
Abstract
Introduction/Objectives:
An unhealthy relationship with food can lead to disordered eating in adolescence, highlighting the importance of screening. This study describes the frequency of disordered eating behavior among female adolescents, as well as associated characteristics and health behaviors.
Methods:
Data are from a multidimensional risk factor screening survey administered at a university medical center’s adolescent clinic from 2016 to 2018. The instrument was adapted from existing screening tools such as the Rapid Assessment for Adolescent Preventive Services (RAAPS), the American Medical Association’s Guidelines for Adolescent Preventive Services (GAPS), and the Youth Risk Behavior Survey (YRBS). Analysis was limited to self-reported responses provided by females aged 10 to 21 years (N = 915). Statistical analyses included chi-square tests and independent sample T-tests.
Results:
Of the N = 915 females who reported on disordered eating behavior, n = 57 (6.2%) had engaged in some form of disordered eating behavior within the past 12 months. Disordered eating was significantly associated (P < .001) with not consistently wearing a helmet while biking, having tried e-cigarettes, being bullied in the past 30 days, having an adverse childhood experience (ACE), and being African American (P = .005). Subgroup analysis of the relationship between disordered eating and bullying, by race, yielded significant findings: disordered eating was more highly associated with being bullied in the past 30 days among African American females (P = .038). The relationship between disordered eating and ACE was also significant (P < .001) among Caucasian girls when stratified by race.
Conclusions:
Adolescent risk behaviors often co-occur, and disordered eating behavior may be differentially observed by race. Findings highlight the importance of education and screening to prevent the development of disordered eating, and identify those who may be struggling. These results can be useful to community health education and in healthcare to develop and implement health promotion and eating disorder prevention strategies. Further studies are needed to assess additional factors that promote or protect against disordered eating to improve prevention.
Introduction
As adolescents become independent and begin to take greater responsibility for personal health including diet and exercise, they may also engage in risky behaviors such as unhealthy eating, nicotine use, sexual activity, and not using seatbelts and helmets. The development during adolescence of health-compromising habits and risky behaviors can have short- and long-term consequences, making health education critical. The life-course framework states that early life events and lifestyle choices made as children and young adults influence later health outcomes. 1 Adolescent behaviors contribute to adult chronic health conditions such as cardiovascular disease, cancer, and stroke, and contribute to adolescent mortality from unintentional injuries, substance use, and mental health struggles. 2
Since risky adolescent behaviors are largely preventable, it is critical to screen for health behaviors and intervene before they become adulthood habits. Health education and screening tools form the cornerstone of adolescent care. Providing health education to adolescents about their actual and potential risky behaviors is fundamental to promoting health, preventing disease or injury, and motivating positive behavior change. Healthy People 2030, a national health promotion and disease prevention initiative of the Office of Disease Prevention and Health Promotion, provides a framework to evaluate and strengthen efforts to improve the health and well-being of all people. 3 Among its adolescent health objectives is to increase annual preventive health care visits, to promote access to screenings, health counseling, and interventions. Healthy People 2030 emphasizes the importance of screening during adolescence because establishing healthy behaviors early can be more effective than trying to change unhealthy habits during adulthood.
Among the significant adolescent risk behaviors is an unhealthy relationship with food that can lead to disordered eating. Professionals working with adolescents must understand when eating behaviors are healthy and normal and when they shift into disordered eating behaviors that risk progressing to clinical eating disorders (EDs). Healthy eating is when one mindfully consumes food when hungry and is able to stop when full. People exhibiting healthy eating also incorporate different types of food into their diets and generally have a positive body image. Disordered eating describes a variety of abnormal or unusual eating behaviors specifically used to achieve or maintain a lower body weight, including restricting food intake, rigid dietary rules, exercising to burn calories or in response to eating, misuse of laxatives or other substances, binge eating, and purging. 4
The key differences between disordered eating and EDs are frequency and degree of severity. An individual with disordered eating habits often engages in some of the same behaviors as someone with EDs but less often or less severely. This distinction is important for this study, and also important to make clinically; just because someone falls short of the diagnostic criteria for an ED does not mean that person is maintaining a healthy relationship with food. Extreme dieting was the most important predictor of developing an ED in 14 and 15 year olds, with those who dieted moderately 5 times more likely to develop an ED, and those who practiced extreme restriction 18 times more likely to develop an ED than those who did not diet. 5 Screening for disordered eating behaviors, and associated behaviors, is critical to preventing the development of an ED and identifying adolescents struggling with an ED.
Literature regarding disordered eating often pertains to clinical threshold EDs as defined by the DSM-5 and does not concern subthreshold disordered eating behaviors. For this reason, the exact prevalence of sub-threshold disordered eating behaviors among adolescents or any population is not well-understood. One study aiming to understand disordered eating behavior in adolescents across 15 years found that nearly 51% of female adolescents and 34% of male adolescents engaged in at least one disordered eating behavior. 6 These rates are extremely high, especially when compared to the prevalence rates of EDs; according to the DSM-5, the 12-month prevalence of anorexia nervosa, bulimia nervosa, and binge-eating disorder among young females is 0.4%, 1.5%, and 1.6%, respectively. 7 This emphasizes that more research needs to be done in regard to sub-threshold disordered eating behaviors as they impact larger groups of adolescents and these behaviors are predictors of going on to develop an ED.
Additionally, few studies have investigated associations between disordered eating behaviors and other adolescent risk behaviors. Significant research regarding adolescent risk behaviors exists, but few studies focus specifically on disordered eating as a risk behavior.8,9 Prevention and screening of risk behaviors such as disordered eating are critical to set the emerging adult on a trajectory of wellness. Understanding sub-threshold disordered eating behaviors and how they relate to other behaviors in adolescence is important for detecting and preventing an ED. This paper examines the prevalence of disordered eating among adolescent girls and identifies associated characteristics and health behaviors to facilitate early detection and prevention efforts in schools and healthcare settings.
Methods
This survey and IRB approved research (Georgetown University IRB, Biomedical Committee, 2015-0787: Pediatric Health Promotion Program) were conducted at a university medical center’s adolescent clinic. Adolescents self-reported on a multi-item questionnaire administered via electronic tablet as part of standard care. This component of the study was conducted as a quality improvement initiative to monitor population-level prevalence of adolescent risk behaviors, and how these behaviors may have changed over time following screening program implementation. The instrument was a composite risk behavior survey consisting of 70+ items adapted from the Rapid Assessment for Adolescent Preventive Services (RAAPS), the American Medical Association’s Guidelines for Adolescent Preventive Services (GAPS), and the Youth Risk Behavior Survey (YRBS).2,8,9 Most items were yes/no or structured responses, and data were originally collected from 2016 to 2018. Responses were used during patient visits to guide conversations between patients and their healthcare providers.
The target population for this study was all adolescents being seen in this university-based adolescent clinic from 2016 to 2018 and the analytic sample was limited to female adolescent patients who visited the clinic during the sampling period. The total number of adolescents that responded to the survey was 2801 and the analytic sample includes 915 adolescent females whose ages ranged from 10 to 21 years old (M = 14.4, SD = 2.0).
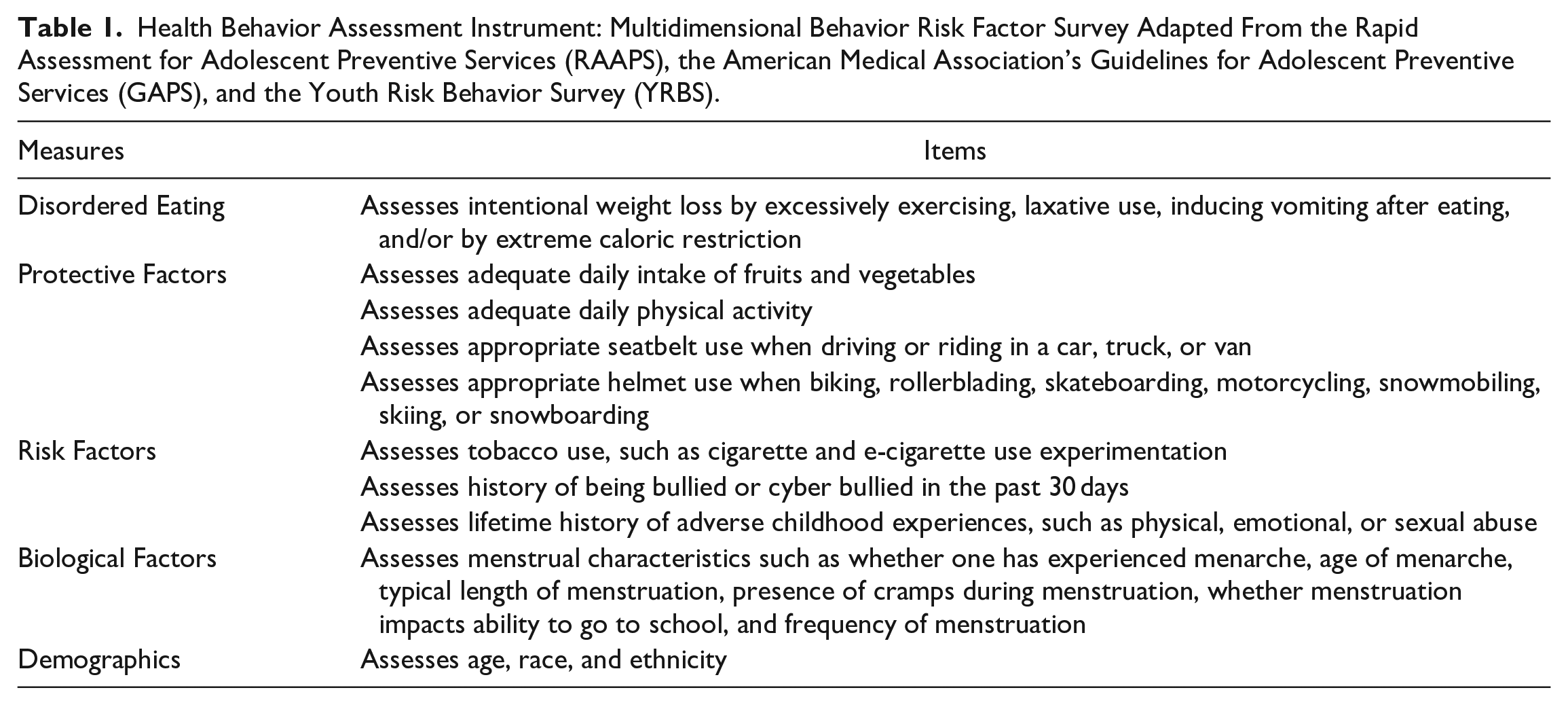
Instrument items used to assess disordered eating, protective factors, risk factors, biological factors, and demographics appear in Table 1. The main outcome, disordered eating, was defined as a positive response to the following survey question about engaging in inappropriate behaviors for weight control: “In the past 12 months, have you tried to lose weight by excessively exercising, taking diet laxatives, making yourself vomit (throw up) after eating, or starving yourself?” The biological factors found in Table 1 were used to construct a new variable, early menstruation, that was used in data analysis and is found in Table 2. All other items found in Table 1 were individually utilized in the bi-variate analyses found in Table 2. Statistical secondary data analyses were conducted using SPSS software. Descriptive statistics were used to make frequency tables and cross tabulations. Frequency tables were used to display the frequency of various outcomes for each variable or variable index. Cross tabulations were used to describe relationships between each independent variable with the dependent variable (disordered eating). Chi-square tests were used to determine whether there was an association between each categorical independent variable with the dependent variable. Independent sample T-tests were used to compare the means of each continuous independent variable with the dependent variable to determine whether the associated population means are statistically different (P < .05).
Health Behavior Assessment Instrument: Multidimensional Behavior Risk Factor Survey Adapted From the Rapid Assessment for Adolescent Preventive Services (RAAPS), the American Medical Association’s Guidelines for Adolescent Preventive Services (GAPS), and the Youth Risk Behavior Survey (YRBS).
Bivariate Associations Between Adolescent Health Behavior and Disordered Eating.

Abbreviation: ACE, adverse childhood experience.
P < .05.
Results
In this sample of N = 915 adolescent girls, n = 57 (6.2%) reported engaging in disordered eating behavior in the past 12 months. Disordered eating in this sample was significantly associated (P < .001) with not consistently wearing a helmet while biking, having tried an e-cigarette, being bullied in the past 30 days, and experiencing at least 1 ACE (eg, physical violence or abuse). Additionally, disordered eating behavior was significantly associated with being African American (P = .005; Table 2).
Further inspection of the interaction between being bullied and engaging in disordered eating, stratified by race, revealed additional findings (Figure 1). Disordered eating was significantly associated (chi-square = 4.29, P = .038) with being bullied in the past 30 days among African American girls; 26.7% of African American girls who had been bullied in the past 30 days reported engaging in disordered eating behavior, compared to the 9.3% of African American girls who had not been bullied. Statistical significance (chi-square = 5.82, P = .016) was also found among Caucasian girls, but with lower prevalence rates: 11.1% of Caucasian girls who had been bullied in the past 30 days reported engaging in disordered eating behavior, compared to the 3.0% of Caucasian girls who had not been bullied. The relationship between being a bullying victim and disordered eating was shown to be significant across races (overall chi-square = 10.68). However, this effect was more pronounced in African American girls, as there was a doubling of the effect for African Americans compared to Caucasians.

Interaction among bullying and disordered eating stratified by race and interaction among adverse childhood experience(s) and disordered eating stratified by race.
The interaction among those who had an ACE and engaged in disordered eating, stratified by race, also presented a significant finding (Figure 1). The relationship between disordered eating and having an ACE was shown to be significant (chi-square = 17.48, P < .001) among Caucasian girls: 25.0% of Caucasian girls who had ever experienced an ACE reported engaging in disordered eating behavior compared to the 3.3% of Caucasian girls who never experienced an ACE. Among other protective and risk factors analyzed within this dataset, no significant findings emerged.
Discussion
These results reinforce and highlight the importance of health behavior screening and anticipatory guidance for disordered eating prevention and overall health promotion. The data show, as reflected in prior literature, that adolescent risk behaviors are often grouped, rather than isolated. 10 Adolescents tend to engage in multiple risk behaviors simultaneously, highlighting the importance of screening adolescent girls for a range of risk behaviors, including disordered eating, when trying to prevent and detect EDs. 1
There is consistent evidence that tobacco use is associated with body shape concerns and disordered eating behavior, with studies confirming tobacco use for appetite suppressant characteristics.11,12 Our finding regarding the correlation between e-cigarette experimentation and disordered eating behavior possibly reflects this hypothesis that tobacco products, including e-cigarettes, can be mis-used to suppress hunger. The association between disordered eating and e-cigarette use but not cigarette use could be explained by the recent increase in e-cigarette popularity among adolescents. 13 Counselors and healthcare providers should discuss tobacco use with their adolescent patients to determine the intent of such use as a further means of screening for disordered eating.
Results also indicate a relationship between having been bullied and disordered eating. This interaction was further emphasized when stratifying by race; both African American girls and Caucasian girls were shown to have significantly higher rates of disordered eating if they reported being bullied in the past 30 days compared to other races. Healthy People 2030 identified bullying as an emerging issue requiring further exploration, and these findings highlight the importance of this exploration. 3 If adolescent girls are shown to engage in disordered eating at higher rates when they have been victims of bullying, this will aid healthcare providers in screening for disordered eating and indicates that combating bullying may support disordered eating prevention.
A correlation between disordered eating and experiencing an ACE, such as suffering physical, sexual, emotional, or verbal abuse, was also seen. This interaction was further emphasized when stratified by race; Caucasian girls were shown to have significantly higher rates of disordered eating if they reported experiencing an ACE when compared to other races. These findings regarding bullying and ACEs support prior conclusions about the development of EDs, that teens with EDs were significantly more likely to have been bullied or teased,5,14 and prevalence rates of all types of childhood maltreatment appeared to be 2 to fourfold higher in ED samples than in healthy control samples. 15 This co-occurrence of disordered eating and specific hardships, such as experiencing bullying and ACEs, emphasizes the importance of screening for disordered eating behaviors among adolescents who report experiencing such events. Additionally, a study conducted in Sweden found that frequent childhood victimization correlated positively with disordered eating in adulthood, suggesting that being bullied is not only associated with disordered eating but can be a risk factor for it. 16
Additionally, the results indicate that being an African American female adolescent is correlated with risk for disordered eating behavior. EDs have historically been thought to primarily impact thin, white, affluent girls. These results validate recent research that this is not the case; many studies have shown EDs to be prevalent across diverse cultures and populations.17,18 This finding that disordered eating is significantly associated with being African American is noteworthy and indicates that more research is needed regarding disordered eating and EDs among African Americans.
Strengths of this study include the large sample size, the use of a standardized and comprehensive screening instrument, the assessment of a diverse and wide-ranging set of adolescent behaviors, and the focus on more general, sub-threshold disordered eating behavior rather than psychiatric eating disorder criteria. Limitations include the cross-sectional nature of the data collection, inability to establish the temporal relationship of the associations, and the possibility of recall bias among survey participants. Additionally, the possible presence of a parent or guardian while participants responded to the survey could have led to underreporting of the risky behaviors, only highlighting that the results of this study and prevalence rates of the risk behaviors are likely underestimations. Further studies that extend this research to males, are more longitudinal in design, and include a survey more specifically tailored toward screening for disordered eating are needed.
Conclusions
Education and screening are critical to understanding adolescent behavior and to encouraging healthy behaviors that promote positive health outcomes later in life. Results indicate that screenings for a variety of behaviors and comprehensive educational programs are needed across the public health sector to prevent the development of disordered eating and identify adolescents who may be struggling with disordered eating. More outreach and attention must focus on African American communities, since results show African American girls are at particular risk for disordered eating and related behaviors. Further research is needed to identify the complex factors related to disordered eating at the individual and population levels so that more effective detection and prevention efforts can be implemented.
Footnotes
Acknowledgements
The authors would like to thank the patients and providers of the adolescent clinic for their participation, and Tania Lobo and Felice Yang of the Survey, Recruitment, and Biospecimen Collection Shared Resource at Lombardi Comprehensive Cancer Center.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was made supported by the National Cancer Institute [CA192950, CA051008].