
Abstract
The integration of artificial intelligence (AI) into clinical decision-making has introduced unprecedented ambiguity regarding professional accountability when AI-assisted care results in adverse patient outcomes. Nurses, positioned as frontline users of AI clinical decision support systems, face a complex landscape where traditional notions of professional responsibility intersect with algorithmic opacity, shared decision-making processes, and evolving legal frameworks. This commentary examines the accountability challenges confronting nurses in AI-enabled practice environments, exploring the ethical tensions between following AI-CDSS recommendations and exercising independent clinical judgment. The commentary argues that clear frameworks for responsibility attribution, robust institutional policies, and strengthened professional guidance are urgently needed to protect both patients and nurses as AI becomes increasingly embedded in healthcare delivery.
Keywords
Introduction
The proliferation of artificial intelligence (AI) in healthcare has fundamentally altered the landscape of clinical decision-making. From predictive analytics that identify patients at risk for deterioration to diagnostic algorithms that analyze medical images, AI systems increasingly contribute to decisions that directly affect patient outcomes (Rajpurkar et al., 2022; Wei et al., 2025). For nurses, who serve as primary users of many AI clinical decision support systems (AI-CDSS), this technological transformation raises a critical question: when AI-assisted care results in patient harm, who bears responsibility?
This question is not merely theoretical. As AI systems become more sophisticated and more deeply embedded in clinical workflows, the potential for AI-related errors, whether through algorithmic failure, data bias, or inappropriate application, grows correspondingly. For example, AI-powered clinical decision support systems (CDSS) in nursing now span real-time patient deterioration prediction, sepsis early warning, automated nursing diagnoses, and medication safety alerts (Bi et al., 2025; Brydges, 2025). The CONCERN (Communicating Narrative Concerns Entered by Registered Nurses) early warning system, a nursing-led AI tool that analyses nursing documentation patterns to predict patient deterioration up to 72 hours before adverse events, exemplifies how AI is being embedded directly into frontline nursing workflows (Rossetti et al., 2021). Yet the legal and ethical frameworks governing professional accountability were developed for an era when clinical decisions were made exclusively by human practitioners. The resulting ambiguity places nurses in an increasingly precarious position, expected to incorporate AI-CDSS recommendations into practice while remaining accountable for their professional judgment, nursing actions, and documentation as members of the broader healthcare team.
For the purposes of this commentary, AI refers to nurse-facing, electronic health record-integrated systems including machine learning clinical decision support tools, predictive early warning systems, risk stratification algorithms, and AI-powered documentation systems. This commentary examines the accountability challenges these technologies create for nursing practice and proposes strategies for navigating professional responsibility in the AI era.
Throughout this commentary, “AI-assisted” is used to describe clinical practice in which AI systems inform or support decision-making, while “AI-CDSS” refers specifically to the technological systems that generate clinical recommendations.
Brief Review and Discussion
The Accountability Gap in AI–Assisted Care
Traditional healthcare accountability structures rest on clear lines of professional responsibility. Nurses are accountable for decisions made and actions taken in the course of nursing practice, with the expectation that professional judgment guides clinical decision-making (American Nurses Association, 2015). However, when AI systems contribute to or influence clinical decisions, this clarity dissolves. Qualitative research has documented nursing concerns about this ambiguity directly: nurses express uncertainty about who should be held accountable in cases where AI systems make errors or cause harm, noting that while traditionally nurses assume responsibility for direct care actions, the introduction of autonomous systems disrupts clear attribution of liability (Bodur et al., 2025). Similarly, a systematic review by Cao et al. (2025) identified that the absence of clear governance pathways for nursing predictive analytics and early warning systems amplifies ethical risks, including unclear responsibility attribution when algorithmic outputs contribute to clinical decisions. These concerns are consistent with broader findings in the implementation science literature, which identify accountability ambiguity as a key barrier to the safe adoption of algorithmic decision support in high-stakes clinical environments (Goddard et al., 2012).
The challenge is compounded by the multiple parties involved in AI-assisted care. When an adverse outcome occurs, potential responsibility may rest with the healthcare provider who acted on the recommendation, the institution that implemented the AI system, the developers who created the algorithm, or some combination of these parties (Pham, 2025). Current legal frameworks provide little guidance on how to apportion responsibility across this complex web of actors. Under existing malpractice law, liability typically rests on whether the healthcare provider met the standard of care, with courts judging the clinician’s conduct regardless of whether AI was involved (Gerke et al., 2020; Pham, 2025).
These accountability challenges can be understood through established theoretical lenses. Responsibility attribution theory, as applied to human–AI interaction, suggests that when outcomes are negative, humans tend to assign greater blame to the human user than to the AI system, viewing AI as a tool rather than an autonomous agent (Brailsford et al., 2025). This asymmetry places nurses in a structurally disadvantaged position: they absorb blame for adverse outcomes regardless of whether the AI contributed to the error. Furthermore, the principlist framework of biomedical ethics, encompassing autonomy, beneficence, non-maleficence, and justice (Beauchamp & Childress, 1994), offers a useful lens for examining ethical tensions in AI-assisted practice. The principle of non-maleficence demands that nurses do no harm, yet algorithmic opacity may prevent nurses from fully assessing whether following an AI-CDSS recommendation could cause harm. The principle of justice raises questions about equitable distribution of accountability across clinicians, institutions, and technology developers rather than concentrating liability on individual nurses.
The Double Bind: Following or Overriding AI–CDSS Recommendations
Nurses face a troubling double bind in AI-assisted practice. If a nurse follows an AI-CDSS recommendation that proves incorrect, they may be held liable for failing to exercise independent clinical judgment. Conversely, if a nurse overrides an AI-CDSS recommendation and an adverse outcome results, they may be held liable for departing from what the AI identified as appropriate care. Clinicians are increasingly concerned about malpractice exposure when AI recommendations conflict with their clinical judgment, creating anxiety about documentation, decision-making, and professional risk (Chew et al., 2025; Pham, 2025). This double bind resonates with the concept of “moral distress” in nursing ethics, where nurses experience psychological harm from being unable to act in accordance with their professional judgment due to institutional or systemic constraints (Jameton, 1984). AI systems that constrain or override nursing judgment without transparent rationale may intensify moral distress, particularly when nurses are held accountable for outcomes they could not fully evaluate or control.
This double bind is intensified by the emerging expectation that healthcare providers should use AI when available. Legal scholars have noted that as AI becomes more accurate and widely adopted, litigators may begin arguing that clinicians were negligent for underutilising advanced AI-CDSS tools (Chew et al., 2025; Cohen et al., 2014). Thus, nurses may face liability not only for errors when using AI but also for failing to use AI at all. This creates an impossible situation: nurses are expected to rely on tools they may not fully understand, and are blamed whether they do or do not follow algorithmic advice.
Consider two illustrative scenarios. In Scenario A, a nurse receives a high-risk AI-generated sepsis alert for a post-operative patient. The nurse’s clinical assessment reveals an alternative explanation, with the patient’s elevated temperature and heart rate being consistent with expected post-surgical inflammation rather than infection. The nurse documents the AI alert, records the clinical rationale for not initiating the sepsis protocol, and continues close monitoring. The patient recovers uneventfully. In Scenario B, a nurse receives a low-risk score from an AI-CDSS for a patient who appears to be clinically deteriorating, as evidenced by increasing restlessness, diaphoresis, and anxiety despite stable vital signs. The nurse overrides the AI assessment, escalates care, and the patient is subsequently diagnosed with an evolving myocardial infarction. In both cases, the nurse exercised appropriate professional judgment. However, under current accountability frameworks, had the outcomes been adverse in either scenario, the nurse could have faced liability — in Scenario A for overriding the AI, and in Scenario B for deviating from a system designed to detect risk. These scenarios illustrate why clear documentation practices and institutional policies that support clinical judgment alongside AI recommendations are essential.
The Black Box Problem and Informed Decision–Making
A fundamental challenge to professional accountability in AI-assisted care is algorithmic opacity. Many AI systems, particularly those based on deep learning, function as “black boxes” where even developers cannot fully explain how the system arrives at its recommendations (Chew et al., 2025; Rudin, 2019). This opacity creates significant barriers for nurses attempting to exercise professional judgment. How can a nurse critically evaluate an AI-CDSS recommendation when the reasoning behind that recommendation is inaccessible? How can a nurse be held accountable for following or overriding advice whose basis cannot be understood?
The black box problem directly implicates nursing ethics. The Code of Ethics for Nurses emphasises that systems and technologies are adjunct to, not replacements for, the nurse’s knowledge and skill, and that nurses are accountable for their practice even in instances of system or technology failure (American Nurses Association, 2015). Yet exercising this professional accountability requires the ability to understand, question, and when necessary override technological recommendations. When AI-CDSS provide recommendations, nurses are placed in the untenable position of being accountable for decisions they cannot fully evaluate.
To operationalise professional judgment in this context, nurses need structured approaches to AI-CDSS interaction. This includes training in identifying situations where AI outputs should be questioned (e.g., when recommendations conflict with clinical presentation, when patient populations differ from training data, or when system outputs appear inconsistent), as well as institutional protocols that explicitly empower nurses to override AI recommendations without fear of punitive consequences when their clinical assessment provides reasonable grounds for deviation.
Institutional Responsibility and Implementation Practices
Healthcare organisations bear significant responsibility for how AI systems are selected, implemented, and monitored in clinical practice. Institutions that deploy AI-CDSS tools without proper vetting, training, or safeguards may share liability when adverse outcomes occur (Pham, 2025; Price et al., 2019). Yet many hospitals lack clear guidelines or standards for introducing AI into nursing practice, making it difficult to ensure safe and appropriate use (Bi et al., 2025). This institutional gap shifts risk onto individual nurses who must navigate AI-CDSS recommendations without adequate organisational support, training, or clear policies governing when and how to incorporate AI into clinical decision-making.
The absence of standardised approaches to AI implementation creates variability in how nurses encounter and are expected to use these technologies. In some settings, AI-CDSS recommendations may be presented as advisory; in others, they may carry implicit or explicit expectations of compliance. Without clear institutional policies, nurses cannot know whether following AI-CDSS recommendations is expected, optional, or subject to independent professional judgment. This ambiguity exposes nurses to accountability risks regardless of how they respond to AI outputs.
Toward a Multi–Level Shared Accountability Framework
The challenges described above suggest the need for a multi-level shared accountability framework that distributes responsibility across four key stakeholder levels: (1) Individual clinician level: Nurses retain accountability for exercising professional judgment, including the responsibility to critically evaluate AI-CDSS outputs, document clinical reasoning, and override recommendations when clinical assessment warrants deviation. (2) Institutional level: Healthcare organisations bear accountability for selecting validated AI systems, providing adequate training, establishing clear policies on the advisory status of AI recommendations, maintaining incident reporting mechanisms, and conducting ongoing performance monitoring. (3) Developer level: AI developers and vendors bear accountability for algorithmic transparency, bias testing, post-deployment surveillance, and timely disclosure of known system limitations. (4) Regulatory level: Professional bodies and legal authorities bear accountability for updating standards of practice, establishing liability frameworks that recognise shared responsibility, and mandating transparency requirements for healthcare AI.
Multi–Level Shared Accountability Framework for AI–Assisted Nursing Practice
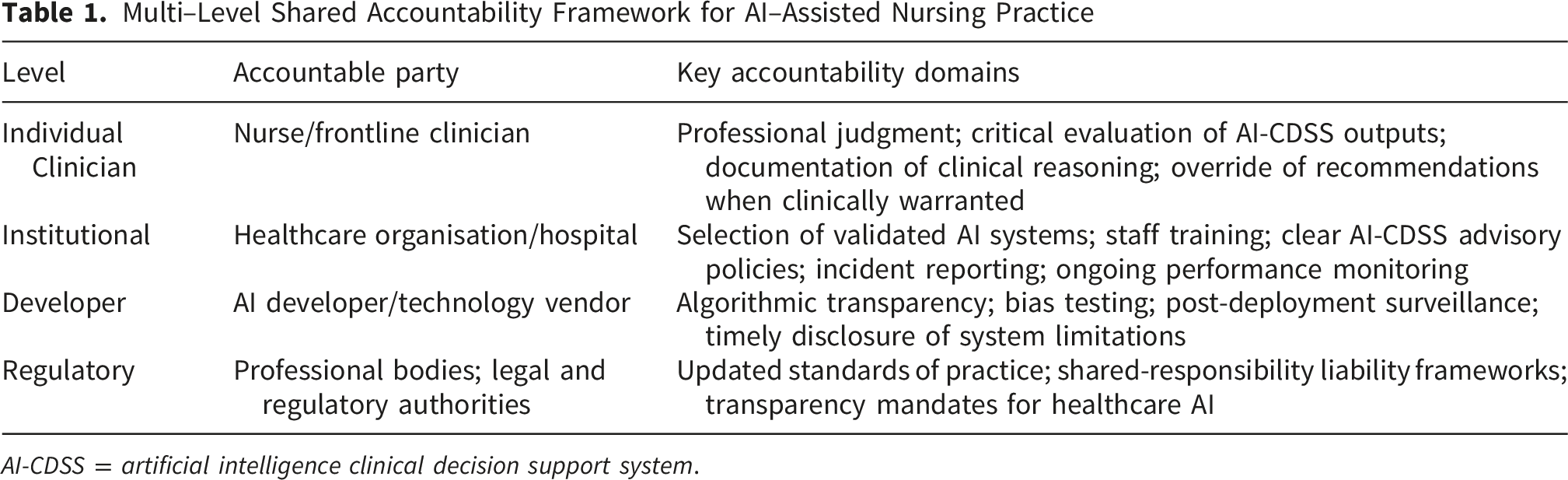
AI-CDSS = artificial intelligence clinical decision support system.
Current Insights and Recommendations
Clarify Professional Standards for AI–Assisted Practice
Professional nursing organisations must develop explicit guidance on accountability in AI-assisted practice. The American Nurses Association’s position statement on ethical AI use provides a foundation, emphasising that AI augments rather than replaces nursing judgment and that nurses remain accountable for their practice regardless of technological assistance (American Nurses Association, 2022, 2025). However, more specific guidance is needed addressing when nurses should follow versus override AI-CDSS recommendations, how to document decision-making processes involving AI, and what constitutes appropriate professional judgment when AI outputs conflict with clinical assessment. For instance, when a predictive early warning system generates a high-risk alert for patient deterioration, nurses should be guided to document: (a) the specific AI-generated alert and its risk score, (b) their independent clinical assessment at the time of the alert, (c) the rationale for following or overriding the AI-CDSS recommendations, and (d) the clinical actions taken and their outcomes. Such structured documentation creates an auditable trail that protects nurses by demonstrating the exercise of professional judgment while also generating institutional data for quality improvement. Regulatory bodies should integrate AI-related competencies into nursing standards, including content on evaluating AI-CDSS recommendations, recognising AI limitations, and maintaining independent clinical judgment (Brydges, 2025). Dornan (2025) proposed the APDDS framework arguing that “every nurse an AI nurse” requires embedding AI literacy, governance participation, and accountability mechanisms across all nursing roles, not merely informatics specialists.
Demand Algorithmic Transparency and Explainability
Nurses should advocate for AI systems that provide explainable outputs, enabling clinicians to understand how recommendations were derived and to identify potential limitations or errors. The World Health Organization’s guidance on AI in healthcare emphasises transparency and explainability as essential requirements for safe AI deployment (World Health Organization, 2024). When nurses can understand the basis for AI-CDSS recommendations, they are better positioned to exercise professional judgment about whether to incorporate those recommendations into care. Institutions should require that AI vendors provide interpretable outputs and clear documentation of system limitations, and nurses should be trained to critically evaluate AI explanations rather than accepting recommendations uncritically.
Establish Institutional Accountability Frameworks
Healthcare organisations must develop clear policies governing AI use in nursing practice, including explicit guidance on the status of AI-CDSS recommendations, documentation requirements for AI-assisted decisions, and procedures for reporting concerns about AI outputs. Institutions should establish AI governance committees with nursing representation to oversee implementation, monitor performance, and address safety concerns. When adverse events involve AI-CDSS, root cause analyses should examine not only individual clinician actions but also system design, implementation practices, and organisational factors that may have contributed to the outcome. This systems-level approach distributes accountability appropriately rather than placing full burden on individual nurses. Operationally, this could include establishing mandatory AI incident reporting systems analogous to existing medication error reporting, creating standardised AI decision-logging templates within electronic health records, and conducting regular audits of AI system performance disaggregated by clinical unit and patient population. Institutions should also designate AI safety officers or integrate AI oversight into existing clinical governance structures, ensuring that frontline nursing concerns about AI system performance are systematically captured and addressed.
Advocate for Legal Frameworks that Recognise Shared Responsibility
Current malpractice law, which assigns responsibility primarily to individual clinicians, is poorly suited to AI-assisted healthcare where multiple parties contribute to clinical decisions. Nurses should support advocacy efforts for legal frameworks that recognise the shared nature of AI-assisted decision-making. Although the European Commission’s proposed AI Liability Directive, which would have applied non-fault rules to high-risk AI failures, was withdrawn in 2025 following legislative review, the underlying principle of distributing responsibility more equitably across developers, deployers, and users remains a compelling model for healthcare (Pham, 2025). In aviation, fault is distributed across pilots, systems, and manufacturers when automation fails; healthcare could benefit from similar approaches that acknowledge the complex interplay between human judgment and algorithmic recommendations. Until legal frameworks evolve, nurses must document their clinical reasoning thoroughly, particularly when AI-CDSS recommendations are followed or overridden.
Conclusions and Importance to the Nursing Profession
The integration of AI into nursing practice creates accountability challenges that current ethical and legal frameworks are ill-equipped to address. Nurses find themselves in an increasingly difficult position: expected to incorporate AI-CDSS recommendations into practice while remaining accountable for their professional judgment, nursing actions, and documentation as members of the healthcare team, unable to fully understand the algorithmic processes generating those recommendations, and lacking clear guidance on how to navigate conflicts between AI outputs and professional judgment.
Resolving these challenges requires action at multiple levels. The multi-level shared accountability framework proposed in this commentary offers a structured approach for distributing responsibility across individual, institutional, developer, and regulatory levels. Professional organisations must provide clearer guidance on accountability in AI-assisted practice. Healthcare institutions must develop robust policies for AI implementation that support rather than expose nurses. Technology developers must create more transparent and explainable systems. Legal frameworks must evolve to recognise the shared nature of AI-assisted decision-making. Through these coordinated efforts, nursing can embrace the benefits of AI while protecting both patients and practitioners from the unintended consequences of poorly governed technological integration.
Ultimately, the nursing profession must assert that accountability in AI-assisted care is not solely an individual burden but a shared responsibility requiring appropriate systems, training, and institutional support. By advocating for frameworks that recognise this complexity, nurses can help ensure that the promise of AI-enhanced healthcare is realised without sacrificing the professional integrity and patient protection that define ethical nursing practice.