
Abstract
Introduction
This systematic review provides the first comprehensive synthesis of empirical studies on Artificial Intelligence (AI) integration in nursing education, offering actionable insights for nurse educators and clinical leaders. It highlights how AI transforms learning environments by enhancing personalization, feedback, and instructional efficiency.
Aims
To examine how AI is applied across nursing education settings and its impact on learning outcomes.
Methods
A systematic search of PubMed, CINAHL, IEEE Xplore, and Scopus identified peer-reviewed studies published from January 2010 to April 2025. Eligible studies focused on empirical AI applications in academic, clinical, or hybrid nursing education contexts. Studies were appraised using the Critical Appraisal Skills Programme (CASP) checklist, and findings were synthesized thematically.
Results
Twenty-eight studies met the inclusion criteria. AI-enhanced nursing education in four main areas: (a) personalized learning systems tailored content to individual needs, (b) simulation-based training improved decision-making in high-acuity scenarios,(c) automated assessment tools provided immediate, unbiased feedback, and (d) at the institutional level, AI supported curriculum management and predictive analytics. Common risks included technological inequities, faculty preparedness gaps, and ethical concerns around privacy and bias.
Conclusion
To support implementation, this study recommends: (a) integrating AI-powered simulation into emergency care training, (b) deploying adaptive platforms to support at-risk learners, and (c) using automated tools for real-time formative feedback. Diagnostic accuracy is proposed as a measurable outcome to assess impact. The next step for educators is to initiate multi-site pilot programs over 6–12 months, evaluating improvements in learning outcomes, trust, and system integration.
Keywords
Introduction
Nursing education serves as the backbone of healthcare systems, equipping future nurses with the clinical, cognitive, and ethical competencies necessary for safe and effective patient care (Ma et al., 2025; Zhou et al., 2024). Traditional pedagogical methods, rooted in classroom instruction, clinical practicums, and simulation labs, are increasingly challenged by the growing complexity of patient needs, workforce shortages, and the accelerating pace of healthcare innovation (Lifshits & Rosenberg, 2024). In response to these pressures, nursing education requires adaptive and scalable strategies that enhance learning efficiency, clinical preparedness, and instructional effectiveness (Seibert et al., 2021). AI has emerged as a transformative tool to address these evolving educational demands by bridging gaps in supervision, feedback, and personalization (Buchanan et al., 2021; Hwang et al., 2024).
AI technologies encompass a wide range of applications within nursing education. These include intelligent tutoring systems for personalized learning, machine learning platforms for performance prediction, virtual and augmented reality tools for clinical simulation, and automated systems for assessment and feedback (Abdelwahab et al., 2025; Harmon et al., 2021; Jallad et al., 2024). AI modalities such as natural language processing, generative models like ChatGPT, decision-support tools, and rule-based algorithms are increasingly being deployed across educational contexts to assist both learners and educators (De Gagne et al., 2024; Nesa et al., 2025; Shorey et al., 2019). The scope of this review includes populations such as pre-licensure nursing students, nurse educators, and continuing education participants across academic, clinical, and hybrid learning environments (Montejo et al., 2024; Topaz et al., 2025; Tran et al., 2024).
Although interest in AI integration has surged in healthcare, much of the existing research has concentrated on clinical applications such as diagnostics and robotic surgery, rather than the pedagogical use of AI in nursing education (Luo et al., 2024; O’Connor et al., 2023). Previous reviews often aggregate findings from broader medical education contexts, making it difficult to isolate outcomes that are specific to nursing and its unique professional competencies (Schneidereith & Thibault, 2023; Von Gerich et al., 2022). Additionally, there has been insufficient attention to how AI impacts essential educational dimensions like knowledge retention, diagnostic reasoning, learner equity, and faculty workload (Ahmed, 2024; Jung, 2023; Lebo & Brown, 2024). This gap in consolidated evidence limits the ability of educators, administrators, and policymakers to make informed decisions about AI integration that align with nursing pedagogy and ethics (Colborn et al., 2023; Rasouli et al., 2021).
The present review sought to fill this gap by providing a structured synthesis of current empirical evidence on the integration of AI in nursing education (Gunawan et al., 2024; Martinez-Ortigosa et al., 2023). It evaluates the educational utility of AI tools across various settings and modalities and organizes findings through three practical lenses: their impact on learning outcomes, their role in improving instructional workflow, and their ethical and safety considerations, including data privacy, algorithmic fairness, and equity in access (Castonguay et al., 2023; Foronda & Porter, 2024). By mapping emerging patterns and persistent challenges, the review aims to offer a balanced, evidence-informed perspective that guides the responsible adoption of AI in nursing curricula (Farsi, 2025). It emphasizes the importance of aligning technology with pedagogical goals, preparing faculty for implementation, and safeguarding humanistic values such as empathy, communication, and critical thinking. In doing so, this work contributes to a future-ready vision for nursing education in the digital age.
Methodology
Study Design
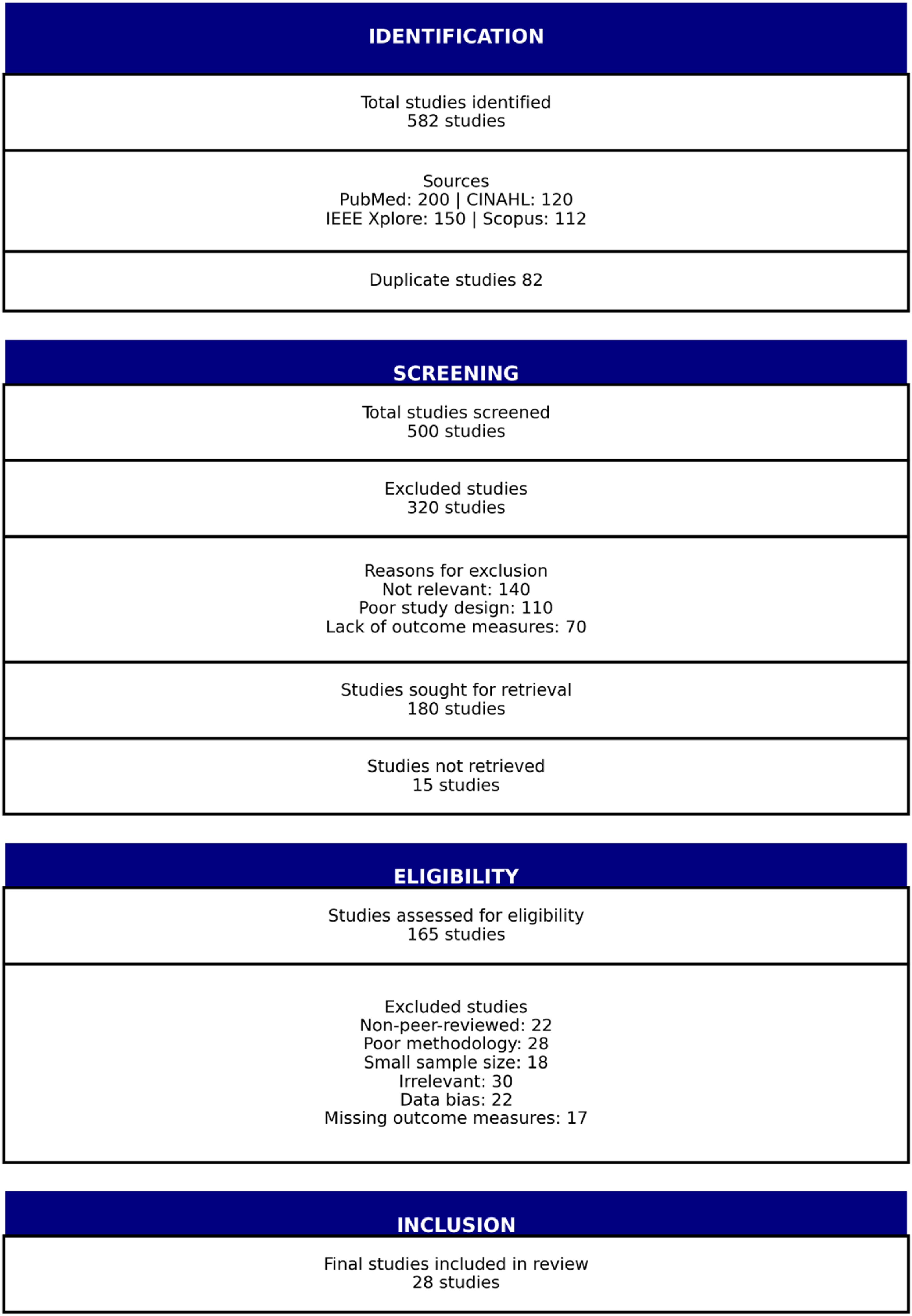
This systematic review was conducted to thoroughly examine how AI is being integrated into nursing education. The systematic review methodology was chosen because of its rigorous approach and its ability to compile and analyze data from a wide range of study designs and sources. This ensures a broad and in-depth understanding of existing literature. By providing a structured and unbiased evaluation of published research, this method is essential for assessing the various ways AI technologies are applied in nursing education and their overall impact. The review design is particularly justified given the diversity and novelty of AI applications in educational contexts, which require comprehensive aggregation and thematic analysis across qualitative, quantitative, and mixed-methods research. Outcomes of interest were defined a priori and included knowledge acquisition, skills development, learner engagement, diagnostic reasoning, faculty workload, instructional efficiency, and educational equity. This review explored both the scope and depth of AI integration in nursing education, identified gaps in existing research, and provided recommendations for future studies. To provide a clear representation of the study selection process, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram was used to illustrate the number of records identified, screened, excluded, and included in the final synthesis, as shown in Figure 1 (Page et al., 2021). This systematic selection process ensured that only the most relevant and credible studies contributed to the findings of this review.
PRISMA diagram.
Search Strategy
The literature search was conducted across multiple electronic databases to ensure a comprehensive collection of relevant studies. These databases included PubMed, CINAHL, IEEE Xplore, and Scopus, all well-regarded for their extensive coverage of medical and technological research (Table 1). To capture all pertinent studies, carefully selected search terms were used, incorporating combinations of keywords such as “artificial intelligence,” “nursing education,” “medical education,” “AI in healthcare education,” “AI tools in education,” “technology in education,” and “technological innovation in nursing.” To maintain consistency in language interpretation, the search was limited to studies published in English. Additionally, the publication timeframe was restricted from January 2010 through April 2025, allowing the review to focus on the most recent advancements in the field. Grey literature was excluded to ensure the inclusion of peer-reviewed studies only, thereby maintaining a higher level of methodological rigor and reliability in the synthesis.
Search Strategy.

Inclusion and Exclusion Criteria
The inclusion criteria were carefully designed to focus on original studies that explore the application of AI in educational curricula. This included empirical research offering insights into the effectiveness, challenges, and outcomes of AI implementation in educational settings. Eligible populations were nursing students, nursing educators, or both, in academic, clinical, or online learning contexts. Studies were included if they examined AI interventions such as intelligent tutoring systems, virtual simulations, adaptive learning platforms, or AI-driven assessment tools, with outcomes related to knowledge, skills, competencies, attitudes, or educational performance. Both quantitative and qualitative study designs were considered, provided they were peer-reviewed and met minimum quality standards based on CASP assessment. Interprofessional or medical education studies were included only if data specific to nursing could be clearly identified. To maintain a high standard of evidence, exclusion criteria were established to omit studies not directly related to educational improvement, as well as opinion pieces and editorials. This approach ensured that only data-driven, peer-reviewed research was considered for analysis.
Selection and Screening Process
A structured approach was employed to identify and include the most relevant studies. The initial phase involved screening titles and abstracts to evaluate their alignment with the research questions. Subsequently, a comprehensive full-text review was conducted to determine eligibility based on predefined inclusion and exclusion criteria. To enhance efficiency and organization, EndNote was utilized for reference management and to streamline the screening process. To ensure rigor and minimize bias, two reviewers independently screened all titles/abstracts and full texts against the eligibility criteria. Disagreements were resolved through discussion, and when consensus could not be reached, a third reviewer was consulted. Inter-rater agreement during the screening process was assessed using Cohen's κ statistic, which demonstrated substantial agreement (κ = 0.82).
Data Extraction
Data were systematically extracted from each selected study, emphasizing key elements such as authors, publication year, study objectives, sample size, methods, key findings, recommendations, and types of AI utilized (Table 2). This structured approach ensured a comprehensive and organized evaluation of the collected data. To synthesize the extracted information, findings were tabulated, and a thematic analysis was conducted to identify common themes, emerging trends, and notable outliers within the data.
Features of the Selected Studies.

Quality Assessment
In this systematic review, the quality of each included study was meticulously assessed using the CASP checklists to ensure the reliability and validity of the findings (Table 3) (Long et al., 2020). Each author played a significant role in evaluating key aspects of the research methodologies. The process began with an assessment of validity, examining whether the research questions were well-defined and if the study design is appropriately aligned with them. The selection of participants was analyzed for potential biases to maintain the integrity of the outcomes. Reliability was then assessed by evaluating the consistency and reproducibility of data collection methods, ensuring that findings could be replicated in future research.
Quality Assessment of Studies Using CASP Checklists.
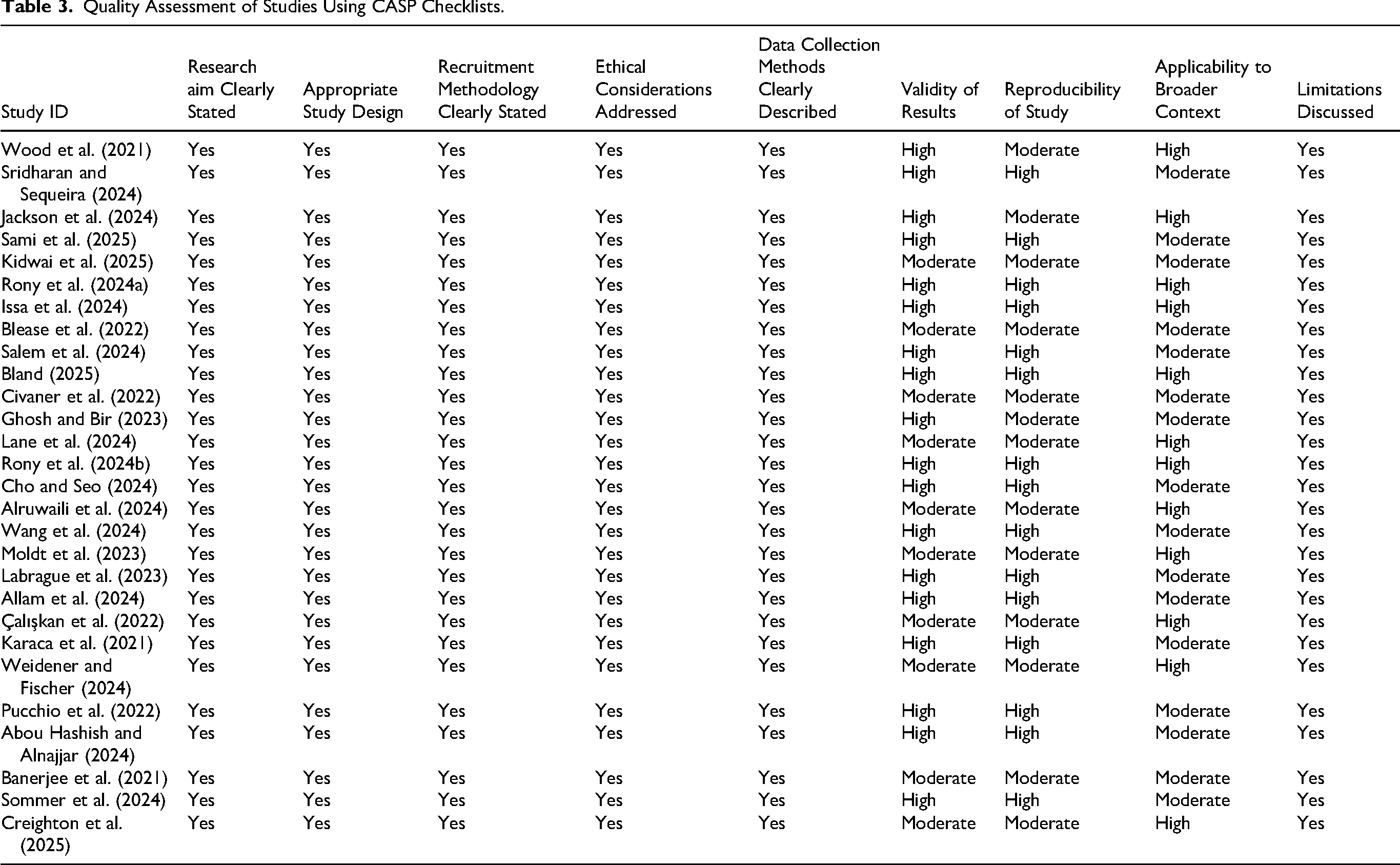
Additionally, the specificity of the results was scrutinized by analyzing the sensitivity and appropriateness of the measurement tools to confirm that the outcomes directly addressed the research questions. The significance of the findings was also considered, particularly their practical implications and contributions to nursing education. Finally, the applicability of the results was evaluated to determine whether they could be generalized to broader contexts and implemented in real-world educational settings. Overall, most of the included studies were scored as high quality, while others were assessed as moderate quality. This appraisal process enhanced transparency and reproducibility, providing a clear framework for evaluating study rigor. Throughout this process, the collaborative efforts of the authors ensured a systematic and unbiased evaluation, ultimately enhancing the validity and impact of the systematic review's conclusions.
Data Synthesis
The data synthesis approach employed a narrative synthesis, which is well-suited for systematic reviews that include diverse study designs and methodologies. This method enables detailed descriptions and discussions of findings in a narrative format, making it easier to interpret complex and heterogeneous data. Additionally, the synthesis accounted for variations and inconsistencies across studies, ensuring that the conclusions drawn were both robust and representative of the potential state of AI applications in nursing education. To guide the process, this review followed the framework proposed by Popay et al. (2006) for narrative synthesis. Studies were grouped thematically according to their primary focus areas, such as personalized learning, simulation-based training, automated assessment, clinical reasoning, administrative applications, and ethical considerations. Within each theme, findings were compared and contrasted to identify consistencies, divergences, and unique contributions. Meta-analysis was not feasible due to heterogeneity in outcome measures, AI modalities, and research methodologies across the included studies. Therefore, the narrative synthesis framework provided a flexible yet rigorous approach to organize and interpret results.
To ensure robustness, the researchers performed sensitivity analyses by considering study design, methodological quality (based on CASP assessments), and risk of bias. Findings from studies assessed as low quality were interpreted cautiously and compared against higher-quality evidence to evaluate stability of conclusions. Although quantitative meta-analysis was not possible, potential publication bias was considered qualitatively. This involved assessing the distribution of included studies across countries, publication outlets, and study types, and reflecting on whether overrepresentation of positive findings may have influenced conclusions.
Results
Overview of Study Selection
The study selection process for this systematic review followed a structured approach to ensure the inclusion of relevant and high-quality research. Initially, a total of 582 records were identified through comprehensive searches across multiple databases, including 200 from PubMed, 120 from CINAHL, 150 from IEEE Xplore, and 112 from Scopus. After removing 82 duplicate records, the remaining 500 studies were subjected to a title and abstract screening process. Based on predefined inclusion and exclusion criteria, 320 articles were excluded at this stage for reasons such as lack of relevance in 140 studies, poor study design in 110 studies, or lack of outcome measures in 70 studies. Following the title and abstract screening, 180 full-text articles were sought for retrieval. However, 15 studies could not be retrieved, leaving 165 studies for full-text assessment of eligibility. Studies were excluded from being non-peer-reviewed in 22 cases, having poor methodology in 28 cases, small sample sizes in 18 cases, irrelevance in 30 cases, data bias in 22 cases, or lack of clear outcome measures in 17 cases. After the full-text review, a total of 28 studies met the inclusion criteria and were included in the qualitative synthesis. The included studies comprised different research designs, with cross-sectional studies being the most common (18/28; 64.3%). Qualitative studies accounted for 4/28 (14.3%), mixed-methods studies also represented 4/28 (14.3%), while Delphi and quasi-experimental studies each contributed 1/28 (3.6%).
Characteristics of Included Studies
The included studies, conducted in the USA, India, Pakistan, the Netherlands, and Bahrain, explored the role of AI in nursing education using diverse methodologies such as cross-sectional surveys, semi-structured interviews, online questionnaires, proof-of-concept studies, and mixed-method approaches. Sample sizes varied, with some studies involving large cohorts of 702 and 325 students, while others focused on smaller groups, such as 15 students in qualitative interviews. A range of AI technologies was examined, including general-purpose large language models (LLMs) such as those developed by OpenAI (e.g., ChatGPT), Anthropic (Claude), Google (Gemini), and Meta, as well as machine learning (ML) applications. In cases where studies did not specify exact versions or platforms, these tools were treated collectively as general-purpose LLMs/ML classifiers. Some studies assessed AI literacy and perceptions without specifying particular AI tools, whereas others explored AI applications in structured learning objective generation, AI-assisted curriculum development, and automated medical training support.
Findings suggest that while AI holds significant promise in nursing education, its awareness and adoption remain inconsistent among students and faculty. While some research highlights high acceptance rates and AI's potential to enhance learning efficiency and decision-making, others report limited AI proficiency among educators and healthcare professionals. To bridge this gap, recommendations emphasize integrating AI into nursing curricula, developing AI-specific educational tools, incorporating ML training, and optimizing AI-driven learning approaches to improve education quality, clinical decision-making, and adaptive learning experiences. However, most included studies were concentrated in middle- and high-income countries, which may limit the generalizability of findings to resource-limited settings. Equity considerations are important, as technological infrastructure, faculty preparedness, and access to AI-driven tools vary widely across contexts, suggesting that benefits observed in well-resourced environments may not be directly transferable to low-resource educational systems.
Results: Integration of AI in Nursing Education
High-Acuity Settings: Simulation-Based Learning and Decision Support
AI-driven simulations in high-acuity environments replicate emergency conditions such as trauma resuscitation, cardiac arrests, or respiratory failure using virtual and augmented reality platforms (Issa et al., 2024; Salem et al., 2024). These immersive tools allow learners to engage in complex clinical situations with instant, AI-generated feedback tailored to their performance level (Bland, 2025). The real-time adaptation of difficulty ensures that learners remain engaged and challenged, while instructors use performance dashboards to assess competency and conduct targeted debriefings (Civaner et al., 2022). Blease et al. (2022) found that such platforms improve clinical judgment and emotional readiness. In one pre/post-test study, students exposed to AI simulations showed a statistically significant improvement in clinical confidence with a mean gain of 1.06 on a 5-point scale (Creighton et al., 2025). AI simulations in high-acuity training enhance emergency preparedness by providing risk-free, personalized, real-time learning experiences.
Ambulatory Settings: AI-Supported Clinical Reasoning
AI tools in ambulatory settings focus on enhancing diagnostic reasoning through longitudinal, case-based simulations. These platforms present evolving patient scenarios enriched by AI-generated diagnostic suggestions, which help students interpret lab results, assess symptoms, and compare intervention outcomes (Labrague et al., 2023; Çalışkan et al., 2022). Machine learning algorithms predict patient trajectories and simulate outpatient decision-making workflows, often embedded in electronic health records (Moldt et al., 2023). These tools promote anticipatory thinking by presenting learners with evolving clinical cases. Sridharan and Sequeira (2024) highlight that AI modules help bridge the gap in clinical supervision for students during ambulatory care rotations. AI-driven case simulations in outpatient contexts sharpen diagnostic skills and encourage predictive, patient-centered reasoning.
Academic Settings: Personalized Learning Platforms
In academic environments, AI is primarily used to customize learning paths. These adaptive systems track individual progress, analyze performance data, and deliver tailored content based on knowledge gaps (Wood et al., 2021; Sami et al., 2025). Features include dynamic quiz generation, personalized study recommendations, and just-in-time remediation (Ghosh & Bir, 2023). AI tutors replicate conversational engagement and simulate diagnostic pathways using virtual patient interactions (Kidwai et al., 2025; Rony et al., 2024a). Gamified elements such as achievement tracking and competitive leaderboards further enhance engagement (Jackson et al., 2024). These platforms also provide predictive analytics to identify students at risk and recommend support interventions (Allam et al., 2023; Sridharan & Sequeira, 2024). AI-powered personalization supports learner autonomy and improves outcomes through targeted, data-informed instructional delivery.
Assessment and Feedback: Automated Evaluation Systems
Automated assessment systems use AI to evaluate clinical reasoning, communication, and procedural knowledge. Tools employing natural language processing analyze student responses in reflections, quizzes, and simulated conversations (Cho & Seo, 2024; Lane et al., 2024). These systems reduce grading time and eliminate subjective bias, improving the consistency of evaluation across cohorts (Civaner et al., 2022). Feedback loops are central to these platforms. AI systems provide real-time performance reports during simulations, highlighting strengths and pinpointing reasoning errors (Rony et al., 2024b; Wang et al., 2024). These immediate responses reinforce learning and reduce the likelihood of repeating mistakes. Longitudinal tracking also allows educators to monitor learner growth and address knowledge gaps proactively (Alruwaili et al., 2024). Karaca et al. (2021) underscore the effectiveness of these systems in fostering reflective learning and academic self-regulation. AI-enabled assessments deliver rapid, consistent feedback that accelerates clinical reasoning and performance improvement.
Institutional Applications: Administrative and Curriculum Management
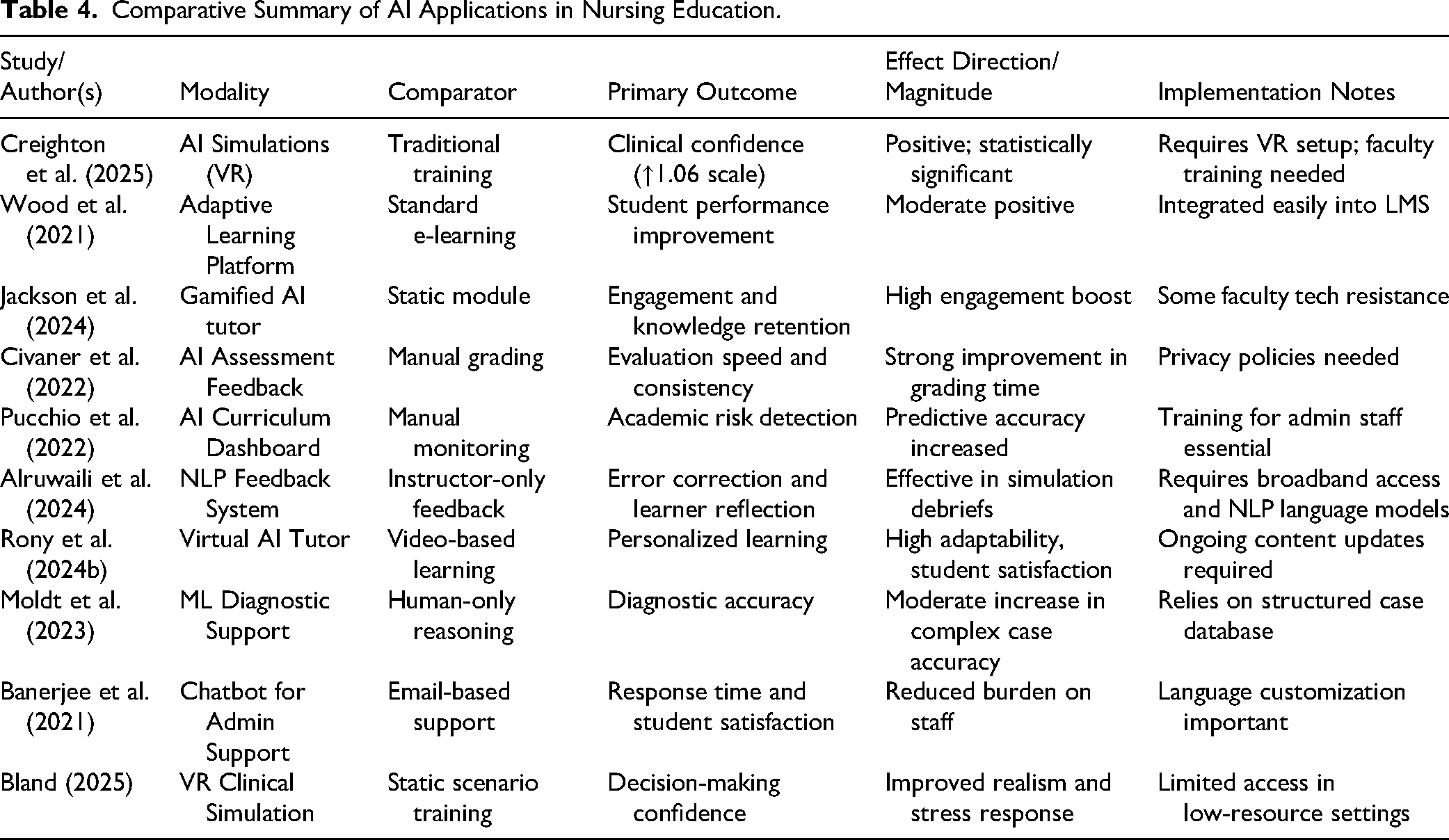
At the institutional level, AI systems streamline academic administration and curriculum design. Learning management systems enhanced with AI can track attendance, assignment submissions, and engagement metrics to identify students at risk (Pucchio et al., 2022; Sommer et al., 2024). Predictive models assist administrators in making data-driven decisions about scheduling, resource allocation, and curriculum development (Wang et al., 2024). AI-based chatbots handle common administrative inquiries, improving responsiveness and reducing staff workload (Abou Hashish & Alnajjar, 2024; Banerjee et al., 2021). These systems also enable competency-based education by allowing students to progress according to skill mastery rather than fixed timelines (Creighton et al., 2025; Rony et al., 2024b; see Table 4 for comparative details). Despite the promise, barriers remain. Implementation requires significant infrastructure investment and faculty training (Cho & Seo, 2024; Kidwai et al., 2025). Faculty engagement is crucial to ensure alignment between AI-generated insights and pedagogical goals (Jackson et al., 2024; Lane et al., 2024). AI integration into institutional systems supports efficient academic planning, student monitoring, and personalized support at scale.
Comparative Summary of AI Applications in Nursing Education.
Cross-Setting Considerations: Ethics and Implementation Challenges
While the integration of AI has advanced educational outcomes, ethical concerns remain. Data privacy, informed consent, and algorithmic transparency are major issues as AI systems handle sensitive student information (Civaner et al., 2022; Karaca et al., 2021). Jackson et al. (2024) and Blease et al. (2022) caution against over-reliance on AI, which may diminish the role of human mentorship and affect the development of empathy and interpersonal skills. Educators also expressed concern over feedback generated by AI systems that sometimes contradict human instructors or appear impersonal (Alruwaili et al., 2024; Weidener & Fischer, 2024). Implementation inequities are evident in under-resourced settings, where infrastructure gaps and poor connectivity restrict AI access (Abou Hashish & Alnajjar, 2024; Sommer et al., 2024). Faculty readiness remains a critical bottleneck. Many instructors lack the technical training needed to implement AI tools effectively, limiting their pedagogical potential (Bland, 2025; Moldt et al., 2023). Ethical AI adoption in nursing education requires faculty training, transparency, and equitable access to technological infrastructure.
Discussion
This systematic review demonstrates how AI applications can either augment or complicate nursing education depending on their alignment with educational contexts, workflows, and stakeholder readiness. In environments where AI systems were purposefully integrated to support existing pedagogical strategies (such as adaptive learning tools mirroring individualized instruction or simulation platforms reflecting real clinical encounters), the benefits were more pronounced (Marr & Tsang, 2025). These outcomes often stemmed from congruence between AI capabilities and instructional needs, fostering greater engagement, efficiency, and diagnostic acumen (Akca Sumengen et al., 2025; Huang et al., 2025). In contrast, implementation in contexts lacking institutional preparedness, faculty buy-in, or technological infrastructure tended to yield modest or uneven results (Alwadani et al., 2024; Habib et al., 2024; Simms, 2025).
One key driver of successful implementation was the integration of AI into student-centered workflows that promoted autonomy and personalization. When students could control the pace and depth of their learning through real-time feedback and interactive modules, AI became a scaffold for critical thinking rather than a prescriptive tool (Sridharan & Sequeira, 2024; Sami et al., 2025). Conversely, resistance emerged when AI tools were perceived as undermining human mentorship or oversimplifying complex clinical reasoning tasks. This highlighted a trade-off between automation and the cultivation of nuanced judgment (Bodur et al., 2024; Fazlollahi et al., 2022). Educators also expressed concerns about the erosion of interpersonal skills and ethical reasoning, which remain core competencies in nursing practice and are difficult to capture through algorithmic assessments (Harishbhai Tilala et al., 2024; Russell et al., 2023).
Trust and accountability emerged as central boundary conditions in the integration of AI. Faculty skepticism often stemmed from limited AI literacy and concerns about data privacy, fairness, and opaque algorithmic processes (Alghamdi & Alashban, 2024; Alwadani et al., 2024). These concerns were exacerbated in systems where AI decisions were not easily auditable or lacked transparent justifications (Alier et al., 2021; De Gagne et al., 2024). Similarly, students demonstrated reluctance when feedback from AI lacked contextual nuance or appeared inconsistent with human evaluators. To mitigate these tensions, studies emphasized the need for a “human-in-the-loop” model. This approach embeds human oversight into automated systems to balance efficiency with ethical safeguards (Jonathan, 2025; Lane et al., 2024; Pucchio et al., 2022). It also fosters greater trust in AI-enhanced learning environments, particularly when systems are designed to augment (rather than supplant) the educator's role.
Translating these insights into actionable principles, the review suggests several implementation strategies. Aligning AI adoption with pedagogical goals is essential, ensuring that tools complement rather than disrupt faculty workflows (Grunhut et al., 2022; Jha et al., 2022). Faculty training should extend beyond technical know-how to include ethical reasoning, data governance, and scenario-based decision-making to maintain accountability (Marr & Tsang, 2025; Mehta et al., 2021). Tool selection should also be guided by equity considerations, making sure that AI does not widen digital divides but instead enhances inclusivity through accessible formats and mobile-friendly designs (Kansal et al., 2022; Lee et al., 2021; Majumder & Haque, 2025). In addition, iterative evaluation should be embedded in implementation plans, with metrics tied to learning outcomes, user satisfaction, and system transparency (Harrison, 2024).
In resource-constrained settings, where infrastructure limitations and workforce shortages pose formidable barriers, the findings offer critical guidance. Phased deployment of AI tools (starting with low-cost, open-source platforms or AI-integrated mobile learning apps) can enable gradual capacity-building without overburdening institutions (Mousavi Baigi et al., 2023). Faculty development initiatives, including regional train-the-trainer models, can multiply impact while minimizing cost (Castonguay et al., 2023). Cloud-based platforms and regional resource-sharing networks could facilitate collaborative curriculum design and AI deployment, especially for simulation and assessment tools (Choi et al., 2025; Farghaly Abdelaliem et al., 2022). These strategies, if guided by community needs and aligned with curricular goals, can help bridge the digital divide and ensure that AI contributes meaningfully to equitable nursing education across diverse global contexts.
Implications for Education
To support structured AI integration in nursing curricula, this study proposes a four-tier competency ladder: Awareness, User, Supervisor, and Designer. At the Awareness level, learners should recognize AI's role in healthcare and education, with outcomes such as identifying AI tools and articulating ethical concerns. Assessment may include a multiple-choice quiz or reflective paragraph. Suggested activity: completing a short module on AI in nursing. The User level focuses on operational use of AI tools in simulations or personalized learning platforms. Outcomes include demonstrating AI-assisted decision-making. Assessment methods include Objective structured clinical examination (OSCE) stations or skill-based rubrics. A suggested activity is engaging in a chatbot-based clinical case. At the Supervisor level, learners critically appraise AI-generated outputs and guide ethical applications. Outcomes include evaluating data bias and explaining human-AI collaboration. Assessment may involve annotated case reviews or portfolio artifacts. A suitable activity is mentoring junior peers in AI-supported labs. At the Designer level, learners co-develop AI-enhanced teaching tools or simulations. Outcomes include creating a use-case or prototype for AI integration. Capstone projects or pilot-tested instructional materials serve as assessments.
To scale this model, institutions should implement a faculty development program of 12–15 h over 4 weeks, covering AI fundamentals, hands-on practice, ethics, and curriculum mapping. Resources needed include interactive demos, sample rubrics, and AI toolkits. Uptake can be evaluated via pre/post-tests, peer-reviewed teaching plans, and self-reported implementation rates. This framework enables rapid yet sustainable AI integration by aligning competencies with teaching strategies, assessments, and institutional support systems.
Implications for Practice
Practice Implementation and Staged Rollout
A staged rollout model is recommended for the safe and effective integration of AI tools into clinical education. This includes three phases: (1) Discovery: identify specific clinical use-cases; responsibility lies with unit heads or nurse educators; success is measured by relevance to workflow and stakeholder readiness. (2) Pilot: implement small-scale trials with run-chart metrics such as error detection rates, time-to-completion of tasks, and reliability of escalation; faculty leads and clinical supervisors oversee this phase. (3) Scale: institutional governance ensures alignment with accreditation standards, while audit trails track AI tool performance, outcomes, and human oversight. A pre-implementation checklist should include workflow mapping, identification of high-risk failure points, ethical risk scenarios, and a defined fallback plan if the AI tool underperforms or fails. Documenting oversight mechanisms is critical to maintain safety and accountability in AI-supported clinical decisions. This model allows nursing institutions to evaluate efficacy, minimize risk, and foster trust while integrating AI into real-world practice.
Ethics and Governance
To support ethical and accountable AI integration in nursing education, this review proposes a practical governance bundle organized around four key principles: transparency, fairness, safety, and responsibility. Transparency involves documenting the model type, version, and rationale for use to promote clarity in AI selection. Fairness includes conducting pre-defined checks that reflect the needs of the local learner population, such as evaluating bias or performance across demographic groups. Safety requires identifying specific trigger conditions for AI activation and establishing escalation pathways for when AI recommendations are uncertain or potentially harmful. Responsibility entails assigning named individuals or teams to oversee monitoring, system updates, and ethical compliance.
For institutional auditability and continuous improvement, this study proposes recommends storing AI prompts, configuration settings, version history, and evaluation rubrics in a shared appendix or repository accessible to faculty and governance committees. This centralized documentation will support periodic review, ensure transparency, and strengthen trust in AI tools used for education. Implementing this governance approach will enable nursing institutions to integrate AI responsibly while safeguarding student learning and ethical standards.
Practice-Oriented Recommendations and Future Directions
Based on the review findings, the researchers propose three testable recommendations to guide future research and practice. First, evaluate the impact of AI-based simulation tools on clinical reasoning using a randomized design, with competency scores as the primary endpoint assessed over a 6-month follow-up. Second, assess AI-driven personalized learning platforms via a quasi-experimental design, focusing on knowledge retention and skill application at 3 months. Third, examine ethical AI integration by implementing a faculty development intervention, measuring changes in AI literacy and ethical confidence over a 12-week period. To enhance cross-study comparability, this review advocates for a minimal common outcome set including measures such as learner engagement, diagnostic accuracy, faculty workload, and patient safety proxies. Implementation reporting should include training time, required staffing, and downtime protocols. Finally, this study urges replication of interventions across high- and low-resource institutions to assess scalability, feasibility, and equity of AI adoption in nursing education (Table 5).
Prioritized Recommendations for Future Practice and Research.

Strengths and Limitations
This review has several limitations. Despite these limitations, a key strength of this review lies in its comprehensive narrative synthesis across diverse educational settings and AI modalities, supported by a rigorous quality appraisal framework. First, there was notable heterogeneity across educational settings, AI modalities, and outcome measures, which limited comparability and prevented meta-analysis. Some outcome defects such as equity, long-term skill retention, and patient-level effects, were insufficiently reported. The review focused exclusively on English-language, peer-reviewed publications, introducing possible selection and publication bias. Additionally, most studies were from high-income countries, limiting generalizability to low-resource settings. Rapid developments in AI models, especially LLMs, may also affect the future applicability of current findings. Although a rigorous quality appraisal was conducted, sparse data in some areas reduced the ability to assess effect durability. To address these concerns, sensitivity checks were applied based on study quality and design, and this study recommends future reviews include grey literature and non-English studies to broaden perspectives. These limitations may tilt interpretation toward optimistic findings and underscore the need for more robust, longitudinal, and inclusive research.
Conclusion
AI is currently most actionable in nursing education through adaptive learning systems, simulation-based training, and automated assessments that support personalized instruction and diagnostic reasoning. For safe and effective integration, governance mechanisms must ensure data privacy, transparency, role-based accountability, and ethical oversight. The first measurable improvement should focus on enhancing diagnostic accuracy among students, as it directly impacts patient care and clinical readiness. A critical next step is to conduct a multi-institutional, longitudinal study that evaluates the effectiveness of AI-enhanced clinical simulations compared to traditional methods. This evaluation should assess performance outcomes, user trust, and implementation feasibility across varied resource settings. Such evidence could drive meaningful policy changes, inform curriculum design, and establish standards for scalable AI adoption in nursing education. By aligning innovation with pedagogical and ethical priorities, stakeholders can responsibly harness AI to improve learning outcomes while preserving the human values at the heart of nursing practice.
Footnotes
Acknowledgements
The authors are deeply grateful to the Miyan Research Institute, International University of Business Agriculture and Technology, Dhaka, Bangladesh. Additionally, this research was supported by the Deanship of Scientific Research, King Saud University, Riyadh, Saudi Arabia.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.