
Abstract
Although immigration enforcement has been linked to poor health outcomes among Latinx populations in the United States, little is known about how interpersonal interactions between immigrants and immigration enforcement agents potentially influence Latinx immigrant health. The author estimated heterogeneity in health outcomes among deported Mexican immigrants by experiences of immigration enforcement abuse using data from respondents to the Survey of Migration in the Northern Border of Mexico (n = 28,853). Experiences of abuse were significantly associated with worse self-rated health and various health symptoms, with particularly large disparities for mental health symptomology. Given the magnitude of the deportation regime enacted against Mexican immigrants in the United States, thousands of immigrants may return to Mexico at an elevated risk for relatively poorer health. These results emphasize the importance of considering micro-level interactions as a mechanism of health stratification within the larger system of immigration enforcement in the United States.
Many immigrants in the United States suffer because they endure “legal violence” from the state (Menjívar and Abrego 2012). “Legal violence” refers to bodies of laws, policies, and practices that cause social suffering or create the conditions for its existence, representing violence that is normalized as part of “the law” (Menjívar and Abrego 2012). A hallmark of legal violence is the U.S. deportation regime. Deportation constitutes a gendered racial removal program (Golash-Boza and Hondagneu-Sotelo 2013) that primarily targets Latinx men, with Mexican immigrants constituting the single largest group of deportees (Moinester 2018, 2019). Indeed, contemporary immigration policy, especially in relation to undocumented immigrants, aims to either deport immigrants directly (Menjívar, Gómez Cervantes, and Alvord 2018; Ngai 2004) or make their lives so miserable that they choose self-deportation (García 2019; Park 2019; Rocha et al. 2014).
Two burgeoning literatures describe the effects of legal violence on the lives of U.S.-born Latinxs and Latinx immigrants. One traces the health impacts of restrictive immigration policies at the federal, state, and local levels (Martinez et al. 2013). Many studies that empirically assess the association between restrictive immigration policies and Latinx health show that immigration enforcement policies are associated with declines in health (Bruzelius and Baum 2019; Hacker et al. 2012; Lopez et al. 2016; Mann-Jackson et al. 2018; Torche and Sirois 2019; Wang and Kaushal 2018) and health service use (Hacker et al. 2011; Rhodes et al. 2015; Toomey et al. 2014). The other literature describes how structurally racist immigration policies create a context in which immigration enforcement officials engage in persistent everyday violence against anyone who “looks Mexican” (Romero 2016; Sabo et al. 2014; Viruell-Fuentes, Miranda, and Abdulrahim 2012). Everyday violence against immigrants entails excessive physical force, verbal harassment, and confiscation of belongings during the apprehension and detention of individuals constructed as deportable (Martínez, Slack, and Hyman 2013; Phillips et al. 2002, 2006; Sabo and Lee 2015; Sabo et al. 2014; Slack et al. 2016). Immigration agents are seldom punished for the violence they commit against immigrants (Martínez, Cantor, and Ewing 2014).
Despite developing in tandem, the two literatures largely speak past one another. Research on the health impacts of restrictive immigration policies generally focuses on policy environments, assessing the health outcomes of Latinx residents by way of the variation they experience in immigration enforcement across geographic units (Philbin et al. 2018; Wang and Kaushal 2018). Thus, studies on health impacts usually do not identify immigrants who have direct system contact via arrest, detention, and deportation. In contrast, research on state violence committed by immigration agents uses individual-level data to examine abuse as it is experienced by immigrants who report interactions with immigration officials (Martínez et al. 2013; Phillips et al. 2006; Sabo et al. 2014) but typically ignores health. Therefore, although scholars continue to produce work on the health outcomes of various Latinx populations living under various enforcement policies, as well as work on the prevalence of state violence against immigrants, little is known about how forms of state violence committed during interpersonal interactions between immigrants and immigration agents potentially affect the health of Latinx immigrants who experience deportation. The omission of the micro-level interactions that produce state violence is important not just empirically because we should wish to identify who experiences such violence but also theoretically because those interpersonal interactions act as one bridge in explaining how immigration-related structures and institutions enact violence in everyday life, shedding light on how legal violence is produced and reproduced over time.
Immigration Enforcement and Latinx Health
Fear of arrest, detention, and deportation is a ubiquitous mechanism explaining the health impacts of immigration enforcement on Latinx populations (Hardy et al. 2012). Immigration raids, arrests, and deportations are highly visible events that shape the everyday behaviors of community members (Hagan, Rodriguez, and Castro 2011), immigrant and nonimmigrant. Unsurprisingly, immigration arrests and raids are at the center of the literature on immigration enforcement and Latinx health. Bruzelius and Baum (2019) estimated the impact of exposure to state-level immigration arrests on mental health among Latinx respondents, finding that exposure to relatively higher immigration arrest rates was associated with a significantly higher risk for worse mental health, including more frequent mental distress (Bruzelius and Baum 2019). Other scholars, using the timing of immigration raids, found that the postraid periods were associated with significantly elevated risks for negative psychological consequences, delays in pregnancy (Fleming et al. 2019), immigration enforcement–related stress, and worse self-rated health (Lopez et al. 2016).
Immigration raids are public spectacles designed to engender fear, but immigrants, particularly the undocumented, are keenly aware of how immigration enforcement policies aside from raids shape their daily lives (García 2019). Local police cooperation with Immigration and Customs Enforcement (ICE), for instance, was associated with worse health for Latinx populations across a number of studies, whether it was Hacker et al.’s (2011) case study of a town in Massachusetts or Wang and Kaushal’s (2018) demonstration that various enforcement tactics under section 287(g) and the Secure Communities program were associated with worse emotional distress and worse self-rated health. In addition to poor health and mental health outcomes, local police cooperation with ICE was associated with increased mistrust of health services and delayed health services among Latinx mothers after Arizona’s infamous Senate Bill 1070 immigration legislation (Toomey et al. 2014) and section 287(g) cooperation agreements in North Carolina (Rhodes et al. 2015).
In contrast to studies that attempt to produce estimates of impacts of specific immigration policies on Latinx health (Rhodes et al. 2015; Toomey et al. 2014; Wang and Kaushal 2018), other scholars have attempted to assess how policy climates affect the physical and mental well-being of Latinx residents across states. Vargas, Sanchez, and Juárez (2017) constructed a measure of state-level immigration policy perceptions among Latinx residents to assess how unfavorably Latinx residents viewed immigration policies in their respective states. Living in states with relatively higher anti-immigrant policies was associated with worse self-rated physical and mental health. Self-reported health outcomes were worst for Latinx respondents who lived in states that had both high anti-immigrant and anti-Latinx climates (Vargas et al. 2017). Hatzenbuehler et al. (2017) constructed a policy climate index by aggregating information on 14 policies across four domains (immigration, race/ethnicity, language, and agricultural worker protections) in 31 states. Latinx residents in states with the most exclusionary policy climates reported higher rates of poor mental health days. The association between policy climates and poor mental health was significantly stronger for Latinx residents than non-Latinx residents (Hatzenbuehler et al. 2017).
Immigration Enforcement and Abuse Committed against Immigrants
Immigration enforcement efforts have targeted Mexican immigrants since the Border Patrol was founded in 1924. Ngai (2004) argued that immigration enforcement efforts at the border historically served two projects: (1) to “de-Mexicanize” the U.S. border states and (2) to create an “imported colonialism” that depends on the existence of a Mexican agricultural proletariat consisting of racial “others” with various legal statuses. The de-Mexicanization process and creation of a vulnerable agricultural proletariat were facilitated by pervasive racial violence that consisted of predominantly white Border Patrol agents beating and killing Mexican immigrants (Hernández 2010) as well as their enforcement of intrusive and dangerous physical examinations and chemical baths (Molina 2011, 2016). Contemporary accounts of abuse against immigrants by the Border Patrol and ICE demonstrate that current immigration agents have not shed the violent tendencies of their forebearers (Martínez et al. 2013; Phillips et al. 2002, 2006; Sabo et al. 2014). Abuse committed against immigrants at the interpersonal level is not an aberration but a systemic problem produced by the structural and institutional forces underlying border and immigration enforcement (Slack et al. 2016).
The structural underpinnings of interpersonal abuse are rooted in laws that direct the use of federal resources, expand interactions between immigrants and enforcement officers, and transform the U.S.-Mexico border into a militarized zone. The case of U.S. Customs and Border Protection (CBP) is illustrative. The 1996 Immigration Reform and Immigrant Responsibility Act called for the hiring of 1,000 new Border Patrol agents per year in order to reach 10,000 total agents by 2001 (Andreas 2009a) before post-9/11 laws doubled Border Patrol agents from approximately 10,000 in 2001 to more than 20,000 in 2010 (CBP 2020). Immigration enforcement has turned increasingly toward the criminalization and deportation of immigrants since the passage of the 1996 Immigration Reform and Immigrant Responsibility Act (Menjívar et al. 2018). Indeed, the total number of deportations since 1997 amounts to more than twice the number of all deportations before 1997 (Golash-Boza and Hondagneu-Sotelo 2013). Deportations are now endemic to Latinx immigrant life in the border regions as well as the U.S. interior (Moinester 2018). Increased immigration enforcement, in conjunction with the recent militarization of the U.S.-Mexico border and the agents who patrol it (Andreas 2009b), creates the potential for abuse by increasing the total number of interpersonal interactions between immigration officers and immigrants (Jancsics 2019a), shifting power toward enforcement agents, and framing Mexican immigrants as a threat in the “war” on U.S. borders. Falcón (2001) demonstrated that violence toward immigrants is the inevitable consequence of border militarization in her analysis of interpersonal abuses committed against Mexican immigrant women by Border Patrol officers.
Macro-structural changes in immigration enforcement do not alone determine the prevalence of micro-level abuse against immigrants, as meso-, organizational-, and/or institutional-level factors also play a role in shaping enforcement officers’ behavior. The cognitive and cultural elements of employment in federal immigration agencies may influence types and rates of interpersonal abuse. For instance, immigration enforcement agents internalize the “Latino threat narrative”—the widespread demonization of Latinx people in the United States (Chavez 2008)—by assimilating into dehumanizing processes that prioritize the operation of their respective agencies over the humane treatment of immigrants under their control (Rodriguez and Paredes 2013). The process of assimilation into dehumanizing methods of control is achieved through what Rodriguez and Paredes (2013) referred to as “bureaucratic ideological work,” constituting work that endorses the view that coercive—often lethal or fatal—enforcement is valid and essential for survival. A core tenet of bureaucratic ideological work is that the negative construction of immigrants must be socialized into the cognitive frames of some bureaucratic officials such that violence enacted by immigration agents does not diminish their sense of their own humanity. In addition to the dehumanization of Latinx immigrants, immigration enforcement officials incorporate narratives of moral authority and guardianship over the homeland into their ideological work as a means to engage in coercive enforcement with impunity (Rodriguez and Paredes 2013). Bureaucratic ideological work (Rodriguez and Paredes 2013) thus serves as one example of how the motivations and justifications for immigration enforcement–related abuse at the micro-level are rooted in group-level cognitive and cultural mechanisms embedded firmly within institutions of enforcement.
Institutional relations such as power dynamics among enforcement officers and their supervisors potentially influence officers’ behavior toward the immigrants they police. Two dynamics are relevant: lack of supervision and lack of oversight and discipline. Specific forms of abuse committed against immigrants (e.g., physical abuse) are largely subject to the discretion of individual enforcement officers. Immigration enforcement officers fit Lipsky’s (1983) seminal conceptualization of “streel-level bureaucrats” (see Romero 2016). Immigration agents are street-level bureaucrats who enforce immigration laws with impunity because they are not subject to supervision or discipline. For Border Patrol agents, the physical location of land borders, especially in remote areas, generates the opportunity for interpersonal abuse because their supervisors cannot view their day-to-day operations, creating what Vaughan (1982) referred to as structural “secrecy” within the organization. In general, it is almost impossible for supervisors to monitor their officers’ behavior on the line (Jancsics 2019a), giving Border Patrol officers among the highest level of discretion of any uniformed officers in a federal enforcement agency (Falcón 2001). A high level of discretion is more problematic when considering the lack of formal oversight and discipline under which immigration enforcement officers operate. Almost all (97 percent) of complaints against Border Patrol agents, for example, go unaddressed because the agency has no formal process for accepting and addressing complaints (Martínez et al. 2014). The internal investigative authorities within the U.S. Department of Homeland Security (DHS) for CBP are underfunded, understaffed, and even hostile to outside investigators. Several internal CBP investigators were convicted of obstructing investigations and coaching Border Patrol officers to avoid prosecution for unlawful behavior (Nowrasteh 2017). Corruption within CBP is endemic (Jancsics 2019a, 2019b), and the mechanisms available for oversight and discipline are weak, and yet Border Patrol officers between 2006 and 2016 were 2.8 times more likely to be terminated for discipline and performance issues than officers in federal law enforcement agencies who did not enforce immigration laws, suggesting that misconduct within U.S. immigration enforcement is particularly high (Nowrasteh 2017). Thus, immigration enforcement agents use their discretion to engage in micro-level interactions that impose “everyday violence” on Latinx immigrants (Sabo et al. 2014). These important micro-level interactions are inadequately attended to by studies that examine the effects of enforcement regimes or policies measured in the aggregate.
I conceptualize state violence against immigrants as three forms of abuse immigration officials choose to commit against Mexican immigrants: physical aggression, verbal aggression, and confiscation of belongings. This conceptualization of state violence is consistent with the extant literature on the abuse of immigrants in state custody. Martínez et al. (2013) found that 11 percent of respondents to the Migrant Border Crossing Study reported physical aggression (hit, pushed, grabbed, attacked physically) from enforcement officials. In the same report, the authors found that 23 percent of respondents reported verbal aggression (yelled at, threatened, verbally abused) while in U.S. custody (Martínez et al. 2013). Roughly 34 percent of Mexican immigrants in the Migrant Border Crossing Study data set also reported having possessions taken and not returned prior to deportation. Possessions included clothes, cell phones, money, and identifying Mexican documents (Martínez et al. 2013). In their sample of Salvadoran deportees, Phillips et al. (2006) found that about 25 percent of deportees experienced verbal harassment during their arrest and/or detention, while 20 percent and 11 percent experienced physical force during their arrest and detention, respectively. In their analysis of use of force during immigration arrests, Phillips et al. (2002) found that 16 percent and 8 percent of Salvadoran deportees in their sample experienced physical force in their arrest and detention, respectively.
Abuse and Health
This article advances knowledge on abuse committed by state agents and health among immigrants by using individual-level data to estimate the associations between experiences of abuse and health. This is the first research, to my knowledge, that estimates how micro-level interactions enacting the violence of ideological and historical structures surrounding immigration policy—operationalized as abuse by immigration officials—are associated with health. In the extant literature, it is impossible to discern which, if any, respondents across various studies were directly targeted by immigration policy (arrested, detained, and/or deported). Rather, existing research assumes exposure to immigration enforcement results from residence in a geographic unit of analysis that includes some level of enforcement. Thus, the approach I use constitutes both empirical and theoretical contributions. Empirically, I provide descriptive estimates of how abuse is associated with the health of deported Mexican immigrants, the single largest group the United States deports. In the realm of theory, I demonstrate that the current literature ought to move beyond its narrow focus on important macro-level systems of stratification and examine how abuse perpetrated through micro-level interactions potentially creates heterogeneity in health outcomes. Moreover, the forms of abuse included in this article are consistent with the forms of abuse analyzed in the literature on abuses committed against immigrants by immigration enforcement officials (Martínez et al. 2013; Phillips et al. 2002, 2006; Slack et al. 2016). Thus, I integrate the literature on such abuse into the domain of health. The health outcomes in this article include a wider range of outcomes than most work on immigration enforcement and health, including self-reported health, fever, diarrhea, cough, lack of interest, sadness, and desperation.
Focusing on health outcomes among deported Mexican immigrants allows several contributions to the larger literature on deportation. Comparing deported Mexican immigrants with nondeported Mexican immigrants would serve to homogenize deportees and erase variation in their experiences of apprehension, arrest, and deportation. Prior studies on experiences of deportation among Mexican immigrants demonstrate that interpersonal abuse by immigration agents was experienced by only a (sizable) minority of Mexican deportees (Martínez et al. 2013). I use individual-level data to estimate within-group heterogeneity in experiences of interpersonal abuse, uncovering important variation in outcomes for Mexican immigrants deported by the DHS between 2010 and 2013, a group numbering 779,033 people in total (DHS 2021). Furthermore, focusing on deported immigrants allows an assessment of how specific types of interpersonal abuse may be associated with health outcomes. The literature on interpersonal abuse committed by police officers suggests that physical abuse, sexual abuse, and the use of a weapon are associated with significantly elevated odds of poor mental health outcomes (DeVylder, Frey, et al. 2017; DeVylder, Oh, et al. 2017). Yet similar knowledge about the potential associations between different forms of immigration enforcement–related abuse and health are, to my knowledge, estimated for the first time in the present article.
Methods
Data
I analyze data from the Survey of Migration in the Northern Border of Mexico (EMIF Norte; https://www.colef.mx/emif/basescuestionarios.html), an ongoing probability survey of migratory flows in the Mexican border region. I use data on respondents to Migrantes Devueltos por las Autoridades Migratorias de Estados Unidos (Immigrants Returned by U.S. Immigration Authorities) module of EMIF Norte for the years 2010 through 2013. Thus, the sample is restricted to Mexican immigrants who were deported by U.S. immigration enforcement during those four years. The EMIF Norte is a multistage probability survey that selects time and place units before selecting individuals within those units. EMIF Norte survey administrators sample at points within zones of return migration (e.g., airports, bridges, and bus disembarking spots) through which migrants must pass, observing each sampling zone for 24 hours a day for seven consecutive days so that they may enumerate all persons passing through and attempt to administer the filtering questions that determine eligibility for inclusion in the sample to as many migrants as possible. Thus, Mexican immigrants are surveyed about their experiences in the United States during the first moments in which they return to Mexico (Carriquiry and Majmundar 2013). Given the ubiquity of EMIF Norte data in research on Mexican migration, more information about the sampling procedures can be found elsewhere (Carriquiry and Majmundar 2013; EMIF Norte 2022).
EMIF Norte began collecting data on general health status in 2010. Information on various past 15-day physical and mental health symptoms was collected between 2012 and 2014. I restrict the analytic sample to survey years 2010 through 2013 for analyses of general health status because 2014 data include significant missingness on the independent variables of interest. I restrict the analytic sample to survey years 2012 and 2013 for the analyses of past 15-day health symptoms. The frequency of missing data is less than 3 percent and 6 percent, respectively.
Measures
Dependent Variables
For all survey years (2010–2013), respondents rated their current self-reported health status on a five-point, Likert-type scale including responses ranging from “very poor” to “very good.” The health scale ranges from 1 to 5, with 5 indicating “very poor.” 1 To conduct logistic regression and estimate predicted probabilities, I dichotomized the general health scale such that 0 = “very good”/“good” health and 1 = “fair”/“poor”/“very poor” health, given low frequencies of “poor” and “very poor” health among respondents. For the survey years 2012 and 2013, respondents endorsed whether they experienced the following symptoms over the past 15 days: fever, diarrhea, cough, little interest in doing things, sadness, and desperation. Separate dichotomous variables (yes/no) represent each symptom.
Abuse from Immigration Officials
Respondents were asked, During the persecution and until your arrest by immigration agents, were you subject to: (1) physical aggression (pushes, hits/slaps, etc.), (2) verbal aggression (screams or insults), (3) confiscation of your belongings?
I dichotomize each measure of abuse into a separate dichotomous (yes/no) variable.
Covariates
Sociodemographic controls include gender (man/woman), age (continuous), educational attainment (treated as a categorical variable, from none to doctorate), fluency in an indigenous language (yes or no), and fluency in English (yes or no). 2 Migration-related controls include the lifetime number of crossings into the United States (continuous), whether respondents had family or friends living in the United States (yes or no), the location respondents were apprehended by immigration enforcement (work, home, on the street or highway, while crossing the border, desert or mountain areas, other), and whether respondents had proper documentation to cross the border (yes or no). A binary variable (yes or no) indicates whether a respondent received medical attention during the most recent trip to the United States in the form of any health service, although the question was asked only for the 2012 and 2013 survey years.
Statistical Analyses
After presenting descriptive statistics, I use multivariable logistic regression to estimate the conditional associations between the binary self-reported health outcome and each form of immigration enforcement–related abuse for the respondents to the survey years of 2010 through 2013. Results for multivariable ordinal logistic regression models using the original health scale as the outcome are provided in Table S1 of the online supplement. I then use multivariable logistic regression to estimate the conditional association between each of the six past 15-day health symptoms and the three forms of abuse for respondents to survey years 2012 and 2013 before reestimating the models to include all three abuse variables simultaneously. 3 The multivariable logistic regression models for past 15-day health symptoms also include the control for health treatment use in the United States, as that variable was included only in survey years 2012 and 2013. I present regression results as odds ratios (ORs) and 95 percent confidence intervals (CIs). In addition to the ORs, I graph the predicted probabilities of health outcomes, stratified by experiences of immigration enforcement–related abuse. All models include robust standard errors and survey year fixed effects, computed using Stata MP 17.
Twenty-four models constitute the analyses involving past 15-day health symptoms wherein each of the three abuse variables were used to estimate associations across six outcomes before being included simultaneously for each outcome. To correct for the multiple tests performed in those analyses, I calculated false discovery rate–adjusted p values exploiting the Romano-Wolf multiple hypothesis correction method using the rwolf command in Stata (Clarke, Romano, and Wolf 2019). The Romano-Wolf correction procedure (Romano and Wolf 2005a, 2005b, 2016) uses bootstrap resampling to control for the familywise error rate (the probability of rejecting at least one true null hypothesis). I use 1,000 bootstrap replications. Tables S2 and S3 in the online supplement present the Romano-Wolf-corrected p values.
Results
Descriptive Statistics
Table 1 includes the descriptive statistics for the samples used in the self-rated health and past 15-day health symptoms analyses. Among the 28,853 respondents to the 2010 through 2013 EMIF Norte surveys included in the analyses of self-reported health, most respondents reported either good or very good health (89.88 percent). Approximately 10 percent of the sample reported fair, poor, or very poor health. The most common form of abuse was verbal aggression (9.39 percent), followed by confiscation of belongings (7.13 percent) and physical aggression (4.12 percent). Most deportees in that sample were men (83.28 percent) with a mean age of 30.08 years and a mean of 1.77 lifetime border crossings. The modal level of education among deportees in the sample was junior high school (secundaria). The most common locations of arrest by immigration enforcement officials were desert or mountain areas (41.52 percent), the street or highway (27.28 percent), and while crossing the border (17.07 percent).
Descriptive Statistics.

Frequencies (N) and percentages (%) are presented for dichotomous or categorical variables and means and standard deviations (S.D) are presented for continuous variables. Modal education percentage reported here but treated as categorical with full number of attainment possibilities in the statistical analyses.
The descriptive results for the past 15-day health symptoms analytic sample using 2012 and 2013 EMIF Norte data were like the sample for the self-reported health analyses. The most common health symptoms were sadness (26.74 percent) and desperation (25.31 percent), whereas the least common symptoms were diarrhea (3.13 percent) and fever (3.94 percent). Again, most deportees were men (83.62 percent) with a junior high school education and a mean number of 2.06 border crossings. The most common locations of apprehension were desert or mountain areas (38.66 percent), streets or highways (27.87 percent), and while crossing the border (23.60 percent).
Self-Rated Health
The results for the logistic regression analyses estimating the association between self-rated health and the three forms of abuse are presented in Table 2. On average and conditional on the covariates, reporting physical aggression from immigration agents was associated with significantly elevated odds of reporting worse overall health (OR = 1.54, 95 percent CI = 1.29–1.83). Similarly, both verbal aggression (OR = 2.36, 95 percent CI = 2.12–2.63) and confiscation of belongings (OR = 1.56, 95 percent CI = 1.36–1.79) were associated with significantly higher odds of reporting worse self-rated health. In the model that included all three forms of abuse simultaneously, verbal aggression (OR = 2.41, 95 percent CI = 2.21–2.73) and confiscation of belongings (OR = 1.26, 95 percent CI = 1.08–1.46) were associated with significantly elevated odds of reporting worse health, whereas physical aggression (OR = 0.80, 95 percent CI = 0.65–0.98) was associated with lower odds of reporting worse health, although only marginally. Results from ordinal logistic regression models that use the original five-point health scale as the outcome, presented in Table S1 in the online supplement, were substantively similar.
Logistic Regression of Self-Rated Health on Immigration Enforcement Abuse.

Note: All models control for gender, age, educational attainment, fluency in an indigenous language, fluency in English, family and friends in the United States, total number of lifetime border crossings, location of apprehension, and immigration documents. All models include survey-year fixed effects. Self-rated health (1 = “regular,” “malo,” “muy malo”; 0 = “bueno,” “muy bueno”).
p < .05. **p < .01. ***p < .001.
Past 15-Day Health Symptomology
The conditional associations between the three categories of abuse and past 15-day health symptoms are presented in Table 3, the top half of the table representing the abuse categories being modeled separately from each other and the bottom half representing models in which they were included simultaneously. Reporting physical aggression, conditional on the covariates and on average, was associated with a significantly higher likelihood of reporting all six health symptoms. Like physical aggression, reporting verbal aggression from immigration agents was significantly associated with higher odds of reporting all six past 15-day health symptoms. Having belongings confiscated during apprehension was associated with a significantly higher likelihood of four health symptoms, including cough (OR = 1.65, 95 percent CI = 1.34–2.01), lack of interest (OR = 2.70, 95 percent CI = 2.02–3.61), sadness (OR = 1.37, 95 percent CI = 1.17–1.60), and desperation (OR = 1.59, 95 percent CI = 1.37–1.86). When all three abuse types were included in the models simultaneously, the association between physical aggression and all six health symptoms became too imprecise to make an inference either way. The associations for verbal aggression and confiscation of belongings remained substantively similar to the models in which abuse types were included separately from one another.
Logistic Regression of Past 15-Day Health Symptoms on Immigration Enforcement Abuse, Abuse Types Included Separately Then Simultaneously.

Note: All models control for gender, age, educational attainment, fluency in an indigenous language, fluency in English, family and friends in the United States, the total number of lifetime border crossings, location of apprehension, immigration documents, and health treatment use in the United States. All models include survey-year fixed effects.
p < .05. **p < .01. ***p < .001.
I report the corresponding Romano-Wolf-adjusted p values in Tables S2 and S3 in the online supplement. Although the more conservative p values reduced the statistical significance of the point estimates in most cases, all the results, with the sole exception of the association between confiscation of belongings and sadness when all three abuse types were controlled for together, were robust to the correction.
Predicted Probabilities
Figure 1 presents the predicted probabilities of endorsing past 15-day health symptoms and fair, poor, or very poor self-rated health, stratified by experiences of immigration enforcement–related abuse, and holding covariates at their means. Graphical representations of percentage point differences constitute a more intuitive way of understanding the magnitude of the results than attempting to interpret ORs. The most common symptoms experienced among deported immigrants were sadness and desperation, with about a third of the sample reporting those symptoms. The predicted probabilities of experiencing sadness and desperation were approximately 9 percentage points higher for respondents who reported physical aggression. For the respondents who reported verbal aggression, the disparities in sadness and desperation were 10 percentage points and 12 percentage points, respectively. For the respondents who reported having their belongings confiscated, the disparities in sadness and desperation were six and nine percentage points, respectively. The third largest disparity in health for all forms of abuse was for experiences of coughing, with a 4 to 7 percentage point difference between deported immigrants who experienced immigration enforcement–related abuse and those who did not. All other disparities (fever, diarrhea, and lack of interest) ranged between approximately 1 and 4 percentage points. For ease of interpretation, I report disparities in self-rated health as the predicted probability of reporting fair, poor, or very poor health. The frequency of fair, poor, or very poor health was approximately 10 percent among deported immigrants. Experiencing physical abuse from immigration agents was associated with an approximate 4 percentage point increase in the endorsement of fair, poor, or very poor health among deported Mexican immigrants. The associated changes were 9 and 4 percentage points for experiencing verbal aggression and confiscation of belongings, respectively.
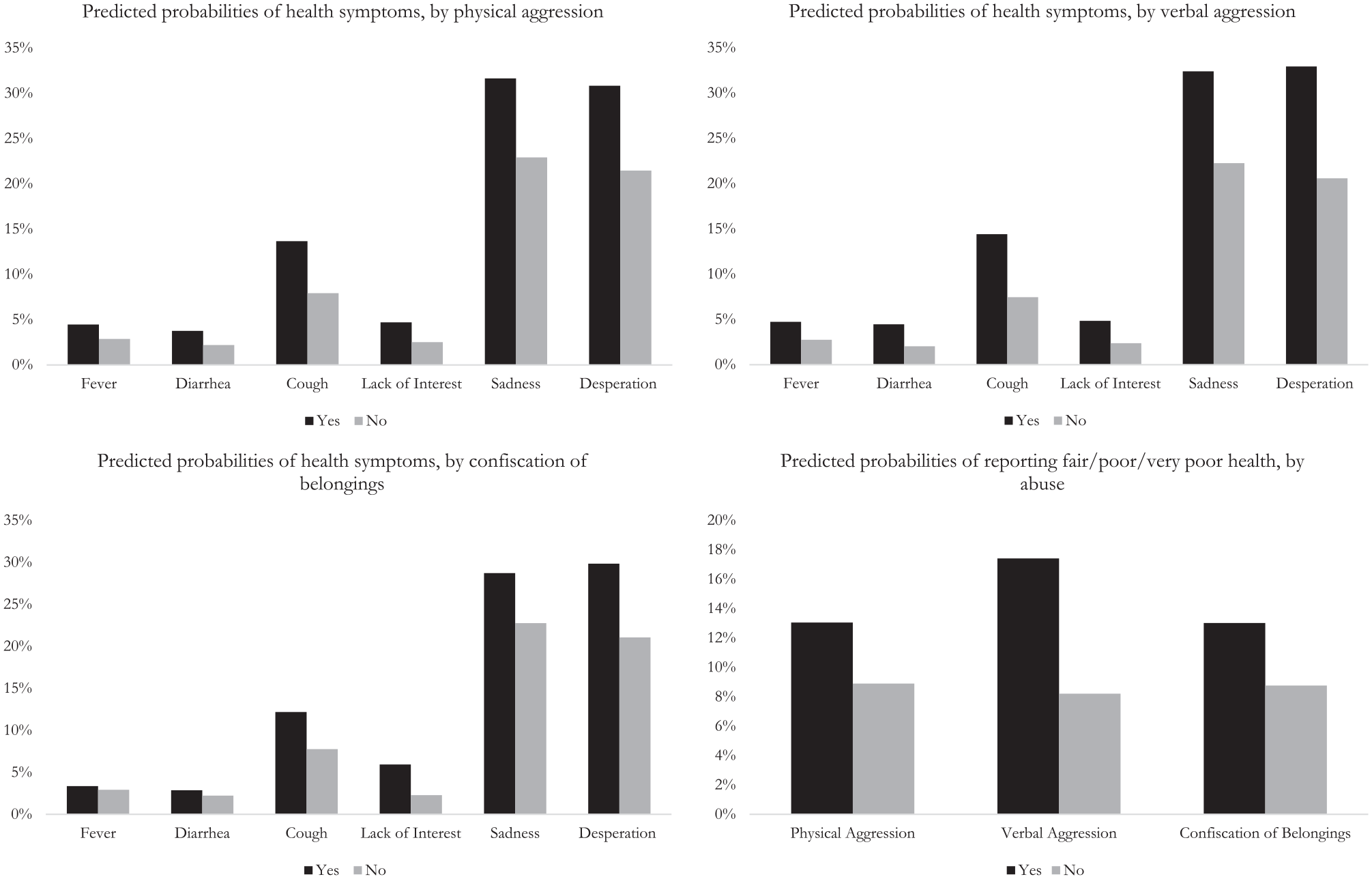
Predicted probabilities o health outcomes by abuse type.
Discussion
In this study I use individual-level data on immigration enforcement abuse to estimate associations between abuse and various health outcomes. Given the congruence between the operationalization of abuse in this article (physical aggression, verbal aggression, confiscation of belongings) and previous works (Martínez et al. 2013; Phillips et al. 2002, 2006), I demonstrate that the most commonly studied forms of immigration enforcement abuse were associated with significantly higher odds of poorer health. Although not exactly uniform across types of abuse and all health conditions, interpersonal abuse was significantly associated with poorer self-rated health and significantly higher likelihoods of reporting short-term fever, diarrhea, cough, lack of interest, sadness, and desperation. Disparities in short-term mental health between deported immigrants who did and did not experience immigration enforcement abuse were largest in magnitude for symptoms of sadness and desperation, with differences in those outcomes ranging from 6 to 12 percentage points. The deleterious associations between interpersonal abuse and health outcomes were robust to corrections for multiple hypothesis testing.
Potential Population-Wide Impacts (Descriptive Projections)
The magnitude of the estimates in conjunction with the magnitude of the deportation regime enacted against Mexican immigrants is cause for concern. I find it useful to present back-of-the-envelope calculations by combining the EMIF Norte estimates with data on deportations from the DHS Yearbook of Immigration Statistics for the years included in this study. The case of verbal aggression is illustrative. Between 2012 and 2013, DHS reported deporting 220,025 Mexican immigrants (DHS 2020). The frequency of verbal aggression for the EMIF Norte 2012 and 2013 survey years is 10.62 percent. Thus, if we assume for a moment that the EMIF Norte data are broadly representative of all deported Mexican immigrants in that period (a strong assumption, of course) then approximately 23,367 Mexican immigrants were exposed to verbal aggression during their apprehension and arrest. The estimates in this study demonstrate how the potential consequences of interpersonal abuse at the individual level aggregate into massive health disparities when the U.S. government forcibly removes millions of Mexican immigrants.
Potential Limitations
The results presented in this article should be interpreted bearing in mind various potential limitations. The EMIF Norte data are cross-sectional, precluding claims of causality. It is possible that reverse causality may be at play in that immigration enforcement officials commit the greatest levels of abuse against immigrants with preexisting health conditions. In the literature on policing, for instance, police are more likely to arrest (McCauley 2017; Sutton 2018) and kill (Myers 2017; Saleh et al. 2018) people with underlying disabilities and/or mental illness. Although an imperfect proxy for underlying health issues, the results for the analyses of past 15-day health symptoms were robust to the inclusion of a control for seeking medical treatment while in the United States, suggesting that potential health selectivity of abuse did not fully explain subsequent health symptoms. In any case, more research needs to be conducted to determine if immigration enforcement agents disproportionately target immigrants with health ailments. If immigration enforcement agents do engage in significantly greater abuse against immigrants with preexisting health ailments, this research uncovers a previously underexplored determinant of enforcement-related abuse against immigrants in the United States.
Furthermore, information should be collected on forms of abuse other than physical abuse, verbal abuse, and confiscation of belongings. Sexual violence is endemic in institutionalized settings, including immigration detention (Khullar and Chokshi 2019; Longazel, Berman, and Fleury-Steiner 2016). Trump-era separation of children from guardians during immigration proceedings constitutes state-sanctioned child abuse that affects both parents and children, raising the need for scholars and health practitioners to understand experiences of such violence (Miranda and Legha 2019). Additionally, I am able to examine abuse only at the beginning of the deportation process—apprehension and arrest—whereas future studies should assess how abuse while incarcerated is associated with health. Finally, the sampling design of the EMIF Norte survey only allows estimation of associations between abuse and short-term health. Future work should assess whether immigration enforcement–related abuse is associated with long-term health outcomes. Previous evidence suggests that returned Mexican migrants, despite having more favorable early-life health profiles than nonmigrant Mexicans, have significantly higher rates of physical and/or psychiatric disorders, even years after their return (Ullmann, Goldman, and Massey 2011). Waldman, Wang, and Oh (2019) demonstrated the same findings with respect to psychiatric health, pointing specifically to the deleterious association between undocumented migration and psychiatric problems. Although the literature on the health of returned immigrants does not adjudicate between the different causes of long-term health issues, it is possible and worth exploring whether and how abusive interactions with the state influence immigrant health over the life course.
Conclusion and Policy Implications
The potential health impacts of abuse enacted against deported Mexican immigrants during interpersonal interactions with immigration agents are considerable, particularly for mental health. The deportation regime perpetrated against Mexican-origin and Mexican American people in the United States means that millions of residents have been exposed to such abuse. There are at least two non–mutually exclusive paths forward regarding policy responses to immigration enforcement abuse. The first is abolition of an enforcement-centered immigration regime that entails centering the dignity and humanity of immigrants. Any systems change should foreclose, to the greatest extent possible, opportunities for the state to commit abuse against immigrants. Such a foreclosure naturally entails the dismantling of Border Patrol and ICE. The results of this study suggest that although enforcement is associated with immigrant health at the population level, more attention needs to be paid to variation in how immigrants are treated by agents of the U.S. government, the latter of whom should be held accountable when they abuse people who are detained and defenseless. Given the low probability of abolishing CBP and ICE, alternative policy solutions can focus on codifying standards for agents’ behavior and strengthening oversight and discipline. Martínez, Heyman, and Slack (2020) suggested various changes that intersect with the aspects of enforcement named in this article, including institutionalizing a uniform set of procedures for handling, tracking, and returning all nonperishable items taken from immigrants; streamlining current investigative bodies and establishing an independent civilian review board; publicizing all cases of potential misconduct above a certain threshold; establishing and enforcing standards of appropriate speech toward immigrants; updating, publicizing, and strictly enforcing use of force policies; and creating an open, free complaint process (with translation services) under the control of an external review board that records follow-through on all complaints. Second, state abuse committed against deported immigrants creates a system of transnational health stratification because immigrants, abused in the United States, return to Mexican communities with the consequences of their victimization. Consistent with calls to expand health services for immigrants on both sides of the U.S.-Mexico border (Waldman et al. 2019), Mexican communities should consider assessing the health needs of involuntary return immigrants. Just as state-sanctioned abuse results from deliberate enforcement policy choices, so too can it be prevented and remedied by deliberate policy interventions.
Supplemental Material
sj-docx-1-srd-10.1177_23780231221113635 – Supplemental material for Micro-level Interactions and Health Stratification: Abuses Committed against Deported Mexican Immigrants
Supplemental material, sj-docx-1-srd-10.1177_23780231221113635 for Micro-level Interactions and Health Stratification: Abuses Committed against Deported Mexican Immigrants by Kyle E. Waldman in Socius
Footnotes
Acknowledgements
I thank Mary C. Waters for helpful feedback on multiple drafts of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
1
The EMIF Norte was administered in Spanish. The verbiage used in this article reflects my translation of the original survey instrument.
2
A preferred measure of English fluency would be an ordinal scale. EMIF Norte includes such a scale, but the rate of nonresponse is too high to incorporate it into the present study.
3
3 The highest tetrachoric correlation between the abuse types is 0.78 (physical and verbal abuse), and the variance inflation factors for the abuse types are far below the commonly used standard of 10. To assess the potential impact of correlation across the abuse types, I recoded the abuse variables into a categorical variable including eight mutually exclusive combinations of abuse types. The results of that robustness check are consistent with the results in the main analyses in terms of both the direction of the association between abuse types and health outcomes as well as in statistical significance. See Tables S4 and S5 in the online supplement.
Author Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.