
Abstract
Two largely separate schools of sociological theory seek to explain to whom we turn in times of need. The first argues that we turn to network members who occupy socially important roles, highlighting how support behaviors cluster in certain social roles (i.e., role effects). The second argues that we turn to network members possessing relevant resources and with whom we have strong ties. The authors unite these perspectives, examining how role effects on living kidney donation behavior are explained by role groups’ endowments of situationally relevant resources and tie strength. The authors analyze two original data sets: a sample of kidney transplantation patients reporting on their social networks (n = 70 patients and 1,421 ties) and a separate sample surveying kidney disease patients’ family members (n = 1,560). The authors find that role effects on living kidney donation behavior are largely explained by the conjunction of relevant resources and tie strength, which offers several key lessons for medical support-seeking research.
To whom do we turn in times of need, and why? Sociological theory on this question is dominated by two general strains of thought. An older research tradition on role theory posits that we turn to those who occupy certain role relationships: socially recognizable groups characterized by “a set of mutual (but not necessarily harmonious) expectations of behavior between two or more actors, with reference to a particular type of situation” (Goode 1960). 1 A dominant strain in the social support literature assesses the distribution of support across role relations (e.g., Seeman and Berkman 1988; Wellman and Wortley 1989). 2 Even as it is well established that we turn to different types of role relations for different types of social support (e.g., Wellman and Wortley 1990), efforts to parse what we obtain from different sources remains relevant (Alsubaie et al. 2019). Likewise, the “convoy model” describes changing support sources over the life course as originating from “the performance of related roles” (Kahn and Antonucci 1980). 3 These and other models have inspired substantial empirical work on whether and how culturally relevant role relationships (e.g., parents, neighbors; Fischer 2011) vary in their social support dispositions. We refer to role relationships’ differences in social support probabilities as role effects.
The second tradition also seeks to categorize those to whom we turn, but rather than occupants of roles it focuses instead on attributes of people and relationships accessed (on the basis of our need, the resources they possess to meet that need, and our access to them). For instance, social capital theory attends both to social capital’s 4 creation (through “investment in social relations with expected returns”; Lin 1999:30) and activation (as “individuals capture the embedded resources in the relations to generate a return”; Lin 1999:32). Because resources are “functionally specific” and unequally distributed across network members (Perry and Pescosolido 2010), this literature highlights how network members’ situationally dependent resources structure to whom we turn to meet our needs. Similarly, the vast literature on tie strength argues that we turn to “strong ties” with whom we have durable, intimate, and frequent connections (Marsden and Campbell 1984) for support during times of crisis (e.g., Hurlbert, Haines, and Beggs 2000) and discussing “important matters” (Fischer 1982). Although Small (2017) questioned this consensus by claiming that weak ties are often vital, this work also emphasizes factors like proximity and availability. Thus, both the social capital and strong ties literatures emphasize that relationship characteristics beyond role groups dictate to whom we turn.
Only limited research seeks to unite these two traditions despite the theoretical costs of their separation. On one hand, leaving these literatures separated leaves the role effects literature resting primarily on normative expectations and obligations that arise largely unexplained. Social capital and tie strength explanations for social support could considerably enrich this understanding. On the other hand, separating these literatures also leaves social capital and tie strength explanations less fulfilling, ignoring how most social support resources come from specific role relations. For instance, close kin constitute 69 percent of close confidantes in recent years and even more in the past (Marsden 1987; McPherson, Smith-Lovin, and Brashears 2006). Without connecting these traditions, we are left with a diminished understanding of to whom we turn in times of need.
The subject of this article is help seeking during a medical crisis. There is a robust literature available on help seeking in such times, but much of it emphasizes what features of people’s networks influence assistance provision (Perry and Pescosolido 2010; Pullen, Perry, and Maupome 2018; Song and Chang 2012; see Song et al. 2011 for conceptual distinctions and further overview). In their seminal study, Perry and Pescosolido (2015:122) observed that “little is known about who is chosen to help during an episode of illness,” and accordingly examined health matters discussions during mental illness, finding substantial role effects. For instance, partners and mothers each had about a 0.5 probability of discussing health matters with the patient, a larger probability than that of any other role relations and similar to that of health professionals. In addition, they found that several network member attributes predicted health discussion partnerships, including the network member’s own mental illness history (a situationally relevant resource), emotional closeness, frequent contact, and a lack of conflict (measures of tie strength). However, our work assesses the extent to which health matters discussion role effects can be explained by network members’ situationally relevant resources and tie strength.
Our focal case is the search for a living kidney donor, which is a unique type of medical help seeking (described in detail below) that differs substantially from mental health crises. Just four role relationships account for two thirds (66.2 percent) of all completed living donations: recipients’ siblings (20.7 percent), friends and acquaintances (16.6 percent), children (15.4 percent), and spouses (13.5 percent). 5 However, the reasons for this concentration are unclear; as we argue below, it could be driven by the distribution of medical characteristics facilitating transplantation (biomedical resources), relationship characteristics promoting living kidney donation behaviors (tie strength), or some combination of these and other factors.
To assess the relative contribution of biomedical resources and tie strength to role effects on living kidney donation behaviors, we analyze two original, separately collected data sets of kidney disease patients and their network members: one reported from kidney transplantation patients’ perspective and the other reported from kidney disease patients’ family members’ perspective. Our focal living kidney donation behavior is the living donor discussion (LDD), in which the patient and network member discuss donating a kidney. In supplementary analyses, we also examine whether this discussion resulted in agreement for evaluation and whether the potential donor was tested for evaluation. Our analytical strategy is to estimate role effects on living kidney donation behaviors, then determine the degree to which network member resources and tie strength mediate these role effects. We conclude by reflecting on how these results advance understandings of living kidney donation processes and medical help seeking more generally.
Background
The Social Process of Living Kidney Donation
Living donor kidney transplantation is a medically important form of help seeking. The prevalence of end-stage kidney disease (i.e., kidney failure) has been increasing for decades (Saran et al. 2020). Three major treatment options are available for end-stage kidney disease treatment; the most common is dialysis (home or clinic based), followed by kidney transplantation from deceased donors and then kidney transplantation from living donors. However, living donor kidney transplantation offers the greatest therapeutic benefit (Hart et al. 2020; Saran et al. 2020). For instance, in the 2011 U.S. end-stage kidney disease cohort, 90 percent of living donor kidney transplant recipients survived for ≥60 months, compared with 77 percent of deceased donor kidney transplant recipients and 42 percent of dialysis recipients.
Living kidney donation is the clinical result of a social and institutional process of living donor recruitment and evaluation that occurs almost exclusively within the transplantation patient’s family or social network. Prior to donation, the patient and network member typically complete at least some of a series of precursor behaviors: (1) they have a LDD, (2) this discussion results in agreement for the network member to be medically evaluated, (3) an evaluation takes place, (4) the potential donor is approved for donation, and (5) the donation takes place. However, because steps 3 to 5 occur in transplantation clinics and are reflected in medical records, much more is known about them than earlier steps that largely occur outside of clinic walls.
Research on the preclinical processes of living kidney donor recruitment suffers from several limitations, most notably a focus on patient-reported willingness to discuss donation with network members or similar patient characteristics with uncertain correlations with actual behaviors (e.g., Lunsford et al. 2006, 2007; Reese et al. 2009). However, research also indicates that search barriers arise from difficulty initiating LDDs, patient concerns about burdening or coercing family members, and difficulty identifying willing, eligible donors (e.g., Boulware et al. 2005, 2011). Finally, among the most effective interventions at promoting living kidney donation are house calls to explain the benefits of living kidney donation to family members and friends (Rodrigue et al. 2014) and appointing patient advocates to encourage network members to consider living kidney donation (Garonzik-Wang et al. 2012). Despite the array of evidence that social network search dynamics are key determinants of precursor outcomes, very little is known about what determines to whom people turn in the early steps of the living kidney donor recruitment process. As described above, we know a little about role effects in this process, but much less about what explains them. To address this limitation, we next describe our treatment of social capital and tie strength theories as applied to living kidney donation.
Role Effects, Social Capital, and Tie Strength in Living Donor Kidney Transplantation
Although two thirds of living kidney donations are made by people in just four role relationships, it is unclear whether this pattern is evidence for role effects. Role effects for living kidney donation mean that individual members of some role relations are more likely to engage in living kidney donation as well as steps along the pathway to doing so (i.e., talking about donating, agreeing to be evaluated, being evaluated). Differences in group sizes might produce these differences (Daw 2022), but we focus on role effects that persist after such demographic expectations are accounted for and seek to document whether this is the case, then explain what accounts for these role effects. Our analyses focus on the contribution of factors emphasized by social capital theory (including situationally beneficial concentrations among certain role relations) and tie strength theory (including better social access to different types of role relations) or some combination of the two.
Network Member Resources
To contribute to one’s situationally dependent endowment of social capital, network members must possess situationally beneficial resources. Although some network member resources may be beneficial across a variety of situations, in other cases the most beneficial resources may be situation specific (Perry and Pescosolido 2010; Sandefur and Laumann 1998; Wellman and Wortley 1990). Most prior research on social capital and social support addresses social and economic resource exchange, such as the provision of financial or instrumental assistance, which are likely to be beneficial in a broad array of situations. In the health domain, most studies of social support focus on how people mobilize their networks for access to “health related cultural capital, including the ability to identify symptoms of illness, recognize a need for formal and informal support, and help secure access to health and social services” (Perry and Pescosolido 2015:117). However, in the medical support domain, nonbehavioral and noninformational health attributes can also function as health resources embedded in someone’s social network, and much less is known about how people access such benefits.
We particularly focus on what we call “biomedical resources,” which we define as the situationally beneficial health resources in one’s social network that arise from biomedical processes. Although, in principle, one may benefit from others’ biomedical resources that cannot be directly transferred (e.g., one benefits from others’ immunity to a disease in herd immunity), here we concern ourselves with biological products with directly transferable utility between individuals. Among biomedical resources, several key distinctions between biomedical resources may prove relevant for the social determinants of exchange. First, some biomedical resources (e.g., blood, sperm, bone marrow, livers) can be regenerated, whereas others (e.g., eggs, kidneys) cannot. Second, donating some biomedical resources (e.g., blood, sperm, eggs) involves essentially no risk or medical recovery period, whereas donating others (e.g., bone marrow, livers, kidneys) does involve small risks and moderate medical recovery periods. Third, some biomedical resources (e.g., kidneys, livers) are exchanged between individuals connected directly, whereas others (e.g., blood, plasma, bone marrow) are often exchanged through brokers. We expect that regeneratable biomedical resources, those with low donation risk and medical recovery periods, and those exchanged through a broker will not depend as strongly on tie strength as nonregeneratable resources, those with small donation risk and moderate medical recovery periods, or those exchanged through directly connected individuals.
Finally, it is noteworthy that with technological and cultural development, the set of biological materials with directly transferable utility has shifted dramatically over time. For instance, the major human blood groups were not identified until 1901 (Landsteiner 1901), and Rh groups were not identified for 40 more years (Landsteiner and Wiener 1941). Prior to these discoveries, blood did not have a directly transferable and reliable medical benefit without risking severe health consequences. The same is true of kidneys; the first successful kidney transplantation did not occur until 1954, when a kidney was transplanted between monozygotic twins after previous failures between non–genetically identical pairs, which led to discovering the laws of tissue compatibility and the development of effective immunosuppression (Tilney 2003). As a result of these discoveries, transferable biomedical resources have become an increasingly important component of contemporary medicine and are likely to continue to grow in prominence, and as such are worth examining in the context of health-related help seeking.
Application to Living Donor Kidney Transplantation
With respect to living donor kidney transplantation, biomedical resources describe the likelihood that members of patients’ networks are sufficiently healthy and genetically well matched to the patient and that they are medically able to donate with minimal risk for harm to the donor or recipient. Living kidney donation evaluation is a form of “biological, psychological, and sociological . . . gatekeeping” (Fox and Swazey 1974:5) through which medical professionals evaluate potential donors to minimize risks to donors and recipients. Potential donors are screened for medical conditions (known as contraindications for donation) that would raise the risk of donation for the donor (e.g., hypertension, diabetes, kidney disease) or the recipient (e.g., cancer or serious infectious diseases). Psychological screening ensures that the donor is free from pressure and able to meaningfully consent. The type of sociological gatekeeping that Fox and Swazey (1974) described is largely a relic of a past era when doctors would more often dictate rather than collaborate with patients in care decision making, as is more the norm today (e.g., Timmermans 2020). 6
Blood (blood types A, B, and O or AB coded in the ABO gene) and tissue (human leukocyte antigen, coded principally in the HLA-A, HLA-B, and HLA-DR genes) compatibility of the donor-recipient pair is another aspect of biological gatekeeping. Although transplantation can result from incompatible donors through therapeutic and organizational innovations in many cases, living kidney donation is far simpler to arrange between donor-recipient pairs with compatible blood and tissue types. Compatibility likelihood is positively related to the donor-recipient genetic relationship 7 and negatively related to the genetic diversity of the population (Kanter and Hodge 1990). Thus, all else equal, transplantation patients’ biologically related parents, children, and siblings will have greater biomedical resources than more distant relations, nonbiological relatives, friends, or other acquaintances with respect to blood and tissue matching. However, role groups do not perfectly correspond to genetic relationships, as many role groups include a mixture of genetically related and non–genetically related pairs, such as the distinction between biological and adoptive siblings, or between aunts or uncles by blood and marriage (see Appendix Table D2). Nonetheless, all else equal, patients with many living biological children, full siblings, and parents will have greater situationally relevant social capital because they have more high probability opportunities for compatible donors.
Potential donors with contraindications for donation or who are less genetically related to the recipient may anticipate medical gatekeeping. To the extent that patients and potential donors are aware of these gatekeeping factors, they would be expected to suppress the likelihood of engaging in steps leading to donation (e.g., discussing donation, agreeing to donate, being evaluated for donation). Therefore, the biomedical mediation hypothesis is that role effects will be substantially attenuated by role groups’ health and genetic relationships with the patient.
Tie Strength
Network members to whom a person has greater tie strength may be more likely to provide situationally relevant resources in times of need. Efforts in the 1980s to understand representative features of American social networks demonstrated that individuals typically have a discussion “core” consisting of close friends and family members to whom they turn to discuss important matters (Fischer 1982; Marsden 1987; McPherson et al. 2006; Small 2017). Communication frequency proxies the persistent ties that comprise core discussion networks (Verdery et al. 2018), while emotional closeness seeks to measure “the depth of the relationship” (Marsden and Campbell 1984). Spatial proximity between social ties also enhances the potential for social support in multiple ways, including as a predictor of tie strength (Marsden and Campbell 1984) and interaction frequency (Butts 2002; Latané et al. 1995). In classic social support models, proximity is a key discriminant between service provision (which must occur in person) and other support dimensions because people “are able to provide some forms of companionship, emotional aid, and financial aid over large distances” (Wellman and Wortley 1990:569). However, empirical evidence suggests that proximity is also important for dimensions of support that do not require in-person interactions (Hogan, Eggebeen, and Clogg 1993; Sarkisian and Gerstel 2004). Spatial proximity also varies systematically by role relationship. For instance, parent/child and sibling pairs are much more likely to coreside, live in the same census tract or county, or live in tracts that are closer together, than more distant kin (Daw, Verdery, and Patterson 2019; Verdery et al. 2012).
Application to Living Donor Kidney Transplantation
Tie strength considerations offer mixed predictions. On the one hand, it is natural to expect that living donor kidney transplantation is predicated on strong ties, with more frequent communication, the potential donor is almost certainly more likely to know of the potential recipient’s health condition and more likely to understand what he or she needs. But, at least for emotional support, there are competing perspectives that emphasize the avoidance of strong ties. Small’s (2017) argument that close relationships are often avoided during the search for social support has a corresponding concern in the sociology of kidney transplantation. In Mauss’s (2000) classic treatment, the expectation of symmetrical gift exchange is the foundation of the gift-giving relationship, and failure to symmetrically reciprocate causes considerable social strain. Fox and Swazey (1974) introduced the concept of the “the tyranny of the gift,” writing, what recipients believe they owe to donors and the sense of obligation they feel about repaying “their” donor . . . weigh[s] heavily on them. This psychological and moral burden is especially onerous because the gift the recipient has received from the donor is so extraordinary that it is inherently unreciprocal. . . . As a consequence, the giver, the receiver, and their families may find themselves locked in a creditor-debtor vise that binds them to one another in a mutually fettering way (Fox and Swazey 1992: 40).
In this way, transplantation patients may be loath to imperil their closest relations by incurring an unpayable debt, leading them to turn elsewhere for assistance. Indeed, groundbreaking work by Simmons, Marine, and Simmons (1987) revealed that 60 percent of living donor kidney transplant recipients in their study experienced guilt about taking a kidney from a relative before the transplantation, and 20 percent felt guilty about their inability to repay their donors afterward (p. 172). Because their sample consisted of living donor kidney transplant recipients (and not those who did not obtain one), these statistics may understate the extent of the issue.
Pair-level spatial proximity is also a strong determinant of living kidney donation behaviors, for several reasons. Pairs that reside near one another are more likely to engage in a variety of forms of instrumental assistance and caregiving, which prior research on living kidney donation has shown is a key social determinant of living kidney donation behaviors (Gillespie et al. 2020). Practically, although living kidney donor medical evaluations can sometimes take place elsewhere, those who live nearby one another will be able to coordinate potential donor evaluations and donation more easily and with less travel required.
The tie strength mediation hypothesis holds that relational characteristics such as communication frequency, perceived intimacy of the relationship, and spatial proximity are key mediators of role effects on living donation behaviors. As such, we expect that role groups that typically have close social relationships will be advantaged by these relationships compared with role groups that typically have weaker social relationships, and that tie strength will positively mediate (i.e., attenuate) both role group sets’ role effects.
Data, Methods, and Analysis 8
Data
We test these hypotheses in two distinct data sets, one reported from the perspective of transplantation patients and the other reported from the perspective of kidney disease patients’ family members. Because living kidney donation is a dyadic, relational process, it is important to gather information reflecting both potential donors’ and patients’ perspectives in order to ascertain possible misalignment in their perceptions (e.g., a patient misappraising a potential donor’s health, or the two not agreeing on their relationship quality). As such, we use data from both perspectives. As will be described, there are many differences between these data sets. For this reason, we focus our interpretations on the shared insights we can gain from both studies. This approach has the benefit of conceptual replication, testing the same hypotheses in two separately collected data sets with similar measures fielded in different target populations, which is a high standard of evidence (Hüffmeier, Mazei, and Schultze 2016).
Transplantation Patient Reports: Ego Networks among Candidates for Transplant
Overview
We first measured living kidney donation processes from the patient’s perspective. Between May and December 2015, our research team conducted the Ego Networks among Candidates for Transplant (ENaCT) study, which is a sample of 73 kidney transplantation patients at a single, large transplantation center in the southeastern United States. Participants were recruited following a kidney transplantation educational session that was part of their initial evaluation to be placed on the waiting list. We gave each transplantation patient a survey (the “patient survey”) that asked them to report their own demographic traits, medical history, and transplantation-related knowledge and attitudes. Second, we gave each patient an ego network survey, wherein each transplantation patient responded to (1) a name generator asking for the names or initials of living network members age 20 or older who were members of a defined set of role groups (parents, children, siblings, spouses, grandparents, grandchildren, aunts or uncles, nieces or nephews, cousins, other family, and friends) and (2) a name interpreter containing a series of nine questions about each nominated network member’s demographic characteristics, health, social and genetic relationship with the respondent, and transplantation-related attributes. The data collection instruments we used were developed after conducting in-clinic, formative research in this population to elicit complete networks of relatives and very close friends. To elicit close friends, we used a modification of the General Social Survey’s “important matters” name generator (Burt 1987), which is commonly used in networks research; the only modification of note being that we asked the “important matters” generator last and asked respondents to limit their responses to alters not already nominated in the preceding kinship rosters. An abridged version of this data collection instrument is found in Appendix E.
The 73 ENaCT respondents reported on a total of 1,611 members of their network. This sample was restricted to those with appropriate relationship types (see Appendix A) and those with complete data on all analyzed variables, resulting in an analytical sample of 70 transplantation patients reporting on themselves and 1,421 network members (averaging 20.3 per patient). Both surveys were self-administered under the supervision of a member of the research team unless respondents requested help taking the survey, in which case a companion or research team member was allowed to assist them. Hereafter, we refer to the respondents to this survey as “patients” and their network members as “alters.” Additional details on this data set are available in Appendix A.
As it is restricted to a convenience sample of transplantation patients at a single center, ENaCT is not intended to be interpreted as a representative data set of all transplantation candidates. However, the richness of the data collected on patients’ social networks and transplantation-related processes is unparalleled in any other existing data set.
Patient Survey Variables
We use four demographic variables from ENaCT’s patient survey in this analysis. Patient race/ethnicity measures self-reported responses to a Hispanic ethnicity question and a race question, using the 2010 census approach. These values were recoded as non-Hispanic White, non-Hispanic Black, and Hispanic of any race, as no other categories were marked. We also measure patient age (≤50 vs. ≥51 years), patient sex (male vs. female), and patient education (less than a high school diploma, high school diploma or equivalent, some college but no four-year degree, and four-year college degree or higher).
Network Member Dependent Variables
We use two dependent variables from ENaCT: whether the pair had a LDD (1 = they had a discussion, 0 = they did not), and whether the pair agreed to pursue donation (1 = yes, 0 = no or “don’t know”).
Network Member Independent Variables
We also use ENaCT’s ego network data to measure a number of key independent variables. Role group is our focal independent variable, measured in the following categories: friend, spouse or partner, sibling, parent, child, cousin, aunt or uncle, niece or nephew, or other family. Because relatively few reported network members were grandparents or grandchildren, we merged these role categories with the other family category. We control for network member age (ages 20–30, 31–50, 51–70, and ≥71 years) and network member gender (male or female).
Mediating Variables
Our key hypotheses concern the extent to which biomedical resources and tie strength mediate the role effects we expect to see. We measure the donation-relevant biomedical resources of each network member through two items: whether the patient believes the network member is healthy enough to donate (1 = yes, 0 = no or “don’t know”), and whether the network member is a blood relative (e.g., distinguishing an aunt by marriage from an aunt by common ancestry; we do not ask this question of spouses and partners or friends). We combine the latter variable with the role group to assign an approximate genetic relationship (i.e., kinship coefficient; Wright 1922) between the network member and transplantation patient, as follows: (1) all nonblood relatives are assigned a genetic relationship of 0; (2) parents, children, and siblings who are blood relatives are assigned a genetic relationship of 0.5; (3) aunts or uncles, grandparents, grandchildren, and nieces or nephews who are blood relatives are assigned a genetic relationship of 0.25; (4) cousins who are blood relatives are assigned a genetic relationship of 0.125; and (5) other family who are blood relatives are assigned a genetic relationship of 0.0625. 9 Finally, we measure tie strength on the basis of a measure of communication frequency, (distinguishing those who communicate “once a week or more” [reference category] from each category who communicate less often) 10 and emotional closeness (distinguishing “extremely close” [reference category] alters from those who are “very,” “somewhat,” or “not very” close). Though theoretically relevant, the time-limited, in-clinic nature of data collection for ENaCT precluded us from asking about geographic proximity to kin, a tie strength factor we consider in the second survey we fielded.
Realistic Donor Reports: Families of Renal Patients Survey
Overview
In a second study, we sought to obtain information about living kidney donation from the perspective of potential donors. We fielded two rounds of surveys through the Qualtrics Online Panel (in April and May 2019 and August and September 2019) that included a screener question for inclusion in our sample, asking if potential respondents had a relative with “weak or failing kidneys.” These two rounds of original data collection provided a sample of realistic potential living kidney donors, a population heretofore only studied conditional on completing in-clinic donation behaviors. For those respondents who met the survey screening criteria, the surveys instructed them to indicate their relationship to this person and consider this person for the duration of the survey; we asked respondents with more than one such relative to choose one. In total, 2,072 respondents participated in the two rounds of the Families of Renal Patients Survey (FoRPS), 1,469 in wave 1 and 603 in wave 2; of these, we excluded 512 because of poor indicators of data quality for an analytical sample of n = 1,560 (970 in round 1, 590 in round 2; see Appendix B for details). In this analysis, we subset the data to respondents who report that the patient is seeking kidney transplantation (n = 765).
Respondents to this survey answered a series of items relating to their own and the sick relative’s characteristics, living donor kidney transplantation–related behaviors and attitudes, living donor kidney transplantation–related policy preferences, and the role linking the respondent and the relative. Survey content differed slightly between waves, as described below. We use poststratification weights to match survey-reported patient demographic characteristics (i.e., the attributes of the sick relative) to the demographic profile of transplantation patients in the U.S. Renal Data System’s database. Finally, we subset all analyses of these data to respondents who report that their sick relative was seeking kidney transplantation. Appendix B includes full details on sample inclusion, data cleaning, relationship recode procedures, and weighting. Hereinafter, we refer to the survey respondents who are realistic potential living donors as “respondents” and their ill family members as “patients.”
Dependent Variables
We analyze three dependent variables in the FoRPS data, indicating respondent agreement with the following statements vis-à-vis the patient: “We have discussed me becoming a living kidney donor to this person” (LDD); “I have agreed to be medically evaluated as a potential living kidney donor to this person” (agree); and “I was medically evaluated as a potential living kidney donor to this person” (tested). 11
Independent Variables
The primary independent variable of interest is the role group linking the respondent and the kidney disease patient. The prompt was “The person you are thinking of is . . .,” and respondents chose from the following response options: “my spouse or a boyfriend/girlfriend or life partner who lives with me,” “my child,” “my parent,” “my sibling,” “my grandparent,” “my aunt/uncle,” “my niece/nephew,” “my cousin,” “my grandchild,” or “a different type of family member not already indicated (specify).” We reverse coded these ties to make them comparable with those constructed from the transplantation patient’s perspective in the ENaCT data set (so that, for instance, responses of “my child” are recoded to indicate that the respondent is the patient’s parent).
We measure respondent and patient demographic characteristics as follows: sex (1 = female, 0 = responses of male or other); 12 race/ethnicity (Caucasian or White, Hispanic or Latino/a, Black or African American, Asian or Pacific Islander, or other). 13 Note that we model each of these variables for both respondents and patients.
Mediating Variables
In the FoRPS data as in the ENaCT data, our focus is on the extent to which biomedical resources and tie strength mediate role effects. We use two items to capture respondents’ biomedical resources. First, we calculate approximate genetic relationship identically as in ENaCT. Second, we constructed a composite measure of whether the respondent was healthy enough to donate on the basis of a series of self-reported health conditions. These conditions were drawn using the list of contraindications employed by a transplantation clinic our research team collaborates with. This measure distinguishes between “absolute” and “relative” contraindications for donation by assigning respondents to unhealthy status if they have one or more absolute contraindications and/or two or more relative contraindications for donation. To measure absolute contraindications, respondents in FoRPS indicated whether they have ever been diagnosed with the following conditions (marking all that applied): HIV/AIDS, diabetes, melanoma, or a serious psychiatric condition or clinical depression. Using the same survey stem, we measured relative contraindications as untreated hypertension, cancers other than melanoma not currently in remission, kidney stones, reduced kidney function, a body mass index ≥35 kg/m2, or being younger than 30 years with a family history of polycystic kidney disease. Age > 70 years was also used as a relative contraindication. Because of a survey error, the measure of reduced kidney function (where the respondent indicated they had “weak or failing kidneys”) was omitted from the contraindication list in wave 1 of FoRPS, and in wave 2 we added more detailed measures of hypertension (asking whether the respondent had been told more than twice that they had hypertension, and whether their hypertension was being treated with medication). Accordingly, we multiply impute these three measures in wave 1 (see Appendix B for details), and all analyses of FoRPS data account for the multiply imputed nature of the data.
Finally, we assess respondent-patient tie strength through two indicators. The first, as with ENaCT, measures the communication frequency between the pair: “How often do you communicate with this person?” We compare each other category to “most days or every day.” Our second measure of relationship attributes is geographic proximity, which respondents report as travel time using their preferred mode of travel, ranging from 15 minutes or less to “more than 1 day of travel.” In this analysis, we operationalize this measure categorically, comparing each category to the “less than 15 minutes” reference category.
Analytical Strategy
The core goal of this analysis is to establish the association between potential donor roles and living kidney donor behaviors, and then examine how well biomedical resources and tie strength indicators explain these patterns. To address the latter goal, we use the Karlson, Holm, and Breen (2012) mediation model, which extends the classic Sobel (1982, 1986) mediation model to nonlinear dependent variables. Mediation models work by estimating models with (full model) and without (reduced model) the mediating variables. Comparing the focal coefficients for these two models, we calculate the percent mediated as
However, Karlson-Holm-Breen handles an additional issue introduced when estimating mediation in logistic regression models. Unlike in linear regression, adding independent variables to a logistic regression can change the original independent variables’ estimated coefficients even if the added variables have no association with the dependent variable (Mize, Doan, and Long 2019; Mood 2010). To account for this, Karlson-Holm-Breen includes residualized versions of the mediating variables in the reduced model specification to separate these nonlinear regression model rescaling effects from true mediation. For maximum interpretability and to facilitate cross-model comparisons in nested logistic regression models, we also report all regression coefficients as average marginal effects (AMEs), which express the difference in the predicted probability of the outcome associated with a unit change in the independent variable in question. Because many sociodemographic characteristics are likely to be related to both social network characteristics and social support behaviors, we use a demographically adjusted reduced model for all mediation analyses, where the reduced model is specified as role effects net of controls for patient (and, in FoRPS, respondent) age, sex, education, and race/ethnicity. In ENaCT, network member age and sex are also specified in the demographically adjusted reduced model.
Because role group is a nondichotomous categorical independent variable and because the findings may vary across role group, we characterize the percentage of the baseline effect eliminated by the introduction of these variables to the model for each role group separately vis-à-vis a reference category. Because of this approach, mediating variable groups that explain one role’s association with the dependent variable may not do so for another. 14 Finally, all regression models are estimated using robust standard errors to account for the nonindependent nature of the ENaCT data wherein each candidate reports about multiple potential donors. Note that we adopt this strategy rather than multilevel modeling to privilege the use of a consistent approach across the two data sets; in FoRPS each potential donor reports about only one candidate (thus precluding a multilevel modeling approach in those data).
Results
Sample Descriptions
ENaCT Sample Description
Table 1 describes the ENaCT data at the patient level. The sample is majority male (60 percent), majority non-Hispanic Black (61 percent) and non-Hispanic White (33 percent), and close to evenly divided between those younger (54 percent) and older than 50 (46 percent). Educational attainment was primarily in the middle categories, including high school or equivalent degree (33 percent) and some college but no college degree (39 percent).
Sample Description, Ego Networks among Candidates for Transplant Study (Sample of Transplantation Patients), Patient Level.

Note: HS = high school; SC = some college.
Table 2 describes the structure of ENaCT’s network data. A total of 1,433 ties (an average of 20.5 ties per patient) are included in the analytical sample. Reflecting typical kinship network structure, cousins (n = 336, mean = 4.8, 23 percent of all ties), siblings (n = 221, mean = 3.2, 15 percent), aunts or uncles (n = 216, mean = 3.1, 15 percent), friends (n = 190, mean = 2.7, 13 percent), and nieces or nephews (n = 187, mean = 2.7, 13 percent) were the most numerous reported role groups. Less numerous role groups included parents (n = 59, mean = 0.8, 4 percent), children (n = 88, mean = 1.3, 6 percent), spouses (n = 34, mean = 0.5, 2 percent), and other family (n = 102, mean = 1.5, 7 percent).
Sample Description, Ego Networks among Candidates for Transplant Study (Sample of Transplantation Patients), Pair Level.

Note: LDD = living donor discussion.
These role groups vary systematically in the proportion of ties with different living kidney donation-relevant characteristics. For example, although 18 percent of all ties had had a LDD with the patient, 56 percent of spouses had done so, followed by lower but substantial percentages of parents (32 percent), children (31 percent), and siblings (30 percent) and notably lower levels (6 percent to 18 percent) among aunts or uncles, nieces or nephews, cousins, other family, and friends. These role patterns of LDDs are magnified for patterns of agreement for evaluation.
Role groups differ considerably in their indicators of biomedical resources and tie strength. Patients rated 82 percent of nieces or nephews, 76 percent of children, 54 percent of cousins, 62 percent of spouses, and 59 percent of friends or other family as healthy enough to donate, while parents (24 percent) and aunts or uncles (18 percent) were thought to be healthy at much lower rates. Of the role groups frequently perceived to be healthy, children, siblings, and to a lesser extent nieces or nephews are also typically close genetic relatives, meaning these role groups’ biomedical resource endowment is well above average. Turning to tie strength, respondents report that they talk at least weekly with their spouses (100 percent), parents (93 percent), children (81 percent), friends (76 percent), and siblings (61 percent) at above-average rates, while they do so with members of other role groups considerably less often. Similar patterns are observed for relationship closeness. There are also age and gender patterns by role group that conform with what would be expected on the basis of the kin group definitions (e.g., parents are older) and gender differences in longevity and child contact.
FoRPS Sample Description
Table 3 provides weighted descriptive statistics on the demographic composition of the respondent and patient members of FoRPS, which offers a different perspective on potential donors’ characteristics and relationships with transplantation patients than we see in ENaCT. Respondent characteristics are reported on the left; characteristics of their family members with kidney disease are reported on the right. Because the sample is weighted to the U.S. end-stage kidney disease patient population’s characteristics, their distribution reflects the demographic selection processes leading to end-stage kidney disease, with male, Black, high school graduates or equivalent, and age ≥ 51 persons considerably overrepresented in the patient group and female, White, college graduates or more, and age ≤ 50 persons underrepresented in the patient group. 15 The distribution of these same characteristics among respondents is different, as female, college-educated, and age ≤ 50 respondents are overrepresented compared with the population and their patient counterparts, while Black race is overrepresented compared with the general population but comparable with that of their patient counterparts.
Families of Renal Patients Survey (Sample of Relatives of Transplantation Patients), Pair Descriptive Statistics.

Note: API = Asian or Pacific Islander; HS = high school; SC = some college.
Table 4 mirrors Table 2 in describing the distribution of role groups, living kidney donation behaviors, and indicators of biomedical resources and tie strength in FoRPS. Children (n = 190 [25 percent]) and spouses (n = 243 [32 percent]) are the most common respondent roles in these data, followed by a second tier of nieces or nephews (n = 85 [11 percent]) and siblings (n = 71 [9 percent]), with smaller representation of grandchildren (n = 54 [7 percent]), cousins (n = 45 [6 percent]), parents (n = 39 [5 percent]), and other family (n = 38 [5 percent]). As in ENaCT, these role groups show considerable variability in living kidney donor behaviors. Spouses, children, and siblings have above-average rates of LDDs; spouses, parents, and children have above-average rates of agreement; grandchildren, spouses, nieces or nephews, and parents show the highest proportions of prior testing. Notably, role differences in common indicators of living kidney donation behaviors are smaller in FoRPS than in ENaCT, perhaps reflecting the differential geographic scope or reporter effects across these two data sets. Of course, many other factors could also explain differences between the two data sets, including sampling variability, different time periods of data collection, processes like “the friendship paradox” (Feld 1981), or other factors – for these reasons we concentrate our interpretations on shared results.
Families of Renal Patients Survey (Sample of Relatives of Transplantation Patients) Patient and Donor Characteristics.

Note: LDD = living donor discussion.
As in ENaCT, role groups in FoRPS differ in the distribution of biomedical resources and tie strength. Relatives in younger kin groups (nieces or nephews, children, and grandchildren) rarely report medical conditions that would disqualify donation. As before, genetic proximity boosts parent and sibling donation capacity. Tie strength is concentrated among spouses, children, and siblings owing to their closer geographic proximity and more frequent contact between such kin types.
Role Effects and Mediation Analyses
Evidence from ENaCT
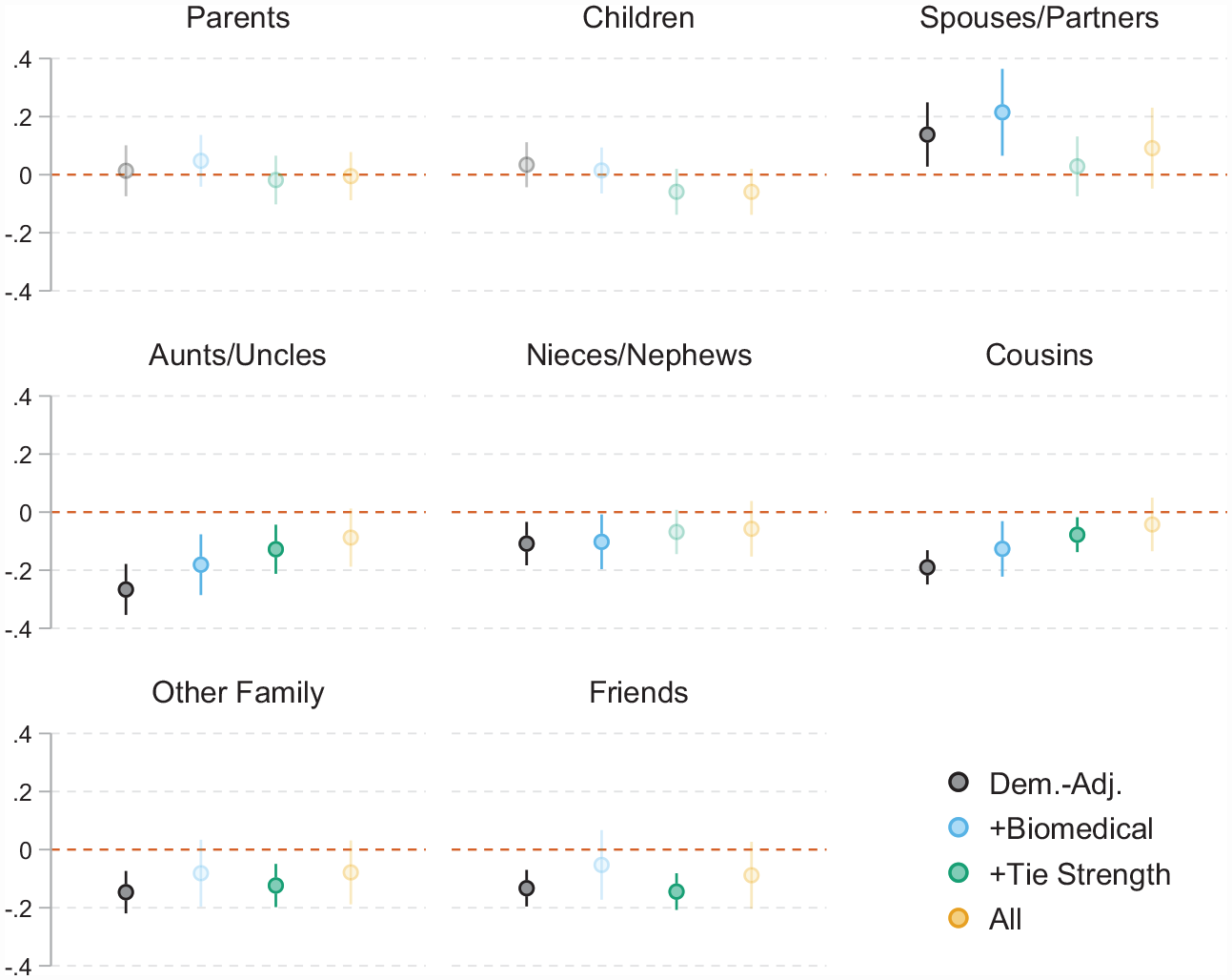
Figure 1 presents the associations of eight role groups with LDDs in ENaCT, using siblings as the reference category. Results are presented as AMEs on the y-axis, shown for four model specifications for each role: adjusted for candidate demographic characteristics only, adjusted for demographic characteristics and biomedical resources, adjusted for demographic characteristics and tie strength indicators, and adjusted for all covariates. Therefore, the gap between the markers for each role group indicates the degree to which role effects are accounted for by biomedical resources and tie strength indicators, with the more formal mediation analysis found in Table 5, and fully detailed mediation analysis results in Appendix C. As a supplemental analysis, Appendix C also shows equivalent results for which network members agreed to be evaluated for living donation conditional on having an LDD. These results are presented in the appendix in the interest of brevity and because the results are imprecise because of small cell sizes.
Average marginal effects with and without all controls (Ego Networks among Candidates for Transplant sample of transplantation patients).
Mediation Analyses of Role Effects (Ego Networks among Candidates for Transplant Sample of Transplantation Patients).

Note: AME = average marginal effect; CI = confidence interval; LDD = living donor discussion.
LDD Role Effects and Their Mediation
Under all specifications, parents, children, and siblings have very similar demographically adjusted probabilities of having an LDD with the candidate. The differences that are observed between these groups are substantively small and statistically insignificant in all model specifications. Parents (AME = 0.03, 95% confidence interval (CI) = −0.06 to 0.12) and children (AME = 0.02, 95% CI = −0.06 to 0.10) have slightly higher demographically adjusted probabilities of LDDs than siblings (see blue markers in Figure 1 and “Role Effect” columns in Table 5). For parents, this small effect is best explained by tie strength in the mediation model (reduced model AME [AMEred] = 0.05, full model AME [AMEfull] = −0.02, 136 percent mediated), as parents’ role effect is suppressed by biomedical resources (AMEred = 0.01, AMEfull = 0.05, −256 percent mediated). Together, the conjunction of biomedical resources and tie strength mediates parents’ role effect on LDDs almost perfectly (AMEred = 0.04, AMEfull = −0.01, 99 percent mediated). In contrast, children’s role effect is best explained by biomedical resources (AMEred = 0.03, AMEfull = 0.01, 58 percent mediated), while it is suppressed in the tie strength model (AMEred = 0.01, AMEfull = −0.06, 1,266 percent mediated) and in the full model (AMEred = 0.01, AMEfull = −0.06, 628 percent mediated). In short, parents, children, and siblings have similar probabilities of LDDs, but the small, statistically insignificant parental advantage over siblings is best explained by tie strength (and is suppressed by biomedical resources), and the small child advantage over siblings is best explained by biomedical resources (and is suppressed by tie strength).
Spouses and partners’ LDD probabilities differ from parents’, children’s, and siblings’ in some model specifications. In demographically adjusted models, spouses and partners are substantively and statistically significantly more likely to have LDDs than siblings (AME = 0.14, 95% CI = 0.03–0.25). Moreover, this already large effect is suppressed by biomedical resources (AMEred = 0.14, AMEfull = 0.21, −55 percent mediated). In contrast, tie strength substantially mediates this role effect (AMEred = 0.14, AMEfull = 0.03, 79 percent mediated). Accounting for both biomedical resources and tie strength, moderately mediates this role effect (AMEred = 0.014, AMEfull = 0.09, 34 percent mediated). In short, spouses and partners are much more likely to have an LDD than siblings, and this difference is best explained by tie strength (and is suppressed by biomedical resources).
Extended kin are much less likely than nuclear family members to have an LDD with the transplantation candidate in demographically adjusted models. Aunts or uncles (AME = −0.26, 95% CI = −0.34 to −0.17), cousins (AME = −0.19, 95% CI = −0.25 to −0.13), nieces or nephews (AME = −0.12, 95% CI = −0.20 to −0.05), and other family (AME = −0.15, 95% CI = −0.23 to −0.08) all have substantively and statistically significantly lower probabilities of an LDD than siblings. For all four roles, biomedical resources partially mediate these role effects (aunt or uncle AMEred = −0.27, AMEfull = −0.18, 32 percent mediated; niece or nephew AMEred = −0.11, AMEfull = −0.10, 6 percent mediated; cousin AMEred = −0.19, AMEfull = −0.13, 34 percent mediated; other family AMEred = −0.15, AMEfull = −0.08, 45 percent mediated), as does tie strength (aunt or uncle AMEred = −0.24, AMEfull = −0.13, 46 percent mediated; niece or nephew AMEred = −0.14, AMEfull = −0.07, 50 percent mediated; cousin AMEred = −0.18, AMEfull = −0.08, 57 percent mediated; other family AMEred = −0.15, AMEfull = −0.12, 20 percent mediated). For all aunts or uncles and cousins, the role effect remains statistically significant in the demographically adjusted, biomedical resources, and tie strength model specifications; for nieces or nephews and other family, it is not statistically significant in the tie strength model specification. For all four of these relationships, specifying both biomedical resources and tie strength results in greater mediation and smaller estimated role effects than either alone, and all four role effects are substantively moderate and statistically insignificant in these models. In short, extended kin are much less likely to have LDDs than siblings, and for all kin types except other family, this is better explained by tie strength than by biomedical resources, although both contribute to the role effects.
Friends are much less likely to have LDDs than siblings, and biomedical resources explain this better than tie strength. Friends are much less likely to have an LDD than siblings in demographically adjusted models (AME = −0.14, 95% CI = −0.20 to −0.07). This difference is better explained by biomedical resources (AMEred = −0.13, AMEfull = −0.05, 60 percent mediated) than by tie strength, which slightly suppresses the friendship role effect (AMEred = −0.13, AMEfull = −0.14, −11 percent mediated). Both mediating variable groups together moderately mediate the friendship role effect (AMEred = −0.13, AMEfull = −0.09, 32 percent mediated). In sum, friends’ lower probability of LDD than siblings’ is primarily attributable to biomedical resources.
Supplemental Analyses and Robustness Checks
Analyzing agreement to evaluation is more difficult because the sample is necessarily subset to those who had had an LDD, leading to small cell size issues (see Appendix Table D1). Nonetheless, the role effects and mediation patterns in this analysis may be informative. The bottom half of Appendix Table C1 replicates the demographically adjusted role effects on LDDs: parents, children, and spouses and partners are more likely than siblings to agree to evaluation if they had an LDD (a statistically significant difference for spouses and partners), while extended kin and friends are less likely than siblings to do so. Patterns of mediation, however, differ somewhat from LDDs. Agreement biomedical resource mediation aligns directionally (positive vs. negative) with LDD results for parents, children, and aunts or uncles, but reverses for all other role groups. Tie strength mediation is more consistent for agreement, aligning directionally with LDD mediation in all eight comparisons. Similarly, although all relationship groups were positively mediated in the full model accounting for both biomedical resources and tie strength for LDD, this is true for only five of eight relationship groups in agreement (with nieces or nephews, other family, and friends’ role effects negatively mediated, although the percentages are small for nieces or nephews and other family).
Another set of robustness checks evaluate the potential for collinearity bias due to the association of genetic relationship and role group. Table D2 shows there is reasonable within-group variation in this measure, and Table D3 shows that variance inflation factors for each variable in the fully specified models are considerably lower than 10 (a common cutoff for collinearity checks). As an additional check on whether collinearity between role relation and genetic relationship skews the study’s findings, we also estimated biomedical resource and tie strength/biomedical resource mediation models without including genetic relationship as a mediating variable. The results of this exercise (Table D4) are similar for the “both” mediation models, but differ somewhat for the biomedical resource mediation analysis, particularly for more distantly genetically related role groups.
Two additional regression models were estimated as further robustness checks. Table D5 assesses whether a conditional logit model predicting LDDs using within-candidate variation yields statistically significantly different results from the primary model above on the basis of comparing each conditional logit role effect AME with the corresponding AME in a logistic regression using a Wald test. Of 40 comparisons so estimated (for eight role effects in five model specifications), only two role effects differed statistically significantly between the logistic regression and conditional logit analyses. This is the same number of differences we would expect at random in 40 hypothesis tests with α = .05. Furthermore, these significant differences occurred in unadjusted models, which we do not use in our primary analyses. Accordingly, we conclude that within-patient unobserved heterogeneity is unlikely to be systematically biasing our estimates in the ENaCT data. Table D6 provides mediation analysis results for LDDs using binary multilevel models with random intercepts rather than robust standard errors to account for the nonindependence of alter observations in the ENaCT data. The results are virtually identical to the primary analysis results.
Evidence from FoRPS
LDD Role Effects and Their Mediation
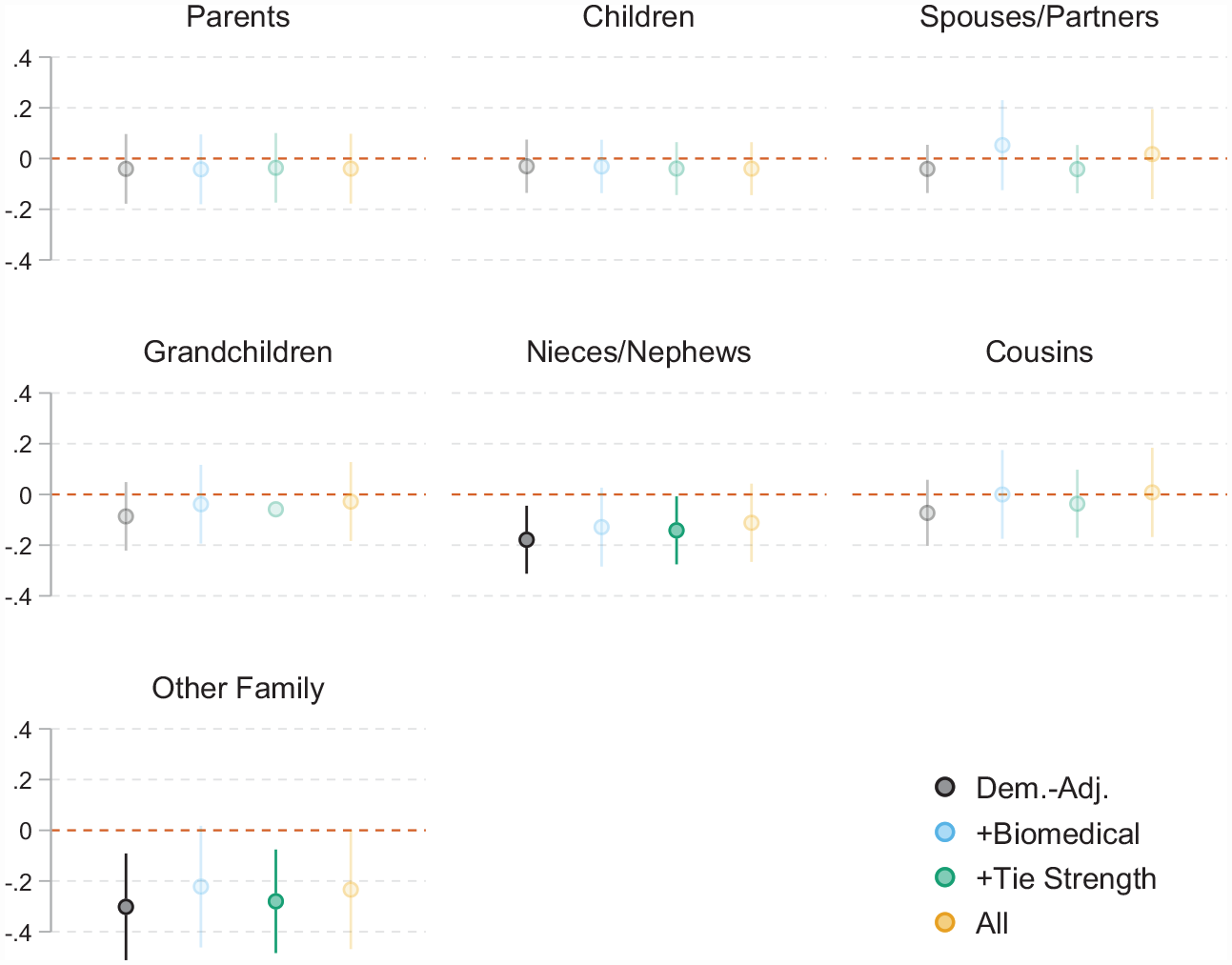
Are these patterns reproduced when realistic potential donors are reporting on themselves instead of transplantation patients reporting on their network members? Figure 2 and Table 6 depict parallel analyses in FoRPS, albeit with a slightly different set of role groups included in the analysis. Furthermore, we also compare role effects on being tested for living kidney donation in the supplement.
Average marginal effects with and without all controls (Families of Renal Patients Survey sample of relatives of transplantation patients).
Mediation Analyses of Role Effects (Families of Renal Patients Survey Sample of Relatives of Transplantation Patients).

Note: AME = average marginal effect; CI = confidence interval; LDD = living donor discussion.
Generally, demographically adjusted role effects on LDDs are weaker in this data set compared with ENaCT. The only statistically significant demographically adjusted role effects are for nieces or nephews (AME = −0.18, 95% CI = −0.31 to −0.04) and other family (AME = −0.29, 95% CI = −0.50 to −0.08) compared with siblings in LDD. Although other demographically adjusted role effects are not statistically significant in these analyses, the pattern of AMEs across roles is consistent with those documented in ENaCT, as nonnuclear kin uniformly have lower predicted probabilities of LDD than siblings and other nuclear family members. However, the FoRPS results differ from ENaCT’s in that siblings have the highest probability of LDD, and cousins have probabilities of LDD much more similar to siblings’ than what was observed in ENaCT.
As in ENaCT, mediation analyses of LDD in FoRPS show evidence in favor of both the biomedical resource and tie strength mediation hypotheses. Which group of mediating variables best explain demographically adjusted role effects varies by role group. Parents and children show essentially no evidence of biomedical resource mediation (−5 percent and −3 percent mediated, respectively), but moderate tie strength mediation (30 percent and 10 percent mediated, respectively). Spousal role effects, in contrast, show evidence of biomedical resource mediation (230 percent mediated) but none for tie strength mediation (−1 percent mediated). All extended kin show support for both hypotheses, with nontrivial mediation due to biomedical resources (55 percent mediated for aunts or uncles, 28 percent for nieces or nephews, 100 percent for cousins, 26 percent for other family) and tie strength (41 percent mediated for aunts or uncles, 28 percent for nieces or nephews, 65 percent for cousins, and 9 percent for other family). Finally, all relationship groups showed evidence of substantial mediation when both biomedical resources and tie strength mediating variables were specified in the model.
Supplementary Analyses
We also fit these models to two additional outcome variables: agreement to be evaluated and having completed testing for potential living donation (see Appendix Table C2). Each of these are modeled conditionally on having had an LDD, and accordingly role group cell sizes are once more limited and estimates correspondingly imprecise (see Table 4). However, some useful information can be gleaned from these results. First, these results suggest that role effects on post-LDD outcomes may differ substantially from role effects on LDDs. For agreement outcomes, although children are in the top tier of LDD probabilities, they are substantially less likely than siblings to agree to evaluation in demographically adjusted models (AME = −0.19). Similarly, parents were slightly less likely than siblings to have an LDD but are somewhat more likely to agree to evaluation conditional on having an LDD (AME = 0.09). A similar pattern is observed for other family (AME = −0.29 for LDD but AME = 0.10 for agreed conditional on LDD). Furthermore, role effect estimates are considerably different for reporting actual testing for evaluation conditional on an LDD. For testing, siblings and children are substantially less likely than all other groups to report completing testing for living donation in demographically adjusted models, with AMEs for this model ranging from 0.23 for spouses and partners to 0.58 for other family compared with siblings.
Mediation patterns for agreement and testing are similar for biomedical resources mediation but not for tie strength mediation. As with LDD outcomes, spouse/partner, aunt or uncle, and niece or nephew agreement and testing outcomes are substantially mediated by biomedical resource measures. The same is observed for cousins for agreement, but testing results could not be estimated for this group because of collinearity. Parents’ agreement role effects are moderately positively mediated by biomedical resources, unlike in LDD outcomes. For these two outcomes, however, there is little correspondence between the tie strength mediation results for LDD, agreement, and testing. This may be due to the very high imprecision of the demographically adjusted estimates in this model. Similarly, there is little correspondence between the mediation results in the fully specified model for agreed and the same results for LDD, but testing mediation bears some resemblance to the LDD results for spouses/partners and extended kin, while parent and child role effects are not substantially mediated in this model (unlike in LDD).
Because our FoRPS contraindication measure was multiply imputed (because of the addition of key items to wave 2 that were not present in wave 1), as a robustness check, we reestimated this analysis with the imputed measures omitted. As shown in Table D7, no mediation analysis results are nontrivially affected.
Discussion
Explaining Role Effects on Living Kidney Donor Precursor Behaviors
Motivated by recent work on to whom people turn in times of need, we examine what might explain role effects in help seeking behaviors during a medical crisis. Building from social capital theory and strong tie theory, we hypothesized two factors would be critical components in explaining role effects on living kidney donation discussions: biomedical resources and tie strength. Both data sets provide evidence in favor of both biomedical and tie strength mediation of role effects on LDDs. However, there is stronger support for biomedical resources mediation in FoRPS (from realistic donors’ point of view) than in ENaCT (from patients’ point of view). In contrast, tie strength mediation is better supported in ENaCT than in FoRPS. Finally, there is evidence that the direction, size, and mediation patterns on role effects may differ across stages of the living kidney donation process (from LDD to agreement to actual testing), but data with larger sample sizes should be collected to confirm these findings.
Several interpretations of these findings are possible. First, these data sets are collected through different approaches: ENaCT from a single-center population of transplantation patients and FoRPS from an online U.S.-based survey screening for relatives with kidney disease. It may be that ENaCT’s conclusions are geographically bounded, or restricted to more pressing cases where a transplant is being actively pursued. Second, it may be that more detailed, accurately reported medical data from realistic donors may more robustly contribute to role effects on living kidney donation behaviors than patients’ indirect reports on network members’ health. A third possibility is that the potential donors’ self-assessments are reasonably accurate and comparable, and that transplantation patients actually systematically underrate the willingness of many network members who are not nuclear family members to be living donors. A fourth is that issues such as the “friendship paradox” (Feld 1981) may generate an illusion of support when examining the perspective of network members reporting on a sick relative that might differ when examining only one patient’s perspective about their access. Given the many differences between these two surveys, it is difficult to parse the relative importance of these explanations. Future research should investigate whether directly linked patient and network member reports of willingness to donate are positively correlated and which is the better predictor of concrete living donation behaviors.
Lessons for Help Seeking I: The Importance of the Ask
One critical lesson of this investigation for theories of help seeking behavior may be that who you ask may depend on what the ask is. We hypothesize that the more socially significant and more intimate the support sought, the more closely help-seeking behaviors will hew to one’s core discussion and intimate family network.
Previous research supports this hypothesis. In Small (2017), the ask is typically the opportunity to get something off one’s chest, that is, someone to talk to. Perhaps given that relatively modest ask, it is unsurprising that the tie strength barrier is low, and a wide network of ties may be activated for support. Somewhat more involved social support types such as one-time instrumental support (e.g., moving assistance, baby, pet, or plant sitting) and modest financial assistance shows similar but less profligate patterns: family and close friends predominate (Verdery and Campbell 2019), but more tangential or disposable ties may be found in these networks as well (Desmond 2012).
For heavier asks, however, it seems that nuclear family and very close friends heavily predominate. For instance, in the more involved asks studied by Perry and Pescosolido (2010, 2015:125), which entailed discussing health-related issues during serious mental health crises, people tended to turn to strong ties “characterized by frequent verbal and face-to-face contact,” who were often members of socially significant role groups such as mothers and partners. This pattern also exists for caregiving during extended illness (Wolff and Kasper 2006), dealing with logistical challenges after a child’s death (Gage-Bouchard et al. 2015), financial assistance (O’Brien 2012), and living kidney donation.
In short, when the stakes are high and the assistance is intimate, we tend to look homeward.
Lessons for Help Seeking II: Situation-Specific Network Member Resources
Network member resources vary in their flexibility. Money, knowledge, social connections, and institutional efficacy are all flexible resources that confer advantages to those who possess them across a wide range of contexts. This is the core principle of fundamental cause theory: that the stratified distribution of these flexible resources is responsible for the enduring association between social position and health, because as novel situations, technologies, and information arise, those who possess greater endowments of these flexible resources are better positioned to capitalize upon them to benefit their health (Link and Phelan 1995). The same principle may apply to theories of help seeking behavior: connections to those with a greater endowment of flexible resources will confer advantages across a wide variety of domains, resulting in more general mechanisms of health advantage.
However, money cannot legally buy you a kidney in most of the world. Sometimes, even the most useful, flexible resources are no replacement for the specific resources that are most needed in particular situations, such as when you have end-stage kidney disease and are seeking living donor kidney transplantation. 16 In this context, the most critical resource is very specific: a healthy, well-matched kidney. Our findings suggest that the likelihood of meeting these criteria significantly shape alters’ inclination to engage in living kidney donation precursor behaviors.
Lessons for Help Seeking III: Roles, Resources, and Relationships
Our results also suggest a more general point. Cohen and Syme (1985:11) distinguished between structural and functional conceptualizations of social support, where “structural measures describe the existence of and interconnections between social ties [and functional] measures assess whether interpersonal relationships serve particular functions.” These distinctions remain to this day, with the structural conceptualization more closely aligning with social capital and tie strength theories and the functional conceptualizations more closely aligning with role relationship theories. Surprisingly in our view, prior work has not assessed how different these perspectives really are. Our results suggest deep symmetry between them: role relationships that strong ties can provide situationally beneficial resources, and strong ties that can provide situationally beneficial resources overwhelmingly concentrate among certain role relationships. Across both data sets, an enormous amount of the role effects we observe are mediated by the small number of variables we examine.
This result has both theoretical and methodological takeaways. On the theoretical side, it suggests that role theory may be underprivileging on-the-ground truths (the clustering of resources within, and tie strength governing access to, certain role relationships) with its heavy focus on norms, expectations, and obligations. Our results indicate there may be considerably less room for these functional considerations to drive who people turn to and that much of the action lies in the structural properties of the tie. Although norms, expectations, and obligations are clear determinants of why people communicate and spend time with, feel close to, and live near one another, we still find that resources are a clear determinant of to whom we turn in times of need. Methodologically, these results suggest that the social networks and health literature would benefit from greater attention to collecting data on people’s role relations (Chapman, Verdery, and Moody 2022 also highlighted this). So much of this literature focuses on measuring network ties that people are actively engaged with, such as convoys of support providers or those elicited through name generators surrounding who people spend time with or talk to, and it is rare that there is a systematic effort to collect data on role relations (e.g., few name generators ask respondents to enumerate extended family, neighbors, or coworkers of significance). An alternate strategy, position generators (Lin, Fu, and Hsung 2017; Lin et al. 2001), focuses on collecting data on ties to people with specific roles, but is used much less frequently, especially in health research. The results presented here suggest both efforts are worthwhile and that future work should more carefully consider the extent to which they provide complementary or redundant information on health-related help seeking.
Conclusion
Role effects on social support are ubiquitously documented when people turn to their networks during times of need, as social support activation rarely occurs at random. However, this important process is understudied in medical support seeking. We develop a theoretical perspective whereby we link social capital and strong ties theories to those about role effects in social support activation and apply it to an important case: living kidney donation behaviors. We find that role effects on living kidney donation behaviors are substantial and best accounted for by a combination of biomedical resource and tie strength mediation. Together, these findings have the potential to inform interventions to promote living kidney donation and make further sense of the diversity of observed role effects on social support.
Supplemental Material
sj-docx-1-srd-10.1177_23780231231171097 – Supplemental material for Roles, Relationships, Resources, and Renal Exchange: Applying Social Capital Theory to Role Effects on Living Kidney Donation Behaviors
Supplemental material, sj-docx-1-srd-10.1177_23780231231171097 for Roles, Relationships, Resources, and Renal Exchange: Applying Social Capital Theory to Role Effects on Living Kidney Donation Behaviors by Jonathan Daw and Ashton M. Verdery in Socius
Footnotes
Acknowledgements
We would like to thank Shawn Bauldry, Chenoia Bryant, Robert Gaston, Bryant Hamby, Katie McIntyre, Léa Pessin, Sarah Rutland, Mary Roberts, Zarmeen Salim, and the Population Health Working Group at the Population Research Institute at the Pennsylvania State University for their assistance and advice with this research and manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by the UAB Comprehensive Transplant Institute Arnold G. Diethelm Research Acceleration Grant; a seed grant from the Pennsylvania State University Population Research Institute, which is supported by an infrastructure grant by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (P2C-HD041025); and National Diabetes and Digestive and Kidney Disease grant R01DK114888.
Supplemental Material
Supplemental material for this article is available online.
1
The term role has long been used ambiguously (e.g., ![]() ; Wasserman and Faust 1994:345–92; Kahn and Antonucci 1980). To avoid ambiguity, we use the term role as shorthand for role relationships (e.g., parent, sibling, friend). Although status (“the class of roles which is institutionalized” and for which expected and obligated behaviors are agreed upon; Goode 1960:250) is a tempting alternative, we avoid this term because the behaviors we examine are not clearly agreed upon, and the role concept is more general than status.
; Wasserman and Faust 1994:345–92; Kahn and Antonucci 1980). To avoid ambiguity, we use the term role as shorthand for role relationships (e.g., parent, sibling, friend). Although status (“the class of roles which is institutionalized” and for which expected and obligated behaviors are agreed upon; Goode 1960:250) is a tempting alternative, we avoid this term because the behaviors we examine are not clearly agreed upon, and the role concept is more general than status.
2
Thoits (1982) and Song, Son, and Lin (2011) provided an extensive review of divergent social support conceptualizations with a focus on how social support interfaces with health.
3
![]() viewed convoys as complementary to role relations: “we propose to think of support as coming from a personal network of family, friends, and others. . . . Such networks . . . we have called convoys. We regard the concept of convoy as complementary to that of role, and we propose to use these concepts jointly” (p. 267).
viewed convoys as complementary to role relations: “we propose to think of support as coming from a personal network of family, friends, and others. . . . Such networks . . . we have called convoys. We regard the concept of convoy as complementary to that of role, and we propose to use these concepts jointly” (p. 267).
4
The most commonly referenced definition of social capital is “the aggregate of the actual or potential resources which are linked to possession of a durable network of more or less institutionalized relationships of mutual acquaintanceship or recognition” (Bourdieu, quoted in Portes 1998:3). Conceptual distinctions between different conceptualizations of social capital are reviewed in Portes (1998), Lin (1999), and, when applied to health, Carpiano (2006) and ![]() .
.
5
Based on our analyses of the Standard Transplant Analysis and Research data set from the United Network for Organ Sharing, covering 2008 to 2017. Details and code are available upon request.
6
This is not to say that sociological gatekeeping is altogether absent from living donor kidney transplantation. Transplantation nephrologists long hesitated to accept living kidney donations from more distant kin and nonkin even after it was proved medically feasible (Spital 1989, 1994, 1996, 2000). Similarly, nonmedical contraindications for living kidney donation are still used today, as many transplantation programs will not accept living kidney donations from prisoners (British Transplantation Society 2015; ![]() ) or those suspected of engaging in illegal financial exchanges.
) or those suspected of engaging in illegal financial exchanges.
7
8
Stata code to replicate all analyses will be released with the published version of this article. Additionally, we will work with interested parties to conduct supplemental analyses upon request.
9
This measure is somewhat imprecise in the interest of minimizing respondent burden. It does not distinguish between half, full, or monozygotic twin relations, and the “other family” blood relative value is arbitrary. As a robustness check, we reestimated all analyses with half of all imprecisely measured genetic relationships reassigned to other possible values, and the results were highly correlated with those presented in this article (see ![]() ).
).
10
For each network member, the transplantation patient is asked, “How often do you talk to this person?” Response options included “once a year or less,” “2 to 11 times a year,” “once a month,” and “once a week or more.” All four categories are used in the analysis.
11
The stem for this item read, “Continuing to think of your relative with weak or failing kidneys, check all that apply.”
12
We combined “male” and “other” because few respondents marked the latter.
13
For respondent’s race/ethnicity, the respondents could select multiple races, but because of a survey error, they could only select one race for the patient. We assigned Hispanic/Latino to any respondent who marked it; otherwise, if they selected multiple races we coded them as other. We also combine the American Indian or Alaska Native option with other because of small cell size.
14
15
16
This is not to say that financial resources are of no use when seeking an organ transplant. Although it is illegal in the United States to purchase a living kidney donation outright, it is legal to provide financial support for the indirect costs incurred by living kidney donors such as foregone wages and dependent care. Furthermore, financial resources could also better position one to pursue a deceased donor organ transplant, because transplantation candidacy decisions are influenced by the patient’s insurance and financial resources.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.