, friend support; n = 3,630). The sample was further limited to respondents with valid responses to the independent variables, education (n = 3,625), and parenthood status (n = 3,618). The final analytical sample size was 3,618. When running the models separately by gender, the samples were 1,723 cisgender women and 1,768 cisgender men. Given that there were only 127 noncisgender individuals, we did not run a third set of models for gender minoritized respondents. However, supplemental models described below show the association between noncisgender identities and mental health.
Measures
Depression
Depression was measured by asking respondents, “Below is a list of ways you might have felt or behaved. How often have you felt this way in the past 7 days?” Responses ranged from 1 = “rarely or none of the time (less than 1 day)” to 4 = “most or all of the time (5–7 days).” We calculated the average score for respondents’ answers to the following 10 statements: “I was bothered by things that don’t usually bother me”, “I had trouble keeping my mind on what I was doing”, “I felt lonely”, “My sleep was restless”, “I felt depressed”, “I felt like everything I did was an effort”, “I felt hopeful for the future”, “I felt fearful”, “I was happy”, and “I could not get going” (α = .87). The items “I felt hopeful for the future” and “I was happy” were reverse-coded in the analyses.
Anxiety
Anxiety was measured by asking the question “In the past 7 days, how often have you been bothered by the following problems?” and obtaining the average score for respondents’ answers to the following seven options: “Feeling nervous, anxious, or on edge”; “Not being able to stop or control your worrying”; “Worrying too much about different things”; “Trouble relaxing”; “Being so restless that it is hard to sit still”; “Becoming easily annoyed or irritable”; and “Feeling afraid as if something awful might happen.” Responses ranged from 1 = “not at all” to 4 = “nearly every day” (α = .92).
Loneliness
Loneliness was measured on the basis of the short version of the UCLA Loneliness Scale (Hughes et al. 2004). Respondents were asked, “In the past 7 days, how often have you been bothered by the following problems?” We obtained the average score for the respondents’ answers to the following items: “How often did you feel that you lacked companionship?” “How often did you feel left out?” and “How often did you feel isolated from others?” Responses ranged from 1 = “never” to 5 = “very often.”
Sexual Identity
The question used to identify sexual identity was “What do you consider yourself to be? Select all that apply,” with 11 responses: “heterosexual or straight,” “gay or lesbian,” “bisexual,” “same-gender loving,” “queer,” “pansexual,” “omnisexual,” “asexual,” “don’t know,” “questioning,” and “something else,” with an option to specify. We coded respondents into four mutually exclusive categories: “exclusively heterosexual,” “exclusively gay/lesbian,” “bisexual plus pansexual, omnisexual, and queer,” and “another/multiple sexual identities.” Those in the “bisexual plus pansexual, omnisexual, and queer” category are those who selected only bisexual as a sexual identity as well as those who chose both bisexual and any combination of the latter three identities. Those selecting exclusively pansexual, omnisexual, and/or queer were categorized in the “another/multiple” category.
Gender Identity
Gender identity was measured by responses to the question “Which of the following best describes your gender?” Responses were “man,” “woman,” “trans man,” “trans woman,” and “do not identify as any of the above.” We coded gender into three mutually exclusive categories: “cisgender man,” “cisgender woman,” and “transgender or another gender identity.”
Emotional Support
Emotional support was measured with three questions (Procidano and Heller 1983): “How much do you rely on each of the following people for emotional support . . . I rely on my spouse/partner for emotional support, I rely on my family for emotional support, I rely on my friends for emotional support.” Responses ranged from 1 = “not at all” to 5 = “a great deal.”
Aggressions
Aggressions were measured by scaling respondents’ answers to the following nine statements: “You were treated with less respect than other people”; “You received poorer service than other people at restaurants or stores”; “People acted as if they were afraid of you”; “People acted as if they thought you were dishonest”; “People acted as if they were better than you”; “You were called names or insulted”; “You were threatened or harassed”; “You were hit, beaten, physically attacked, or assaulted”; and “You were robbed, or your property was stolen, vandalized, or purposely damaged.” Respondents were asked, “In your day-to-day life over the past months how often did any of the following things happen to you?” Responses ranged from 1 = “never” to 5 = “very often” (α = .86). These measures were modeled after measures used by Williams et al. (1997) and the Generations Study Baseline Questionnaire and Measure Sources (Meyer et al. 2016).
COVID-19 Stress
COVID-19 stress was measured by scaling respondents’ answers to the question “How stressed are you about the following?” and scaling their responses to the items “Getting coronavirus”; “My spouse or partner getting coronavirus”; “My parents, siblings, or other family members getting coronavirus”; and “Giving someone the coronavirus” (α = .87). Responses ranged from 1 = “not at all stressed” to 5 = “very stressed.”
Covariates
The models included indicators measuring race/ethnicity (non-Hispanic White, non-Hispanic Black, non-Hispanic Asian, Hispanic/Latinx, non-Hispanic multirace, and another), age as a continuous variable, education level (high school or less, some college, college degree), marital status (married, cohabiting), and parenthood status (have children, don’t have children).
Analytic Strategy
We estimated a series of ordinary least squares models to regress emotional support from partners, friends, and family onto mental health indicators for sexual minoritized and heterosexual people. We ran initial models to test significant gender differences in mental health outcomes net of support indicators and sociodemographic covariates (tables not shown). We then estimated models separately by gender because of established differentials in mental health and emotional support, using each mental health indicator as a separate dependent variable (depressive symptoms, anxiety, and loneliness) and sexual identity and emotional support as key independent variables. A baseline model included sexual identity and month of interview, a second model included the indicators of emotional support, and the third model included the sociodemographic covariates. We conducted formal mediation analyses using a sequential mediation model (Baron and Kenny 1986; Hayes and Preacher 2014). To test significance of the indirect effects, 95 percent bias-corrected bootstrapped confidence intervals were generated using 2,000 samples, and results indicating significance are presented in the text. The analyses were weighted in accordance with weights established by Gallup. Further details about the study and weighting can be found in Kamp Dush et al. (2023).
Results
Overall, mean levels of depression, anxiety, and loneliness were higher for partnered cisgender women than partnered cisgender men, as shown in Table 1. Initial multivariable models were estimated that did not separate respondents on the basis of gender identity (results not shown). Partnered cisgender women and respondents identifying as transgender or another gender identity had significantly higher levels of depression, anxiety, and loneliness than partnered cisgender men (results not shown). Furthermore, partnered cisgender women had significantly higher levels of depression and anxiety than transgender and those reporting another gender identity, but not loneliness (results not shown). The small sample size of noncisgender respondents prevented separate analyses. Given these findings and prior work on mental health and gender, subsequent analyses were run separately for cisgender women and men.
Descriptive Table of the Full, Cisgender Men, and Cisgender Women Samples.

Source: National Couples’ Health and Time Study.
Note: COVID-19 = coronavirus disease 2019; NH = non-Hispanic.
Cisgender Men
Table 1 includes the distribution of the sample separately for partnered cisgender men and women. There were 1,768 cisgender men in the sample. The weighted mean levels for the dependent variables were as follows: depression, 1.68 (range = 1–4); anxiety, 1.51 (range = 1–4), and loneliness, 1.87 (range = 1–5). Of the cisgender men, 97.82 percent (n = 1,039) identified as exclusively heterosexual, 1.23 percent (n = 487) as exclusively gay, 0.33 percent (n = 117) as bisexual (plus pansexual, omnisexual, and queer), and 0.61 percent (n = 125) with another or multiple sexual identities. The weighted mean levels for the support variables were as follows: family support, 3.17 (range = 1–5); friend support, 2.71 (range = 1–5); and partner support, 4.01 (range = 1–5). Regarding race, 55.02 percent (n = 1,005) of the cisgender men in this sample identified as non-Hispanic White, 6.99 percent (n = 149) as non-Hispanic Black, 7.92 percent (n = 126) as non-Hispanic Asian, 19.97 percent (n = 278) as Hispanic, 3.68 percent (n = 98) as non-Hispanic multiracial, and 6.41 percent (n = 112) as another racial/ethnic identity. The mean age of cisgender men was 43.59 years. Just under half (41.98 percent [n = 1,044]) of the cisgender men in this sample had a college degree or higher, with 31.38 percent (n = 340) reporting less than or equal to a high school degree and 26.64 percent (n = 384) reporting some college education. The majority (80.68 percent [n = 487]) of cisgender men in this sample were married, the remaining 19.31 percent (n = 1,281) were cohabiting. Fewer than one third (30.14 percent [n = 446]) of the cisgender men in the sample had children, and the remaining 69.86 percent (n = 1,322) did not. Last, the weighted mean levels for the other covariates for cisgender men were as follows: aggressions, 13.36 (range = 0–41) and COVID-19 stress, 9.72 (range = 3–20).
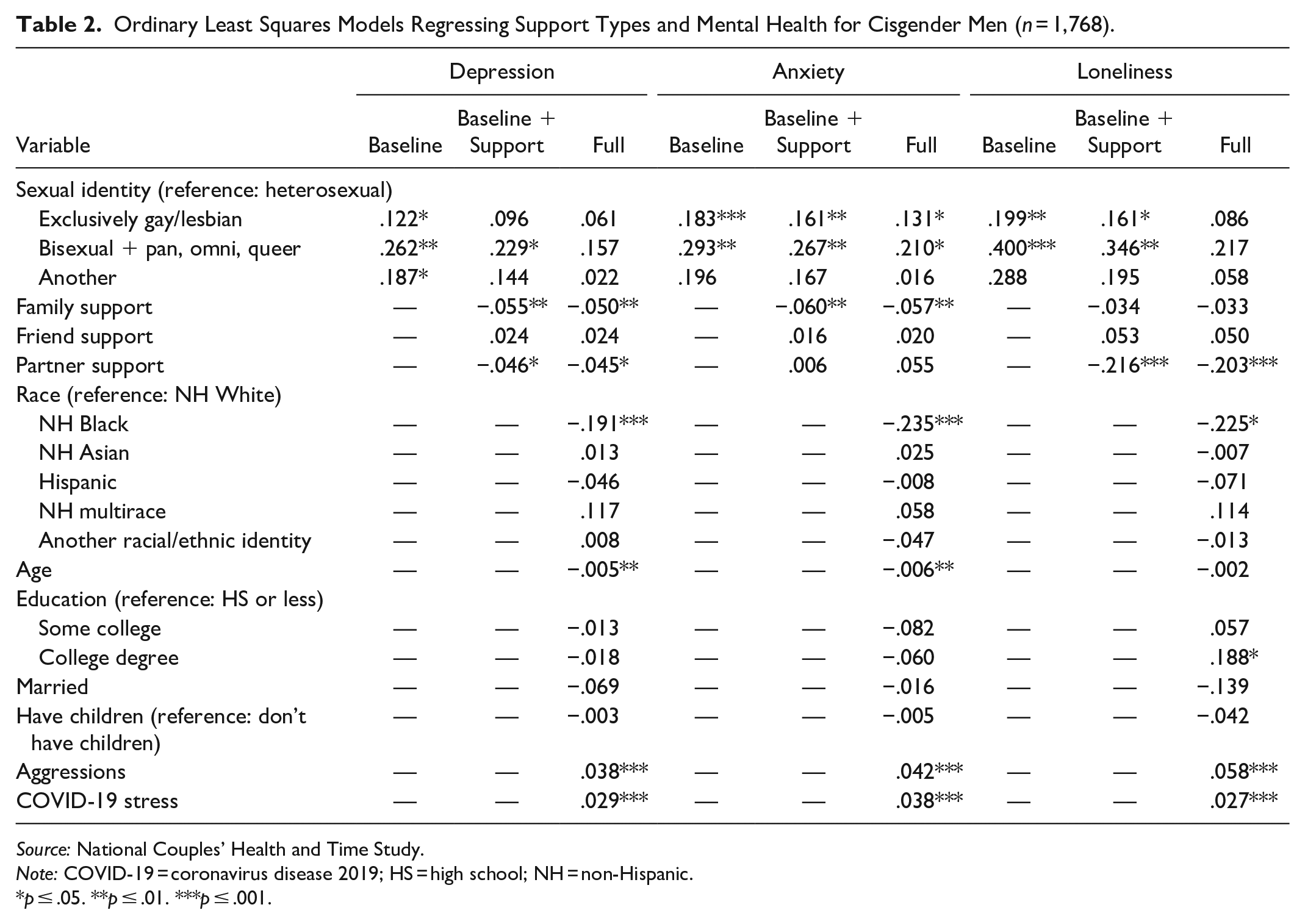
Table 2 includes the multivariable regression results for partnered cisgender men. The first three columns focus on depressive symptoms, the next three anxiety and the final set loneliness. The first model shows that gay and bisexual cisgender men had significantly elevated levels of all three mental health outcomes (depression, anxiety, and loneliness) than exclusively heterosexual cisgender men. Cisgender men reporting another or multiple sexual identities also had significantly higher levels of depression than cisgender heterosexual men.
Ordinary Least Squares Models Regressing Support Types and Mental Health for Cisgender Men (n = 1,768).
Source: National Couples’ Health and Time Study.
Note: COVID-19 = coronavirus disease 2019; HS = high school; NH = non-Hispanic.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
The second model, which added the measures of emotional support, shows that only bisexual cisgender men had significantly higher levels of depression, while gay and bisexual men had significantly higher levels of anxiety and loneliness compared with cisgender heterosexual men. Family support was directly associated with lower levels of depression, anxiety and loneliness. Partner support was only associated with lower levels of loneliness and friend support was tied to lower levels of anxiety. Mediation analyses indicated that sexual minoritized identities (relative to heterosexual men) were indirectly associated with depression and anxiety through family support (gay men depression 95 percent confidence interval [CI] = 0.013 to 0.042 and anxiety 95 percent CI = 0.014 to 0.051; bisexual men depression 95 percent CI = 0.012 to 0.046 and anxiety 95 percent CI = 0.013 to 0.053; another/multiple sexual identities depression 95 percent CI = 0.014 to 0.051 and anxiety 95 percent CI = 0.015 to 0.059). Depression and loneliness for partnered gay men were indirectly influenced through partner support (depression 95 percent CI = −0.017 to −0.001; loneliness 95 percent CI = −0.065 to −0.004). Additionally, the association of men with another/multiple identities and anxiety operated indirectly through friend support (95 percent CI = 0.000 to 0.036). Thus, emotional support was a key indirect pathway to mental health for each group of sexually minoritized men.
In the full model including all the covariates, no sexual identity was significantly different from heterosexual cisgender men in levels of depression and loneliness. Gay and bisexual cisgender men had significantly higher levels of anxiety than cisgender heterosexual men in the full model. For cisgender men, family and partner support were significantly associated with all three mental health outcomes, but not friend support. Similar to the prior models for partnered cisgender men of all sexual minoritized identities, family support was indirectly associated with depression and anxiety (gay men depression 95 percent CI = 0.015–0.042 and anxiety 95 percent CI = 0.016–0.050; bisexual men depression 95 percent CI = 0.012–0.043 and anxiety 95 percent CI = 0.012–0.048; another/multiple sexual identities depression 95 percent CI = 0.015–0.050 and anxiety 95 percent CI = 0.017–0.058) with all covariates in the models. Partner and friend support were no longer significant mediators in the full model.
In the full model, there were other covariates associated with the mental health outcomes. Regarding the sociodemographic indicators, non-Hispanic Black cisgender men had lower levels of depression, anxiety, and loneliness when accounting for emotional support indicators. Age was negatively associated with depression and anxiety but was not statistically significantly associated with loneliness. Of particular relevance to sexual minority men, experience of aggressions and COVID-19 stress were significantly positively associated with all three mental health indicators. Given the time frame of the study in supplemental models we found that COVID-19 stress operated similarly for all except cisgender bisexual men. The association between COVID-19 stress and depression was significantly stronger for cisgender bisexual men than cisgender heterosexual men.
Cisgender Women
The next set of results are limited to partnered cisgender women, and there were 1,723 in the sample. The weighted mean levels for the dependent variables were as follows: depression, 1.83 (range = 1–4); anxiety, 1.75 (range = 1–4); and loneliness, 2.11 (range = 1–5). Of the cisgender women, when weighted, 95.88 percent (n = 962) identified as exclusively heterosexual, 0.79 percent (n = 234) as exclusively gay or lesbian, 1.81 percent (n = 315) as bisexual (plus pansexual, omnisexual, and queer), and 1.52 percent (n = 212) with another or multiple sexual identities. The weighted mean levels for the support variables were as follows: family support, 3.52 (range = 1–5); friend support, 3.25 (range = 1–5); and partner support, 4.14 (range = 1–5). Regarding race, 56.86 percent (n = 1,037) of the cisgender women in this sample identified as non-Hispanic White, 7.67 percent (n = 153) as non-Hispanic Black, 5.40 percent (n = 73) as non-Hispanic Asian, 23.61 percent (n = 287) as Hispanic, 3.12 percent (n = 93) as non-Hispanic multiracial, and 3.34 percent (n = 80) as another racial/ethnic identity. The mean age of cisgender women was 42.71 years. More than half (51.16 percent [n = 1,153]) of cisgender women in this sample had a college degree or higher, with 31.13 percent (n = 287) having less than or equal to a high school degree and 17.71 percent (n = 283) having some college education. The majority (80.92 percent [n = 1,037]) of cisgender women in this sample were married, the remaining 19.08 percent (n = 416) were cohabiting. Fewer than one third (31.47 percent [n = 479]) of the cisgender women in the sample had children, and the remaining 68.53 percent (n = 1,244) did not. Last, the weighted mean levels for the other covariates for cisgender women were as follows: aggressions, 12.93 (range = 0–41) and COVID-19 stress, 11.27 (range = 3–20).
Table 3 presents the multivariable regression results for partnered cisgender women. Among cisgender women, gay/lesbian and heterosexual women shared similar levels of depression, anxiety, and loneliness. Cisgender women who identified as bisexual or “another” or multiple sexual identities reported significantly higher depression, anxiety, and loneliness levels than their heterosexual counterparts in the initial model.
Ordinary Least Squares Models Regressing Support Types and Mental Health for Cisgender Women (n = 1,723).

Source: National Couples’ Health and Time Study.
Note: COVID-19 = coronavirus disease 2019; HS = high school; NH = non-Hispanic.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
The emotional support indicators did not explain the sexual identity disparities in mental health outcomes. For partnered cisgender women, family and partner support were significantly negatively associated with depression and anxiety, but only friend and partner support were associated with loneliness. Mediation analyses indicated that relative to heterosexual cisgender women, sexual minoritized identities were indirectly associated with depression, anxiety, and loneliness through family support (lesbian women depression 95 percent CI = 0.018 to 0.055, anxiety 95 percent CI = 0.016 to 0.061, and loneliness 95 percent CI = 0.014 to 0.064; bisexual women depression 95 percent CI = 0.017 to 0.054, anxiety 95 percent CI = 0.015 to 0.059, and loneliness 95 percent CI = 0.013 to 0.062; another/multiple sexual identities depression 95 percent CI = 0.019 to 0.060, anxiety 95 percent CI = 0.018 to 0.066, and loneliness 95 percent CI = 0.014 to 0.068). Additionally for cisgender women, the association between sexual minoritized identities and depression and loneliness were indirectly influenced via partner support, but anxiety was not (lesbian women depression 95 percent CI = −0.048 to −0.014 and loneliness 95 percent CI = −0.124 to −0.050; bisexual women depression 95 percent CI = −0.041 to −0.010 and loneliness 95 percent CI = −0.124 to −0.050; another/multiple sexual identities depression 95 percent CI = −0.038 to −0.008 and anxiety 95 percent CI = −0.105 to −0.025). Last, all mental health outcomes for women who identified as bisexual and another or multiple sexual identities were indirectly influenced by friend support (bisexual women depression 95 percent CI = −0.018 to −0.001, anxiety 95 percent CI = −0.023 to −0.001, and loneliness 95 percent CI = −0.028 to −0.003; another/multiple sexual identities depression 95 percent CI = −0.016 to −0.000, anxiety 95 percent CI = −0.020 to −0.000, and loneliness 95 percent CI = −0.027 to −0.002).
After the addition of the sociodemographic indicators, the disparity in anxiety and loneliness between cisgender women reporting another or multiple sexual identities and cisgender women with heterosexual identities was explained, but the disparity in depressive symptoms remained. In our formal mediation analysis, all three mental health outcomes for partnered cisgender women of all sexual minoritized identities were indirectly associated with family support (lesbian women depression 95 percent CI = 0.015 to 0.048, anxiety 95 percent CI = 0.009 to 0.051, and loneliness 95 percent CI = 0.004 to 0.053; bisexual women depression 95 percent CI = 0.009 to 0.037, anxiety 95 percent CI = 0.007 to 0.041, and loneliness 95 percent CI = 0.003 to 0.040; another/multiple sexual identities depression 95 percent CI = 0.012 to 0.046, anxiety 95 percent CI = 0.009 to 0.045, and loneliness 95 percent CI = 0.003 to 0.049). Additionally, women of all sexual minoritized identities were indirectly associated with depression and loneliness through partner support (lesbian women depression 95 percent CI = −0.046 to −0.012 and loneliness 95 percent CI = −0.120 to −0.043; bisexual women depression 95 percent CI = −0.030 to −0.003 and loneliness 95 percent CI = −0.077 to −0.004; another/multiple sexual identities depression 95 percent CI = −0.027 to −0.001 and loneliness 95 percent CI = −0.074 to −0.001). Last, the association between bisexuality and loneliness operated indirectly through friend support (95 percent CI = −0.022 to −0.000) and friend support was not indirectly related to mental health for other minoritized sexual identities.
The final model showed how the other covariates were associated with mental health outcomes for partnered women. The disparities between bisexual and heterosexual cisgender women remained significant and positive in every model for each of the mental health outcomes. Regarding the sociodemographic covariates, non-Hispanic Black cisgender women had lower levels of depression, anxiety, and loneliness compared with non-Hispanic White cisgender women. Non-Hispanic Asian cisgender women had lower levels of anxiety, and cisgender women with another racial/ethnic identity had lower levels of loneliness than non-Hispanic White cisgender women. Age was negatively associated with all three mental health outcomes for cisgender women. We found that experience with aggressions and COVID-19 stress were positively associated with all three mental health outcomes. Additional analyses indicated that COVID-19 stress operated similarly for each sexual identity.
Discussion
Consistent with prior work there were distinct gender differences in mental health and emotional support. Stratifying the sample between partnered cisgender men and cisgender women allowed us to examine how emotional support shaped associations between mental health outcomes and sexual identity. Our findings parallel prior work that showed women reported higher levels of negative mental health outcomes but received more emotional support than men. However, among both men and women emotional support was associated with improved mental health. Family support was most consistently significantly associated with lower levels of depression, anxiety, and loneliness. Friend support was only related to lower levels of loneliness among women. Partner support was directly associated with lower levels of depression and loneliness for partnered cisgender men and women, but not anxiety.
A contribution of our work is a focus on individuals with a range of sexual identities. MST suggests that individuals with marginalized identities face unique stressors as a result of their stigmatized identity. The initial models stratified by gender provided support for MST as those with sexual minoritized identities generally had higher levels of depression, anxiety and loneliness. The stress process framework posits that increased stress may lead to adverse outcomes, and these outcomes may be mitigated by buffers or coping resources. We found for gay, cisgender men, and men with another or multiple identities that emotional support, specifically family and partner support, served as a buffer to two mental health outcomes: depression and loneliness. In contrast, these framework’s suppositions did not hold for partnered cisgender women identifying as bisexual (plus pansexual, omnisexual, and queer) as their lower mental health persisted across models, thus resulting in partial support for the stress process framework. Partnered lesbian women reported levels of depression, anxiety and loneliness on par with heterosexual women. Among both cisgender women and men, experiences with aggressions and COVID-19 stress were associated with negative mental health outcomes. This suggests that the individuals who struggled with COVID-19 stress the most during the pandemic and those who experienced aggressions did not fare well.
It is notable that both bisexual men and bisexual women had lower levels of mental health than heterosexual individuals, and these associations were not attenuated with the inclusion of emotional support or the sociodemographic, minority stress or COVID-19 stress measures. Individuals with bisexual identities are a significant population, as they represent about half of individuals identifying as sexual minoritized people, and the bisexual identity is especially more common among younger individuals (Julian, Manning, and Westrick-Payne 2024). We found that for bisexual women there were indirect pathways to at least one indicator of mental health via family, partner, and friend support, but for bisexual men the only indirect pathway was via family support to depression and anxiety. Thus, this showcases the unique ways that bisexual identities operated for men and women and calls for further attention to the specific and potentially unique sources of stress and emotional support among the bisexual population.
We found several key indirect pathways through which minoritized sexual identities were associated with mental health. Although in the final model there were no direct associations between sexual identity and depression as well as anxiety for men, there were indirect associations through family support. These findings suggest that family support is an important factor to consider in analysis of sexual minoritized men’s mental health. Among partnered cisgender lesbian women there were no direct associations with mental health, but there were indirect pathways through family and partner emotional support. Bisexual women both directly and indirectly (via friend, family, and partner support) experienced lower levels of loneliness. Women who identified as another sexual identity indirectly experienced lower levels of mental health through family support and lower levels of depression and loneliness through partner support. Thus, the pathways between emotional support and sexual identity are important to consider among men and women but do appear more complex for women.
Although this study makes an important contribution to literature on sexual identity, emotional support, and mental health, it is not without limitations. One limitation of this study is that it was cross-sectional, which hindered our ability to observe pre-pandemic effects of emotional support and mental health outcomes by gender. Furthermore, the lack of longitudinal data meant our analyses were restricted to associations among the indicators.
Second, only measures of emotional support were included in this study, so the analyses did not account for other forms of support such as instrumental and informational support. The measures of support also were not specific to individuals with minoritized sexual identities. Additionally, in this study we examined friends, family, and spouses or partners as sources of support and not sources of micro- and macro-aggressions.
Third, NCHAT included only partnered individuals so we cannot observe emotional support and mental health linkages among unpartnered sexual minority people. Single individuals may have greater demands for emotional support and are an important population to study.
Fourth, although this study was focused primarily on internalized mental health, we acknowledge research by Rosenfield and Mouzon (2013) indicating that men and women manifest issues differently, with men being more likely to externalize their mental health challenges.
Fifth, we did not consider overlapping minoritized identities related to race/ethnicity or social class. Future research should carefully assess how these intersecting identities are related to emotional support and mental health.
Last, this study was limited to individuals identifying as cisgender, excluding transgender and gender-nonconforming individuals. Furthermore, attention to this population is warranted as they may face even greater threats to their mental health.
This study contributes to our understanding of how emotional support may shape mental health outcomes. Although men receive lower levels of emotional support, it appeared to play a larger direct role in the association between sexual identity and mental health outcomes for cisgender men than cisgender women. Strikingly, people who identified as bisexual had the lowest mental health outcomes and emotional support did not appear to directly attenuate these disparities. This suggests a need for further investigation for individuals identifying as bisexual and their levels of and access to emotional support. We found many indirect pathways through which sexual identity operated, suggesting that future research should consider the more nuanced ways that sexual identity and mental health are linked. These findings present a more complex portrait of sexual identity and mental health that needs to be further developed in minority stress framework. MST could be expanded to incorporate the complexities of intersecting gender and sexual identities. Furthermore, our work confirms minority stress perspectives arguing that emotional support is a key mechanism through which sexual identities relate to mental health, but an important next step is to extend the theoretical focus to variation according to specific sexual and gender identities, sources of support, and mental health outcomes. Net of the emotional support indicators and other covariates, aggressions and COVID-19 stress were crucial factors when examining mental health outcomes by sexual and gender identity. Future research should take these into account, as well as include individuals who do not identify as cisgender for a more diverse understanding of mental health and gender identity. As growing shares of the population possess more complex gender and sexual identities, these questions will be increasingly important. Emotional support is vital for mental health, and not all individuals have equal access to support from their families, partners, and friends.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NCHAT is funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development of the National Institutes of Health (grant 1R01HD094081-01A1). This project benefited from support provided by P2C infrastructure grants from the Eunice Kennedy Shriver Eunice Kennedy Shriver National Institute of Child Health and Human Development to the Minnesota Population Center (grant P2CHD041023), the Center for Family and Demographic Research (grant P2CHD050959), and The Ohio State University Institute for Population Research (grant P2CHD058484).