
Abstract
Despite numerous studies on educational disparities in U.S. adult health, explanations for the disparities and their growth over time remain incomplete. The authors argue that this knowledge gap partly reflects an individualist paradigm in U.S. studies of educational disparities in health. These studies have focused largely on proximal explanations (e.g., individual behaviors) to the neglect of contextual explanations (e.g., economic policies). The authors draw on contextual theories of health disparities to illustrate how U.S. states, as institutional actors, shape the importance of education for health. Using two nationally representative data sets and seven health measures for adults aged 45 to 89 years, the authors show that the size of the educational gradient in health varies markedly across states. The size varies because of variation in the health of lower educated adults. The authors use state excise taxes on cigarettes to illustrate one way states shape educational disparities in health. These findings underscore the necessity of contextualizing these disparities.
Why do U.S. adults with more years of education have better health than their peers with less education, and why has this disparity grown in recent decades? Hypotheses typically point to the ways in which more years of schooling provide individuals the agency and resources to secure good jobs, avoid financial hardship, create healthy lifestyles, and develop salubrious social ties. Although these individual-level explanations are important, they account for only part of the association and its growth over time (e.g., Cutler and Lleras-Muney 2008). We propose that existing explanations are incomplete in part because of the dominance of the individualist paradigm in U.S. studies of educational disparities in health. These studies have focused almost exclusively on individual-level (agentic) explanations for educational disparities in health to the neglect of contextual-level (structural) explanations. This is a surprising oversight given that key perspectives for elucidating health disparities in general—for example, the theory of fundamental social causes (Link and Phelan 1995), socioecological frameworks (Diderichsen, Evans, and Whitehead 2001), institutional theories of health inequality (Beckfield et al. 2015; Beckfield and Krieger 2009), and constrained choices (Bird and Rieker 2008)—emphasize the importance of social and political contexts in creating health disparities.
We draw on these perspectives to develop a contextual framework for understanding educational disparities in U.S. adult health and their growth over time. In many ways, our aim is similar to Cockerham’s (2005) in his construction of health lifestyle theory. That is, we develop a framework that “includes considerations of both agency and structure, with an emphasis upon restoring structure to its appropriate position” (p. 51). In this article, we first develop the argument that U.S. states are an important institutional context in the production of educational disparities in health and that state contexts differ in ways that should influence adult health. Next, we use two nationally representative data sets to show that educational disparities in a range of health outcomes vary across states. We then show an example of an important policy mechanism (state excise taxes on cigarettes) through which states ought to shape the disparities, to illustrate the value of contextualizing these disparities.
This article heeds the call from Link and Phelan (1995) that medical sociologists and social epidemiologists need to counter the trajectory of modern epidemiology toward identifying risk factors that are increasingly proximate to disease—ones for which “biological plausibility” can be argued. One way they can do this is by “contextualizing” individually-based risk factors. (p. 84)
Indeed, our findings support the view that the association between education and health is not simply a reflection of higher educated adults possessing certain characteristics and greater agency; the association also reflects the ways in which contexts make one’s education important (or not) for obtaining resources and avoiding risks.
Background
Educational Attainment, Fundamental Causes, and Adult Health
Educational attainment is one of the strongest social determinants of health among U.S. adults (e.g., Galea et al. 2011). Higher educated adults experience better overall health and fewer chronic conditions such as diabetes, cognitive limitations, and physical disability (see review in Montez and Friedman 2015). Higher educated adults tend to live longer and spend a greater portion of their years in good health (Montez and Hayward 2014). The educational gradient in health and mortality has grown since the early 1980s (Goesling 2007; Hayward, Hummer, and Sasson 2015; Masters, Hummer, and Powers 2012; Miech et al. 2011).
What explains educational disparities in health and their growth over time among U.S. adults? The conceptual framework frequently drawn on is the theory of fundamental social causes (Link and Phelan 1995; Phelan and Link 2005), denoted here as FCT. It posits that social disparities in health exist when resources that can be used to prevent disease and premature death (e.g., money, power, social connections) are unevenly distributed in the population. In the United States, these resources are unevenly distributed by educational attainment (and by other social categories such as race and gender). As societies develop health-beneficial technology and new information arises, disparities in health widen when advantaged individuals are more likely to have access to and benefit from these resources (e.g., Baker et al. 2017). Disparities can potentially shrink to a small, stable level as these health-related resources become more universally distributed (Clouston et al. 2016).
Within the context of FCT, scholars have focused on three types of resources to explain the health advantage of higher educated adults: economic well-being, psychosocial resources, and lifestyle behaviors (e.g., Lynch 2006; Ross and Wu 1995). For instance, higher educated adults are more likely to avoid financial hardship and be employed in jobs that are stable and fulfilling, all of which enhances health (Mirowsky and Ross 2007). They tend to possess a greater sense of personal control and beneficial social ties (Mirowsky and Ross 1998). They are more likely to exercise, avoid tobacco, drink alcohol in moderation, and maintain a healthy body weight (Pampel, Krueger, and Denney 2010). In addition, they are more likely to incorporate new health-related information into their lifestyles (Baker et al. 2017).
These explanations assume that the education-health association occurs in large part because of a causal effect of education on health. In addition, the association may partly reflect the selection of healthy individuals into higher education, as well as the existence of certain traits that lead to both higher education and better health. Although these additional processes are important to bear in mind, reviews of the evidence conclude that the direction of the association runs primarily from education to health (Hummer and Lariscy 2011; Mirowsky and Ross 2003; Montez and Friedman 2015).
As the discussion above illustrates, U.S. studies’ explanations for educational disparities in health have been conceptualized largely at the individual level. They have mostly overlooked the contextual conditions that undergird these disparities and their growth over time. 1 This is a surprising omission given that FCT emphasizes the importance of place and time in the emergence of health disparities (Link 2008; Phelan and Link 2005). The focus on individual-level, proximal mechanisms for educational disparities in health may reflect the dominant view in U.S. studies, whether implicit or explicit, that education is a personal resource. Consequently, U.S. studies of the education-health association have focused on agentic mechanisms: adults with more education are hypothesized to coalesce healthy lifestyles, seek out medical knowledge, avoid financial hardship, and so on. Although these explanations are important, they ignore the fact that individuals are embedded in historical, socioeconomic, and policy contexts that influence the extent to which education matters for health.
Contextualizing the Association between Education and Health
In contrast to U.S.-focused studies, research outside the United States often explicitly conceptualizes educational disparities in health as shaped by broader policy contexts (Bambra, Netuveli, and Eikemo 2010; Brennenstuhl, Quesnel-Vallée, and McDonough 2012; Cambois et al. 2016; Frohlich, Ross, and Richmond 2006; Mackenbach et al. 2008; Navarro and Shi 2001). This work tends to draw on FCT but also socioecological frameworks (Diderichsen et al. 2001; Solar and Irwin 2010) and institutional theories of health inequalities (Beckfield et al. 2015; Beckfield and Krieger 2009), thereby making the contextual component of FCT more prominent. Socioecological frameworks and institutional theories assert that contexts not only shape how resources are distributed in the population, they shape the importance of those resources for health via social, economic, and health policies. Relating these frameworks to educational disparities in health, they imply that although education varies in every population, this variation may be less consequential for health in contexts (e.g., countries, U.S. states) that, for example, offer strong safety nets, provide labor protections, subsidize child care, and impose strict controls on tobacco consumption.
Numerous studies have described marked cross-national differences in educational inequalities in health (e.g., Bambra et al. 2010; Cambois et al. 2016; Mackenbach et al. 2008). Many of these studies focus on Europe and categorize countries by welfare regime. Although there is no strong evidence that certain welfare regimes are associated with particularly small or large disparities in health, a systematic review by Brennenstuhl et al. (2012) found that about half of studies reported that health inequalities were smallest, or that population health was best, in social-democratic countries. Taken together, these studies indicate that the education-health association is not simply a reflection of higher educated adults possessing certain characteristics or greater agency; it is also a reflection of the ways in which contexts make education important (or not) for obtaining salubrious resources and avoiding risks.
The importance of contextualizing educational disparities in health is threefold. First, doing so expands the types of explanations that are investigated. Explanations are no longer limited to individual-level mechanisms; rather, they also encompass structural factors that create, maintain, and alter the disparities. Second, expanding the range of possible explanations also expands the range of possible strategies for reducing the disparities. Third, strategies that focus on contextual conditions may be more efficacious than those that focus on individual-level mechanisms. This last point is supported by both theory and evidence. Theory asserts that the “massive multiplicity of connections” (Lutfey and Freese 2005) between education and health at the individual level, combined with the shifting salience of those connections over time and place (Link and Phelan 1995), makes eliminating them particularly challenging. Evidence suggests that contextual solutions (e.g., water fluoridation) are more likely to reduce disparities than are individual-level solutions (e.g., encouraging people to brush and floss their teeth); the latter of which can unintentionally widen disparities because of factors such as uneven diffusion of information and technology (White, Adams, and Heywood 2009).
U.S. States as Context
Although research on Europe has focused on countries or welfare states as the key contextual level to elucidate educational disparities in health, our focus here is U.S. states. Like European countries, U.S. states vary in their policies, resources, and opportunity structures in ways that influence population health. Underscoring the decisive role that states play in nearly every aspect of our lives, Robertson (2012) wrote, The American states always have done most of the routine governing in the United States. State laws still regulate birth and death, marriage and divorce, crime and punishment, and commercial law, such as the purchase and sale of property. States manage education, prisons, highways, welfare, environmental protection, corporate law, and the professions. (p. 1)
As examples, U.S. states regulate approximately 20 percent of the U.S. economy, issue 90 percent of environmental permits, hold the majority of criminal trials, generate the majority of convictions, and are the “chief managers” of welfare and health services for the disadvantaged (Robertson 2012). In sum, states profoundly shape population health and its social determinants.
Even though states have always done the majority of routine governing, two parallel trends have made states an increasingly salient political actor since the late 1970s. The gradual decentralization of political authority from federal to state levels (sometimes referred to as devolution) gave states more discretion over funding certain programs such as welfare and Medicaid (Conlan 1998). In addition, the more recent proliferation of state preemption laws has prohibited or severely limited legislative authority at the local level. Many states now prohibit localities from enacting laws and ordinances such as requiring sprinklers in new homes, banning hydraulic fracking, imposing nutrition labeling in restaurants, enacting smoke-free laws, requiring paid sick days, raising the minimum wage, and much more (Riverstone-Newell 2017).
A robust literature has documented the population health consequences of states’ economic, social, and public health policies. Economic policies, such as state minimum wages and earned income tax credits (EITCs), help individuals avoid economic hardship and its health insults. For instance, raising the state minimum wage reduces postneonatal mortality (Komro et al. 2016), adolescent fertility (Bullinger 2017), and heart disease mortality among working age adults (Van Dykea et al. 2018). State EITCs elevate maternal employment rates and earnings and, partly as a consequence, increase birth weights (Strully, Rehkopf, and Xuan 2010). They are also associated with lower disability risk across the life course (Montez, Hayward, and Wolf 2017).
State policies also affect psychosocial resources. States decide which social relationships are legal and protected; they set incarceration strategies, which have implications for families; they legislate on issues of family planning, including adoption and abortion; and they choose which mental health services are covered by Medicaid. The effects on population health are wide-ranging. For instance, living in a state with weak or absent protections for lesbian, gay, and bisexual populations elevates rates of generalized anxiety disorder, posttraumatic stress disorder, and dysthymia among these populations (Hatzenbuehler, Keyes, and Hasin 2009).
States also influence behaviors through a range of policies, such as tobacco control, nutrition labeling, eligibility and enrollment criteria for the Supplemental Nutrition Assistance Program (SNAP), and marijuana legalization. For instance, by reducing food insecurity and freeing up resources that can be used to purchase other necessities such as medical care, SNAP improves a host of health outcomes for infants and adults (see review in Carlson and Keith-Jennings 2018). State tobacco control efforts, such as excise taxes and smoke-free laws, can reduce smoking prevalence (Farrelly et al. 2013). With this contextual lens, it is clear that the individual-level mechanisms proposed to explain educational disparities in health (economic well-being, psychosocial resources, behaviors) cannot suffice on their own. Rather, they should be conceptualized as inextricably embedded within, and influenced by, state policy contexts.
Heterogeneity in the Health Effects of State Contexts
State contexts and policies may have different consequences for population subgroups. In fact, this assertion is a core element of the constrained choices model, originally developed to explain gender differences in health (Bird and Rieker 2008). The model asserts that social contexts and policies can constrain the choices that individuals have for creating a healthy life and that marginalized populations tend to have more constraints and hence fewer choices. Relating the model to education and health, one implication is that U.S. states and their policies may affect the health of low-educated adults more so than their higher educated peers. Indeed, many state policies, such as state EITCs, minimum wages, Medicaid generosity, SNAP, tobacco taxes, and unemployment and incarceration policies are disproportionately relevant for economically marginalized individuals, among whom the vast majority are low educated. These policies directly shape the opportunities and choices that low-educated adults have for social and economic well-being, intentionally and unintentionally shape health behaviors, and ultimately affect health. In contrast, higher educated adults may be largely unaffected. Their social, economic, and lifestyle advantages acquired during schooling may act as a “personal firewall” to protect their health regardless of context. In fact, this protective feature of education is evident in the narrowing of health inequities across gender among high-educated adults (Ross, Masters, and Hummer 2012).
Framework, Aims, and Expectations
We use a contextual perspective to examine educational disparities in health by shining a light on U.S. states as institutional actors on those disparities. FCT implies that higher educated adults will be better able to acquire health-beneficial knowledge and resources, and avoid health-related risks, regardless of state contexts. Consequently, their health may be similar across states. At the same time, the socioecological framework and constrained choices model imply that states’ contexts and policies have a strong impact on the social, economic, and lifestyle choices and constraints faced by low-educated adults. Consequently, their health may differ dramatically across states. Taken together, these perspectives suggest that educational disparities in health are simultaneously shaped by the myriad advantages and resources of higher educated adults, which transcend states, and the disadvantages and constrained choices of lower educated adults, which in many ways are manufactured by states.
We provide two empirical examples of this contextual perspective and demonstrate its utility for understanding educational disparities in U.S. adult health. First, we document that educational disparities in health vary across states. We pay close attention to how states vary in their health for higher and lower educated persons. As noted earlier, we expect that state variation in health will be greater for lower educated persons. Second, we illustrate one way (excise taxes on tobacco) through which states “act” to produce educational disparities in health.
Taken together, the empirical evidence we develop below is highly consistent with a contextual framework in which U.S. state contexts shape educational disparities in health. We emphasize that our analyses are not intended to prove causality or definitively test the framework. Instead, our analyses and intent are similar to those of the seminal works that developed FCT (Link 2008; Link and Phelan 1995; Phelan and Link 2005). Like those, our analyses are descriptive, and our intent is to offer a compelling framework. Our ultimate aim is to shift the narrative and research on the education-health association in the United States from one focused on individual-level mechanisms to one that also, and prominently, considers contextual influences such as U.S. states.
Documenting the Pattern: Educational Disparities in Health by U.S. State
Data and Measures
Our assessment of state variation in educational disparities in multiple health outcomes is based on two nationally representative surveys: the American Community Survey (ACS) and the National Longitudinal Mortality Study (NLMS). We chose these surveys because they contain information on state of residence, unlike other surveys commonly used to assess health outcomes, such as the public-use National Health Interview Survey. We use current public-use versions of both surveys: 2010–2014 ACS and 2000s NLMS.
We examined all health measures available in the two surveys. The ACS includes six measures assessing difficulty with dressing or bathing, doing errands alone, lower body mobility, vision, hearing, and cognition. We dichotomized each of the six measures into 1 (has difficulty) or 0 (does not have difficulty). The NLMS contains data on self-rated health. We dichotomized the measure into “good” (which includes “excellent,” “very good,” and “good”) and “poor” (which includes “fair” and “poor”). We categorized education into less than high school, a high school credential or some college (among older birth cohorts, such as those included in our study, these two groups have similar health profiles), and a bachelor’s degree or higher.
We restricted the sample to U.S.-born adults because the health benefits of education may differ for education obtained abroad (Walton et al. 2009). We also restricted the sample to ages 45 to 89 years. We set the upper limit to 89 years because both surveys top-code at 90 years; setting the lower limit to 45 years gives education sufficient time to “play out” and shape adult health. These restrictions provided a sample of 6,090,440 adults in the ACS and 175,858 adults in the NLMS.
For each outcome, we estimated a logistic regression predicting the log odds of the health outcome from 150 combinations of 50 states and three education levels, adjusting for age in years, gender, and race/ethnicity (non-Hispanic white, non-Hispanic black, non-Hispanic other, Hispanic). All analyses accounted for the survey weights. We show the results graphically. For each state, we show the predicted probability of the outcome for non-Hispanic white women 65 years of age.
Findings
Educational disparities in each health measure by U.S. state are displayed in Figure 1. For instance, the top left panel shows the percentage of women who reported difficulty dressing or bathing, by education level, in each state. States are sorted from highest to lowest prevalence among the low-educated group. In the first state on the left (West Virginia), 12.4 percent of women without high school credentials had difficulty dressing or bathing compared with 3.4 percent of women with bachelor’s degrees or higher, a 9 percentage point gap. In the last state on the right (Utah), 7.1 percent of women without high school credentials had difficulty dressing or bathing, compared with 2.6 percent of women with bachelor’s degrees or higher, a 4.5 percentage point difference. In absolute terms, the disparity is twice as large in West Virginia as it is in Utah.

Disparities in adult health by education level within U.S. states.
The pattern shown in Figure 1 reveals two key insights. First, educational disparities in health differ dramatically across the 50 U.S. states. Second, the size of the disparity differs across states primarily because the health of lower educated adults differs. Continuing with our example, the correlation between the educational disparity in the difficulty with dressing and bathing in each state and the prevalence of this difficulty among low-educated adults in each state is 0.95. The correlation between the disparity and the prevalence among high-educated adults is just 0.36. This pattern is robust across all health measures, as shown in Table 1. 2
Correlation between the Probability of Each Health Outcome for Particular Education Level in a U.S. State and the Gap in the Health Outcome across Education Levels (n = 50 States).

Note: Gap in each health outcome = health outcome for adults with less than a high school education – health outcome for adults with a bachelor’s degree or higher. All health outcomes are estimated from logistic regressions models with 150 combinations of 50 states and three education levels, controlling for age, gender, and race/ethnicity. Data on difficulty measures are from the 2010–2014 American Community Survey. Data on self-rated health are from the National Longitudinal Mortality Study spanning the 2000s.
In sum, these findings are consistent with our argument that U.S. state contexts shape the importance of education for health. Also as expected, states appear to have the strongest influence on the health of low-educated adults. In general, the less education an individual has attained, the more important his or her state of residence is for their health.
The dramatic differences in the disparities across states raise several important questions. For instance, how does this process unfold? How and why do states disproportionately affect the health of low-educated residents? The answers are surely complex. We expect that states’ socioeconomic and policy contexts shape the education-health association in myriad ways. Our next set of analyses illustrates one such way.
U.S. States as Institutional Actors: Cigarette Taxes and Educational Disparities in Smoking
To illustrate the role of states in the production of educational disparities in health, we examine cigarette smoking. We chose smoking for two reasons: smoking is a major risk factor for all health problems in Figure 1, and it was used extensively in the conceptual development of FCT (Link 2008). Consequently, our example can easily be situated within the FCT framework. The development of FCT pointed to the fact that the inverse association between education and smoking become prominent after the 1964 Surgeon General’s report, which provided some of the strongest language linking smoking to lung cancer, chronic bronchitis, and emphysema.
Within the FCT framework, the emergence of educational disparities in smoking is typically explained by the unequal distribution of resources such as information and beliefs about the dangers of smoking, particularly after the 1964 Surgeon General’s report (Baker et al. 2017; Link 2008). Higher educated adults were more quickly and likely than lower educated adults to claim that they had heard and believed the information, and accordingly, their smoking rates declined more quickly (Link 2008). However, central to our argument, individuals were not the only actors. States eventually made decisions about various tobacco control policies, such as raising the price of tobacco (often via excise taxes), restricting smoking in public places, raising the age for purchasing tobacco, requiring health warnings on tobacco products, and funding cessation programs (often via excise taxes). 3 The divergence in excise taxes across states was pronounced. As displayed in Figure 2, throughout most of the twentieth century, state excise taxes on cigarettes were negligible across states. In 1950, for instance, they were at most five cents per pack across all states except Louisiana (Orzechowski and Walker 2014). About 1990, excise taxes started to noticeably diverge across states. By 2014, the taxes ranged from just 17 cents in Missouri to $4.35 in New York.
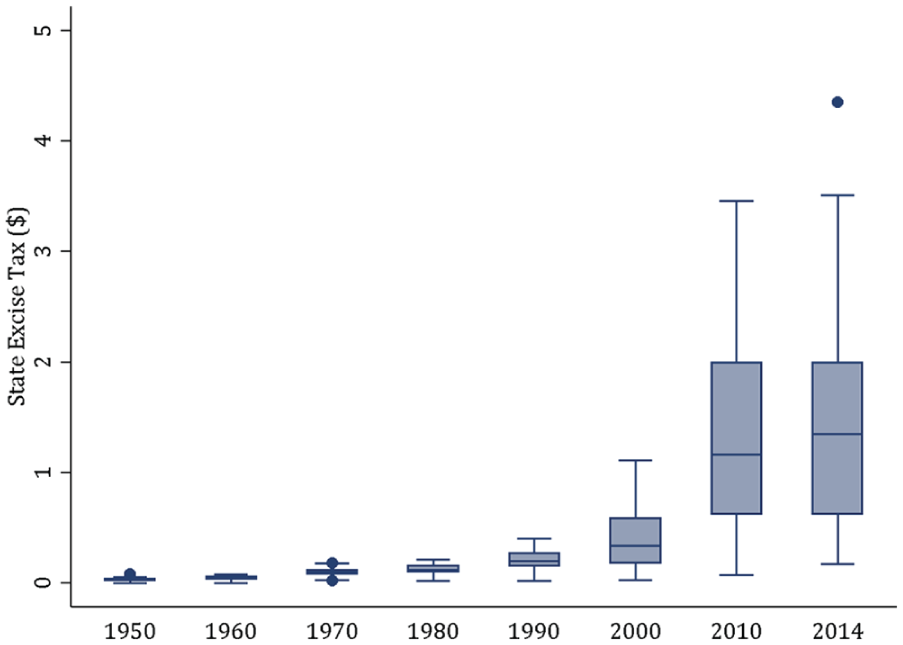
U.S. state excise tax on a pack of cigarettes, 1950 to 2014.
Excise taxes are particularly important in our framework for an additional reason. According to two reviews of international studies (Brown, Platt, and Amos 2014; Thomas et al. 2008), while various tobacco control policies can reduce overall smoking prevalence, the one policy with the most consistent evidence for reducing social disparities in smoking, which is our focus here, is raising the price of tobacco. In addition, a U.S. study found that economically disadvantaged adults were more than four times as responsive to rising prices (Farrelly et al. 2001); and low education is a major cause of economic disadvantage. The implication is that a state’s decisions to increase the price of tobacco would predominately deter smoking among low-educated adults, thereby reducing educational disparities in smoking.
We recognize that varying excise taxes across states reflects more than varying concern over tobacco consumption from state legislatures. The political leanings of legislators, the attitudes of constituents, and tobacco industry pressure all play a role (Golden, Ribisl, and Perreira 2013). Nevertheless, tobacco excise taxes shape smoking behaviors regardless of legislators’ motivation for raising them. The increased costs of tobacco deter consumption, help fund cessation programs, and send a powerful message that smoking is harmful for health. The bottom line is that states’ policy decisions, such as excise taxes, affect the incentives and capacities of their residents to create healthy lives (Bird and Rieker 2008), and those decisions may have disproportionate consequences for low-educated individuals.
U.S. States’ Cigarette Excise Tax and the Education Gap in Smoking
We illustrate the utility of our conceptual framework for explaining the gap. We draw on the five-state strategy used by Fenelon (2013) to elucidate mortality trends. Specifically, we examine trends in smoking for the five states with the largest increase in excise taxes (Minnesota, Rhode Island, Connecticut, Massachusetts, and New York) and the five states with the smallest increase (Missouri, North Dakota, Alabama, Louisiana, and Georgia) during our study period. We refer to these as “leading” and “trailing” states, respectively. On the basis of our framework, we derive several expectations:
We expect prevalence and trends in smoking among higher educated adults in the five leading states to be similar to those in the five trailing states. Supporting our framework, this would indicate that smoking among higher educated adults is largely influenced by factors operating independently of their state of residence. These factors may include, for example, individuals’ own human capital and cognitive abilities for processing health-related information, social networks, and national media coverage of public health issues.
We expect trends in smoking prevalence among lower educated adults to be dissimilar between leading states and trailing states. We expect to see a marked decline in smoking prevalence among low-educated adults in leading states, a decline that is greater than that of their higher-educated peers in those states as well as their similarly educated peers in trailing states. This would suggest that smoking behaviors of low-educated adults are influenced by their state of residence, including its cigarette taxes.
We expect that the education gap in smoking within leading states to decrease more than the gap within trailing states. This is consistent with the crux of our argument that states are institutional actors in the production of educational disparities in population health.
Data and Measures
We contrast trends in smoking prevalence, by education level, in the five leading states (Minnesota, Rhode Island, Connecticut, Massachusetts, and New York) to those in the five trailing states (Missouri, North Dakota, Alabama, Louisiana, and Georgia) (Orzechowski and Walker 2014). We estimated smoking prevalence using data from the Current Population Survey (CPS) because it provides one of the longest running series of questions on smoking. The CPS is a monthly survey of roughly 50,000 households, representative of the civilian, noninstitutionalized population aged 15 years and older. In September 1992, the CPS began periodically asking questions about smoking as part of its Tobacco Use Supplement. Individuals were asked if they had smoked at least 100 cigarettes in their entire lives, and if so, whether they currently smoked every day, some days, or not at all. We defined adults as current smokers if they smoked every day. 4
For reliable state-level estimates of smoking, the CPS recommends that three consecutive Tobacco Use Supplement waves be combined (U.S. Census Bureau 2015). For instance, it recommends that the September 1992, September 1993, and May 1993 waves be combined for reliable state-level estimates of smoking circa 1993. Collapsing waves in this way allows estimates for eight time periods between circa 1993 and 2015. Because we further disaggregated the data by education level, we took an extra precaution and combined six consecutive waves for reliable estimates, which yielded data for four time periods, 1992 to 1996, 1998 to 2002, 2003 to 2007, and 2010 to 2015. We estimated the prevalence of daily smoking in each of these periods among adults aged 25 to 89 years by education level. All estimates were weighted and age-standardized to the 2000 U.S. population.
Findings
The estimated prevalence of smoking across the four periods is shown in Figure 3. Figure 3A shows trends in smoking for the five leading states, with the black lines representing adults without high school credentials (“low educated”) and the gray lines representing adults with bachelor’s degrees or higher (“high educated”). Figure 3B shows the same information for the five trailing states.

Percentage of adults aged 25 to 89 years who currently smoke by education level and state of residence, 1992 to 2015.
Figure 3 supports our first expectation that smoking among high-educated adults is influenced largely by factors operating independently of their states of residence. Trends in smoking prevalence are similar for both leading and trailing states. In addition, the prevalence levels are also strikingly similar between these two groups of states.
We also find compelling support for our second expectation that smoking among low-educated adults depends on their states of residence. This can be seen in two ways. First, unlike smoking prevalence among high-educated adults, smoking prevalence among low-educated adults differs markedly across states. For instance, in the first time period the prevalence among low-educated adults ranged from 23 percent in New York (a leading state) to 41 percent in Missouri (a trailing state). Second, among low-educated adults, the range in smoking prevalence across the leading states shrank by two thirds (from an 11.2 percentage point gap to a 3.8 percentage point gap) but nearly doubled across trailing states (from 8.4 to 16.1) across the study period.
Last, we also find support for our third expectation. Figure 4 shows trends in the educational gap in smoking for each state. Leading states are shown in Figure 4A. The educational gap in smoking narrowed considerably, by an average of 7.1 percentage points. These states experienced a homogenization of smoking prevalence among lower educated adults. Trailing states are shown in Figure 4B. Here, the educational gap in smoking shrunk by just 3.1 percentage points on average. Across both groups of states, it is clear that any narrowing of the gap during the study period reflects reductions in smoking among low-educated adults.
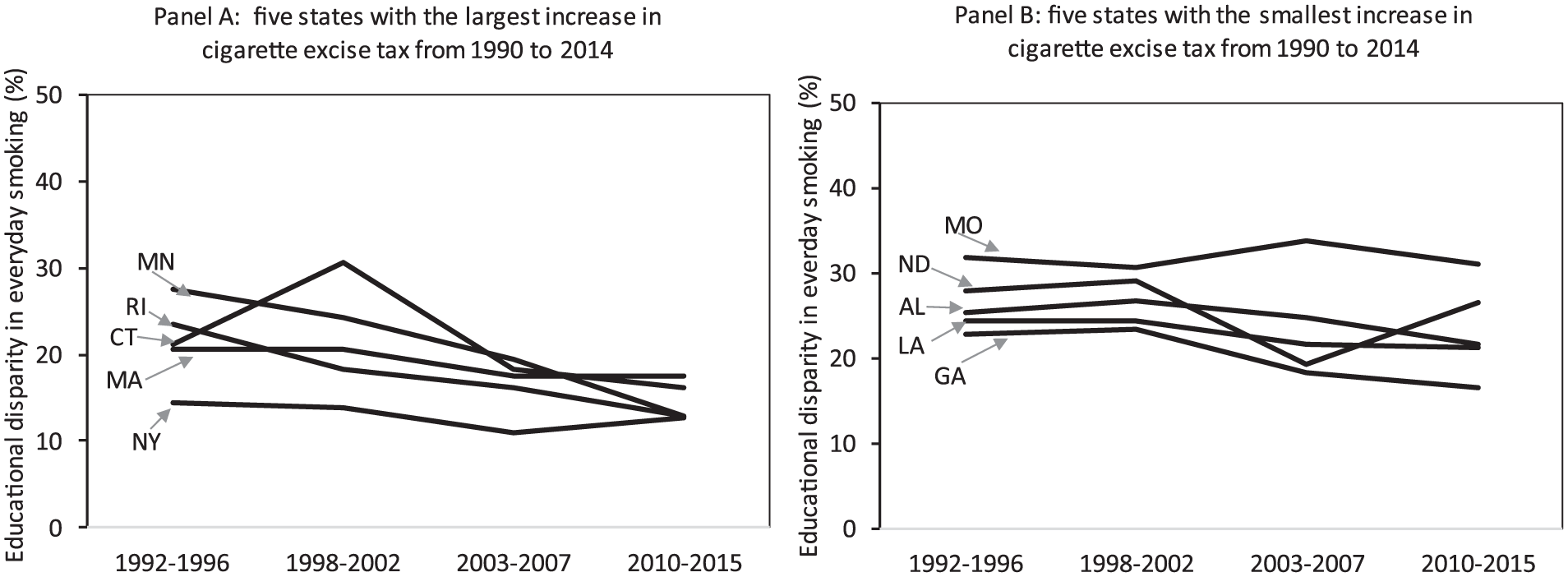
Educational disparities in current smoking among adults aged 25 to 89 years by state of residence, 1992 to 2015.
In sum, this example suggests that decisions made by states on cigarette taxes influence the prevalence of smoking among low-educated adults but have a muted effect on their more educated peers. The smoking habits of low-educated adults appear more closely tethered to their states of residence than the habits of higher educated adults. It implies that efforts to understand why education has become a stronger predictor of smoking (and health more generally) in some parts of the country could benefit from investigating the role of state policies rather than focusing on presumed deficits in decision making or endowments of low-educated residents. Last, our finding that smoking prevalence among higher educated adults is similar across 10 states with markedly different social, economic, and policy contexts (and cigarette taxes) is astonishing.
Implications
We examined educational disparities in U.S. adult health using a new lens that highlights the critical role of U.S. state contexts. In doing so, we provide at least three insights into the reasons for these disparities within the U.S. context. First, the findings imply that educational disparities in U.S. adult health are not simply a reflection of higher educated individuals possessing certain traits, characteristics, knowledge, lifestyles, social ties, or greater agency. On the contrary, the disparities are also strongly shaped by the policy contexts of the U.S. state in which individuals reside (as well as contexts at multiple levels, from federal to state to local). This calls into question explanations for educational disparities in health that exclusively focus on individual-level mechanisms. It also underscores the need to reorient research on these disparities and their growth over time to focus on the contextual factors that drive them. As Hayward et al. (2015) stated in their study of the education-mortality association, “there is no inherent causal association between educational attainment and adult mortality; instead, the causal association is dependent upon the time, place, and social environment under study” (p. 16).
Our second insight derives from our finding that the size of educational disparities in adult health varies across states mainly because the health of low-educated adults varies across states. In contrast, higher education, especially a college education, provides somewhat of a “personal firewall” against state contexts (see also Montez, Zajacova, and Hayward 2017). This finding offers a more nuanced understanding about the extent to which education is a personal resource for health. It suggests that higher education is a personal resource across contexts but that low education is a personal risk primarily in certain contexts. Interestingly, this finding differs from studies comparing educational disparities in health across European countries. Several of those studies have reported that the disparities vary across countries because the health of both low and high educated adults varies across countries (Bambra et al. 2010; Cambois et al. 2016). Perhaps high-educated adults in the United States have maximized their potential for good health under current social and economic conditions. This is an area for further study.
A third insight is that educational disparities in health reflect circumstances in the lives of both high- and low-educated adults that may be changing in unique ways and for unique reasons. This is contrast to the presumption that higher educated adults simply “have more” of the things that enhance health or that health disparities have grown over time because higher educated adults have “benefited more” from new technologies and information. Our results indicate it is more complex than that. Low-educated adults are not simply riding further back on the same wave; their health appears to be shaped by somewhat different forces (e.g., state policies). This raises important questions and hypotheses about why education has become an increasingly strong predictor of adult health. Specifically, if the health of low-educated adults is uniquely influenced by certain social, economic, and political factors than is the health of higher educated adults, could changes in those factors in recent decades help explain why the health and longevity of low-educated adults has been moving in a different direction than their higher educated peers? We speculate on some of these contextual forces below.
Limitations
As we stated above, our analyses are intended to be illustrative, not a bulletproof validation. No single study provides definitive evidence, and our analyses are no exception. We aimed to establish a compelling and feasible framework. Our intent was to bring institutional context back into discussions about, and studies of, educational disparities in U.S. adult health and to highlight the role of U.S. states. Our findings provide a foundation for future studies to empirically tease out the role of U.S. states (and other types of contexts) in creating educational disparities in health.
We focused on a crucial state policy in our illustration in part because the pathways linking excise taxes to smoking are clear and direct. We recognize that other tobacco control policies can also deter smoking, such as smoking bans in public places. This is unlikely to materially affect our conclusions for two main reasons. First, a recent U.S. study found that excise taxes, not smoking bans, are the main deterrent of daily smoking (packs per day) and that the presence of each policy does not magnify the efficacy of the other (Vuolo, Kelly, and Kadowaki 2016). Second, raising the price of cigarettes (usually via excise taxes) is the only tobacco control regulation that tends to shrink social disparities in smoking (Brown et al. 2014). Nevertheless, even if additional tobacco control efforts contributed to the descriptive trends we reported, it would not change the overall conclusion that these efforts had disproportionate consequences for low-educated adults and that the prevalence and trends in smoking for college-educated adults are remarkably similar across states, despite vastly different policy contexts.
We focused on states for the many reasons outlined above and because a robust literature finds that states shape population health, even after accounting for local area characteristics (Arcaya et al. 2012; Montez, Hayward, and Wolf 2017) and individuals’ characteristics (e.g., Kawachi et al. 1997; Montez, Zajacova, and Hayward 2016; Subramanian, Kawachi, and Kennedy 2001). In addition, a study of educational disparities in disability across states found that they persisted even after accounting for local and individual socioeconomic characteristics (Montez, Zajacova, and Hayward 2017). Nevertheless, we recognize that local areas also matter. The framework we provide here may ultimately benefit from incorporating multiple levels, including individual, work-family, local, and state factors (Bird and Rieker 2008; Vuolo, Kadowaki, and Kelly 2016).
Our analyses also raise many questions. For example, which state-level policies shape disparities in population health? Given the myriad social, economic, and health policies, answering this question is beyond the scope of this or any single study; instead, it will require a major reorientation of the field at large. Our analyses also raise the question of whether states shape educational disparities in some health outcomes more so than others. Examining heterogeneity by health outcome and cause of death could further flesh out key processes. And finally, what state-level strategies and policies can reduce the disparities?
Future Directions
Drawing from FCT, the socioecological framework, and the constrained choices model, we use a contextual perspective to examine educational disparities in health and their growth over time by shining a light on U.S. states as institutional actors on those disparities. Our intention is similar to Cockerham’s (2005) in his construction of health lifestyle theory, to put forward a perspective that “accords structure a role that is consistent with its influence in the empirical world” (p. 64). Similarly, explanations for the historical decline in U.S. mortality in the early part of the twentieth century, for example, often drew on macro-level explanations such as industrialization and improvements in standard of living, sanitation, nutrition, and public health infrastructure. We have argued here that macro-level explanations remain important explanations of population health and health disparities, although the types of explanations almost certainly have changed over the course of the twentieth century and now into the twenty-first century (Montez 2017; Zajacova and Montez 2017).
Our general framework can be used to develop important macro-level hypotheses about the causes of recent health and mortality trends. These trends show, for example, that states’ life expectancies became highly unequal over the latter part of the twentieth century. In 1980, for example, life expectancy at birth in New York and Mississippi differed by only 1.6 years (Institute for Health Metrics and Evaluation 2018). By 2014, the difference was 5.5 years. The difference between the highest and lowest states was about 6.3 years (Institute for Health Metrics and Evaluation 2018). Placed in international context, New York’s mortality resembles that of Denmark, while Mississippi’s mortality resembles that of Romania. During this same time period, three major macro-level structural changes emerged: deregulation, devolution of political authority from federal to state levels, and state preemption laws (Montez 2017). These initiatives are recognized for their effects on many domains of life, but rarely have they been invoked as potential explanations for the troubling trends in U.S. health disparities. The deregulation of industries has led to a shrinking industrial and economic base in many parts of the country and, as discussed in the introduction, devolution of political authority and the proliferation of state preemption laws have increasingly given more authority to states.
These recent historical changes point to a highly dynamic landscape in which states are playing an increasingly central role in how macro-level contextual factors shape trends in population health and health disparities. Other contextual factors at various levels are playing important roles too, such as the broad societal effects of fast moving technological change. Nonetheless, it seems evident that macro-level changes in population health and health disparities require reorienting our traditional, individualized explanations and solutions for educational disparities in adult health to incorporate macro-level explanations (Zajacova and Montez 2017). A critical piece in reorienting this narrative is recognizing the growing importance of states as key institutional actors. Bringing states back into the conversation about America’s health and mortality trends is one means to putting the “social” back into studies on the social determinants of our nation’s health.
Footnotes
Acknowledgements
This article has benefited from comments by members of the Network on Life Course Health Dynamics and Disparities in 21st Century America (R24AG045061) and the Policy, Place, and Population Health (P3H) Lab at Syracuse University.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Aging (grant R01AG055481-01), the Carnegie Corporation of New York (grant G-F-18-56197), and the Eunice Kennedy Shriver National Institute of Child Health and Human Development (grant P2CHD042849). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the Carnegie Corporation.
1
Some exceptions include studies of how U.S. regional (Sheehan, Montez, and Sasson 2018) or urban-rural (Hayward, Pienta, and McLaughlin 1997) contexts shape the association between education and adult mortality.
2
The pattern is also robust across different subgroups and model specifications. For instance, it is robust to interstate migration: individuals who were born in their states of residence illustrate the same pattern. The pattern also persists when adjusting for adults’ employment and income. In addition, the pattern is not due simply to “floor effects” among high-educated adults: it persists for adverse health outcomes that have high prevalence across education levels (e.g., fair or poor self-rated health among adults 80–89 years of age). These analyses are available from the authors.
3
We focus on individuals and states but recognize that local areas can also enact tobacco control policies; that is, they can within U.S. states that do not preempt such local legislation. In fact, local legislation can often precede state legislation (![]() ). However, local areas cannot, by definition, enact legislation on state excise taxes, which is our focus here.
). However, local areas cannot, by definition, enact legislation on state excise taxes, which is our focus here.
4
We focus on daily smokers to minimize the influence of other tobacco control regulations (in particular, smoking bans in public places) on smoking behavior. Prior research has found that the association between excise taxes and “daily smoking” is statistically independent of the presence of smoking bans, while the association between excise taxes and “any smoking” is contingent on the presence of smoking bans (Vuolo, Kelly, and Kadowaki 2016). Nevertheless, our ancillary analyses of any smoking generated similar conclusions (analyses available from the authors).