
Abstract
A growing body of research has begun to identify the social and ecological predictors of community overdose rates. However, questions remain about these relationships, and it is unclear whether the predictors of community overdose concentrations mirror those of other fatal social problems, such as homicide and suicide. Drawing on three leading ecological theories of overdose concentrations, the present study provides a longitudinal macro-level analysis of the community “determinants of death” for overdose (overall and by substance type), homicide, and suicide. Specifically, the authors use Centers for Disease Control and Prevention restricted-access mortality data, combined with measures of community social, economic, legal, and health indicators for the period from 2000 to 2015. Findings from time-series models reveal that county concentrations of overdose are linked to multiple theoretically driven factors—including opioid prescription rates, population decline, county health problems, and manufacturing employment—with several key similarities in the determinants of death across overdose, homicide, and suicide.
During the early decades of the twenty-first century, the United States experienced an unprecedented epidemic of drug overdose deaths. Between 1999 and 2019, drug overdose death rates more than tripled, rising from 6.1/100,000 to 21.6/100,000 to become the leading cause of injury deaths in the United States (CDC 2020; Hedegaard, Miniño, and Warner 2018). During this time, overdoses claimed more than 800,000 total lives and more than 70,000 deaths per year by 2019 (CDC 2020). Furthermore, annual deaths from the overdose crisis surpassed the number of lives claimed by the AIDS epidemic at its peak (approximately 50,000 in 1995; CDC 2011) and accounted for nearly three times the number of deaths from homicide seen during the height of the crime waves in the 1980s and 1990s (approximately 25,000 in 1989–1990; Cooper and Smith 2012). In part because of this rising wave of overdoses, research indicates that the average life expectancy in the United States has begun to decline for the first time in more than half a century (Case and Deaton 2015, 2017; Woolf and Schoomaker 2019).
Although the drug overdose crisis has affected people across all places and walks of life, it has affected some communities much more than others. As shown in Figure 1, states such as West Virginia, New Hampshire, and Ohio have experienced some of the nation’s highest overdose death rates (40/100,000 or more), whereas Nebraska, South Dakota, Texas, and Minnesota have seen rates that are nearly four times lower (at or below 10/100,000) (Hedegaard et al. 2018; Rudd et al. 2016). Similarly, there has been wide variation across communities within each of these states, with some places experiencing rises in overdose rates that are two or three times greater than those in neighboring locales (CDC 2019).

U.S. county overdose death rates per 100,000 Residents, 2015.
In light of this geographic variation, macro-level explanations for community overdose patterns have begun to coalesce around three theoretical perspectives, which we refer to as follows. First, the opportunity and availability perspective argues that community concentrations of overdose have been driven by increased drug availability, as more pills, more prescriptions, and more illicit heroin and fentanyl supply flooded communities throughout the United States (e.g., see Cicero et al. 2014; Peters et al. 2020; Ruhm 2019). Second, the communities of despair perspective proposes that declining economic conditions and weakening social systems (e.g., declines in manufacturing jobs, increased disadvantage, population decline, and weakened social services) have contributed to rising drug overdose concentrations across many communities (see Case and Deaton 2015, 2017; Monnat 2018, 2019; Woolf and Schoomaker 2019). Third, the community health problems perspective suggests that chronic health conditions, limited health resources, and greater emphasis placed on pain management may have also contributed to community overdose concentrations as people turned to opioids and other drugs to treat persistent ailments and conditions (see Ciccarone 2019; Dasgupta et al. 2018; Guy et al. 2017).
Although a growing body of research has assessed these arguments, key questions remain about the “ecological” or community predictors of overdose deaths. Researchers continue to debate which theoretical explanations and factors matter most, and when, where and for whom (and for which substances) they matter (see Maclean et al. 2020; Peters et al. 2020; Ruhm 2019). Much of the extant research examining macro-level predictors of overdose has also relied on cross-sectional analyses (Ford, Sacra, and Yohros 2017; Haffajee et al. 2019; Monnat 2018; Rosenfeld, Wallman, and Roth 2021) and assessments of total overdose rates or a single substance type (e.g., Dean and Kimmel 2019; Haffajee et al. 2019; Lin et al. 2019; Thombs et al. 2020; Venkataramani et al. 2019). In addition (and of central interest here), research has provided few analyses comparing macro-level predictors of overdose with those of other well-studied fatal social problems, such as homicide and suicide (but see Rosenfeld et al. 2021).
In light of these issues, the present study provides a longitudinal analysis and comparison of the macro-level predictors of overdose (overall and by substance type), homicide, and suicide deaths. Drawing from the three leading theories of macro-level overdose patterns, our goal is to examine the contextual factors—social/economic, legal, and health-related characteristics—associated with drug overdose concentrations throughout U.S. communities. More important, we compare the contextual sources of overdose deaths with those of homicide and suicide to assess whether the predictors of overdose concentrations are unique or whether they reflect “general” community determinants of death for each of these fatal social problems (Case and Deaton 2015, 2017; Siddiqi et al. 2019). 1 Notably, such comparisons are important for (1) identifying and combating the sources of overdose, homicide, and suicide and (2) developing consolidated theoretical understandings on overdose concentrations and other community determinants of death.
To conduct this analysis, we examine county-level patterns of overdose deaths, homicides, and suicides drawn from the Centers for Disease Control and Prevention’s (CDC) restricted-access Multiple Cause of Death (MCOD) mortality data files from 2000 to 2015. County-level mortality data are combined with measures of community social, economic, legal, and health indicators drawn from multiple databases to create a unique macro-level data set. Using these data, we rely on hybrid time-series models (or “within-between” models; Allison 2009) to identify the macro-level determinants of overdose deaths by substance type (total overdoses, natural and semisynthetic opioids, synthetic opioids, heroin, and cocaine) as well as for homicide and suicide. As a prelude to this analysis, we first review the leading theories used to explain overdose death concentrations and existing macro-level research that explores these perspectives.
Macro-level Theory and Research on Drug Overdoses
As described in the preceding section, overdose deaths have risen to epidemic proportions, increasing by approximately 300 percent from 1999 to 2019 (CDC 2020; Monnat and Rigg 2018). Although drug-related mortality has increased in 99.8 percent of all U.S. counties since 1980 (Dwyer-Lindgren et al. 2016, 2018), the overdose crisis has been far more concentrated in some places than others, as illustrated in Figure 1. To explain this geographic variation, research has relied on three theoretical explanations for community overdose concentrations, which are depicted in Figure 2 and described in more detail below.

Conceptual framework and leading macro-level theories for community overdose concentrations.
First, according to the opportunity and availability perspective, concentrations of drug overdoses stem from greater opportunity for drug use and greater availability of opioids, prescription pain medications, and other substances. Multiple sources have shown that pharmaceutical companies increased production of prescription opioids and aggressively marketed and distributed these substances in recent decades, which may have contributed to rising levels of opioid (and perhaps heroin) addiction (see reviews in Cicero et al. 2014; Pitt, Humphreys, and Brandeau 2018; Van Zee 2009). In addition, there is growing evidence that health care professionals prescribed and dispensed pain medications at higher rates in the early 2000s, which may have also contributed to increased opioid use and unintentional overdoses (Cicero et al. 2014; Dowell et al. 2017; Guy et al. 2017; Kuehn 2014; Van Zee 2009). Research suggests that opioid prescriptions saw widespread increases across a variety of medical providers in the early 2000s, as broader concerns about patient pain levels overshadowed concerns about addiction (Monnat 2018, 2019). Furthermore, increased availability of heroin and synthetic opioids such as fentanyl flooded markets in the first few decades of the twenty-first century but especially after 2010, providing yet another supply of potentially lethal substances to many communities (Monnat 2018, 2019; Peters et al. 2020; Quinones 2015). In sum, this supply-based perspective suggests that communities throughout the United States saw widespread growth in opportunity and availability for drug use (especially opioids), which may have fueled concentrations of overdoses in such locales.
In line with this perspective, empirical studies have shown that overdose death rates are greater in places with higher opioid prescription rates and greater drug availability (Alpert et al. 2019; Monnat 2019; Monnat et al. 2019; Peters et al. 2020; Ruhm 2019; Thombs et al. 2020). However, other research suggests that opioid prescribing has not been the primary source of overdose deaths, especially in later stages of the overdose epidemic, which are more likely to have stemmed from fentanyl and heroin (Rose 2018). In addition, some research indicates that opioid prescribing is related to rural overdose patterns but may have less impact on urban overdose rates (Peters et al. 2020).
Second, according to the communities of despair perspective, a key driver of overdose problems has been rising patterns of community deprivation, disorganization, and despair (Case and Deaton 2015, 2017; Denney et al. 2013; Monnat 2018, 2019; Woolf and Schoomaker 2019). Dating back several decades before the turn of the twenty-first century, many communities throughout the United States began to experience harsh economic circumstances and shrinking opportunities for prosperity, including wide expansions in inequality (see Denney et al. 2013). Economic restructuring initiated in the late twentieth century, which then combined with a near decade-long recession beginning in 2008, continued to pull low-skill, high-wage labor out of many communities and had devastating consequences for those left behind. Booming industrial towns became hollowed-out communities with growing unemployment, rising poverty rates, shrinking populations, declining public education systems, and stagnant wages and home values (Case and Deaton 2015, 2017; Ciccarone 2019; Kristof and WuDunn 2020; Wilson 1987). In addition, the social support systems in these communities began to weaken as hospitals, health providers, churches, and civic support networks and institutions shuttered their doors (Putnam 2000; Zoorob and Salemi 2017). According to this position, as social and economic problems mounted, communities most affected by these changes saw rising mortality for the “deaths of despair,” including overdose and suicide (Case and Deaton 2015, 2017).
Consistent with this perspective, a growing body of research has shown that community levels of economic disadvantage, social organization, and institutional support predict rates of drug use and overdose mortality across locales (Cerdá et al. 2013; Ford et al. 2017; Monnat 2018, 2019; Monnat et al. 2019; Monnat and Rigg 2018; Venkataramani et al. 2019; Zoorob and Salemi 2017). More specifically, studies have shown that overdose death rates are associated with trade-related job losses (Dean and Kimmel 2019), manufacturing employment and automotive plant closures (Monnat 2019; Peters et al. 2020; Thombs et al. 2020; Venkataramani et al. 2019), trade liberalization (Pierce and Schott 2020), median home prices (Brown and Wehby 2017), income inequality (Thombs et al. 2020), and measures of population decline and economic distress (Monnat 2018, 2019; Monnat et al. 2019; Rosenfeld et al. 2021). However, other studies suggest that social and economic hardship may have limited effects on overdoses and deaths of despair (Currie and Schwandt 2020; Ruhm 2019; Siddiqi et al. 2019; see review in Maclean et al. 2020).
Third, a final theoretical perspective suggests that a growing set of community health problems have also led people to seek opioids and other substances (Becker et al. 2008; Guy et al. 2017; Popovich 2016). Research indicates that U.S. populations have seen a rise in the prevalence of chronic pain and in medical conditions creating prolonged discomfort and suffering. High rates of obesity, musculoskeletal disorders associated with aging and overweight populations, increased use of surgeries, and greater rates of survivorship after cancer and severe injuries have left increasingly large portions of the population with long-term, chronic pain (Dasgupta et al. 2018; Keyes et al. 2014). At the same time, patients have grown to expect greater options for discomfort and more responsiveness to their pain, while insurance coverage has diminished for many health care plans. Thus, there are reasons to believe that unmet health needs and chronic pain may have driven people to seek relief with opioids and related substances, which in turn may have led to increased addiction and overdoses. Moreover, this may have been particularly prevalent in communities with limited health resources, fewer treatment options, and larger populations exposed to harsh working and social conditions (e.g., mining towns, Appalachian communities).
Consistent with the community health problems perspective, some research has shown that health problems and health care capacity are associated with macro-level patterns of overdose. For example, research shows that overdose mortality is linked to availability of opioid use disorder medication providers (Haffajee et al. 2019) and presence of health care and social assistance providers (see Maclean et al. 2020; Peters et al. 2020). However, other studies have shown that measures of aggregate health care environment are not associated with overdose death rates (Brown and Wehby 2017; Monnat 2018), and some research shows that greater levels of local health care access are actually associated with more overdose deaths (Lin, Liu, and Ruhm 2020).
Gaps in the Existing Ecological Research on Community Overdose Concentrations
As highlighted above, each of these theoretical perspectives has garnered empirical support and gained traction among researchers, reporters, political figures, and the broader U.S. public. Taken together this literature has made important strides toward identifying the macro-level sources of overdose deaths. However, several key gaps in this line of research remain, suggesting the need for additional inquiry. First, prior macro-level research has typically focused on total overdose rates (e.g., Rosenfeld et al. 2021; Thombs et al. 2020) or on a single substance. Much of this work has centered on opioids (e.g., Dean and Kimmel 2019; Haffajee et al. 2019; Lin et al. 2019; Venkataramani et al. 2019), with several other studies exploring neighborhood characteristics that specifically predict prescription drug misuse (Cerdá et al. 2013, 2017; Ford et al. 2017; Keyes et al. 2014) or heroin overdoses (Meiman, Tomasallo, and Paulozzi 2015). In contrast, research has given less attention to the ecological sources of nonopioid drug use, and even fewer studies have examined multiple substances simultaneously (but see Peters et al. 2020).
Second, macro-level studies of overdose mortality to date have largely been cross-sectional, focusing on a single year or a small window of time (e.g., 2010–2012) (Boardman et al. 2001; Ford et al. 2017; Haffajee et al. 2019; Monnat 2018; Rosenfeld et al. 2021). Although these studies have helped advance knowledge on community patterns of drug abuse, cross-sectional analyses are not able to capture the rapidly changing nature of the overdose epidemic throughout the early twenty-first century. Notably, a small handful of studies have begun this work (e.g., see Alpert et al. 2019; Lin et al. 2020; Ruhm 2019; Peters et al. 2020; Thombs et al. 2020). However, they have been the exception rather than the norm, and additional longitudinal analyses are needed that build on these existing studies.
Third, as highlighted above, existing research offers mixed findings and conclusions about which of the theoretical perspectives and ecological factors described above predict community overdose concentrations. For example, multiple studies indicate that community economic conditions (e.g., inequality, disadvantage, job losses, manufacturing employment) are linked to overdose deaths across places and time (Cerdá et al. 2013; Ford et al. 2017; Monnat 2018, 2019; Peters et al. 2020; Rosenfeld et al. 2021; Thombs et al. 2020; Venkataramani et al. 2019; Zoorob and Salemi 2017). Still, it is unclear whether some of these factors matter more than others. Furthermore, other literature suggests that social-economic conditions have little effect on overdose mortality (Currie and Schwandt 2020; Siddiqi et al. 2019; see review in Maclean et al. 2020), arguing instead that overdose concentrations are largely driven by supply-side factors (Ruhm 2019). In contrast, other studies reach the opposite conclusion and question the impact of drug availability. Some even report that reductions in opioid prescriptions are associated with rising overdose rates for heroin and other substances (see Pitt et al. 2018; Rose 2018). Thus, there is not yet an empirical consensus about the precise determinants of overdose deaths across communities and the degree to which each of these factors have shaped overdose concentrations. Or as Maclean et al. (2020) summarized, researchers have increasingly recognized that although the “causes of the (overdose) crisis include a combination of supply- and demand-side factors . . . there is less consensus regarding the relative importance of each” (p. 1).
Last (and central to the present study), research has provided few analyses that compare the macro-level predictors of overdose with those of other commonly studied fatal social problems, such as homicide and suicide (but see Rosenfeld et al. 2021). As a result, questions remain about whether the community sources of overdose deaths are unique or whether they reflect a general set of ecological risk factors that contribute to multiple community concentrations of death, which has both practical and theoretical implications.
On one hand, there are reasons to expect similarities in the macro-level determinants of death for overdose, homicide, and suicide. Overdoses have often been categorized with suicide and other “deaths of despair” under the assumption that they are connected, occur in similar places, and share similar sources (Case and Deaton 2015, 2017). In many ways, this parallels long-standing ecological traditions and theories in sociology. Dating back to the turn of the twentieth century, the Chicago School of sociology helped plant the early roots of “ecological” research by showing how a variety of social ills—including suicide, infant mortality, mental illness, physical ailments, pollution levels, as well as crime and violence—were concentrated in the same places and could be attributed to the same sets of social conditions (Ousey 2017; Park and Burgess [1925] 1967; Shaw and McKay 1942; Wilcox, Cullen, and Feldmeyer 2018). These and other ecological perspectives were never intended be exclusive to crime, suicide, or a single social problem. Rather, they suggested that large-scale, macro-level forces—including many of those incorporated into the “deaths of despair” or “communities of despair” perspectives—contribute to a variety of social problems (see Agnew 1999; Merton 1938; Pratt and Cullen 2005; Shaw and McKay 1942; Wilcox et al. 2018; Wilson 1987). As such, it is not altogether surprising that the leading macro-level theories of overdose deaths incorporate many of the same factors used to explain community concentrations of crime, suicide, and related social problems, suggesting the possibility of “general” or cross-cutting determinants of death for multiple forms of mortality. 2
On the other hand, there are also reasons to suspect that the determinants of death may differ for overdose, homicide, and suicide. Macro-level research has shown some differences in the predictors of homicide and suicide rates (Breault 1986; Breed 1963; Denney et al. 2009, 2015; Kubrin and Wadsworth 2009; Wadsworth and Kubrin 2007). In addition, there are important differences in the time trends and populations affected by overdose, homicide, and suicide. Since the 1990s, homicide has generally trended downward, whereas overdose and suicide death rates have risen dramatically (CDC 2019; FBI 2020). Overdose and suicide deaths have also been more prevalent among middle-aged (35–54 years) White male populations and have been rising in both urban and rural communities (Hedegaard et al. 2018; Rudd et al. 2016), while violent crimes have been more concentrated in urban areas and among young men (LaFree et al. 2008; Steffensmeier et al. 2010, 2011). However, research has yet to address whether the community-level drivers of drug overdose are entirely unique or share some commonalities with those of other social problems.
Notably, Rosenfeld et al. (2021) offered one of the few exceptions in their analysis examining the ecological predictors of overdose and homicide (but not suicide) for White and Black populations. 3 Specifically, their focus was on whether overdose deaths may have contributed to Black and White county homicide rates. In doing so, they reported several similarities in the predictors of overdose and homicide mortality, especially for Whites (e.g., structural disadvantage, manufacturing employment, home vacancies, and population size), but they also found many differences in the predictors of both types of death (especially for Black populations). Although their research provides an important set of comparisons in the macro-level predictors of overdose and homicide, it is one of the few existing studies to do so. Furthermore, their study relied on cross-sectional analyses and focuses on a single opioid overdose category (i.e., “narcotics and hallucinogens”). Thus, additional work is needed to determine whether the sources of community overdose concentrations are in fact unique or whether they derive from a common set of theoretically driven predictors—or “determinants of death”—that also explain concentrations of homicide and suicide across U.S. locales.
The Present Project, Data, and Methods
In light of the gaps in research identified above, the goal of this project is to provide a comparison of the macro-level predictors of overdose, homicide, and suicide death concentrations. Drawing from the leading theories on drug overdose patterns, in the present study we examine the ecological predictors of overdose, homicide, and suicide death concentrations across all U.S. counties for the period from 2000 to 2015.
Data
Data for the present project are drawn from multiple sources covering 1999 to 2016. Information on overdose, homicide, and suicide deaths are drawn from the CDC’s (2020) restricted-access MCOD mortality data. The MCOD mortality data contain all death records in the United States from 1999 to 2016 and report the underlying cause of death (e.g., overdose, homicide, suicide), other contributing causes of death (including specific substance type present in the deceased on the basis of toxicology reports), and location (county) for each death. Thus, they provide one of the only available sources of data on overdose, homicide, and suicide deaths with national coverage over time that can be aggregated to examine patterns of mortality across place, time, type of death, and drug type. Information on the ecological (e.g., social-economic, legal, and health) characteristics of counties are drawn from the following sources: (1) the U.S. census (decennial and American Community Survey [ACS] five-year estimates), (2) U.S. Census Bureau County Business Patterns data, (3) Institute for Health Metrics and Evaluation (IHME) county profiles, (4) Federal Bureau of Investigation Uniform Crime Reports (UCR), (5) CDC opioid prescription data, and (6) the Bureau of Justice Statistics (BJS).
Data on mortality and ecological context were combined and aggregated to the county level, which is our unit of analysis. County-level measures were compiled at five-year intervals to examine longitudinal changes in mortality and ecological context both between and within counties over time. This resulted in a county-level panel data set that includes 3,139 counties with measures at four time points: 2000, 2005, 2010, and 2015. Hence, results are presented for the period from 2000 to 2015 (using data that span 1999–2016). 4
Although ecological studies of social problems have used a variety of study units (census tracts, counties, cities, metropolitan statistical areas, states), counties are particularly well suited for the present project for several reasons. First, counties are well-established study units for examining aggregate patterns of overdose, homicide, and suicide patterns (see Dwyer-Lindgren et al. 2018; Light and Harris 2012; Monnat 2019; Monnat et al. 2019; Rosenfeld et al. 2021; Ruhm 2019). Second, counties are the smallest study unit identified in the CDC mortality data that may be used to aggregate records by geographic location (CDC 2020). Third, counties are substantively meaningful because they capture the local contextual characteristics of places, and county governments are often on the “front lines” for monitoring and combating problems related to local drug, crime, and suicide patterns (Monnat 2019; Monnat et al. 2019). Last, county-level analyses provide coverage for the nation as a whole (rather than a select set of cities or a sample of neighborhoods within a single city) and include both rural and urban areas, which is particularly important in light of research showing that drug overdoses have been prominent in rural and urban communities (Cerdá et al. 2017; Dombrowski et al. 2016; Keyes et al. 2014).
Dependent Variables
The dependent variables for the present study are county-level overdose, homicide, and suicide death counts. In addition to total overdoses, we also examine substance-specific overdose deaths across counties for (1) natural and semisynthetic opioids (e.g., morphine, prescription pain killers), (2) synthetic opioids (e.g., fentanyl), (3) heroin, and (4) cocaine. Data on overdose (overall and by substance), homicide, and suicide are drawn from restricted-access MCOD data (2020) covering 1999 to 2016. 5 The MCOD mortality data provide individual-level death records on the basis of coroner reports, including underlying cause of death, additional “contributing” or multiple causes of death (e.g., specific substances contributing to death), county of residence, and demographic characteristics of the deceased. We aggregated these individual records to generate county-level death counts for each of the forms of mortality examined here for 2000, 2005, 2010, and 2015. 6 All death counts were calculated using three-year averages (i.e., 1999–2001, 2004–2006, 2009–2011, and 2014–2016) to add stability to estimates and minimize the impact of single-year fluctuations (see Feldmeyer, Harris, and Lai 2016; Feldmeyer, Harris, and Scroggins 2015; Feldmeyer, Steffensmeier, and Ulmer 2013; LaFree et al. 2008; Steffensmeier et al. 2010, 2011).
The restricted-access MCOD mortality data are well suited for the present analysis because they offer one of the only available sources of data on overdose, homicide, and suicide mortality covering the entire United States (i.e., they include all death records) annually from 1999 to 2016. In addition, these data are particularly advantageous because they provide mortality records on locales with fewer than 10 overdoses (or homicides and suicides) in a year. In contrast, the CDC’s (2019) public-access mortality files report data only for places with at least 10 overdose, homicide, or suicide deaths in a year, which presents several problems for statistical analyses. Specifically, this type of “censoring” in the data eliminates places with few or no overdoses (or homicides and suicides) from the analysis, which is problematic for identifying communities and community contexts that are insulated from these forms of death.
Independent Variables
Drawing from the leading macro-level theories on overdose and from prior macro-level sociological research, we include a variety of measures capturing the social, economic, health, and legal contexts of counties during the period from 2000 to 2015. Table 1 provides more detail on these measures and their sources.
Variable Descriptions.

Note: BJS = Bureau of Justice Statistics; CDC = Centers for Disease Control and Prevention; IHME = Institute for Health Metrics and Evaluation; SAHIE = Small Area Health Insurance Estimates; UCR = Uniform Crime Reports.
First, on the basis of the “opportunity and availability” perspective, we include a measure of opioid prescription rates to capture drug availability. This variable was drawn from the CDC’s county opioid prescription data, measuring the number of retail opioid prescriptions per 100 county residents (see Dowell et al. 2017). 7 Although this covers approximately 90 percent of all retail pharmacy prescriptions, these estimates do not account for nonretail prescriptions or availability of illicit substances (heroin, cocaine) (CDC 2020). To address this concern, in supplemental models we included measures of opioid distribution from drug manufacturers to each county (milligrams per 1,000 residents) drawn from the U.S. Drug Enforcement Agency’s (DEA) Automated Consolidated Drug Reporting System (ARCOS) (see discussion of supplemental models). We acknowledge that neither data set accounts for illicit substance availability, a noteworthy caveat that we return to in our discussion of limitations and areas for future research.
Drawing from the “communities of despair” perspective, we include a variety of measures of county social, economic, and organizational context. To capture county socioeconomic context, we created a concentrated disadvantage index. Following practices of prior macro-level research (Land, McCall, and Cohen 1990; Sampson, Raudenbush, and Earls 1997; Steffensmeier et al. 2010), this measure was created using principal components analysis to combine measures of the percentage of residents in poverty, percentage unemployed, percentage aged 25 years or older with less than a high school education, and percentage of female-headed households with children younger than 18 years. All measures used to create the disadvantage index were drawn from U.S. census data. 8
The communities of despair perspective also suggests that employment patterns and changes in job markets (e.g., job losses) in manufacturing, mining, and other sectors may shape overdoses (and other death rates). Thus, we include measures capturing county employment rates (jobs per 1,000 people) in each of the following sectors: (1) manufacturing, (2) agriculture, (3) mining and resource extraction, and (4) professional and service sector employment, drawn from Census Bureau County Business Patterns data (2000, 2005, 2010, and 2015) (see Light and Thomas 2019; Monnat 2018; Ousey 2017). Notably, these measures capture employment in specific sectors net of broader disadvantage and overall employment rates included in the disadvantage index. We measure community institutional support using the presence of social assistance agencies (number of civic associations, nonprofit organizations, and social assistance and health care firms) per 1,000 residents, drawn from Census Bureau County Business Patterns data (U.S. Census Bureau 2018; see Ousey 2017; Zoorob and Salemi 2017). We include several measures of community stability commonly used in macro-level analyses of crime and suicide drawn from U.S. census data. These include residential mobility (percentage of people remaining in the same residence for the past five years) and racial/ethnic heterogeneity (an entropy index of diversity) (Feldmeyer 2009; Osgood and Chambers 2000; Pratt and Cullen 2005). We also include a measure of immigrant concentration (percentage foreign born) because it has been shown to create community organization and cohesion in ways that insulate places from crime and health problems (Ousey and Kubrin 2018; Sampson 2008).
Drawing from the “community health problems” perspective, we include a measure of county health insurance coverage (percentage of residents with health insurance) drawn from Census Bureau Small Area Health Insurance Estimates program from 2000 to 2015 (U.S. Census Bureau 2019). This measure includes coverage from both private insurance and Medicaid and includes Medicaid expansions from the Affordable Care Act (U.S. Census Bureau 2019). To measure county-level health problems, we created a community health problems index using factor analysis to combine county-level, age-adjusted rates of cardiovascular disease (per 100,000), lung disease (per 100,000), and average life expectancy drawn from IHME county profile data (Dwyer-Lindgren et al. 2016, 2018; IHME 2020). 9
We include several additional control measures commonly used in macro-level sociological and criminological research to account for county contextual characteristics that may affect crime or risky behavior (see reviews in Feldmeyer and Cochran 2018; Pratt and Cullen 2005). 10 These include measures of county total population, percentage young men (ages 15–24 years), police presence (police officers per 1,000 residents), and prison population for the state in which the county is located. 11
Preliminary analyses revealed significant spatial autocorrelation in overdose, homicide, and suicide concentrations on the basis of Moran’s I tests. Thus, we created and include spatial lag measures for each of our mortality measures to capture potential spillover effects of neighboring counties. Following the practices of prior research, we created spatial lag measures using the two-stage approach described by Land and Deane (1992). We regressed each of our mortality measures onto the full set of independent variables, and then created a spatial weight matrix (using GeoDA) to identify neighboring counties using the queen contiguity criterion. We then used this matrix and the predicted values to generate spatial lag measures.
Variables drawn from U.S. census, UCR, BJS, and IHME data had almost no missing values. Data on employment sectors and opioid prescription rates were missing for a small set of counties each year. Following the practices of prior research, we used multiple imputation to account for missingness in the data (Allison 2000; Monnat 2018). 12
Analytic Strategy
Using the panel data and variables described above, we use longitudinal analyses to identify the ecological predictors of overdose, homicide, and suicide concentrations within our sample of county years. Specifically, we predict each form of death using Poisson hybrid (“within-between”) time-series models, which incorporate both “fixed-effects” and “random-effects” estimates and are advantageous for several reasons (Allison 2009; Firebaugh, Warner, and Massoglia 2013; Light and Thomas 2019).
First, a key advantage of hybrid models is that they go beyond the cross-sectional models that have dominated macro-level analyses of overdose (and crime and suicide) to date. Although prior cross-sectional analyses have been informative, they are unable to identify how changes in county conditions correspond with the rapid changes in overdose deaths that have occurred within counties in recent decades. In contrast, time-series models (such as hybrid or fixed-effects models) are able to draw on the panel nature of these data to examine and predict change in mortality patterns within counties from 2000 to 2015 (Allison 2009; Firebaugh et al. 2013).
Second, hybrid time-series models are also advantageous because they include both random-effects and fixed-effects analyses (see Allison 2009; Firebaugh 2008; Firebaugh et al. 2013; Light and Thomas 2019). Researchers using panel data have often chosen between random-effects or fixed-effects models, which have their own caveats and trade-offs. The main strength of fixed-effects models is that by focusing exclusively on within-unit changes in predictors and outcomes (e.g., factors predicting increases in overdose within counties over time), they eliminate any potential bias from unmeasured predictors that are time stable. However, fixed-effects models offer little information about between-unit differences in outcomes, such as why there are wide differences in mortality across counties, which is also of interest here. In contrast, random-effects models allow these between-county comparisons but are more vulnerable to omitted variable bias. The hybrid model draws on the strengths of both approaches and estimates both random-effects and fixed-effects coefficients predicting (1) overdose differences across counties and (2) changes in overdose within counties over time.
To estimate the hybrid models, we created two versions of each predictor variable measuring the county mean for the variable during the study period (average of 2000, 2005, 2010, and 2015 values, used to examine between-county differences) and the within-county difference or deviation from its mean at each of the four time points analyzed. Results of the random-effects portion of the analysis are shown in Table 3 and reflect how differences in social, legal, and health context between-counties are associated with county mortality patterns for each cause of death. The fixed-effects portion of the analysis shown in Table 4 includes both time and county fixed effects and reflects how within-county changes in mortality are associated with shifting contextual characteristics within locales from 2000 to 2015.
We rely on count-based Poisson hybrid models with robust standard errors because of positive skewness in overdose, homicide, and suicide measures. We include total population as an exposure variable in each model and report the incident risk ratios (IRR) for coefficients to facilitate substantive interpretation of effects. Notably, we replicated all analyses using square root transformed dependent variables as a robustness check, which we present in the Appendix. We discuss these models in more detail in the supplemental analysis section but note that findings from these models were similar to those produced with the Poisson hybrid models. 13
To ensure that collinearity was not a problem, we were careful to select predictors with low correlations. Evaluation of collinearity diagnostics showed variance inflation factor values that were below standard cutoffs (<4.0) for all variables included in our final models. In addition, we explored several alternative modeling strategies and variables, which we describe in the supplemental analysis section.
Findings
Descriptive Statistics
Table 2 displays the descriptive statistics summarizing county patterns of mortality and ecological context for the period from 2000 to 2015. The overdose patterns shown in Table 2 mirror findings from prior research showing that overdose death rates (overall and for each substance type) increased dramatically from 2000 to 2015. Average total county overdose death rates increased threefold, rising from approximately 4.1/100,000 in 2000 to more than 13/100,000 by 2015. Overdoses for each specific substance type also increased, but the size and timing of these increases varied by drug type. For example, natural opioid death rates rose from .68 in 2000 to 4.1 in 2015 (a 6-fold increase), with most of the increase occurring before 2010 and tapering off by 2015. Cocaine death rates were lower but nearly doubled during this period. Heroin and synthetic opioid death rates both increased nearly 10-fold from 2000 to 2015 (rising from .18 and .27 to 2.0 and 2.5, respectively), with most of these increases occurring between 2010 and 2015. Notably, this aligns with prior research indicating that deaths from heroin and synthetic opioids (such as fentanyl) occurred later in the overdose crisis after prescription painkillers became more tightly controlled (Ciccarone 2019; Pitt et al. 2018). 14
Descriptive Statistics for Dependent and Explanatory Variables, 2000 to 2015.
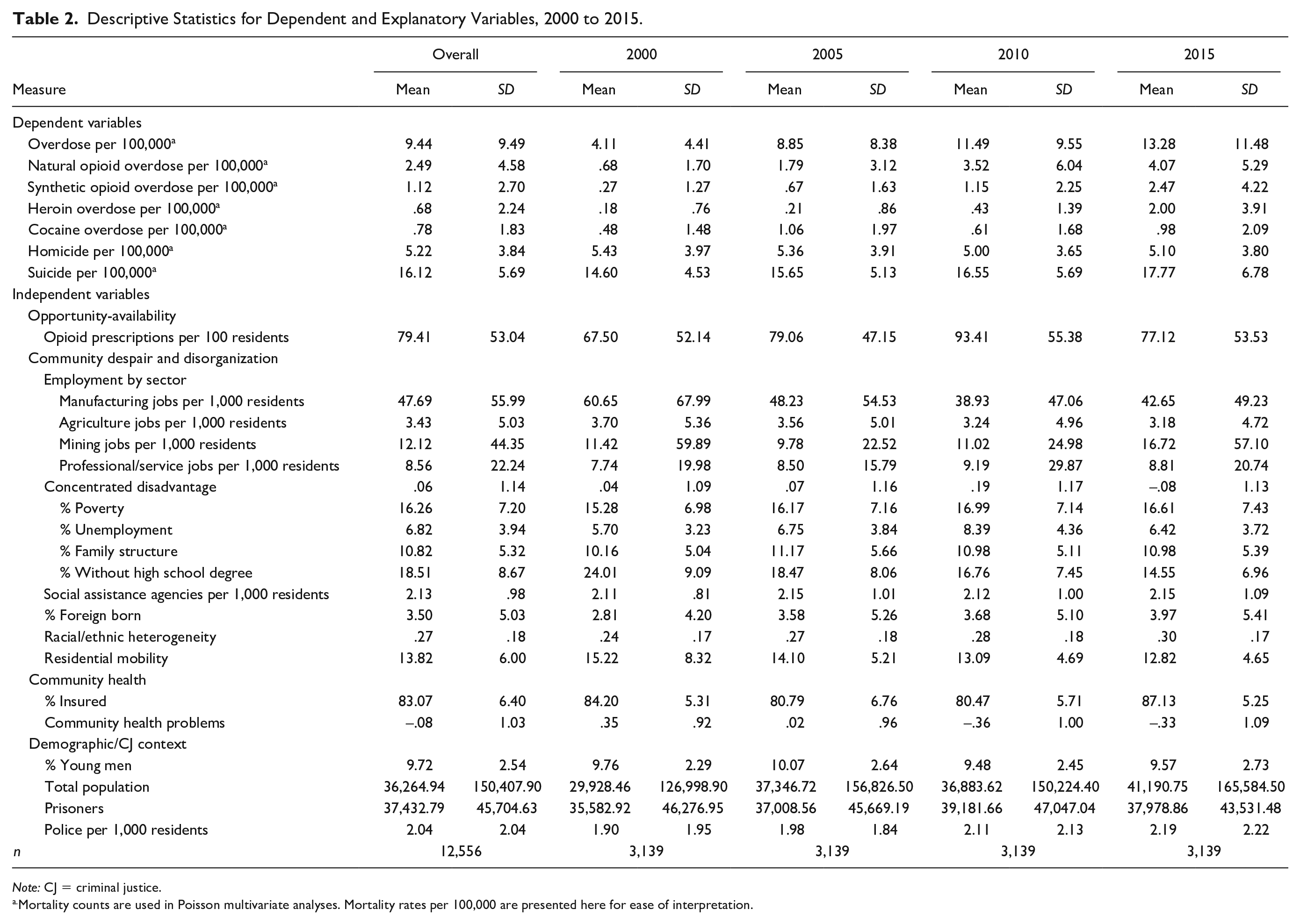
Note: CJ = criminal justice.
Mortality counts are used in Poisson multivariate analyses. Mortality rates per 100,000 are presented here for ease of interpretation.
Table 2 shows that average county suicide rates also rose (though more modestly) during this period, increasing from 14.6/100,000 in 2000 to 17.8/100,000 by 2015. In contrast, average county homicide rates remained fairly stable throughout this period at approximately 5/100,000. In addition, it is important to note that each of these forms of mortality vary widely across counties. Although some counties experienced few or no deaths from drug overdoses, suicides, and homicides, other counties experienced mortality rates that were more than three times the national average for one or more of these causes of death.
Table 2 also shows several noteworthy patterns and trends in our predictors, which align with the leading theories of overdose described earlier. As the opportunity and availability perspective highlights, opioid prescription rates rose from 67.5/100 persons in 2000 to a high of 93.4/100 in 2010 (nearly one opioid prescription per person) but then fell to 77/100 by 2015.
Average county rates of poverty, unemployment, and female-headed households with children (measures in our disadvantage index) also rose from 2000 to 2010, a finding that aligns with the communities of despair perspective and which may reflect declining economic prospects occurring during the early twenty-first century. There were also key shifts in employment sectors during the study period. Mining employment increased slightly from 2000 to 2015, but manufacturing employment saw steep (nearly 30 percent) declines. County levels of immigration and racial/ethnic diversity both increased from 2000 to 2015.
Last, measures of community health and health resources also changed in notable ways. County levels of health problems generally declined over time on the basis of our health index measure. In addition, the percentage of people with health insurance dropped slightly from 84 percent in 2000 to about 80 percent in 2005 and 2010 but then rose to 87 percent in 2015.
Multivariate Results: Between-County Effects
Overdose Deaths
Table 3 provides results of the random-effects portion of the analysis and describes the relationships between ecological contexts and mortality patterns between counties. In line with the opportunity-availability perspective, counties with higher opioid prescription rates have significantly higher levels of overdose deaths overall (b = 0.004, p < .001) and for each of the four specific substance types examined here. Because of the scale of our opioid prescription variable (prescriptions per 100 residents), the IRR values appear small. However, they are more substantively meaningful when one considers large increases in prescriptions (rather than a simple “1 unit” increase). For example, the IRR values indicate that an increase of 10 opioid prescriptions per 100 residents is linked to about 4 percent higher overdose deaths overall (IRR = 1.004) and between 3 percent and 5 percent higher overdose deaths for each of the specific substances examined (net of controls).
Poisson Between-County (Random) Effects of County Context on Overdose, Homicide, and Suicide Counts, 2000 to 2015.
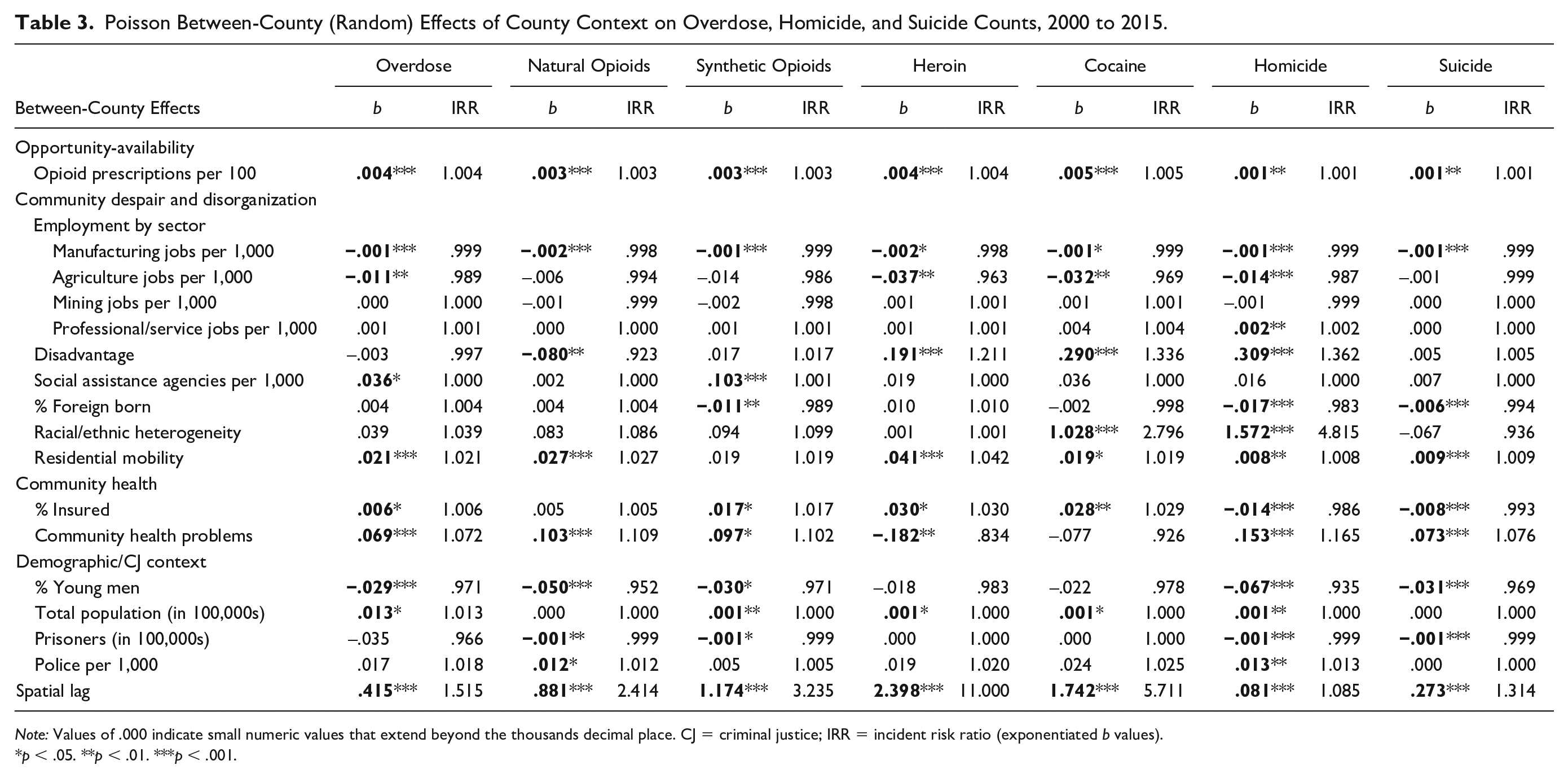
Note: Values of .000 indicate small numeric values that extend beyond the thousands decimal place. CJ = criminal justice; IRR = incident risk ratio (exponentiated b values).
p < .05. **p < .01. ***p < .001.
Table 3 also shows that multiple measures of county social and economic conditions (drawn from the communities of despair perspective) are linked to overdose deaths. The most consistent effects are observed for manufacturing employment, agricultural employment, and residential mobility. Table 3 indicates that counties with larger manufacturing employment sectors (net of broader disadvantage) have significantly fewer overdose deaths overall and for nearly all substances compared with counties with fewer jobs in this sector. Agricultural employment is associated with lower overdoses overall and for heroin and cocaine. In addition, counties with more residential mobility have higher levels of overdose deaths for all substances examined (except for synthetic opioids).
Other measures of social and economic conditions have more varied effects on overdose deaths across substance types. County levels of disadvantage are associated with greater heroin and cocaine overdoses (b = .191 [p < .001] and b = .290 [p < .001], respectively) but fewer natural opioid overdose deaths (b = −.080, p < .01). Counties with higher levels of immigration have fewer synthetic opioid overdoses but no significant associations with other overdose categories. Racial/ethnic heterogeneity is associated with more cocaine overdoses. In addition, the presence of social assistance agencies is linked to higher overdoses overall and for synthetic opioids but not for the other substances examined.
Drawing from the community health problems perspective, Table 3 shows that counties with greater health problems (measured with our health problems index) have more overdose deaths overall (b = .069, p < .001) and for both natural and synthetic opioid categories, but fewer deaths from heroin overdoses. Notably, the IRR values indicate that a one-unit increase in the county health index is associated with 7 percent greater total overdoses and approximately 10 percent to 11 percent greater overdose deaths for natural and synthetic opioids (but 17 percent lower levels of heroin overdoses). County health insurance rates are also linked to higher levels of overdose deaths overall and for all substances examined here other than natural opioids.
With respect to our control variables, counties with larger populations have higher levels of overdose deaths for nearly all substances, perhaps reflecting more urbanized areas where overdoses (particularly for heroin and cocaine) may be more common (Ciccarone 2019). Counties with larger shares of young men tend to have significantly lower levels of mortality for most overdose categories. Last, our spatial lag measures have strong and significant effects on each of the overdose categories, indicating that county overdose deaths are closely associated with those of neighboring counties and that there may be potential spillover effects in overdose.
Homicide and Suicide Comparisons
We now turn to our comparisons with models of homicide and suicide. Notably, correlation coefficients show that homicide and suicide are correlated with county overdose death rates at r = .17 and r = .25, revealing some preliminary indication of overlap in each of these forms of mortality (not shown). Likewise, Table 3 shows several similarities in their determinants of death. Similar to the overdose models, counties with higher opioid prescription rates have significantly higher levels of homicide and suicide, net of other factors. Manufacturing employment is again among the most consistent predictors and is linked to lower mortality for all forms of death examined here. Similar to its effect on overdoses, counties with greater residential mobility have higher levels of both homicide and suicide deaths net of controls. In addition, county health problems have fairly consistent effects across mortality type and are linked with higher levels of overdose, homicide, and suicide. Population size is linked to higher county levels of homicide and several forms of overdose (but not suicide). Likewise, the percentage of young men in the population is linked to fewer homicide, suicide, and overdose deaths.
Notably, there are also some key differences in the predictors of homicide and suicide compared with those for overdose deaths. Counties with higher immigration rates have significantly lower levels of homicide and suicide deaths, but effects of immigration are generally null for overdose deaths (other than for synthetic opioids). Disadvantage is associated with higher levels of homicide, heroin, and cocaine overdose deaths but is not significantly associated with suicide and several other forms of overdose mortality. Health insurance rates are linked to lower levels of homicide and suicide but greater overdose deaths for most substances examined. In addition, several other variables have generally inconsistent or mostly null effects across types of death, such as racial/ethnic heterogeneity and mining employment.
Multivariate Results: Within-County Effects
Overdose Deaths
We turn next to the within-county (fixed effects) portion of the hybrid models in Table 4, which show how changes in ecological conditions are related to within-county changes in overdose (and homicide and suicide) from 2000 to 2015. Focusing first on opportunity-availability, Table 4 shows that changes in county opioid prescription rates are associated with increases in county levels of overdose deaths overall (b = 0.001, p < .01) and for both natural (b = 0.002, p < .01) and synthetic opioids (b = 0.002, p < .01), but not for heroin or cocaine.
Poisson Within-County (Fixed) Effects of County Context on Overdose, Homicide, and Suicide Counts, 2000 to 2015.

Note: All models include county and time fixed effects. Values of .000 indicate small numeric values that extend beyond the thousands decimal place. CJ = criminal justice; IRR = incident risk ratio (exponentiated b values).
p < .05. **p < .01. ***p < .001.
Turning to social and economic measures (and the communities of despair perspective), we again find that manufacturing employment has generally consistent effects on county overdose concentrations. Table 4 shows that rises in county manufacturing employment are linked to declines in total overdose deaths (b = −0.002, p < .05) and overdose deaths from both natural opioids (b = −0.003, p < .05) and synthetic opioids (b = −0.002, p < .01). Conversely, these effects also indicate that declines in manufacturing jobs (net of changes in the disadvantage index) are associated with increases in overdose deaths. Because of the scale of the manufacturing variable in Table 4 (shown in jobs per 1,000 residents), the IRR values for manufacturing effects may appear small. However, these effects are more substantively meaningful for larger changes in manufacturing employment rates (rather than a simple “one-unit” increase). Specifically, they suggest that an increase of 10 manufacturing jobs per 1,000 residents is related to 2 percent lower overdose deaths, and an increase of 100 manufacturing jobs per 1,000 residents is linked to more than a 20 percent decline in overdose deaths (overall and for both forms of opioids).
County population growth (on the basis of changes in the total population variable) is also among the most consistent predictors of overdose deaths. Table 4 shows that county population growth over time is associated with significant declines all forms of overdose deaths examined here. Conversely, this effect also indicates that counties with shrinking populations saw significant rises in all forms of overdose deaths.
Table 4 shows that increases in disadvantage are associated with rising overdose deaths overall (b = .104, p < .05) but not for any of the specific substances examined. Counties with growing immigrant populations and rising residential mobility have increased levels of synthetic opioid overdose deaths. Racial/ethnic heterogeneity is linked to rising heroin overdoses. In addition, increases in the presence of social assistance agencies are associated with greater overdose deaths overall and for both forms of opioids.
Drawing from the community health problems perspective, Table 4 shows that shifts in county health problems (on the basis of our health index measure) are associated with rising county levels of overdose deaths overall (b = .156, p < .05). Specifically, the IRR values indicate that a one-unit increase in our community health problem index is associated with approximately a 17 percent rise in overdose deaths. However, increases in county health problems are associated with declines in synthetic opioid deaths. Notably, insurance coverage rates are not significantly related to any of the overdose deaths examined in the fixed-effects models.
Increases in the share of young males in the population and in incarceration are associated with rising natural opioid overdoses (and cocaine and synthetic opioid deaths, respectively). In addition, the spatial lag variables are again consistently significant, indicating that increases in overdose deaths in neighboring counties are associated with significant growth in county overdose deaths overall and for each substance from 2000 to 2015.
Homicide and Suicide Comparisons
For comparison, we examine within-county models of homicide and suicide. Table 4 shows that manufacturing employment again has some of the most consistent effects across mortality types. Increases in manufacturing employment are associated with declining levels of homicide, suicide, and multiple forms of overdose deaths. Similarly, population growth (on the basis of the total population variable) is also among the most consistent predictors of mortality. County population growth is associated with lower levels of death for homicide, suicide, and all forms of overdose examined here. Conversely, this finding indicates that counties with declining populations saw significant increases in each of these forms of mortality.
Increases in opioid prescription rates are associated with rising levels of suicide and overdoses overall and for both forms of opioids. However, opioid prescriptions are not linked to homicide or overdose deaths from heroin or cocaine in these models. Rising levels of disadvantage are linked to increasing homicide and total overdose deaths, but not to suicide or other forms of overdose. In addition, increases in county health problems are associated with rising deaths from homicide, suicide, and total overdoses (but declines for synthetic opioids).
At the same time, several other ecological factors have unique effects on homicide and suicide that differ from those observed for overdose. For example, increases in immigration are associated with declining suicide deaths but increased synthetic opioid deaths. In addition, racial/ethnic heterogeneity is associated with rising county levels of suicide (and heroin) deaths but it is not associated with homicide or other forms of overdose.
In sum, the within-county effects described above show that some ecological factors, such as manufacturing employment rates and population growth are consistent determinants of county-level deaths for nearly all forms of mortality examined here. Changes in opioid prescription rates, community health problems, and disadvantage are also linked to multiple mortality patterns, with some variation across models and type of death. However, there are also several differences in predictors of within-county changes in mortality for overdose versus homicide and suicide.
Summary of Results
Taken together, these findings provide some support for each of the three leading theories of overdose. However, some factors clearly have more consistent effects on overdose deaths that also extend to homicide and suicide mortality. Table 5 provides a summary of effects from all models to help illustrate consistencies (and differences) in effects. Table 5 shows that manufacturing employment, population decline, and opioid prescription rates are among the most consistent predictors of overdose, homicide, and suicide deaths, followed by community health problems, residential mobility, and disadvantage (with less consistency in effects of these latter variables).
Summary of Significant Effects from Multivariate Analysis.

Note: Plus signs denote significant positive effects, and minus signs denote significant negative effects.
Supplemental Analyses
To fully exhaust the data and assess the robustness of our findings, we conducted an extensive series of supplemental analyses using different modeling specifications and alternative variables. We replicated all models using hybrid regression models with square root transformed dependent variables (rather than Poisson models) to adjust for skewness in mortality measures. Although there were some differences across models (a few coefficients dropped in or out of significance and effects of opioid prescriptions were less consistent in fixed-effects models), the substantive results generally mirrored findings from our main models. Results of this analysis are presented in the Appendix.
Our main analysis includes all counties in the United States, which provides greater generalizability of findings. However, the trade-off of examining all counties is that small counties with few residents may produce unreliable estimates in mortality measures and large fluctuations from year to year. To explore this possibility, we replicated all models using population cutoffs to include only those counties with at least (1) 5,000 and (2) 10,000 residents. Results of these alternative models were similar to our main analysis. As noted earlier, we also estimated models using several alternative measures of county health problems (different versions of the health problem index) and drug availability (using DEA ARCOS data on distribution of controlled substances). Results obtained with the alternative variables were consistent with those shown here. 15
Last, we included several interaction terms to assess whether effects of our predictors were conditioned by other county characteristics (i.e., interactions between opioid prescription rates, disadvantage, manufacturing jobs, and spatial lags). Although most of these effects were not significant, interactions between spatial lag measures and both disadvantage and opioid prescription rates were significant, suggesting that disadvantage and drug availability may have stronger effects when they are located near counties with high levels of overdose, homicide, or suicide. Although it is beyond the scope of the present study to thoroughly explore each of these effects, it raises important questions for future research discussed in the following section.
Discussion
The epidemic of fatal drug overdoses in the early twenty-first century is marked by a salient sociological reality: wide community variation in the toll of overdose deaths. To address this issue, the present study contributes to extant research by examining the macro-level predictors of overdose deaths (overall and by substance type) covering the period from 2000 to 2015. In addition, to assess whether there are general “determinants of death” across communities, we compared the community correlates of overdose deaths with those of homicide and suicide. Drawing from leading macro-level theories of overdose, we specifically examined the ways in which overdose, homicide, and suicide deaths are linked to county-level patterns of (1) “(drug) opportunity and availability,” (2) “community despair” (and disorganization), and (3) “community health problems.” The findings concerning these explanations, similarities in the community determinants of death, and avenues for future research are summarized below.
Explaining Overdose Deaths
As described in the preceding sections, considerable debate remains about the precise mechanisms and contextual factors that shape community concentrations of overdose. Although some studies suggest that social-economic conditions and community health problems are key sources of overdose concentrations (e.g., Monnat 2018, 2019; Peters et al. 2020; Rosenfeld et al. 2021; Thombs et al. 2020), questions remain about the precise factors that predict community overdose patterns. In addition, other studies suggest that these factors have little impact or instead suggest that drug supply measures are more important (e.g., Currie and Schwandt 2020; Ruhm 2019; Siddiqi et al. 2019; see review in Maclean et al. 2020).
Although each of the three leading theoretical perspectives on the overdose crisis have value, a few theoretically derived factors clearly carried more weight than others and had more consistent effects on county overdose deaths in our analysis. First, drawing from “opportunity and availability” perspectives, we found that opioid prescription rates were among the most consistent predictors of overdose deaths. Second, drawing from “communities of despair” perspectives, measures of manufacturing employment losses and population decline (and residential mobility and disadvantage to a lesser degree) were particularly consistent predictors of overdose concentrations. Notably, the manufacturing and population loss effects exist net of county changes in disadvantage, suggesting that shifts in manufacturing employment and population loss have particularly salient effects on overdose deaths, over and above broader patterns of economic decline. Finally, “community health problems” were also closely associated with county overdose concentrations. Consistent with emerging research, these findings link macro-level patterns of overdose deaths to both supply-side and demand-side factors (Monnat 2018, 2019; Peters et al. 2020; Rosenfeld et al. 2021). In sum, our findings indicate that concentrations of overdose deaths are made possible by a combination of drug availability (supply side) and factors that create a propensity to consume drugs (demand side).
General Explanations and Determinants of Death
Our results also hold key implications for ecological research and theories exploring whether multiple forms of mortality are shaped by similar sets of predictors or community “determinants of death.” Drawing from the work of Case and Deaton (2015, 2017), researchers have observed close connections between several different types of “deaths of despair,” which include overdose and suicide. The assumption of this categorization is that these forms of mortality occur in similar places and are driven by the same sets of underlying factors. In many ways, the “deaths of despair” perspective echoes the central tenets of the Chicago School of sociology, which found that myriad social problems (including crime, violence, infant mortality, tuberculosis, and mental illness) occurred in the same set of Chicago neighborhoods and were driven by the same ecological conditions (Shaw and McKay 1942; Wilcox et al. 2018). Although these perspectives are separated by nearly 100 years, they offer a similar theoretical storyline about the ecology of social problems—there is something about place that tends to concentrate multiple social problems in some communities and not others.
Our findings offer support for these positions and indicate that there is overlap in the determinants of death for overdose, homicide, and suicide. Opioid prescriptions are associated with higher levels of overdose deaths as well as greater homicide and suicide, suggesting that drug availability contributes to multiple fatal social problems (not just overdoses). We find that the variable of manufacturing job losses also has particularly consistent effects and is associated with rising levels of death for nearly all types of mortality examined here. Again, we note that these effects exist net of broader community disadvantage levels, suggesting that the loss of manufacturing employment matters above and beyond other measures of economic decline. This finding closely aligns with the “deaths of despair” perspective, which suggests that economic restructuring and shifts in U.S. labor, wages, and community institutions occurring since the late twentieth century have contributed to multiple forms of mortality (Case and Deaton 2015, 2017). Research on overdose has offered growing support for these macroeconomic arguments, highlighting a variety of social and economic problems associated with overdose deaths (e.g., income inequality, disadvantage, median home prices, and declines in manufacturing and trade-related jobs) (see Brown and Wehby 2017; Dean and Kimmel 2019; Monnat 2019; Peters et al. 2020; Thombs et al. 2020; Venkataramani et al. 2019). However, our findings suggest that manufacturing job losses may have had particularly profound effects on overdose mortality (overall and across substances) and that these effects extend to both homicide and suicide. In addition, our results indicate that community health problems and population decline are also linked to multiple forms of mortality. Again, these results align with the “deaths of despair” perspective and related social-economic positions that suggest that factors such as population loss, rising economic deprivation, and the presence of persistent health problems may have general effects that contribute to concentrations of multiple fatal social problems in some communities.
However, there are also some differences in predictors of homicide, suicide, and overdose, which suggest that the ecological predictors of these forms of mortality may overlap but are not identical. For example, health insurance coverage was linked to lower levels of homicide and suicide but higher levels of overdose. In addition, immigration and racial/ethnic heterogeneity have more consistent effects on homicide and suicide than on overdose deaths. Prior research has consistently shown that these factors are associated with macro-level patterns of crime and violence (see Pratt and Cullen 2005; Wilcox et al. 2018), but it was not clear whether these ecological conditions would predict other fatal social problems equally well.
Policy and Prevention
Our results also carry key implications for public policy and efforts aimed at combatting community concentrations of overdose. To date, prevention strategies among state and federal governments have often centered around reducing drug availability and opportunity (e.g., reducing prescriptions, targeting drug manufacturers, increased drug enforcement, implementing prescription monitoring programs). This is a necessary and important step in combating the overdose crisis. As our findings show, opportunity and drug supply matter, and curbing availability of dangerous substances may be key to reducing overdose deaths. However, our findings suggest that additional strategies aimed at reducing demand and propensity for overdose—such as addressing manufacturing job losses, structural disadvantages, and underlying health problems within locales—may be equally important in reducing overdose concentrations.
Policy and prevention efforts addressing these social and economic risk factors can be messier than policies targeting drug supply. Large-scale social and economic programs are often harder to implement and are less politically appealing. It can also be more difficult to assess their effectiveness in reducing the overdose problem. However, the fact that they are not easy solutions does not mean that they should be ignored. In their influential work on the “deaths of despair,” Case and Deaton (2015, 2017) suggested that addressing larger social and economic problems cannot be overlooked in efforts to combat overdose and suicide mortality. Or as Koller (2019) noted, “all of the resources we can muster to address the epidemic of opioid deaths that has captured headlines and the attention of politicians will be ineffective unless paired with the economic and social equivalent of public health prevention.” On the basis of the present findings, we agree. Thus, we encourage policy and prevention efforts to continue to explore ways in which both the supply-side and demand-side sources of overdose deaths may be addressed. Importantly, given the similarity in some determinants of death for overdose, homicide, and suicide, ameliorating one problem may have spillover effects that reduce other forms of death.
Future Research
Although the present study makes important contributions to research and knowledge on the ecological sources of overdose deaths, future research would benefit from attending to three areas. First, although this analysis includes an extensive set of macro-level variables, our list of predictors is far from exhaustive. Given data restrictions, it is impossible for a single study to account for all ecological factors that might be associated with overdose rates (and homicide and suicide), while also examining these relationships over time. However, as more data become available, future research should incorporate additional ecological factors and examine additional time points. As several scholars have noted (Case and Deaton 2015; Denney et al. 2013), the economic decline leading to community “despair” began well before the present study period. Thus, future research should extend this analysis to assess whether community overdose concentrations differ for places with long-standing economic declines versus those with more recent rises in economic and social despair. As in most macro-level analyses of overdose, we were unable to measure the availability of illegal substances, which we acknowledge as a key limitation. Additional analyses that capture other sources of drug availability (especially illegal distribution) are essential for providing a more nuanced analysis of supply-side influences. Likewise, measures of naloxone availability and access to drug treatment and mental health resources were not available across counties for all years of our investigation. Future research should also explore how social capital, social isolation, and social support systems shape these forms of mortality.
Second, the use of counties as a study unit has advantages as well as disadvantages. Counties provide complete coverage of the United States and incorporate both rural and urban communities, which is advantageous. However, they are also large in terms of geographic area and population size. Future research that replicates the present analysis for alternative study units and especially smaller, neighborhood- or place-level analyses is essential for addressing these caveats. Such analyses could better incorporate community-level mechanisms that may shape overdose, homicide, and suicide mortality (e.g., collective efficacy, social ties, informal social control) (Sampson et al. 1997; Wilcox et al. 2018). In addition, future research is needed that explores how larger state-level policies and priorities also shape county-level or more localized concentrations of overdose.
Third, the present analysis provides an important assessment of the macro-level determinants of overdose, homicide, and suicide deaths, but there is reason to expect that findings may differ across demographic groups and across different geographic contexts. Research on the overdose epidemic has increasingly shown that overdose risks vary widely across race/ethnicity, age, gender, and combinations of these groupings (e.g., Peters et al. 2020; Rosenfeld et al. 2021). Likewise, overdose patterns (along with suicide and homicide) differ sharply across regions of the U.S. and for rural versus urban locales (Hedegaard et al. 2018; Monnat 2019). Assessing whether the community sources of overdose, homicide, and suicide differ across these demographic groups and contexts is an important avenue for further inquiry.
Going forward, it is critical that research addresses these caveats and questions in order to obtain a more complete understanding of the overdose crisis and the ecological determinants of death across communities and mortality type. Notably, this is particularly important given growing indications that overdose, homicide, and suicide mortality have all escalated during the coronavirus (COVID-19) pandemic. Prior to the pandemic, overdose deaths had begun to level off, and efforts to combat overdose mortality seemed to be making headway. However, projections now suggest that the social isolation and both social and economic problems associated with the COVID-19 pandemic may result in more than 75,000 additional “deaths of despair” from overdose, suicide, and related forms of death (Petterson, Westfall and Miller 2020). In addition, research indicates that many communities have begun to see surges in homicide and violent crime as the pandemic progressed (Rosenfeld et al. 2021). In light of these observations, identifying the underlying ecological sources of overdose concentrations is an essential step to help aid at-risk communities and reduce the devastating consequences of this epidemic. Clearly, much more work is needed to fully understand the community sources of overdose deaths, both alone and compared with those of homicide and suicide. However, it is our hope that the present study provides an important contribution to this line of work and fosters additional research exploring the ecological determinants of deaths across different communities and forms of mortality.
Supplemental Material
sj-docx-1-srd-10.1177_23780231221100392 – Supplemental material for The Community Determinants of Death: Comparing the Macro-Level Predictors of Overdose, Homicide, and Suicide Deaths, 2000 to 2015
Supplemental material, sj-docx-1-srd-10.1177_23780231221100392 for The Community Determinants of Death: Comparing the Macro-Level Predictors of Overdose, Homicide, and Suicide Deaths, 2000 to 2015 by Ben Feldmeyer, Francis T. Cullen, Diana Sun, Teresa C. Kulig, Cecilia Chouhy and Michael Zidar in Socius
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This material is based upon work supported by the National Science Foundation under grant 1849209. Any opinions, findings, and conclusions or recommendations expressed in this material are those of the authors and do not necessarily reflect the views of the National Science Foundation.
Supplemental Material
Supplemental material for this article is available online.
1
Deaths of despair commonly refers to deaths from drug overdoses, suicide, and alcohol (Case and Deaton 2015, ![]() ). Although we do not examine alcohol-related deaths, we use the term deaths of despair when discussing mortality from overdose and suicide.
). Although we do not examine alcohol-related deaths, we use the term deaths of despair when discussing mortality from overdose and suicide.
2
Our focus here is on the theories and predictors of overdose and whether they apply to other fatal social problems. It is beyond the scope of this analysis to simultaneously test all available macro-level theories of crime, suicide, and overdose. We are unable to measure all of the factors associated with those theories (e.g., collective efficacy, social ties, social cohesion/support, institutional anomie), nor did we develop our data and measures to do so. Instead, our data and measures were designed specifically to address the leading macro-level theories of overdose. However, we encourage future research to provide more explicit assessments of whether criminological and sociological theories of crime and suicide apply to overdose deaths.
3
Although it was not their main focus, ![]() also provided a comparison of overdose and suicide rates over time in their appendices. Their findings showed some differences in suicide and overdose trends, indicating that overdose rates escalated more rapidly than suicide rates in states without more restrictive “triplicate” prescription drug monitoring programs.
also provided a comparison of overdose and suicide rates over time in their appendices. Their findings showed some differences in suicide and overdose trends, indicating that overdose rates escalated more rapidly than suicide rates in states without more restrictive “triplicate” prescription drug monitoring programs.
4
At the time of our analysis, variables for the 2020 period (the next five-year interval) were available for the CDC MCOD mortality data but were not yet available for many of the predictors of interest (e.g., ACS five-year census estimates, CDC opioid prescription data, health insurance coverage rates, employment rates by sector, IHME county profile data). Thus, our analysis covers the period from 2000 to 2015, which offers more complete data coverage.
5
All mortality counts are based on the CDC’s restricted-access MCOD mortality data, using the underlying cause of death recorded for the deceased. Homicide and suicide data were downloaded directly from IHME county profile data, which use advanced estimation procedures to adjust for “garbage categories” and for errors in the MCOD data that may result in misclassifications of homicide and suicide deaths (see Dwyer-Lindgren et al. 2016, ![]() ).
).
6
Mortality counts were based on underlying cause of death codes in MCOD data, following categorizations used in CDC calculations and prior research (e.g., Dwyer-Lindgren et al. 2018; Hedegaard et al. 2018; Peters et al. 2020; ![]() ): overdose, X40 to X44, X60 to X64, X85, and Y10 to Y14; homicide, X85 to Y08.9 and Y87.1; and suicide, X60 to X84.9 and Y87.0. Overdose deaths from specific substances are identified on the basis of the aforementioned underlying causes of death and the following multiple-cause-of-death codes from the International Statistical Classification of Diseases and Related Health Problems, 10th Revision (1999–2016): heroin, T40.1; natural and semisynthetic opioids, T40.2; synthetic opioids excluding methadone, T40.4; and cocaine, T40.5.
): overdose, X40 to X44, X60 to X64, X85, and Y10 to Y14; homicide, X85 to Y08.9 and Y87.1; and suicide, X60 to X84.9 and Y87.0. Overdose deaths from specific substances are identified on the basis of the aforementioned underlying causes of death and the following multiple-cause-of-death codes from the International Statistical Classification of Diseases and Related Health Problems, 10th Revision (1999–2016): heroin, T40.1; natural and semisynthetic opioids, T40.2; synthetic opioids excluding methadone, T40.4; and cocaine, T40.5.
7
County opioid prescription data were available for 2006 to 2017. Estimates for year 2000 and 2005 prescriptions were interpolated on the basis of average annual changes observed in the available data. In preliminary analyses, we used year 2006 estimates as a proxy for 2005 (rather than interpolated 2005 estimates), which did not change the results.
8
Annual ACS data were used in combination with year 2000 and 2010 data to interpolate year 2005 estimates (for similar applications using interpolation for intercensus years, see Ousey 2017; ![]() ). Factor loadings for variables included in the disadvantage index all exceeded .5, indicating that they loaded onto a single underlying construct.
). Factor loadings for variables included in the disadvantage index all exceeded .5, indicating that they loaded onto a single underlying construct.
9
IHME data provide several additional county health measures, including rates of various forms of cancer, diabetes, asthma, and rates of smoking (among others). We created several alternative county health indices using these measures in preliminary analyses. Results obtained using these alternative health indices were nearly identical to those shown in the present analysis.
10
Measures of county population and percentage young men were drawn from U.S. census data (decennial and ACS). Police presence data were drawn from the Federal Bureau of Investigation’s UCR: Police Employee data for 2000 to 2015. Incarceration measures were drawn from BJS National Prison Statistics for 2000 to 2015.
11
Inspection of our data showed no signs of nonlinearity in the relationships between population size and mortality rates, suggesting that log transformation of population size was not required. However, we reran all models using logged population size as a robustness check. Effects of logged county population were consistent with the findings presented in our present models, and the substantive results for other variables were similar to those presented here.
12
Multiple imputation estimates were created using multivariate normal regression procedures with 10 iterations. Results using alternative multiple imputation estimates (e.g., Markov-chain Monte Carlo methods, 20 iterations) and casewise deletion were similar, but effects of opioid prescriptions and professional and service sector jobs were less consistent across substance-specific models when using casewise deletion, perhaps because of the reduced sample and statistical power.
13
In supplemental analyses, we also examined hybrid Poisson regression models using age-adjusted mortality rates, instead of counts. However, models for homicide, suicide, and total overdose would not converge in Stata when using rates. Thus, we rely Poisson models of death counts using total population as the exposure variable.
14
Some of the rising trends in overdose deaths highlighted here may reflect increased recording of overdose mortality. However, research also suggests that large numbers of overdose deaths may still be underestimated, especially for opioid-related deaths (see Buchanich et al. 2018; ![]() ). As such, research indicates that these trends reflect real rises in overdose deaths, with some studies suggesting that overdose trends may be even worse.
). As such, research indicates that these trends reflect real rises in overdose deaths, with some studies suggesting that overdose trends may be even worse.
15
DEA ARCOS data were obtained from the Washington Post data archives, covering 2006 to 2012. As a result, ARCOS measures were available for only two time points of our analysis (2005 and 2010), which reduced the fixed-effects analysis to only two observations per county. Measures obtained from the ARCOS data were highly collinear with measures of opioid prescriptions (r > .80) and produced similar effects to those observed for opioid prescriptions.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.