
Abstract
Previous research shows that married and cohabiting individuals are happier and enjoy greater levels of psychological well-being than single individuals. However, most of this research relies on data from intraracial—mostly white—couples, and less is known about the emotional health outcomes of individuals in interracial partnerships. This study uses fixed-effects regression to examine depressive symptoms among those transitioning into intraracial and interracial relationships in the National Longitudinal Study of Adolescent to Adult Health. Estimating models separately by gender and race, our analyses show that although whites in same-race relationships enjoy the psychological health benefits traditionally associated with union formation, a more complex pattern characterizes these benefits for nonwhites and those in interracial relationships. These findings suggest that although Americans enter increasingly diverse romantic relationships, union formation might not equally benefit all.
Background
Married and cohabiting individuals are happier and enjoy greater levels of psychological well-being than do unmarried individuals (Simon and Barrett 2010; Waite and Gallagher 2002; Wood, Goesling, and Avellar 2007). However, most research examining the psychological benefits of partnership is based on data from intraracial couples—and more specifically, white couples. Less is known about the emotional health outcomes of individuals in interracial partnerships (but see Bratter and Eschbach 2006), even as interracial unions are becoming increasingly common in American society (Qian and Lichter 2011; Wang 2012, 2015).
Given that partners generally provide emotional and social support to each other (Thoits 2011; Waite and Gallagher 2002), one might expect widespread psychosocial benefits. However, given the history of antimiscegenation laws and norms against interracial marriage (Herman and Campbell 2012; Sohoni 2007), as well as higher burdens of stress faced by nonwhite individuals that may spill over across partners (Clavél, Cutrona, and Russell 2017; LeBlanc, Frost, and Wight 2015; Lincoln and Chae 2010; Thoits 2010), one may expect that members of interracial couples may not gain the same psychological health benefits from their partnerships. Finally, the effects of interracial marriage on psychological well-being could vary within the couple: interracial marriage may be beneficial or disadvantageous for one partner but not the other, depending on each partner’s race and gender (Bernard 1976; Mouzon 2014; Simon 2002).
The current study seeks to better understand the potentially heterogeneous relationship between romantic partnerships and psychological well-being. Using two waves of data from the National Longitudinal Study of Adolescent to Adult Health (Add Health) and fixed-effects regression, this article examines depressive symptoms among U.S. young adults in same-race and interracial relationships.
Interracial Relationships Benefit Both Partners: Partnership as a Resource
The resource model of marriage and partnership suggests that being partnered is linked to better psychological health because it brings material and emotional resources to the dyad (Umberson, Thomeer, and Williams 2013; Waite and Gallagher 2002). Partnered individuals tend to have greater financial resources, which can reduce their exposure to risks and stressors and increase their ability to weather adverse events. In addition, a partnered individual is more likely than a single individual to have a companion and a confidant who is concerned with his or her well-being. Having a partner who listens to problems and offers advice reduces stress and supports psychological health (Thoits 2011). A large body of empirical literature supports this theoretical model and shows that partnered individuals have better mental health than do single individuals. Partnered individuals are happier (Demir 2010; Musick and Bumpass 2012), less anxious (Braithwaite, Delevi, and Fincham 2010; DeKlyen et al. 2006), and less depressed (Musick and Bumpass 2012; Simon 2002) than their single counterparts. Most of this work controls for race, which implies that union formation benefits individuals regardless of their race.
Interracial Relationships Disadvantage Both Partners: Homogamy Hypothesis
Though the resource model predicts that all individuals will benefit from union formation, other theories suggest otherwise. The homogamy hypothesis posits that when partners are not matched in educational attainment, religion, or other important status characteristics, conflicts are more likely to occur and can result in psychological distress (Joyner and Kao 2005; Schwartz 2013). Empirical research suggests that greater similarity between partners is associated with better relationship quality (Henderson, Ellison, and Glenn 2017; Keizer and Komter 2015; Luo 2017), which supports psychological well-being (Carr et al. 2014; Holt-Lunstad, Birmingham, and Jones 2008). Conversely, dissimilar partners face more conflict, have lower relationship quality (Hohmann-Marriott and Amato 2008), and are more likely to separate or divorce than more homogamous couples (Bratter and King 2008; Joyner and Kao 2005; Zhang and Van Hook 2009). Thus, there is reason to believe that racially dissimilar partners may report higher levels of psychological distress than singles and compared to their counterparts in same-race relationships.
Interracial Relationships Differ for Each Partner: “His” and “Her” Marriages and the Intersectional Perspective
The benefits and disadvantages associated with interracial relationships also may differ depending on the characteristics of each individual in the union. For example, the theory of “his” and “her” marriages (Bernard 1976; Simon 2002) suggests that the psychological benefits of partnering vary by gender because men and women occupy different relationship roles. Women are more likely to assume the frustrating and devalued roles in a relationship and thus benefit emotionally from union formation less than men do. Recent research finds that, even though men’s and women’s relationship roles have changed, partnered men continue to experience increases in emotional well-being, but partnered women’s increase in psychological health is less pronounced (Simon 2002; Simon and Barrett 2010). The theory of “his” and “her” marriages, then, suggests that women’s emotional well-being will benefit less from union formation than that of men, regardless of the racial composition of the couple.
Last, the intersectional perspective draws on work in race and gender (Collins 2002; Crenshaw 1991), suggesting that gender interacts with race to produce variations in the association between partnership status and psychological well-being. This perspective posits that examining race and gender together is imperative for understanding individuals’ mental health outcomes in romantic relationships. Given evidence that Asian, black, and white men and women report unique experiences in interracial relationships (Bratter and Eschbach 2006; Canlas et al. 2015; Inman et al. 2011; Kroeger and Williams 2011), we predict that the psychosocial benefits associated with partnering will depend on the specific race and the gender of the individual in the partnership.
In testing these perspectives on partnership and psychological well-being, we replicate previous work examining the outcomes associated with interracial relationships (Bratter and Eschbach 2006; Kroeger and Williams 2011) and also extend previous research by using fixed-effects models to account for any time-invariant characteristics of individuals and examining a greater variety of interracial relationships.
Data
To study the relationship between interracial unions and psychological well-being, we use data from Add Health (Harris 2009). Add Health is a nationally representative, longitudinal study of nearly 20,000 adolescents who were in grades 7 through 12 in the 1994–1995 school year in the United States. The study participants were reinterviewed in 1996, 2000–2001, and most recently in 2007–2008, at which time the respondents were aged 24 through 32 and settling into adulthood. Our analyses use data from waves 3 and 4, when respondents were aged 18 through 26 and 24 through 32, respectively, and had begun establishing romantic partnerships and transitioning into marriages and cohabitations.
Our analytic sample includes respondents who were single, married, or cohabiting with a partner in each wave. For our analyses, we combine those in dating and sexual relationships with single respondents. 1 These restrictions leave 7,054 respondents who had complete information about all key variables in both waves.
The outcome of interest is depressive symptoms as measured by a nine-item version of the Center for Epidemiological Studies–Depression (CES-D) scale (Radloff 1977). Respondents were asked, “How often was each of the following things true during the past seven days:”
“You were bothered by things that don’t usually bother you”
“You could not shake off the blues, even with help from your family and your friends”
“You felt you were just as good as other people”
“You had trouble keeping your mind on what you were doing”
“You felt depressed”
“You felt that you were too tired to do things”
“You enjoyed life”
“You felt sad”
“You felt that people disliked you”
Responses range from 0 (never or rarely) to 3 (most of the time or all of the time), and items 3 and 7 are reverse coded. Summing the answers produces a CES-D score that ranges from 0 to 27. Higher scores indicate a greater burden of depressive symptoms. Descriptive statistics in Table 1 show that the average weighted CES-D score is 4.44 in wave 3 and 5.09 in wave 4. In both waves, the average CES-D score is lowest among those married to someone of the same race (4.21 in wave 3 and 4.75 in wave 4). In wave 3, the highest average CES-D score is seen among those married interracially (4.85), but in wave 4, single respondents have the highest average CES-D score (5.46).
Descriptive Statistics.

Note: Means and percentages are survey weighted. Depressive symptoms are measured by the Center for Epidemiological Studies–Depression scale.
The key predictor variable, whether respondents were single, interracially partnered, or intraracially partnered, is constructed using respondents’ self-reported race from wave 3 and the rich relationship data available in waves 3 and 4. In the wave 3 interview, respondents were first asked whether they were Hispanic and then asked whether they identified with any of the following racial groups: white, black, Native American, or Asian. Respondents reporting multiple race categories were asked to choose one race that best described their racial background. We use these data to construct a race variable with six mutually exclusive categories: non-Hispanic white, non-Hispanic black, Native American, Asian, Hispanic white, and Hispanic nonwhite. 2
Then, respondents reported on their relationships. In each wave, respondents indicated whether their current relationship was a marriage, a cohabitation, or something else. Respondents also identified their partners’ racial and ethnic backgrounds. Each respondent was first asked whether his or her partner was Hispanic and then asked to select one race to describe the partner’s background. Respondents could choose white, black, Asian, Native American, or other. Because respondents who indicated their partners’ ethnicity was Hispanic often proceeded to indicate their partners’ race was other, we constructed a similar race variable for partners containing the same mutually exclusive categories of non-Hispanic white, non-Hispanic black, Asian, Native American, Hispanic white, and Hispanic nonwhite.
We used race information from respondents and their partners to categorize relationships as interracial if the respondent’s race differed from that of his or her partner. For example, a non-Hispanic black respondent is in an interracial relationship if her partner is non-Hispanic white, Hispanic white, Hispanic nonwhite, Asian, or Native American. Important to note, given the different patterns that we observed for Hispanics who identified as white versus nonwhite, we categorized Hispanic white respondents as coupled interracially if their partners are Hispanic nonwhite. Our main independent variable has three categories indicating whether a respondent is single, in a same-race marriage or cohabiting relationship, or in an interracial marriage or cohabiting relationship, at each interview wave. Although cohabitation possibly differs from legal marriage in its level of perceived stability (Lyngstad and Jalovaara 2010), and differences in perceived union stability could have an effect on psychological well-being (Dush and Amato 2005), we found similar patterns when comparing marriages and cohabitations separately (results available upon request). As such, we combined these different relationship types to allow us to better estimate differences across racial groups. In wave 3, 69.3 percent were single, 24.9 percent were in a same-race relationship, and 5.8 percent were in an interracial relationship. In wave 4, 37.8 percent were single, 50.7 percent were in a same-race relationship, and 11.5 percent were in an interracial relationship (see Table 1).
Finally, all regression models include controls for age, education, and parenthood. Respondents were on average 22 years old in wave 3 and 29 years old in wave 4. Most respondents reported having completed high school (31.4 percent) or some college (42.1 percent) in wave 3. In wave 4, 36.4 percent of respondents had completed some college, and more than a quarter of respondents had received college degrees (27.4 percent). One fifth (20.5 percent) of respondents were parents in wave 3, and nearly half (48.2 percent) were parents in wave 4.
Methods
Taking advantage of the longitudinal nature of the data, we use fixed-effects regression models (Allison 2009) to examine the relationship between same-race and interracial partnership formation and CES-D scores. Fixed-effects regression models account for each person’s average level of depressive symptoms, allowing us to compare how depressive symptoms change for individuals who enter same-race or interracial partnerships compared with when they were single. Intuitively, these models can be thought of as estimating the average difference in CES-D scores for each individual (comparing CES-D score from when the respondent was single to his or her CES-D score from when he or she was in a relationship), and then averaging across these person-specific differences. Because the individual fixed effects account for all characteristics of respondents that do not change over time, we do not include covariates for time-invariant demographic characteristics (which are collinear with our fixed effects) but do include controls for age and education. Further, we control for parenthood as parental status is related to both the independent and dependent variables. Our models take the general form:

where Yit refers to the depressive symptoms of respondent i at time t, Xit refers to our independent variables (including relationship status variables, a constant, and our controls), αi are our respondent fixed effects, and εit represents the error term.
We estimate models first for all respondents, then separately for men and women to examine how the psychological health outcomes associated with relationship formation might vary by gender (Bernard 1976; Simon 2002). We also estimate regression models separately for non-Hispanic white, non-Hispanic black, Asian, Hispanic white, and Hispanic nonwhite respondents to examine whether the effect of forming intra- and interracial relationships on depression differs by race (Bratter and Eschbach 2006; Kroeger and Williams 2011). We do not estimate results separately for Native American respondents due to small sample size.
We supplement these regression models by interacting gender with relationship type and race with relationship type to identify statistically significant differences in the effect of relationship type on CES-D score across gender and racial groups. In addition to testing whether respondents in interracial partnerships differ from when they were single in the number of depressive symptoms they report, we also test whether the effect of being in an interracial union differs from being in a racially endogamous one in each model.
We build on these models by estimating the changes in depression scores associated with entering specific inter- and intraracial relationships: non-Hispanic black/non-Hispanic white (n = 5,491), Asian/non-Hispanic white (n = 4,647), Hispanic white/non-Hispanic white (n = 4,966), and Hispanic nonwhite/non-Hispanic white (n = 4,553). These models allow us to begin identifying whether forming unions of specific race combinations is especially strongly related to changes in depression. We are unable to estimate models for couples of other race combinations (e.g., black/Asian) because of small sample size. In addition, given the relatively small sample sizes in some of the groups, many of the results discussed are not statistically significant, warranting caution in interpreting them. We have highlighted points where the number of cases is particularly limiting. Nevertheless, as the absence of a statistically significant difference (p > .05) does not imply that there is no difference (Altman and Bland 1995), and given the limited data that exist on this question, we believe that the pattern of results we document is noteworthy. To facilitate the interpretation of our results, we plot the coefficients estimating changes in CES-D score in Figures 1 through 5. Negative coefficients indicate lower CES-D scores, which correspond to better psychological health. Supplemental Tables A1 through A7 contain coefficients from the models underlying these figures as well as results from tests of gender and race interaction effects.
Change in depressive symptoms by relationship type.
Change in depressive symptoms among non-Hispanic black/non-Hispanic white couples.

Change in depressive symptoms among Asian/non-Hispanic white couples.

Change in depressive symptoms among Hispanic white/non-Hispanic white couples.

Change in depressive symptoms among Hispanic nonwhite/non-Hispanic white couples.
Results
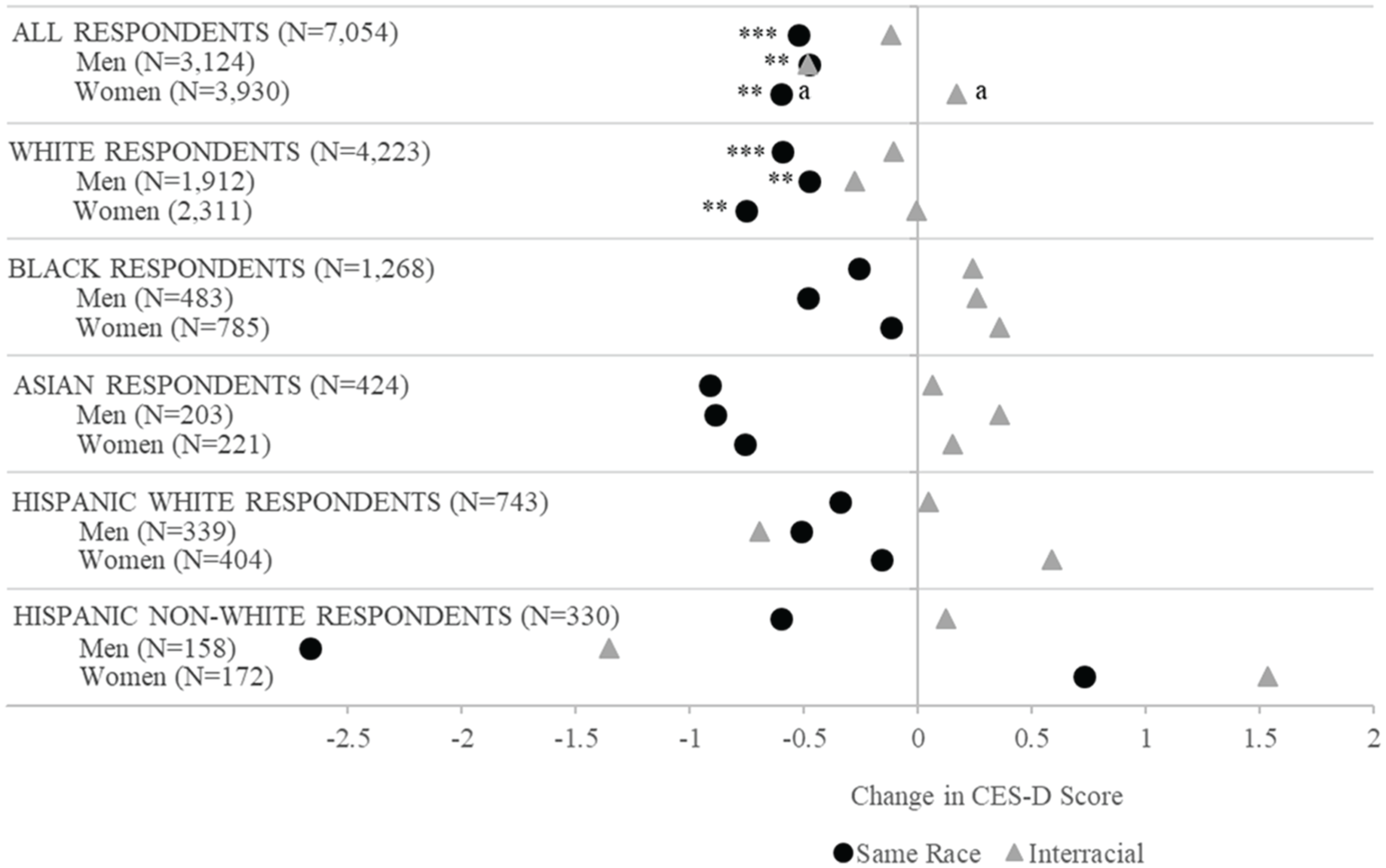
Figure 1 compares the changes associated with entering intra- and interracial partnerships relative to remaining single. The first row of points shows that among all respondents transitioning into same-race unions (the black circle), there is an associated reduction in CES-D scores. On average, individuals who enter same-race marriages or cohabitations experience a 0.53-point decrease in their CES-D score compared to remaining single (p < .001). Transitioning into an interracial relationship (the grey triangle), on the other hand, is not associated with reductions in depressive symptoms (β = −.12, p > .05). A Wald test suggests that the coefficients for same-race and interracial relationship formation are marginally statistically significantly different from each other (F = 3.54, p < .10).
The second and third rows of points in Figure 1 report results separately for men and women. We find that men who enter same-race relationships experience a 0.48-point drop in their CES-D scores (p < .01). The reduction for men who form interracial relationships is similar in magnitude but is not statistically different from zero (β = −.48, p > .05). Among women, forming same-race unions is associated with a reduction in depressive symptoms (β = −.60, p < .01), but transitioning into interracial unions is not. A Wald test confirms that the changes experienced by women entering interracial partnerships differ from changes of those entering intraracial partnerships (F = 6.40, p < .05). Taken together, these findings suggest that the psychological benefits associated with partnership formation may apply only to those entering racially endogamous relationships, though men appear to benefit equally from entering both intra- and interracial relationships.
The next set of results in Figure 1 reports the results for non-Hispanic white respondents in interracial and intraracial partnerships. Our findings here largely mirror those among all respondents depicted above, showing again that entering an intraracial partnership—but not an interracial partnership—is associated with a decrease in depressive symptoms. Likewise, as in the overall results, this pattern is particularly pronounced for women; for men, our point estimates suggest that entering both inter- and intraracial partnerships may be associated with declines in depressive systems (although the declines are larger for those entering intraracial partnerships).
The subsequent results in Figure 1 provide information about non-Hispanic black respondents, Asian respondents, Hispanic white respondents, and Hispanic nonwhite respondents who enter inter- and intraracial partnerships. Given the small sample sizes, these analyses are underpowered, and our results are not statistically significant; nonetheless, we review our findings for these groups because the direction and magnitude of these coefficients are instructive. For non-Hispanic black respondents, our results suggest that forming same-race partnerships may be related to better psychological health relative to being single, but forming interracial relationships may be related to worse psychological health. This pattern is more pronounced for men, and we find little evidence of average differences in changes in depressive symptoms associated with entering partnerships for black women. This pattern of findings suggests that additional work with larger samples would be helpful, as our small sample hampers our ability to rule out meaningful changes.
Looking next at Asian respondents, we find that entering same-race unions is associated with substantial reductions in CES-D symptoms (β = −.91) but entering interracial unions is not (β = .06). Looking across gender, and we see that Asian men seem to experience slightly larger declines (or smaller increases) in depressive symptoms from entering intraracial unions. Among Hispanic white respondents, men show reductions in depressive symptomology when forming either intra- or interracial relationships, while Hispanic white women have reductions only when entering intraracial unions and worse psychological health when entering interracial unions. Thus, for Hispanic white respondents, forming a same-race relationship may be related to reductions in CES-D scores (β = −.34), but entering interracial relationships appears to be associated with only decreases for men and is associated with increases in depressive symptoms among women. For Hispanic nonwhite respondents, men appear to benefit from any kind of partnership, while women who enter unions (either same-race or interracial) may experience more depressive symptoms compared to being single. Again, we caution that none of these coefficients reaches statistical significance, so results should be interpreted with appropriate care.
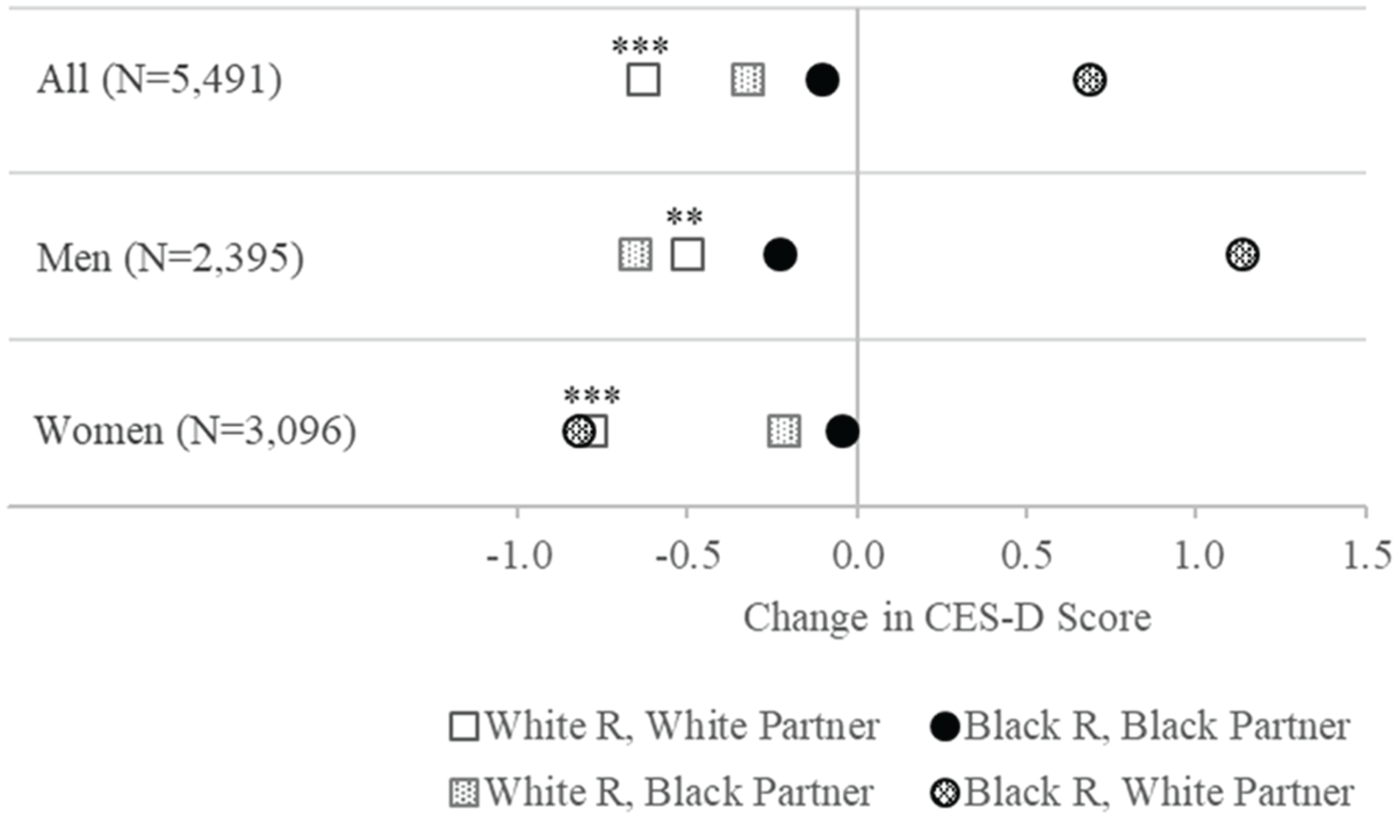
Up to this point we have discussed depression outcomes among respondents transitioning into interracial relationships without examining whether the specific racial combination of the couple matters. Figure 2 presents results for non-Hispanic white/non-Hispanic black couples. These models compare the change in CES-D scores for white respondents who form relationships with white partners (white squares), black respondents who form relationships with black partners (black circles), white respondents who form relationships with black partners (dotted square), and black respondents who form relationships with white partners (dotted circle) to their white and black counterparts who remain single (see supplemental Table A4 for coefficients).
The first row of points shows that white respondents who partner with other whites (white square) have the largest reductions in depressive symptoms (β = −.63, p < .001). Black respondents who partner with blacks (black circle) and white respondents who partner with blacks (dotted square) experience smaller reductions in depressive symptoms that are not statistically significant. By contrast, black respondents who partner with whites (dotted circle) report increased depressive symptoms (β = .69). White respondents may experience psychological benefits when they enter relationships with white partners, but black respondents who partner with whites do not appear to receive the same benefits and may even experience increased levels of depressive symptoms. This pattern of results broadly holds for men, although white men report lower levels of depressive symptoms when they enter unions with black partners than they do when entering unions with white partners. Among women, we see that partner race appears to matter more than respondent race, as both black and white women who partner with whites benefit similarly, although the coefficient for black women is not statistically significant (white women: β = −.79, p < .001; black women: β = −.82, ns).
Figure 3 displays results from an analysis of Asian/non-Hispanic white couples (regression coefficients available in supplemental Table A5). It compares changes in CES-D scores among white respondents who couple with white partners (white squares), Asian respondents who partner with other Asians (black circles), white respondents who form relationships with Asian partners (dotted squares), and Asian respondents who enter relationships with white partners (dotted circles) to themselves when single. All three rows of points suggest that white and Asian respondents who form same-race relationships (white squares and black circles) generally experience reductions in depressive symptoms (results are statistically significant for whites only). Interesting to note, while white men with Asian partners (dotted square) have increased CES-D scores compared to white men with white partners (white square), Asian men and women with white partners and white women with Asian partners all experience very little change in their reports of depressive symptoms.
Figure 4, with results for Hispanic white/non-Hispanic white couples (regression coefficients in supplemental Table A6), provides evidence suggesting that certain interracial relationships could have psychological health benefits that are substantially larger than those associated with entering same-race relationships. Non-Hispanic white women who are coupled with Hispanic white partners (dotted squares) experience substantial reductions in depressive symptoms, as do Hispanic white men coupled with non-Hispanic white women (though this difference is not statistically significant). However, Figure 5 depicts a starkly different pattern for Hispanic nonwhite/non-Hispanic white couples (regression coefficients in supplemental Table A7). Here we see that white women with Hispanic nonwhite partners and Hispanic nonwhite women with white partners experience substantial decreases in their psychological health. By contrast, white men with Hispanic nonwhite partners appear to experience reductions in depressive symptomology similar to white men in same-race unions.
Discussion
Taken together, we find that individuals who marry or cohabit with partners of the same race have lower levels of depressive symptomology compared to being single, which is consistent with previous research on union formation more generally (Musick and Bumpass 2012; Simon 2002; Waite and Gallagher 2002; Wood et al. 2007). Those who form interracial partnerships, however, do not appear to accrue these psychological health benefits. It is possible that transitioning into an interracial union confers the same psychological health benefits to partners as transitioning into a same-race relationship does but also includes some disadvantages that same-race partners do not face, which cancels the positive effects on psychological well-being for interracial couples. For example, the psychological stresses of discrimination and racism experienced by one partner might spill over to the other partner and weaken any emotional benefits generally associated with marriage and cohabitation (Clavél et al. 2017; Lincoln and Chae 2010; Thoits 2010). Or those in interracial relationships may not show changes in psychological well-being when they form marriages or cohabiting relationships because they may get emotional support from other relationships, such as those with extended family and friends, and may depend less on marriage and cohabiting relationships for these psychosocial resources (Mouzon 2014).
These results partially support the resource model of marriage and relationships, which suggests that being partnered is associated with fewer depressive symptoms relative to being single. This pattern holds only for intraracially partnered individuals, and for non-Hispanic white individuals in particular. Given that this framework may have been developed using data from a time when interracial relationships were uncommon, it may primarily reflect the experiences of non-Hispanic white couples. It thus seems plausible that the resource model misses important variation in the kinds of resources partners bring to the relationship and the stressors that may be associated with nonmonoracial white unions.
To the degree that our findings suggest that women who enter interracial unions typically experience smaller reductions in depressive symptoms than women who enter same-race unions, we find some evidence for the homogamy hypothesis, which posits that being interracially partnered is associated with more depressive symptoms relative to being partnered intraracially or being single. However, given that men entering inter- and intraracial unions experience similar decreases in depressive symptomology, the homogamy hypothesis appears to be limited in scope. Likewise, insofar as we find gender differences that we observe vary by race and relationship type, they are ill explained by accounts of “his” and “her” marriages, which focus on the different roles that men and women play in relationships. Rather, the differences in CES-D reduction that we observe by gender, race, and relationship type appear to fit better with the intersectional perspective, which suggests that forming partnerships may have different associations with psychological well-being depending on the race and gender of the partners. Given the additional emotion work expected of women (Reczek and Umberson 2012), the differences in gendered scripts and meanings by race (Collins 2002), and attitudes about different types of partnerships (Herman and Campbell 2012), the variation we observe in the psychological health outcomes associated with union formation is perhaps not surprising.
This study is limited by small sample sizes that reduced statistical power, precluding more definitive statements about the relationship between interracial partnering and psychological health and how this relationship might vary by race and gender. Further, we are unable to test the reasons that interracial couples might not experience better psychological health following union formation. Future research might fruitfully explore whether changes in relationship status are associated with changes in social support from family members, friends, and others (Herman and Campbell 2012) or changes in discrimination experiences (LeBlanc et al. 2015), which could in turn affect depressive symptoms. Future research examining regional variation in the CES-D reductions associated with different unions would also be of interest, particularly given work highlighting regional variation in racial boundaries and meanings (Saperstein, Pickett, and Penner 2015).
Interracial unions often are used as an indicator of the boundaries between different racial groups. Although our study cannot address questions of mechanism or causation, to the degree that those entering interracial unions fail to accrue the advantages because of discrimination and beliefs about interracial unions, our results suggest that simply looking at the levels of interracial unions is insufficient to understand the boundaries between groups. Further, policy makers often encourage union formation, citing the benefits associated with being in such partnerships. Our findings, however, suggest that the relationship between union formation and psychological health varies by gender, race, and whether the partnership is intra- or interracial. The type of relationship most clearly associated with psychological health benefits remains that between non-Hispanic white partners. This pattern suggests that although Americans enter increasingly diverse romantic relationships, union formation may not equally benefit all.
Supplemental Material
SRD814610_Supplemental_Material – Supplemental material for Better Together? Interracial Relationships and Depressive Symptoms
Supplemental material, SRD814610_Supplemental_Material for Better Together? Interracial Relationships and Depressive Symptoms by Jaclyn S. Wong and Andrew M. Penner in Socius
Footnotes
Acknowledgements
We thank Leslie Miller for performing initial data analysis for this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.