
Abstract
Despite growing interest in exploring caregiving alternatives beyond traditional models, limited research has focused on the diverse care networks that provide assistance to older adults. The aim of this study is to illuminate the complexity of older adults’ care networks by developing a typology that considers care from various sources. Using latent class analysis on longitudinal data from the National Health and Aging Trends Study, the authors identify five distinct care network types: spousal care, care exclusively from children, care from both children and other sources, self-care with assistive technology, and care exclusively from nonfamily sources. Further analysis, including multinomial logistic regression and latent transition analysis, reveals that when a spouse is available, older adults, particularly older men, are more likely to rely on spousal care. However, in cases in which spouses and/or children are unavailable, older adults are inclined to turn to diverse care networks involving nontraditional caregivers or resort to self-care using assistive technologies. Additionally, declining health conditions are associated with a higher likelihood of receiving care from more varied care networks. This underscores the evolving nature of care arrangements in response to changing family structures and health needs.
Nearly half of older Americans living at home either require assistance with routine daily activities or are currently receiving such help (Freedman and Spillman 2014). Historically, most of this care has been provided by spouses and adult children. However, the gap between the growing need for care among older Americans and the availability of traditional family caregivers is widening because of significant social changes. The United States is experiencing a rapid aging of its population, families have fewer children, older adults are more likely to remain never married or to experience divorce and repartnering, and adult children often live farther away from their parents than in previous generations (Seltzer and Bianchi 2013; Silverstein and Giarrusso 2010).
On a positive note, older adults are increasingly receiving support from nontraditional caregivers, including siblings, friends, and other nonkin individuals. Additionally, the use of assistive technologies enables older adults to maintain independent living for longer periods. For example, a significant proportion of older adults have successfully accommodated declines in capacity by using assistive devices (Freedman, Kasper, and Spillman 2017). Furthermore, the Internet has become an essential aspect of daily living for most Americans, and older Americans are no exception. Numerous studies have identified beneficial effects of Internet use on the well-being of older adults (Kim and Han 2022; Nam, Han, and Gilligan 2019), prolonging their independence and reducing their reliance on other caregivers (Schlomann et al. 2020). Despite growing concerns about the shortage of family caregivers and increasing interest in alternative care arrangements beyond spouses and adult children, limited research attention has been directed toward the provision of care by these increasingly diverse care networks.
Although many previous studies have explored the use of care among older adults, they often oversimplify the complexity of care networks and overlook the diversity of sources from which care is received. Only recently, a growing number of studies have stressed the significance of studying multiple caregivers or care networks and have pointed out the limitations of previous research, which primarily focused on a single primary caregiver (Ellis et al. 2023; Hu et al. 2023). Care networks for older adults are typically defined as combinations of informal and formal caregivers who provide support because of health issues such as functional limitations and chronic diseases (Jacobs et al. 2018; Keating and Dosman 2009). Furthermore, with the availability of self-care options through assistive technologies on the rise (Anderson and Wiener 2015; Freedman et al. 2017), definitions of care networks must also encompass these self-care possibilities. Thus, there is an urgent need to redefine care networks while examining the diverse sources from which care originates. It is essential to recognize that older adults themselves respond dynamically to complex situations in later life, maintaining, reinforcing, or dissolving certain types of care within their networks.
In this study, we use the rich caregiving data collected from the National Health and Aging Trends Study (NHATS). We first construct a care network typology to capture the diverse sources of elder care, illustrating how the distribution of informal care, formal care, and self-care varies across different network types. We then conduct multivariate analyses to explore potential factors associated with participation in different types of care networks. Our particular focus is on understanding how the availability of traditional family caregivers, the proximity of various types of social network members, and the care needs of older adults may contribute to the formation of distinct care networks. In the final part of our analysis, we leverage the longitudinal design of the survey to examine transitions in care networks over time and their associations with changing life events and declines in the health of older adults. Our goal is to provide a comprehensive understanding of the diverse and dynamic features of care networks in later life.
Background
Population Aging and the Second Demographic Transition
The current growth of the population aged 65 years and older is one of the most significant demographic trends in the history of the United States (Mather, Jacobsen, and Pollard 2015). The proportion of the population aged 65 and older was only 9 percent in 1960, but it increased to 15 percent in 2014, and by 2030, one in five Americans will be aged 65 and older (United Nations 2019). Although we have witnessed declining disability rates among older Americans (Crimmins et al. 2009), the more rapid trend of an aging population has resulted in a greater number of older people with disabilities. Therefore, there is an increasing number of older adults in need of long-term care, and this problem is expected to become more serious with more recent cohorts of older adults, especially those of the baby boom generation, entering old age.
Simultaneously, the American family has also undergone transformation, leading to significant changes in family relations, structures, and behaviors. Family changes such as declining marriage and childbearing, as well as increasing divorces and childlessness, are so profound that some scholars refer to them as the second demographic transition (SDT) (Lesthaeghe and Neidert 2006). For example, the rate of gray divorce doubled between 1990 and 2010 (Brown and Lin 2012), and one in three baby boomers was found to be unmarried (Lin and Brown 2012). Additionally, rates of childlessness have nearly doubled since 1980, and among recent cohorts of women, one in five of them had no children by the end of their childbearing years (Hayford 2013).
The SDT challenges traditional care systems in two different ways. First, family relations of older adults who are affected by the SDT are more fluid and less predictable because of family changes such as reduced fertility and increased divorce and remarriage. Second, older adults are indirectly influenced because their children, who are traditionally expected to provide care, have also experienced the SDT. For example, much-delayed marriage and childbearing increase the probability of the younger generation being sandwiched between multiple caregiving responsibilities for aging parents and dependent children (Wiemers and Bianchi 2015). As a result, the availability of traditional family caregivers cannot be assumed, and a growing number of older adults voluntarily construct care networks with an increasing involvement of nontraditional caregiving sources, such as siblings, grandchildren, friends, formal caregiving, and technologies.
The life course perspective provides a useful framework for studying care networks of older adults within a changing context (Elder, Johnson, and Crosnoe 2003). On the basis of the principle of lifespan development, older adults who have been exposed to different life events because of the SDT may rely on different networks to meet their care needs. Therefore, variations in care networks in later life reflect their family relationships and social networks constructed throughout their life course. The principle of agency emphasizes that individuals do not passively react to social influence, but instead construct their life course through their decision making. When experiencing social changes that may challenge the validity of traditional systems of care for the elderly, older adults also make adjustments in their care networks, such as relying on discretionary, constructed nonkin relationships for help or maintaining independence as long as possible by making use of assistive environments and technologies.
Care Networks beyond a Spouse and Children
Historically, the primary caregivers for older individuals requiring daily care have typically been spouses or adult children. From 1989 to 1999, the proportion of family caregivers that were spouses and adult children remained relatively stable, each accounting for about 40 percent of caregivers (Agree and Glaser 2009). A more recent estimate from 2015, focusing on older adults receiving support, showed that 49 percent of care was provided by spouses, while 36 percent came from their adult children (Wolff et al. 2018). Although both spouses and children were prevalent caregivers, studies have also revealed that spouses often served as primary caregivers without external assistance, whereas adult children often shared caregiving responsibilities with others, including paid caregivers, because of their other commitments such as employment and childcare (Allen et al. 2012). Therefore, understanding care network components beyond traditional caregivers not only aids older adults facing a shortage of traditional caregivers but also eases the burden on these caregivers.
According to the social convoy model, individuals are surrounded by supportive others throughout their life course (Antonucci, Ajrouch, and Birditt 2014). For older adults, a wealth of literature has documented these supportive convoys of social relationships, which have a protective impact on their well-being in later life (Cheng et al. 2009; Cornwell and Schafer 2016; Tolkacheva et al. 2011). Thus, even as the prevalence of traditional caregivers decreases, older adults, being encircled by multidimensional convoys, may still find ways to navigate challenges posed by undesirable life events through their social and familial connections beyond spouses and children or by using other resources to overcome daily activity limitations.
Although the pool of traditional caregivers shrinks, several social trends may introduce alternative care options and contribute to more diverse care networks. First, relationships with extended family members are gaining significance. Siblings are expected to play an increasingly pivotal role as informal caregivers, especially as members of the baby boom cohort, originating from larger families and experiencing higher divorce rates, reach old age (Agree and Glaser 2009). Furthermore, the importance of multigenerational bonds is growing because of extended life expectancies and increasing family diversity (Bengtson 2001). Grandchildren are also poised to take on familial responsibilities. Consequently, these extended kin relationships have the potential to usher in numerous alternative family caregivers beyond spouses and children.
Second, nonkin relationships, such as friends and neighbors, are assuming greater importance in the social networks of older adults. Nonkin connections are often based on voluntary choices by older adults and help maintain their sense of autonomy (Suanet, Van Tilburg, and Van Groenou 2013). Evidence from the Netherlands has shown that friends are becoming increasingly instrumental in providing support in later life; for more recent cohorts of older adults, they are as likely to receive support from friends as from family members (Suanet and Antonucci 2017).
Technological advancements also offer older adults more opportunities for independent living. The use of assistive technology has surged over recent decades and contributed to a decline in disability rates among older Americans (Freedman et al. 2005; Schoeni, Freedman, and Martin 2008). For example, mobility-related devices enable older adults with some level of physical disability to move independently without requiring personal assistance. Other devices, in conjunction with informal and formal care, have bolstered older adults’ capacity to maintain independence in their daily activities (Freedman et al. 2017). In addition to assistive devices, emerging research has found that Internet use can help older adults maintain independence by assisting with daily tasks and increasing social engagement (Kim et al. 2017; Nam et al. 2019). Although there is a growing body of literature examining the role of assistive technologies in supporting older adults in need of care, it remains less studied compared with personal care. Moreover, little is known about how personal care and assistive technologies can be combined to provide support for disabled older adults. In this study, we move beyond traditional measures of care networks that simply treat older adults as care recipients. Instead, we suggest that older adults can choose to self-care with assistive technologies for certain activities. Technology may not entirely replace the role of traditional caregivers, but it can alleviate caregiver burdens and enhance older adults’ independence.
Factors Associated with Care Networks
The behavioral model of health service use (Andersen and Newman 2005) has been widely used to categorize predictors that influence the receipt of care (Andersson and Monin 2018; Jacobs et al. 2018; Potter 2019). The model identifies three dimensions of individual characteristics that may influence older adults’ care networks: predisposing factors, enabling factors, and need factors. Predisposing factors encompass characteristics that predispose an individual to seek care and are often indicated by sociodemographic variables, such as gender, age, race/ethnicity, and socioeconomic status (SES). These factors exist regardless of whether individuals require care. As the primary aim of this study is to explore how older adults adapt to the changing context of caregiving associated with the shrinking availability of traditional family caregivers and the growing care needs in later life, we focus on enabling and need factors while controlling for predisposing characteristics.
Enabling factors signify the family and social contexts through which care from diverse sources is facilitated when older adults require support. The availability of traditional caregivers (i.e., spouses and children) is often considered a major predictor of older adults’ care networks (Jacobs et al. 2018). If a spouse is available, older adults primarily rely on spousal care, often without support from others or formal services (Glauber 2017). In cases in which widowed older adults need care or both members of an older couple require assistance, children play an integral role in caring for their parents. However, compared with spousal care, care from children is more complex because of potential issues related to the allocation of caregiving responsibilities among siblings (Grigoryeva 2017) and the multiple role commitments of children in their midlife (Evandrou, Glaser, and Henz 2002). Thus, although children are still considered major caregivers after spouses, their involvement introduces more uncertainty and heterogeneity into care networks. In addition to spouses and children, older adults’ social networks, consisting of extended kin and nonkin relationships, also provide access to potential helpers outside the household when needed. Existing literature has well documented the benefits of social networks for the well-being of older adults through various psychological and physiological pathways (Cornwell and Schafer 2016).
Need factors pertain to the necessity of care because of health problems and are considered the most significant determinant of whether different types of care will be introduced into the care network (Agree and Glaser 2009). Greater severity of underlying care needs results in the accumulation of multiple sources of care and more intensive care. Conversely, older adults with low to moderate levels of impairment are less likely to use formal home-care services than those with high levels of impairment, particularly those with cognitive impairments (Lee and Penning 2019). Over time, caregiving becomes more complex and challenging because of increasing disability and the burden of chronic diseases. A recent study has also found that although older adults with multiple chronic conditions and dementia have larger care networks than those without such issues, they encounter more difficulty in meeting their care needs (Beach et al. 2020).
Most previous studies applying the behavioral model to the analysis of care use typically examine the cross-sectional association between the aforementioned factors and care networks. Few longitudinal studies have explored care transitions. One exception is Allen et al.’s (2012) research on transitions on transitions in older adults’ informal caregivers. Their findings have identified several primary caregiver characteristics (e.g., gender and relationship type) associated with transitions from informal care to formal care or no care. Another longitudinal study of Dutch older adults identifies a sequence in care arrangements from no care through informal care to professional care, with these transitions driven primarily by changing health conditions of older adults (Geerlings et al. 2005). On the basis of the life course perspective, changes in enabling and need factors, such as the loss of a spouse and declining health, are normative events in later life that may function as “turning points” in older adults’ care arrangements. Therefore, this study extends the behavioral model of care use to examine dynamic features of care networks, including transitions between different types of diverse care networks and how they are associated with changes in enabling and need factors.
Care Networks for Older Women and Men
It is well established that women live longer than men but are more likely to suffer from later life disabilities (Read and Gorman 2010). Recent evidence even indicates that the gender gap in disability prevalence has increased over the past three decades (Freedman, Wolf, and Spillman 2016). Consequently, women experience a longer period of needing care than in previous years. Older women and men may also differ in their care networks. Although men are increasingly involved in spousal care, women still bear a heavier caregiver burden, particularly as they often outlive their husbands and are expected to assume the role of primary caregiver according to traditional gender roles (Swinkels et al. 2019). Additionally, a recent study found that the lack of close kin is more prevalent among women than men (Margolis and Verdery 2017).
Despite continued gender disparities in many social resources, women often serve as kin-keepers in families and are less affected by the absence of a spouse in care networks (Potter 2019). For example, existing literature has demonstrated that women have larger care networks with diverse care sources compared with men (Andersson and Monin 2018). Social network research has also shown that older women maintain more connections to family members, friends, and neighbors and are more engaged in the community (Cornwell and Schafer 2016). Although the use of assistive technologies has seen rapid growth in the past two decades, some recent literature discusses gender differences in the use of various devices and technologies in later life. A higher percentage of older women are found to use mobility devices compared with older men (Peterson et al. 2017), whereas women are less likely to access and use information technology, such as the Internet (Kim et al. 2017). Although gender differences in receiving or using a single type of care have been widely studied in previous literature, to the best of our knowledge, no studies have examined gender differences in combinations of different types of care. Therefore, in this study, we compare diverse care networks between older men and women to understand how they receive different forms of care when facing functional limitations and subsequently explain gender differences in care networks from the perspective of enabling and need factors derived from the behavioral model of care use.
Research Objectives
With a diminishing pool of traditional caregivers and increasing alternatives for new types of caregiving, care networks for older adults have become more complex and multidimensional. However, although there is ample knowledge on traditional caregivers such as the spouse and adult children, beyond these traditional figures, detailed information is lacking on the size and composition of care networks of older adults (Jacobs et al. 2018). Most existing studies characterize elder care in terms of dichotomies, for example, care versus no care, formal versus informal care, family versus nonfamily care, and often fail to capture that care networks may contain mixes of different types of caregivers at any given point in time and may shift as individual needs change. To address this gap in the literature, we apply latent class analysis (LCA) to examine how elder care from multiple sources exists simultaneously but in varying combinations in older adults’ care networks (details are discussed in the “Methods” section). We further explore the determinants and dynamic features of care networks from the perspectives of the availability of potential caregivers and a series of health indicators.
This study starts by developing a care network typology that captures the multidimensionality of care networks with a combination of different types of caregiving, such as informal care from different kin and nonkin relationships, formal care, and self-care with assistive technologies. Instead of analyzing care from different sources separately, we seek to understand mixes of care from diverse sources. With increasing numbers of older adults entering old age with more chronic diseases, which create extra demands for care, it is imperative for older adults to receive support from multiple sources in addition to their primary caregivers. Previous studies have also found that large care networks are beneficial for caregivers involved in this network (Tolkacheva et al. 2011). To enhance the likelihood that multiple types of caregivers are identified, we use information on care provided in a variety of tasks, including personal care, household activities, mobility activities, and medical care. On the basis of all care network components collected for each respondent, we apply LCA to develop a mutually exclusive care network typology with different compositions of care types.
After constructing the care network typology, we continue to explore heterogeneous dynamics in care networks from different perspectives. To understand the determinants of care networks, following the behavioral model of care use and social convoy model, which suggest that older adults’ choice of care is conditioned by enabling and needs conditions, we examine how the availability of potential caregivers and health conditions of older adults are associated with their involvement in different types of care networks. We expect that when the spouse and children are unavailable, older adults are more likely to be supported by nontraditional caregivers and/or engage in self-care with assistive technologies. Related to need factors, older adults with worse health conditions are more likely to receive care from larger and more diverse care networks. Drawing from the life course perspective, changes in enabling and need factors may also lead to transitions in older adults’ care networks in later life. Therefore, using the longitudinal design of NHATS, we further expect that family events (i.e., the loss of a spouse and transition to intergenerational coresidence) and declines in the health of older adults are associated with a higher likelihood of transitions in their care networks, especially transitions into a diverse care network type, compared with those who do not experience such life events.
Considering widespread gender differences in family and social life, we further compare older women and men in their care network compositions. Previous studies have consistently shown that women play the role of kin-keeper and thus have larger kin networks than older men. Older women are also found to be advantaged in nonkin social networks. However, at the same time, women usually have lower SES than men, which may hinder their access to paid formal caregiving and assistive technology uses. Therefore, we hypothesize that older women are more likely than men to receive support from children, extended kin, and nonkin informal caregivers. In contrast, older men are more likely than women to receive support from their spouses, formal caregivers, and/or choose to self-care with assistive technologies.
Methods
Data and Sample
This study uses data from the 2011 to 2018 waves of NHATS, a nationally representative annual survey of adults aged 65 years and older (Freedman and Spillman 2014). NHATS relies on Medicare enrollment files for its sampling frame. Conducted by the Johns Hopkins University Bloomberg School of Public Health in collaboration with the University of Michigan, the study involves in-person interviews to collect information on a broad range of characteristics related to the well-being of older Americans. NHATS was initiated in 2011 with the aim of capturing a detailed picture of daily life functioning among older adults, including the different types of assistance they receive and the service environments in which they live. The sample was replenished in 2015 to provide a refreshed nationally representative cohort of the Medicare population aged 65 and older (Freedman and Kasper 2019).
Figure 1 illustrates how the analytic sample was derived from the NHATS sample to construct the care network typology (using the 2011 wave as an example). We restricted the sample to individuals residing in either communities or residential care settings and also excluded proxy interviews. Furthermore, we selected participants who both needed assistance because of health problems and received help from other people to perform various daily activities. The final sample consists of 20,583 person-year observations (7,692 person-years for men and 12,891 person-years for women) on 7,357 older adults (2,970 men and 4,387 women).
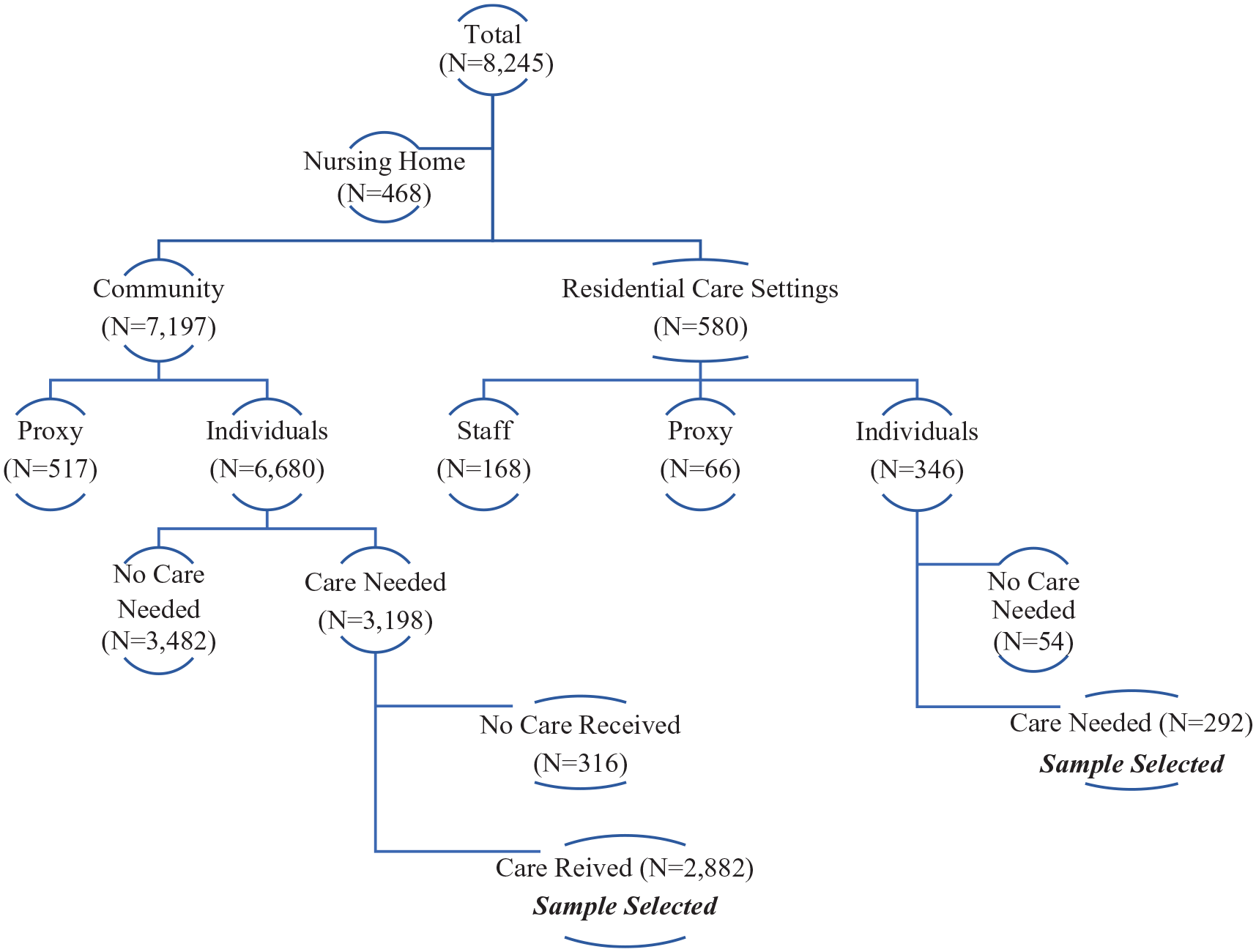
Sample selection for latent class analysis (using the 2011 wave as an example).
Care Network Identifications
The first main purpose of this study is to explore diversity in older adults’ care networks. Each NHATS respondent was asked whether they received any help in the last month with activities of daily living (ADLs), mobility, instrumental ADLs (IADLs), or medical care, and to identify their relationship with each caregiver. Help with ADL tasks is defined as assistance with personal care such as bathing, dressing, eating, and toileting. Mobility-related activities encompass tasks such as getting out of bed, moving around inside the home, and going outside the home. Receiving help with IADL tasks is defined as assistance with a series of household activities, specifically doing laundry, preparing hot meals, shopping for personal items, and managing bills/banking. Medical care is specified as assistance with handling medications, doctor visits, and health insurance matters. For each task, the survey reported every person who provided help with that specific task, and a total of 42 caregiver types were included in NHATS. We collapsed these 42 types into five broad categories: spouse, adult children, extended kin, nonkin informal caregivers, and formal caregivers.
NHATS also collected information on the use of assistive technologies in performing daily activities, mobility tasks, and managing health matters. Assistive technologies include assistive devices for daily activities and the use of the Internet for household tasks and obtaining health-related information. Respondents who used three or more assistive devices were classified as active users, and they were further categorized based on their use of the Internet for household tasks and health matters, such as grocery shopping, ordering prescriptions, and contacting medical providers. Therefore, we have created seven dichotomous variables as care network identifications: (1) spouse, (2) children, (3) extended kin, (4) nonkin, (5) formal caregiving, (6) self-care with assistive devices, and (7) self-care with the use of the Internet. Table 1 provides detailed descriptions of each care network identification included in this study.
Description of Care Network Identifications.

Predictors of Care Networks
Enabling Factors
After constructing their typologies, we continue to explore potential factors that are likely to structure care networks. Following the behavioral model of care use (Andersen and Newman 2005), we focus on enabling factors that facilitate care use and need factors that indicate the necessity of care in this study. For enabling factors, we measure the pool of potential caregivers through older adults’ marital status, characteristics of children, and social networks beyond the spouse and children. Marital status is measured as a dichotomous variable (married or partnered or not). All living children are counted to create three variables: having a coresident biological child; the number of biological children not living with parents, and the number of stepchildren. Older adults are also asked to report up to five social network members that they identify as people with whom they can discuss important matters. Excluding spouses and children, we construct two variables measuring the number of extended kin and nonkin social networks.
Need Factors
For need factors, we measure various health problems faced by older adults, including different types of functional limitations with daily activities, the number of chronic diseases, and their dementia status. Functional limitations are measured as three dichotomous variables regarding whether older adults have difficulty performing ADLs, IADLs, and mobility tasks. Chronic diseases are assessed by asking respondents whether they had been diagnosed with any of 10 chronic illnesses (e.g., heart diseases, diabetes, stroke). For dementia status, NHATS classified respondents into three groups—no dementia, possible dementia, and probable dementia—on the basis of the self-reported diagnosis of dementia or Alzheimer’s disease, an AD8 Dementia Screening Interview, and cognitive tests (Kasper, Freedman, and Spillman 2013).
Sociodemographic Characteristics
We further adjust for other sociodemographic characteristics of older adults, including birth cohorts, age, gender, race, living arrangements, and SES. We categorize older adults into three birth cohorts (born 1901–1926, 1927–1945, and 1946–1950) and four racial/ethnic groups (non-Hispanic White, non-Hispanic Black, Hispanic, and others). The living arrangement of older adults was measured as whether they lived alone and whether they lived in a residential care setting. We used the highest degree of education (less than high school, high school graduate, and some college but no degree, or college graduate) and total household income to measure SES. Household income was a comprehensive measure of the respondent’s earnings, spousal earnings, capital income, pensions and annuities, and other income. For those who were missing in any variables measuring income, we used the imputed values of income provided by the NHATS team (DeMatteis, Freedman, and Kasper 2016). Income was then logged to reduce the skewness and to obtain a better interpretation of the regression coefficient.
Predictors of Care Network Transitions
Finally, to examine the effect of life events and changing circumstances on transitions of latent classes over time, the following dichotomous measures are constructed using information from two adjacent time points: whether older adults become widowed, whether they start living with a child, and whether they experience health declines. Decline in health status is measured as older adults becoming less able to perform mobility tasks, ADLs, IADLs, and acquiring more chronic diseases than in the previous wave (reference, no change).
Analytical Strategies
This study comprises three main phases of analysis. First, we use LCA to identify distinct care networks based on seven dichotomous variables representing care network components. LCA discerns mutually exclusive latent classes, maximizing heterogeneity between them while ensuring homogeneity within each class. The LCA approach offers advantages over previous studies that often analyze each care type separately, enabling us to capture the multidimensional features of care networks. Additionally, LCA has an edge over standard cluster analysis as it makes no assumptions about the distribution of indicators (Vermunt and Magidson 2002). To determine the optimal number of class memberships (i.e., care network types), we compare models using statistics such as the Akaike information criterion and Bayesian information criterion, alongside theoretical considerations regarding the meaningfulness of the class solution.
After constructing the care network typology, we further explore the determinants of care networks by considering potential predictors related to the pool of available caregivers and health conditions. We conduct multinomial logistic regression analysis to predict care network typologies. In line with previous studies using similar clustering methods (Ali et al. 2022; Lin and Chen 2021), we present odds ratios for variables to estimate the likelihood of belonging to a specific care network type compared with the reference group. All continuous variables are standardized to have zero mean and unit variance.
Finally, to examine how care networks of older adults change over the eight waves of this study, we assess the probabilities of latent classes within care networks changing over time using latent transition analysis (LTA). We explore transitions in and out of specific care network types as a function of changes in life events and evolving circumstances. We accomplish this by using a series of logistic regression models (Hogerbrugge and Silverstein 2015). In all multivariate analyses, we cluster the standard errors by individuals to account for arbitrary within-person correlations.
Results
LCA
Appendix A presents the goodness-of-fit statistics obtained from the LCA, including likelihood ratio statistics, Akaike information criterion, and Bayesian information criterion, for models ranging from two to six classes to categorize the care networks of older adults. The statistics clearly indicate that adding a fifth class is meaningful when compared with the four-class model. The decision to distinguish five classes is not only supported statistically but also aligns well with the theoretical framework of the study. In the five-class model, one class from the four-class model is split into two, and these newly formed classes exhibit distinct features relevant to the research questions. The six-class model, on the other hand, further divides one class from the five-class model into two smaller groups, with limited differences in their care network compositions. Given the small size of one of these groups and the similarity between the two new groups, we opt for the five-class model.
Description of Five Care Network Types
Table 2 displays the item-response probabilities associated with the five-class care networks. To facilitate interpretation, we compare these probabilities with the average probabilities for the total sample. Probabilities above the average are reported in bold and are used to define each class. The first class identified is characterized as the traditional care arrangement of “spousal care” (class 1). In this latent class, older adults have a 1.0 probability of receiving care from a spouse and receive minimal assistance from other sources. Interestingly, alongside receiving care from their spouses, older adults in this class often use the Internet (0.357) to perform certain daily activities. The second class represents another traditional care practice of “care exclusively from children” (class 2). In this network, older adults exclusively receive care from their adult children (1.000). The third type of care network (labeled as “care from both children and other sources”) encompasses care from a combination of children, extended kin, nonkin, and formal caregivers. Older adults in this class also have the highest probability of using assistive devices (1.000). In contrast, the fourth group of care network (labeled as “self-care with assistive technology”) comprises individuals who have a 1.0 probability of using the Internet to perform certain daily and medical activities while also occasionally receiving support from nonkin informal caregivers. Finally, older adults in the care network without a spouse and children (class 5) receive care from extended kin, nonkin informal caregivers, and formal services, and this class is labeled as “care exclusively from nonfamily sources.”
Item-Response Probabilities and Distribution of Latent Classes.

Note: Class 1, spousal care; class 2, care exclusively from children; class 3, care from both children and other sources; class 4, self-care with assistive technology; class 5, care exclusively from nonfamily sources. Boldface type indicates the probability that centrally defines the class.
The probability distributions of the latent classes are presented in the lower part of Table 2. In total, 32 percent of cases are cared for by a spouse, 14 percent solely by adult children, 37 percent receive care from children and other diverse sources, 9 percent opt for self-care through assistive technology, and the remaining 8 percent are supported by a care network consisting of extended kin, nonkin, and formal caregivers. Although the aggregate probabilities of latent classes remain relatively stable over time, there are still some changes in care network compositions. A more detailed analysis of transitions in and out of certain care networks across eight waves of the survey is presented in the subsequent section.
Factors Associated with Care Network Types
After constructing the care network typology, we examined the factors associated with involvement in each type of care network relative to the reference group (class 1) using multinomial logistic regression models, as presented in Table 3. Both enabling factors and the necessity of care because of health problems play significant roles in determining how older adults are cared for when they require assistance. Those living with a child have the highest odds of being in class 2, receiving care exclusively from children, followed by class 3, receiving care from both children and other sources. The primary difference between class 2 and class 3 lies in the health conditions of older adults. Individuals who report difficulties in mobility and ADL tasks have significantly higher odds of being in class 3 compared with the reference type, while no such significant findings are observed among class 2. Care network types without support from a spouse and children (classes 4 and 5) rely more on their larger social networks than other care network types. The sizes of both extended kin and nonkin social relationships are positively associated with involvement in classes 4 and 5.
Multinomial Logistic Regression Models Predicting Care Network Classes.

Note: The reference group is class 1. Results are presented in odds ratios, with numbers in parentheses representing standard errors. Results also control for sociodemographic characteristics of older adults, including the birth cohorts, race/ethnicity, age, living arrangements, educational attainment, and household income. Class 1, spousal care; class 2, care exclusively from children; class 3, care from both children and other sources; class 4, self-care with assistive technology; class 5, care exclusively from nonfamily sources. ADL = activity of daily living; IADL = instrumental activity of daily living.
p < .05, **p < .01, and ***p < .001 (two-tailed tests).
To further explore gender differences in care network types, we present predicted probabilities of latent classes by gender in Figure 2, while holding all other variables at their means (for continuous variables) and modes (for categorical variables). When in need of care, older women have a probability of 0.29 of being supported by their spouses, 0.16 of being supported by their children, 0.39 of being supported by a network involving children, extended kin, nonkin informal caregivers, formal caregivers, and assistive devices, 0.09 of conducting self-care through assistive technology, and 0.07 of being in a care network involving support from extended kin, nonkin, and paid formal services. In comparison, older men have higher probabilities of being supported by a spouse (0.35) and care networks beyond a spouse and children (0.12), and lower probabilities of being supported by care networks involving children (0.12 and 0.32).

Predicted probabilities of latent classes by gender.
Transitions in Care Networks
In this part of the analysis, we examined transitions among care network types and the factors influencing these transitions. Table 4 displays the transition probabilities in care network latent classes across the eight waves of measurement. Overall, 24 percent of the sample experienced a transition in care network typology between survey intervals (results not shown). Some classes are more stable than others, with 83.8 percent of older adults receiving care from a spouse (class 1) and 82.6 percent of those receiving support from diverse care sources involving children (class 3) remaining in the same class from 2011 to 2012.
Transition Probabilities for Care Network Classes.

Note: Class 1, spousal care; class 2, care exclusively from children; class 3, care from both children and other sources; class 4, self-care with assistive technology; class 5, care exclusively from nonfamily sources. Boldface type indicates the probability of older adults remaining in the same care network class between waves.
To investigate heterogeneity in transitions, we examined their correlates on the basis of major predictors of care networks mentioned earlier. The analytical sample was limited to respondents who participated in consecutive waves of interviews. For predictive variables, we considered both variables at time T, which were the same as those considered when assessing factors associated with care network types, and a series of dynamic variables measuring changes in family and health status between T and T + 1. Results from logistic regression models predicting transitions in care networks are presented in Table 5. Given the five classes, there were potentially 25 types of transitions and nontransitions between T and T + 1. Rather than taking an exhaustive approach, the LTA focused on the experience of any transition in general, as well as the four most prevalent transitions: the transition into class 3 and transitions out of classes 2, 4, and 5.
Logistic Regression Models Predicting Transitions of Latent Classes.

Note: Results also control for sociodemographic characteristics of older adults, including the birth cohorts, gender, race/ethnicity, age, living arrangements, educational attainment, and household income. Class 2, care exclusively from children; class 3, care from both children and other sources; class 4, self-care with assistive technology; class 5, care exclusively from nonfamily sources. ADL = activity of daily living; IADL = instrumental activity of daily living.
p < .05, **p < .01, and ***p < .001 (two-tailed tests).
The first column in Table 5 shows that the probability of older adults experiencing any transition in care networks increases when they become widowed, start living with a child, and experience health declines. Additionally, being married and having more extended kin in social networks are associated with greater dynamics in care networks. Suffering from difficulty with mobility and IADL tasks also increases the probability of experiencing transitions in care networks between time T and T + 1. The subsequent columns in Table 5 provide predictors of the four most prevalent transitions. To aid interpretation, we present the predicted probabilities of transitioning into class 3, where older adults receive care from children and other sources (see Figure 3). We selected class 3 because it represents the most prevalent care network type, and most life event predictors have a significant impact on transitions into this class. We also presented the results separately for women and men to highlight gender-specific differences in the predictors of this transition. For both women and men, changes in family and health status are closely associated with transitioning into this care network type. Specifically, widowed women and men were twice and three times as likely as those who had a spouse to experience transition into class 3, with widowed women having the highest probability to do so. Similarly, older adults who started living with a child and experienced health declines, characterized by beginning to have difficulty moving, conducting ADL activities, and having more chronic diseases than before, also underwent such changes in care networks.

Predicted probabilities of transitioning into class 3 (care from both children and others) by selected life events among older women and men.
Discussion
For generations, older Americans have traditionally relied on immediate family members, primarily spouses and adult children, for caregiving when assistance is needed. However, in recent decades, sweeping demographic and family changes have transformed the landscape of caregiving. The conventional model of care can no longer be assumed, making it increasingly important to understand the evolving dynamics of care networks beyond traditional family structures. Despite growing public interest in this area, we currently have limited knowledge about the diversity of care networks that extend beyond spouses and children. Moreover, there is a paucity of research examining how these care arrangements change over time. This study fills a critical gap in our understanding by exploring the complexity of care networks and investigating their dynamic nature in relation to individual determinants of care use.
The first objective of this study was to develop a comprehensive care network typology capable of capturing the multidimensional nature of care networks, incorporating various caregiving sources. Using LCA, we derived five distinct and mutually exclusive care network typologies, each characterized by unique compositions of care sources. These typologies include “spousal care,” “care exclusively from children,” “care from both children and other sources,” “self-care with assistive technology,” and “care exclusively from nonfamily sources.” Although nearly half of older adults continue to rely on spouses and adult children as their primary sources of support, a substantial portion of frail older individuals receive assistance or care from diverse sources. This is consistent with a group of recent studies which emphasize the importance of studying multiple caregivers instead of single primary caregiver. Some of them have delved into care intensities within care networks (Hu et al. 2023; Spillman et al. 2020), while others have examined different types of care provided (Ali et al. 2022; Ellis et al. 2023). We acknowledge that all of these studies provide essential insights into our understanding of increasingly complex care networks. However, it is worth noting that our primary focus is on who is involved across the care network, which adds new knowledge to this emerging literature.
One of the main innovations of this study is our incorporation of self-care categories into our typologies. We did this with the understanding that certain assistive devices and technologies empower older adults with physical disabilities to maintain a degree of independence without constant personal assistance. These technologies can significantly impact care needs and the ability of older adults to carry out ADLs. This approach aligns with the recent shift in focus from “successful aging” to “successful accommodation,” where older adults who adopt assistive devices report no reduction in their activity level or difficulty without assistance from others (Freedman et al. 2014, 2017). This shift is of considerable interest because it highlights the potential of these devices to substitute for costly personal assistance. In the future, research should continue to explore the implications of care networks involving self-care categories for older adults’ well-being and the quality of care they receive (Lin and Liu 2023).
To better comprehend the factors influencing care network configurations, we drew upon the behavioral model of care use (Andersen and Newman 2005). This model posits that older adults’ choices regarding care are shaped by enabling and need conditions. The findings from multinomial logistic regression models revealed that, when a spouse is available, older adults, particularly older men, are more inclined to rely on spousal care in their daily lives. However, in cases in which both spouses and children are unavailable, older adults are more likely to turn to diverse care networks involving nontraditional caregivers or resort to self-care with assistive technologies. Additionally, declining health conditions were associated with a greater likelihood of receiving care from more varied care networks. This underlines the evolving nature of care arrangements in response to changing health needs.
Building upon previous cross-sectional research on care networks, this study delved into the transitions that occur within care networks. Leveraging longitudinal data spanning from 2011 to 2018, the LTA uncovered that a substantial proportion of older adults experienced changes in their care networks over this period. These transitions were closely linked to significant life events and health declines. In cases of notable shifts in family structures, such as the loss of a spouse or transitioning into intergenerational coresidence, older adults were inclined to transition into more diverse care networks that involved their children and other caregivers, with women being more likely to do so than men. These changes often occurred in response to the increasing needs for care, particularly in ADLs, mobility tasks, and the management of chronic diseases. From a policy perspective, this highlights the importance of routinely identifying and monitoring older adults and their caregivers to ensure that changing care needs are assessed and supported in the delivery of long-term services and support.
Last, this study identified substantial differences in care arrangements between older men and women. Consistent with prior research on gender differences in spousal care, older men were more likely to rely on their wives for long-term care than the reverse scenario (Glauber 2017; Swinkels et al. 2019). Although the multivariate analysis indicated that many of these gender differences could be explained by enabling and need factors discussed in this study, it is noteworthy that the flow of care within older couples still predominantly involves care provided by wives to husbands. One potential explanation for this pattern is that the caregiver role may conflict with the gendered identity of many husbands, potentially reducing their commitment to caregiving (Allen et al. 2012). In contrast, older women were more likely than older men to have their children involved in their care networks, either relying exclusively on their children for assistance or receiving support from a combination of children and other care sources. These findings reaffirm the kin-keeping roles traditionally associated with older women within families and align with social network literature demonstrating the stronger network connectedness of older women compared with older men (Cornwell and Schafer 2016; Potter 2019).
Several limitations of this study warrant consideration. First, although the NHATS provides comprehensive information on the different sources of care received by older adults, it does not encompass all possible characteristics of caregivers within each care network type. For example, this study identified two distinct care network types involving care from adult children—one reliant solely on children and another in which care is provided by children alongside other diverse sources, such as extended kin and formal caregivers. Although the analysis has revealed that older adults’ care needs are positively associated with receiving care beyond children, it is plausible that the circumstances of adult children may also influence their parents’ receipt of care from various sources. This complex interplay between older adults’ needs and caregivers’ circumstances merits further investigation.
Second, to provide an up-to-date portrayal of care networks among U.S. older adults, we conducted research using the most recent nationally representative data. However, it is essential to acknowledge that the proportion of the baby boomer cohort (born after 1945) within the dataset remains relatively small (7 percent) in comparison with earlier cohorts. Moreover, an even smaller subset (5 percent) of this cohort currently requires care, a prerequisite for inclusion in our analysis. As the baby boomer generation continues to enter older adulthood and experience a growing need for care, future research should aim to explore how the life trajectories of different cohorts of older adults may contribute to the diversification of care networks.
Notwithstanding these limitations, this study stands as one of the pioneering efforts to explore the multidimensional aspects of care networks. By harnessing longitudinal data and innovative caregiving measures, this research offers insights into both the complexities and dynamics inherent in care networks. By including alternative caregiving sources such as extended kin, nonkin, formal caregivers, and assistive technologies, this study paints a more comprehensive picture of caregiving than what is currently available in the literature. Moreover, it provides an updated understanding of caregiving dynamics in a society undergoing significant change. Furthermore, this study carries important implications for social policies related to elder care. In the context of diminishing availability of traditional caregivers, it contributes to our understanding of the alternative options that are accessible to older Americans. This knowledge is invaluable, as it can inform the development and implementation of social policies aimed at supporting older adults in diverse care network arrangements.
In conclusion, this study takes significant strides toward unraveling the intricate tapestry of care networks among older adults in the United States. As the landscape of caregiving continues to evolve in response to demographic shifts and changing family structures, research efforts such as this one are essential for guiding policy decisions and ensuring that the care needs of older individuals are met in a dynamic and adaptive manner.
Supplemental Material
sj-docx-1-srd-10.1177_23780231231223906 – Supplemental material for Diversity and Dynamics in Care Networks of Older Americans
Supplemental material, sj-docx-1-srd-10.1177_23780231231223906 for Diversity and Dynamics in Care Networks of Older Americans by Zhiyong Lin in Socius
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Institute on Aging (grants P30AG059301, P30AG012846, U01AG032947, and P30AG066614) and by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (grant P2CHD042849).
Statement of Ethical Approval
This study used a deidentified publicly available dataset. Therefore, ethical approval was not required.
Supplemental Material
Supplemental material for this article is available online.
Author Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.