
Abstract
Despite the well-documented link between eating disorders (EDs) and female infertility, it is unknown how EDs or disordered eating behaviors (DEBs) influence overall parity in early adulthood. Using longitudinal data, we examine whether EDs or DEBs during adolescence are linked to the number of children born to young women in early adulthood. We find that EDs or DEBs are associated with increased odds of having three or more children compared to no children in adulthood, even when we account for delinquency and sexual behaviors.
Introduction
Although research has shown that eating disorders (EDs) during adolescence can have lasting effects on health, very few studies have explored the role that EDs or disordered eating behaviors (DEBs) play on the transition to adulthood. For example, it is well established that women with EDs are more likely to experience infertility and difficulty becoming pregnant (James 2001; Linna et al. 2013; Stewart et al. 1990); however, it is unclear how EDs may be influencing the transition to parenthood more broadly, such as age at entry into parenthood, number of children, and birth timing. Examining the fertility timing and overall parity of women with EDs is important given recent evidence linking EDs with higher rates of unintended pregnancy (Bulik et al. 2010; Easter, Treasure, and Micali 2011). Using a nationally representative sample from the National Study of Adolescent and Young Adult Health, a longitudinal study of adolescents, we seek to empirically account for how EDs or DEBs in early life may influence women’s childbearing in early adulthood. We also test two potential mediating factors that may explain the relationship between EDs or DEBs and parity in early adulthood: adolescent delinquency and sexual risk taking. The primary research objective of this study is to determine whether EDs or DEBs influence the number of children young women have by the time they reach early adulthood. Our approach is novel in that we utilize a nationally representative sample and apply a sociological life course framework to fertility research on women with eating disorders, which has generally been studied from a biomedical perspective utilizing clinical samples.
Background
Eating Disorders and Disordered Eating Behaviors
EDs, defined here as the range of psychological disorders characterized by abnormal or disturbed eating habits identified by the Diagnostic Statistical Manual of Mental Disorders (DSM-5) (America Psychiatric Association 2013), often begin in adolescence, with an average age of diagnosis at 17 to 18 years (Fairburn and Harris 2003). Swanson et al. (2011) estimate that approximately 2.7 per 100,000 adolescents between the ages of 13 and 18 in the United States have an ED. Since many EDs are not diagnosed, these estimates are likely underrepresented measures of true prevalence. EDs are often chronic conditions that persist into adulthood, with full recovery only occurring for approximately half of adolescent patients (Yaeger and Andersen 2005).
DEBs are the behavioral symptoms of EDs, such as purging, binge eating, and non-purging compensatory behaviors (e.g., fasting or taking laxatives), and are much more common than diagnosed EDs (Stephen et al. 2014). DEBs are likely to develop during adolescence (Neumark-Sztainer et al. 2011, 2012); longitudinal studies indicate that DEBs increase from early to late adolescence, meaning an adolescent’s risk for developing and engaging in DEBs increases across adolescence (Neumark-Sztainer et al. 2011). The high prevalence of DEBs among adolescents and their correlation with adverse physical health and psychosocial outcomes (e.g., depression and weight gain) illustrates that DEBs have long-lasting impacts on well-being (Neumark-Sztainer et al. 2011, 2012; Stephen et al. 2014). Although DEBs have been traditionally utilized as proxy measures of EDs, DEBs are arguably clinically relevant independent of whether they evolve into full-fledged EDs based on diagnostic criteria.
We rely on a life course framework, which suggests that early life experiences influence later life outcomes (Elder 1998; Mortimer and Shanahan 2003). EDs often occur during the life phase called the transition to adulthood. During the transition, most adolescents have been dependent on parents but with age are transitioning into independence both financially and emotionally (Jekielek and Brown 2005). Some adolescents or young adults engage in behaviors or experience setbacks that place the young adult on a disadvantaged trajectory, leading to cumulative disadvantages later in life (Jekielek and Brown 2005). Adolescence and the transition to adulthood is often described as a time when individuals engage in risk-taking behaviors (Steinberg 2004), such as DEBs (Neumark-Sztainer et al. 2011). Given that adolescents who engage in risky behaviors are more likely to take subsequent or additional risks—for example, adolescents who engage in substance use are more likely to engage in risky sexual behaviors throughout the transition of adulthood (Taper et al. 2001)—the presence of EDs in adolescence or young adulthood may indicate a constellation of deviant or risk-taking behaviors.
Events, experiences, or sets of behaviors that result in a significant change to the life or health trajectory of an individual are referred to as “turning points” (Wheaton and Gotlib 1997). EDs and related risk-taking behaviors may act as a turning point, setting an individual on a different life path, thereby resulting in differential successes during the transition to adulthood. We seek to assess whether EDs disrupt or alter the transition to adulthood by affecting the fertility experiences of women. In order to assess EDs as a particular divergent experience, we need to account for the known etiology, associated deviant or risk-taking behaviors, and consequences of adolescent EDs or DEBs. Approaching EDs from a life course perspective is important practically because it improves our understanding of how EDs or DEBs may influence parenthood in early adulthood. This work is also important theoretically because it attempts to understand the validity of life course theory and life course concepts as they apply to EDs.
Underlying causes and risk factors
Gender is one of the most important risk factors predicting the development of EDs and DEBs. Females have been consistently shown to have a higher lifetime prevalence of EDs than males and are more likely to engage in DEBs (Hudson et al. 2007; Santos, Richards, and Bleckley 2007; Stephen et al. 2014). It is well established that females are more prone to societal pressures to maintain or achieve thinness (Grogan 2007). This study explores the relationship between EDs, DEBs, and fertility among a female-only sample for two main reasons. First, the meanings associated with EDs and DEBs are vastly different for men and women. For example, although both men and women with EDs or DEBs exhibit higher perfectionism (Bardone-Cone et al. 2007), characteristics of “perfection” differ by gender. Females with EDs or DEBs may place more value on their physical appearance than males with EDs or DEBs due to female-specific social pressures for thinness (Grogan 2007). Indeed, males with EDs don’t score as highly in bodily dissatisfaction and drive for thinness (Stanford and Lemberg 2012). Second, measuring fertility among men is more difficult, and because of their greater likelihood to be nonresident with their child(ren) (Sorensen 1997), the implication of early adulthood fertility differs substantially between the two groups. As a result, this study focuses exclusively on the experiences of women.
Earlier research suggested that lesbians have a more positive body image and might be less likely to engage in disordered eating (Morrison, Morrison, and Sager 2004; Striegel-Moore et al. 1990). Recent studies, however, suggest that sexual minority women are at higher risk for both purging and diet pill use (Austin et al. 2013). This suggests that in addition to experiencing minority stress, they are not exempt from heterosexist body standards for women (Watson et al. 2015), so it is important to explicitly include this factor in studies of young adults.
The home environment has an important influence on the development of EDs and/or DEBs (Jacobi et al. 2004); in a systematic review of the causes of EDs, Polivy and Herman (2002) identify negative family environments and lack of familial support during early childhood as major risk factors for EDs. EDs are often understood as coping mechanisms for the perceived lack of control or support in the home environment (Polivy and Herman 2002; Wagener and Much 2010). Many societies emphasize culturally idealized thinness, and individuals with EDs are aware of the importance of this ideal, internalize it, and perceive pressure from the media and their peers to be thin (Levine and Murnen 2009). Although researchers have grappled over how to change predominating cultural perspectives idealizing thinness (Levine and Muren 2009), increased positive social support from peers and other adults is protective against disordered eating and the development of EDs, thereby mitigating some of these unhealthy cultural pressures (Limbert 2010; McVey et al. 2003).
In addition, race/ethnicity and socioeconomic status (SES) have been found to influence female drive to thinness, with research indicating that Asian American and white women, particularly those from high SES backgrounds, are more driven to be “thin” than African Americans or Hispanics (Boyd et al. 2011). Therefore, it is commonly stated that racial and ethnic and class-specific identity group relations and dynamics shape female susceptibility to the thinness ideal of mainstream culture, which may be translating to differences in type-specific ED prevalence manifestation (Boyd et al. 2011). For example, white females and those from higher SES backgrounds experience higher prevalence of anorexia nervosa (Swanson et al. 2011), while African Americans and Latinos are found to have higher prevalence of bulimia nervosa (Franko et al. 2001; Marques et al. 2011).
Finally, evidence suggests that EDs are the result of genetic and epigenetic processes, that is, the interaction between the environment and genes (Campbell et al. 2011; Goodman et al. 2014; Strober et al. 2000). When individuals’ genetic predispositions interact with environments rich in potential risk factors, such as a stressful home environment, their likelihood of developing an ED or DEB increases. Indeed, there is a high risk of familial transference associated with EDs, where families “pass” EDs through the family environment, usually from parent to child (Polivy and Herman 2002; Strober et al. 2000). For example, mothers with EDs may have higher expectations for their daughter’s thinness and may be less positive about their daughter’s “attractiveness,” prompting the child to engage in DEBs (Polivy and Herman 2002). This makes understanding fertility behaviors of women with EDs and DEBs all the more important.
Fertility Consequences
There are two different approaches to examining the link between EDs and DEBs and fertility outcomes. Clinical studies indicate that women with prolonged or severe EDs may have difficulty getting pregnant as a result of physical health complications (James 2001; Linna et al. 2013; Stewart et al. 1990). It is well established that EDs and DEBs are associated with long-lasting mental and physical health consequences (Berkman, Lohr, and Bulik 2007; Hudson et al. 2007; Nicholls, Lynn, and Viner 2011; Norris et al. 2012; Swanson et al. 2011). More severe and prolonged EDs and DEBs have the most severe and longest lasting effects on physical and mental health (Yaeger and Andersen 2005). The physical health consequences of eating disorders, low body weight–related menstruation disruption in particular, have been linked to lifetime fertility problems (Freizinger et al. 2010), with women with EDs expressing difficulty becoming pregnant and/or experiencing longer times to conception (Easter et al. 2011). In terms of the influence of EDs on parity, or number of children born, Linna et al. (2013) found that women seeking treatment for EDs were more likely to be childless than the control group in an observational study utilizing a clinical sample. Based on this body of medical research, we might hypothesize that women with adolescent EDs or DEBs will have fewer children in early adulthood.
However, recent research indicates that women with EDs are at greater risk of experiencing an unplanned pregnancy, particularly those studies utilizing broader community samples (Bulik et al. 2010; Easter et al. 2011). We build on this research by proposing an alternative sociological perspective that may provide insight into recent findings linking EDs and unplanned pregnancy.
Deviant behavior and risky sexual behaviors: Adolescent decision making
Sociological research suggests an alternative understanding of the link between EDs/DEBs in adolescence or young adulthood and early adult fertility. Adolescent decision-making theory proposes that while adolescents are able to assess the risk, benefit, and consequences of a particular decision or behavior, adolescents or young adults see occasional or experimental involvement in health-threatening activities as less dangerous than do adults (Cohn et al. 1995) and may also overestimate their ability to recognize and avoid dangerous situations or behaviors (Cohn et al. 1995). Adolescents or young adults with low self-esteem or negative self-image may be even less likely to appropriately understand or respond to the risk or consequences of and more likely to engage in risky behaviors (Smith, Gerrard, and Gibbons 1997; Wheeler 2010).
Similarly, disordered eating behaviors have been conceptualized as a form of internally directed deviance, resulting from negative self-image and low self-esteem (Sischo, Taylor, and Martin 2006). EDs and DEBs have been associated with other forms of externalized deviance and risk behaviors; for example, EDs and DEBs in adolescence are also associated with higher levels of delinquency and substance use (Piran and Robinson 2011; Stephen et al. 2014; Striegel-Moore et al. 2003); such risky behaviors are also commonly associated with a constellation of additional risk behaviors. Important to this study is their association with risky sexual behavior, such as early age of first sexual encounter and higher numbers of sexual partners, and early or unintended pregnancy (Naimi et al. 2003; Pugh et al. 1990; Yamaguchi and Kandel 1987).
Indeed, there is some evidence to conclude that young adults diagnosed with one or more psychiatric disorders, including eating disorders, are more likely to engage in risky sexual intercourse (non-condom use, higher number of partners) and have sexual intercourse at an early age (Ramrakha et al. 2000; Shrier et al. 2001). Young women with EDs or DEBs may be particularly prone to risky sexual behavior, including earlier ages of first sexual intercourse and higher number of sexual partners, due to their compromised self-esteem (Fisher et al. 1991). In addition, women with EDs or DEBs may also be less likely to use effective forms of contraception due to their assumption that they may be infertile and/or a reduced perception of risk (Bulik et al. 2010; Downs et al. 2004), resulting in higher rates of unplanned pregnancy (Bulik et al. 2010; Easter et al. 2011).
Because unintended pregnancy is a risk factor for subsequent, unintended pregnancies (Kuroki et al. 2008), women with EDs or DEBs may not only be at risk of early entry into parenthood but of experiencing multiple births at a younger age than their unafflicted peers. Our study builds on research that has shown that women with EDs are at greater risk of experiencing unplanned pregnancy, particularly those studies utilizing broader community samples (Bulik et al. 2010; Easter et al. 2011). Based on the sociological literature, we expect EDs and DEBs to be associated with higher parity in early adulthood.
Clinical Versus Nonclinical Samples
Prior research examining the influence of eating disorders on fertility has relied on clinical sampling or clinical measurement (i.e., diagnosis) of an ED. To be diagnosed with an ED and included in a clinical study, an individual must have access and the desire to seek the help of a medical professional. As Cohen and Cohen (1984) note, clinical samples are therefore biased toward cases of long duration or greater severity and/or capture individuals actively seeking treatment for an illness or condition, thereby limiting the generalizability of clinical findings to the broader population. This reduces the generalizability of prior clinical studies that examine the influence of EDs on fertility experiences to diverse populations.
Conversely, it can be difficult to examine the influence of EDs on fertility within community or national samples, which better represent the general population, given that there are very small subsamples or cases of individuals who are diagnosed with EDs within these samples. This has led to the use of proxy measures of EDs, including DEBs, in place of clinical diagnosis within nonclinical studies (Stephen et al. 2014; Tabler and Utz 2015). Asking respondents about DEBs that are indicative of eating disorders in community- or population-based surveys is an alternative way of assessing EDs that moves beyond utilization of medical services and may be able to capture individuals who are underrepresented in samples of individuals who are diagnosed and/or actively seeking treatment for an ED.
Current Study
In the current study, we examine whether EDs and DEBs are additional risk factors for higher parity in early adulthood while taking into account other individual characteristics and behaviors, including delinquency and risky sexual behaviors. This study utilizes a nationally representative, longitudinal sample of adolescents and young adults in the United States and examines a combined measure of self-reported diagnosis and disordered eating behavior. The unique sampling design and ED measurement techniques in this study allow for greater generalizability to the US population than prior work examining the influence of EDs on fertility experiences. This study is important because it has the potential to expand our current understanding of the transition to parenthood of women with adolescent EDs and DEBs beyond strictly biomedical considerations. Indeed, most fertility studies sample women with anorexia nervosa and/or women who are trying to get pregnant and are therefore unrepresentative of the overall fertility experiences of women with EDs or DEBs. This study provides a sociological approach to the topic and broadens our understanding of the parenthood experiences of women with EDs or DEBs.
Methods
Data
The data used in this study come from the full (restricted access) sample National Study of Adolescent and Young Adult Health (Add Health), collected by the Carolina Population Center from 1994 to 2008 (Harris et al. 2009). Add Health used a stratified sampling design and followed the same cohort of randomly selected youth from adolescence to young adulthood, collecting data at four different time periods. Wave 1 was collected between 1994 and 1995, when the cohort was aged 11 to 18; Wave 2 was repeated in 1996; Wave 3 between 2001 and 2002; and Wave 4 was collected in 2008 when the cohort was approximately aged 24 to 32. The current study uses data from Waves 1, 3, and 4. Specifically, the early life contexts and demographic information were selected from Wave 1. Information about ED diagnoses and behaviors are only available at Wave 3. Finally, Wave 4 provides measures of education, health, marital status, and entry into parenthood during early adulthood.
Sample
Of the 10,480 women in the full data set, approximately 20 percent (n = 2,128) of respondents were lost by attrition between Waves 1 and 4. An additional 3,008 individuals had missing values on key variables. Finally, an additional 307 individuals were dropped due to missing longitudinal sample weights. This left a final analytic sample of 5,037 female respondents. 1 Table 1 presents the descriptive profile of the estimation sample, which was generated using Wave 4 longitudinal sample weights for individuals who have responded to Waves 1, 3, and 4 (Chen and Chantala 2014).
Descriptive Statistics of Estimation Sample (n = 5,037).

Note. Data come from ADD Health. Results are generated based on sample estimation using the longitudinal sample weight (Wave 4) of individuals interviewed at Waves 1, 3, and 4 constructed by ADD Health. ED = eating disorder; DEB = disordered eating behavior; SD = standard deviation.
Measures
Dependent variable
Parity was measured in Wave 4, when participants’ average age was 28. The national average age of first birth for women in the United States is approximately 26 years (Mathews and Hamilton 2006). We use the measure parenthood, a categorical measure of number of children, which compares those with zero children to those with one or two children and to those with three or more. We have selected this measurement of parity for three reasons; first, given prior research indicating that women with EDs are more likely to be childless than unafflicted peers (Linna et al. 2013), we selected childlessness as our baseline outcome. In addition, the perceived benefits or burdens of having children are different for women who are childless compared to women who have one or two children (Callan 1986). For this reason, we selected women with one or two children as a comparison group. Finally, given that the average completed fertility of women in the United States is approximately two children (Martin et al. 2015), we grouped women with three or more children as a final comparison group because they represent a subsample of women who have higher than average fertility.
Primary independent variable
Survey questions related to EDs and DEBs were only asked in Wave 3. Self-identified ED diagnosis was assessed with a single yes/no question, “Have you ever been diagnosed with an eating disorder?” We further identified individuals participating in unhealthy compensatory behaviors directed at maintaining or losing weight. Respondents were asked, “During the past seven days what did you do to keep from gaining weight?” Individuals who reported behaviors “made yourself vomit, fasted or skipped meals, took laxatives, took diet pills, or diuretics” were coded as having DEBs. We also identified individuals with binge eating symptoms. We included those who reported having “eaten so much in a short period of time that [they] would have been embarrassed if others had seen them do it, in the past seven days” as having a DEB. The measure labeled ED or DEB combines individuals who self-identify as having been diagnosed with an ED with those who engage in unhealthy weight-related compensatory behaviors and/or exhibit binge eating symptoms.
Covariates: Risk behaviors
In this study, we examine whether risk behaviors commonly associated with eating disorders, including delinquent and risky sexual behaviors, may mediate the relationship between EDs or DEBs and parity. Delinquency was measured at Wave 3 and is a composite score of 12 items. Questions evaluated how often in the past 12 months the individual engaged in delinquent behavior. Examples include “How often did you sell marijuana or other drugs?” and “How often did you steal something worth more than $50?” Potential responses include 0 = never, 1 = one or two times, 2 = three or four times, and 3 = five or more times. Scores can range from 0 to 36, with higher scores indicating more delinquent behaviors (α = .710).
Three variables provide information on risky sexual behaviors. Two were measured at Wave 4. Age at first vaginal sex is measured in years (range, 11–30). 2 Number of sexual partners represents a self-reported, estimated count of total number of sexual partners (range, 1–100). Contraceptive use was measured at Wave 3 and is a categorical measure of contraceptive type, comparing those using no birth control in the past 12 months to those using at least one effective form of birth control (including the pill, birth control implant, injection or shot, or diaphragm) and to those using ineffective forms of birth control (including natural planning techniques and emergency contraception).
Additional covariates
We further account for etiological factors, demographic characteristics, and outcomes commonly associated with EDs and DEBs. This study includes covariates that describe their early life context (in this case, early adolescence), the demographic characteristics of the individual, as well as the health and socioeconomic characteristics of the individual in early adulthood. 3
Two variables, measured at Wave 1, provide information on the individual’s early life context. Respondents were asked to choose from six potential categories to specify the highest educational level of their mother (mother’s education). Potential responses include less than high school up to post baccalaureate degree. Respondents were also able to specify if they were unsure of their mother’s highest level of education. The Protective Environment Scale captured the supportiveness of the child’s social network using eight Likert-scale items that measured perceived social support from persons or groups in the child’s social network. For example, respondents were asked, “How much do you feel that adults care about you?,” with 1 = not at all, 2 = very little, 3 = somewhat, 4 = quite a bit, and 5 = very much. Other questions assessed the perceived support from teachers, parents, friends, and family members. Based on the sum of all eight items, scores ranged from 8 to 40, with higher scores representing more supportive social environments. The scale was found to have sufficient internal consistency (α = .782).
Race/ethnicity is a self-identified measure of an individual’s race or ethnicity, measured at Wave 1. Potential categories include Hispanic, non-Hispanic white, non-Hispanic black, non-Hispanic Asian, and non-Hispanic other. We selected these categories due to sample size limitations; more detailed racial and ethnic groups were too small for meaningful comparisons by ED or DEB. The scale was found to have sufficient internal consistency (α > .703). Age, measured in years, was calculated by subtracting birth date from the survey date (of Wave 4). Sexual orientation 4 was measured at Wave 4. This dichotomous variable compares those who identify as being entirely heterosexual (i.e., are exclusively attracted to individuals of the “other” sex) to individuals specifying having any level of same-sex attraction.
Health was measured at Wave 4, when participants were in early adulthood. Mental health was measured by a version of the Center for Epidemiology Studies-Depression Scale (CES-D; Radloff 1977). The CES-D is a composite score of 10 items indicating the presence of depressive symptoms such as “You could not shake off the blues, even with the help from family and friends, in the past seven days.” Possible values of the combined 10-item scale ranged from 0 to 30, with higher scores indicating higher levels of depressive symptoms (α = .83). General health was measured by self-report of global health. Respondents were asked, “How is your general health?” Responses fall on a scale ranging from 0 = poor to 5 = excellent. Body Mass Index (BMI) was calculated by first using the height and weight data measured by the interviewer at Wave 4. Self-reported height and weight was used if the respondent had missing measured data.
In addition, we control for the education of respondents at Wave 4. Educational attainment is a measure of years of completed education. Using the International Standard Classification of Education (ISCED), categorical responses to the question “What is the highest level of education that you have achieved to date?” (i.e., completed high school, some college, completed master’s degree) were transformed into years of completed school. 5
Finally, we controlled for the marital status of the respondent in early adulthood (Wave 4). Married is a dichotomous measure of having been married at least once.
Analytic Plan
In a first step, we present the unadjusted group differences between those with and without EDs/DEBs in our dependent and selected independent variables. In a second step, we estimate a series of nested multinomial logistic regression models. In a third step, we presented predicted probabilities to assess the substantive impact of EDs and DEBS on fertility patterns. All statistic results are based on sample estimates generated using Wave 4 longitudinal sample weights (for individuals who responded to Waves 1, 3, and 4) based on guidelines for analyzing Add Health data (see Chen and Chantala 2014).
Results
About 3.9 percent of the sample reported an eating disorder diagnosis based on sample estimations. A higher proportion of individuals, 22.3 percent, reported engaging in at least one disordered eating behavior. In addition, 23.5 percent of females reported having been diagnosed with an ED or engaging in at least one DEB (Table 1). Table 2 presents group differences that indicate initial support for our hypothesis as women with an ED or DEB were more likely to have had three or more children by early adulthood than those without and ED or DEB (p < .001, based on chi-square tests). In addition, women with an ED or DEB report significantly higher levels of adolescent delinquency (p < .001), younger ages at first vaginal sex (p < .001), and higher numbers of sexual partners (p < .001) than their unafflicted peers. Contraceptive use was not found to be correlated with ED or DEB. We also see that identifying as non-heterosexual was positively correlated with identifying as having an ED or DEB (p < .001). Respondents with an ED or DEB also reported lower general health (p < .001), higher depression scores (p < .001), and higher BMI in adulthood (p < .001). In addition, women with ED or DEB experience lower social support in adolescence (p < .001).
Unadjusted Empirical Relationship between ED or DEB and Selected Covariates.
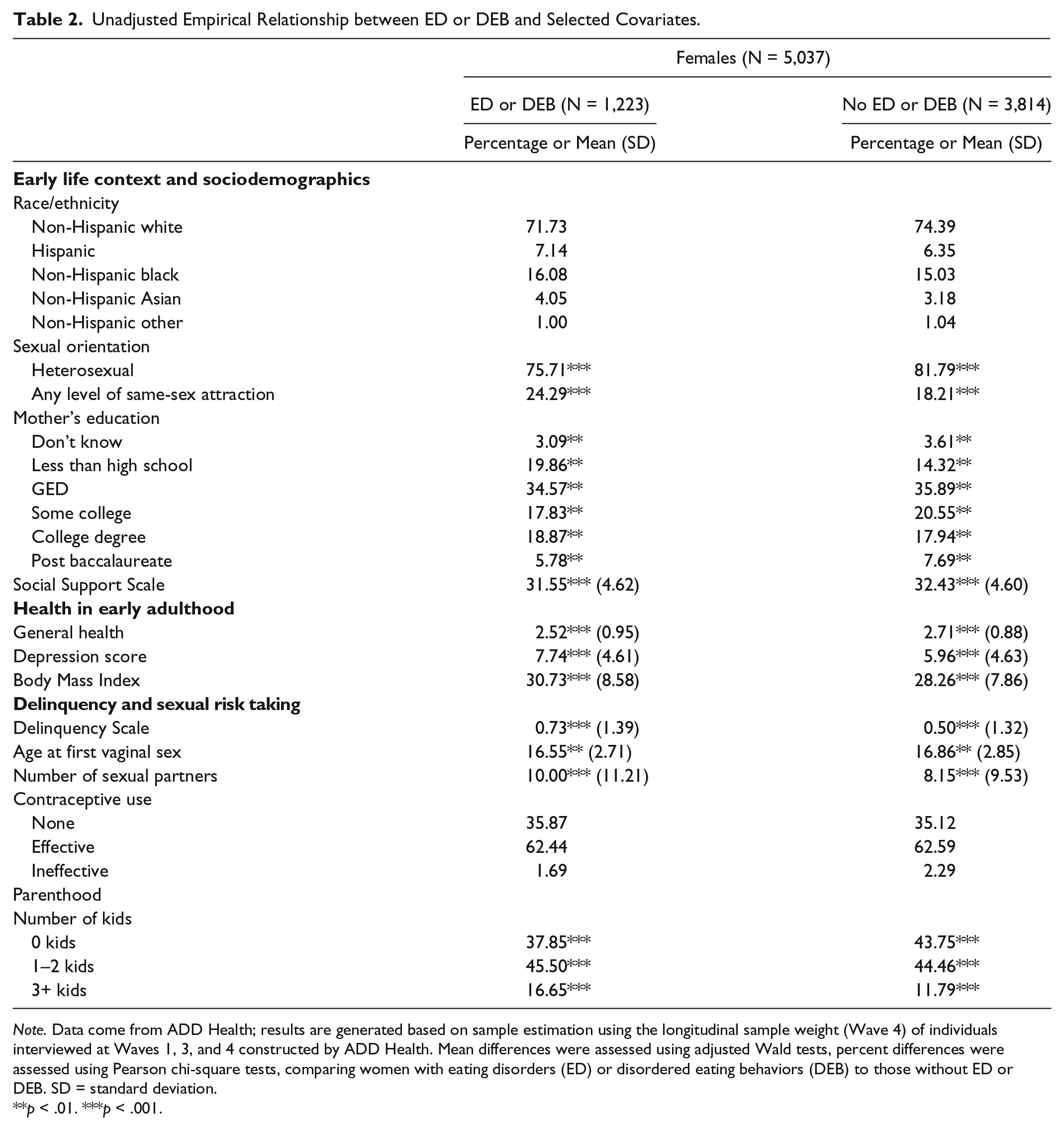
Note. Data come from ADD Health; results are generated based on sample estimation using the longitudinal sample weight (Wave 4) of individuals interviewed at Waves 1, 3, and 4 constructed by ADD Health. Mean differences were assessed using adjusted Wald tests, percent differences were assessed using Pearson chi-square tests, comparing women with eating disorders (ED) or disordered eating behaviors (DEB) to those without ED or DEB. SD = standard deviation.
p < .01. ***p < .001.
In a next step, we test whether this difference in fertility patterns remains once we estimate multivariate models (Table 3). We first present a model that includes ED/DEB and the full set of demographic controls, followed by a model that also includes delinquency and sexual risk-taking behaviors.
Multinomial Logistic Regression Results: Relative Risk Ratios.

Note. Data come from ADD Health; estimates are ran using the longitudinal sample weights (Wave 4) provided by ADD Health for individuals sampled at Waves 1, 3, and 4. Relative risk ratios are reported; linearized standard errors in parentheses; ED = eating disorder; DEB = disordered eating behavior.
p < .05. **p < .01. ***p < .001.
Compares those who identify as having any level of same-sex attraction to those who identify as 100 percent heterosexual (reference group).
Reference group is non-Hispanic white.
Reference group is mother with GED or high school diploma.
Compares those who have never been married to those who have been married at least once (reference group).
Higher scores indicate more depressive symptoms.
Higher scores indicate higher quality of self-rated general health.
Higher scores indicate more delinquent behaviors.
Reference group is effective contraception.
In Model 1, we compare those without children to those who have one or two children in early adulthood (Model 1, column 1) and to women who have three or more children (Model 1, column 2). The individual controls have the expected effects: Older individuals and those who are already married have greater relative risk to have children compared to having no children. Compared to non-Hispanic whites, African American women are more likely to have children in early adulthood, and higher levels of education (both respondents’ and mother’s) are associated with reduced risk of parenthood (at both levels). We find that sexual minority women are less likely to already have children compared to those who do not indicate any same sex attraction.
These results provide us with partial support for our hypothesis that young women with an ED or DEB had a higher relative risk ratio for early transition to parenthood. While having an ED or DEB does not affect the relative risk of having one or two versus remaining childless, there is evidence that ED/DEB women have a greater relative risk of having three or more children compared to being childless in early adulthood (relative risk ratio = 1.48, p < .05).
In Model 2 we further include delinquency and risky sexual behaviors, a set of theoretically relevant factors that potentially mediate the relationship between ED or DEB and parity. Similar to Model 1, Model 2 compares those without children to those who have one or two children in early adulthood (Model 2, column 1) and to women who have three or more children (Model 2, column 2). Contraceptive use, delinquency, and number of sexual partners did not have direct effects on the relative risk of having one or two children versus remaining childless or having three or more children versus remaining childless. Age at first vaginal sex has a significant effect, where for each one-year delay in age at first vaginal sex, women’s relative risk of having one to two children versus remaining childless is reduced by 14 percent (p < .001), and their relative risk of having three or more children versus remaining childless is reduced by 23 percent (p < .001). However, even when we include these potential explanatory variables, ED or DEB remains a significant predictor of parity, where women with ED or DEB have an increased relative risk of having three or more children compared to being childless in early adulthood by 46 percent (p < .05).
We also explored additional models that compared other models with different combinations of delinquency and sexual risk taking, and models presented here provide the best fit (full set of models available on request). It is important to note that in supplementary analyses (not shown) where we excluded those engaging in DEBs, EDs remained a significant positive predictor of having three or more children in early adulthood.
Relative risk ratios do not take into account the underlying probabilities, so large differences reported in regression tables may not translate in substantive differences. In a third analytic step, we estimated probabilities for women with and without ED and DEB, with all other characteristics held at the overall sample mean. Overall, the probability of having three or more children is relatively small, which is not surprising since our oldest respondents are only 33 years old. However, we do find that those with ED or DEB have a significantly greater probability to report three or more children than those without (see Figure 1) (p < .05).

ED or DEB and the probability of having three or more children.
Discussion
This study expands existing research on EDs and DEBs beyond health domains by using a nationally representative community-based survey of adolescents to explore whether EDs or DEBs had an effect on parenthood in early adulthood. Despite previous research linking infertility and compromised reproductive health outcomes among women with EDs (Linna et al. 2013), our findings indicate that adolescent women who experienced EDs or DEBs in early life were more likely to have three or more children by early adulthood. This finding holds even when we take into account adolescent risk-taking and sexual behavior. This suggests that DEBs and particular diagnosed EDs have an independent effect on the odds of entering parenthood early, net of behaviors that increase the risk of early parenthood.
Our finding that women with EDs or DEBs are more likely to have three or more children in early adulthood indicates that women with EDs and DEBs may be entering motherhood at an increased tempo compared to their peers, particularly when we consider contemporary trends toward reduced or delayed fertility among U.S. females (Martin et al. 2015); the United States has seen a steady decline in births to women under the age of 30 and an increase in birth rates among women aged 30 to 39 (Martin et al. 2015). This finding has important practical implications. Becoming pregnant while engaging in DEB places both mother and child at risk, and given the genetic and familial nature of EDs, the children successfully born to women with EDs are in and of themselves at greater risk of engaging in unhealthy eating behaviors (Pike and Rodin 1991; Strober et al. 2000). Women with EDs or DEBs may be making different fertility decisions that move beyond sexual risk taking. Due to survey limitations, we were unable to account for adolescent fertility intentions, but differences in fertility intentions between women with or without EDs or DEBs may help explain their differences in completed fertility. Additional research on the attitudes of women with EDs or DEBs toward parenting, their birth timing, and lifetime parity is thus arguably important not only for elucidating the potential health risks of these women but those posed to their children.
Early childbearing is known to lower the overall educational attainment of young women (Klepinger, Lundberg, and Plotnick 1995). Raising multiple children in early adulthood may place women with EDs or DEBs at cumulative risk for financial and emotional distress, given previous results indicating that young women who experience EDs or DEBs face barriers in achieving socioeconomic independence in early adulthood (Tabler and Utz 2015), and higher rates of depression and anxiety (Hudson et al. 2007; Santos et al. 2007). Disadvantaged women have been found to experience heightened insecurity and fears surrounding whether or not they may be able to achieve motherhood, driving them to pursue it at early ages (Edin and Kefalas 2005). Similarly, becoming pregnant may be more highly valued by women with EDs or DEBs because they fear they might not have the opportunity to achieve a successful pregnancy (or pregnancies) given the link between low self-esteem and unhealthy eating behaviors (Martyn-Nemeth et al. 2009). Both qualitative and quantitative research on the meaning of motherhood among women with EDs would enrich our understanding of the family formation intentions of women with EDs and DEBs. Documenting the long-term implications of adolescent ED and DEB is important from a public health perspective, but it also points to sociological implications. Beyond “deviant” behavior and sexual risk taking, EDs shape young women’s entry into adulthood, and additional research needs to understand how the gendered notion of the body, the striving for perfection, and the motivations for early entry interact among women with EDs. Our research establishes that adolescent experiences, EDs and DEBs in particular, have life course–altering potential.
There are several limitations of this study; due to data limitations, we were unable to distinguish types of EDs or measure the severity or duration of reported DEB. We expect that those with lifetime diagnoses or prolonged untreated behaviors would be more likely to experience fertility complications due to the physical health complications commonly associated with severe and ongoing EDs and DEBs. Finally, our small sample sizes of minorities with EDs or DEBs limited our ability to explore intersectionalities, such as racial/ethnic or gender differences, in outcomes. For example, in this study, only 100 non-Hispanic Asians were identified as having ED or DEBs. Future research should explore the similarities and differences in how EDs or DEBs influence parenthood for racial/ethnic subgroups and both males and females. In addition, these studies should include additional factors, such as fertility intentions or educational aspirations, which may shape the relationship between ED or DEBs and fertility and are likely to vary by particular subpopulations.
The current study uses a nationally representative sample of adolescents, allowing for a comparison of those with ED diagnoses or related behaviors to those without such behaviors. This provides a case-control type of design and allows for better modeling of potential consequences of EDs or DEBs. Not to mention, the addition of extensive control variables afforded by a comprehensive survey like Add Health allowed for us to control for life course processes that would not have been possible with clinical studies of more limited scope or covariates.
In conclusion, while existing medical research has commonly stated that EDs result in fertility issues (Linna et al. 2013), this study has expanded our understanding of the childbearing choices of individuals with EDs or DEBs. Most notably, young women who have experienced EDs or DEBs are more likely to have multiple children in early adulthood even when we account for behavioral differences in risk-taking and sexual behaviors. EDs in early life may represent a turning point that sets women on a different trajectory of opportunities and constraints in early adulthood compared to women without EDs or DEBs.
Footnotes
Acknowledgements
This research uses data from Add Health, a program project directed by Kathleen Mullan Harris and designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill, and funded by grant P01-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 23 other federal agencies and foundations. Special acknowledgment is due Ronald R. Rindfuss and Barbara Entwisle for assistance in the original design. Information on how to obtain the Add Health data files is available on the Add Health website (![]() ). No direct support was received from grant P01-HD31921 for this analysis.
). No direct support was received from grant P01-HD31921 for this analysis.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding from the National Science Foundation-Doctoral Dissertation Research Improvement Grant (NSF-DDRIG 11-547) (PI: Rebecca Utz; Co-PI: Jennifer Tabler) and the Consortium for Family and Health Research Internal Pilot Grant (C-FAHR), University of Utah (PI: Jennifer Tabler) supported this research.