
Abstract
Introductions
Timely initiation of antenatal care (ANC), defined as attending the first visit within the first 12 weeks of gestation, is essential for optimizing maternal and neonatal health. Despite its benefits, delayed ANC initiation remains a significant challenge in low-resource settings, including Ethiopia, with limited data on its prevalence and determinants in specific regions.
Objective
To assess the prevalence and determinants of timely initiation of antenatal care among pregnant women attending public health facilities in, Ethiopia, in 2025.
Methods
A facility-based cross-sectional study was conducted from November 1, 2024 to February 1, 2025, across selected public health institutions. A total of 857 pregnant women mixed residence (both urban and rural) were recruited using systematic random sampling. Data were collected via a structured, interviewer-administered questionnaire based on validated tools and WHO recommendations. Kobo Toolbox supported real-time electronic data collection. Data analysis was performed using SPSS version 27. Bivariable and multivariable logistic regression analyses identified factors associated with timely ANC initiation. Adjusted odds ratios (AORs) with 95% confidence intervals (CIs) were calculated; significance was set at p < 0.05.
Results
Only 29.4% (95% CI: 26.4%–32.4%) of women-initiated ANC timely. Positive predictors included preconception care utilization (AOR: 2.1; 95% CI: 1.21–3.83), paternal involvement (AOR: 3.3; 95% CI: 2.03–5.28), good knowledge of ANC (AOR: 3.3; 95% CI: 2.29–4.77), and use of a self-pregnancy test (AOR: 3.2; 95% CI: 1.68–6.12). Conversely, being internally displaced (AOR: 0.22; 95% CI: 0.103–0.47), using hormonal contraception prior to pregnancy (AOR: 0.29; 95% CI: 0.12–0.78), and having a short inter-pregnancy interval (AOR: 0.58; 95% CI: 0.38–0.88) were significantly associated with delayed ANC initiation.
Conclusion
Timely ANC initiation remains suboptimal. Interventions targeting awareness, preconception care, and support for displaced populations are critical to improving timely ANC uptake and maternal health outcomes.
Keywords
Introduction
Maternal and perinatal mortality are key global indicators for monitoring maternal health, assessing the quality of reproductive healthcare, and evaluating progress toward the Sustainable Development Goals (De Silva et al., 2021). SDG 3.1 specifically aims to reduce the global maternal mortality ratio (MMR) to below 70 per 100,000 live births by 2030, ensuring no country exceeds 140 per 100,000 live births (Hák et al., 2016; UN, 2016). Antenatal care (ANC) is a primary strategy to achieve these targets, as it prevents, detects, and manages pregnancy-related complications (Organization, 2016). ANC involves care provided by skilled health professionals through planned, evidence-based interventions, including health promotion, disease prevention, screening, diagnosis, and management of pregnancy-related conditions (Tunçalp et al., 2017).
The traditional ANC model, established in the early 1900s, relied on frequent visits and early risk classification but proved ineffective in addressing unpredictable pregnancy complications (Peahl & Howell, 2021). To address these limitations, the WHO introduced Focused Antenatal Care (FANC) in 2002, recommending a minimum of four goal-oriented contacts, with the first before 16 weeks of gestation (Lori et al., 2016; Ngxongo, 2019; Oshinyemi et al., 2018; Villar & Bergsjo, 2016). Widely adopted worldwide, including in Ethiopia, FANC improved maternal and perinatal outcomes and supported progress toward the Millennium Development Goals (Assefa et al., 2017; Ayalew & Nigatu, 2018; Birungi, 2006; Lori et al., 2016; Mchenga et al., 2019; Steele et al., 2022).
Although FANC improved maternal health, it had limitations, including inadequate visit frequency to detect late-pregnancy complications, missed opportunities for counseling, and limited impact on perinatal mortality (Mchenga et al., 2019; Tunçalp et al., 2015; WHO, 2016). To address these gaps, the WHO in 2016 introduced a new model recommending at least eight ANC contacts to improve quality, continuity of care, and pregnancy experience while reducing maternal and perinatal morbidity and mortality. The first contact, ideally within 12 weeks, ensures timely confirmation of pregnancy, early risk assessment, individualized counseling, initiation of folic acid, and early detection and management of maternal or fetal conditions (Bhide et al., 2016; WHO, 2016). Despite WHO recommendations to initiate ANC within the first trimester, only 44.3% of pregnant women in low- and middle-income countries begin ANC timely (Jiwani et al., 2020). Country-level estimates vary, with 70% in Nepal and 43% in Bangladesh initiating ANC before 16 weeks (Paudel et al., 2017; Sarker et al., 2021). The situation is more concerning in sub-Saharan Africa, including Ethiopia, where a systematic review reported that only 38% of women accessed ANC timely, and national data indicate a 46% timely initiation rate (Alem et al., 2022; Tesfaye et al., 2017). Timely ANC initiation is influenced by maternal and paternal demographics (age, education, income), distance to health facilities, media exposure, pregnancy intention, parity, male partner involvement, women’s autonomy, prior pregnancy complications, and knowledge about ANC (Alem et al., 2022; Jiwani et al., 2020; Paudel et al., 2017; Sarker et al., 2021; Tesfaye et al., 2017).
Most existing studies in Ethiopia define timely ANC initiation as starting within 16 weeks, based on the outdated FANC model, which does not align with the 2016 WHO recommendation of initiating the first contact within 12 weeks as part of the eight-contact model. Additionally, many studies have overlooked key behavioral and contextual factors, such as women’s knowledge of timely ANC, and the increasingly common use of home-based self-pregnancy tests that may influence early care-seeking. Evidence is also limited regarding populations living in underrepresented and vulnerable settings. The study area hosts diverse groups, including internally displaced people (IDPs), whose unique barriers to timely ANC initiation remain largely unexplored in the literature. By incorporating these novel determinants and applying the updated WHO framework, this study provides context-specific, policy-relevant evidence on the prevalence and determinants of timely ANC initiation among pregnant women attending public health facilities. These contributions address critical knowledge gaps and offer new insights to guide targeted interventions aimed at improving maternal and newborn health outcomes.
Review of Literatures
A 2022 UNICEF report indicated that only 58% of pregnant women in LMICs initiate ANC timely (UNICEF, 2024). Timely ANC initiation is particularly low in sub-Saharan Africa, with a meta-analysis reporting a 36% prevalence (Alem et al., 2022). Country-level studies show similar gaps: 41% in Ghana, influenced by maternal education, parity, and employment (Manyeh et al., 2020); 27–33% in Nigeria, associated with urban residence, media exposure, and household wealth (Fagbamigbe et al., 2021; Steele, 2018); and 29% in Uganda, linked to maternal autonomy and ANC knowledge (Steele, 2018). These findings suggest that while ANC coverage may be increasing, timely initiation remains a critical challenge across the region..
Ethiopia continues to face challenges in ensuring timely ANC initiation. The 2019 Ethiopian Mini Demographic and Health Survey reported that only 28% of pregnant women began ANC timely (Ephi, 2019). A systematic review and meta-analysis across multiple regions found a pooled prevalence of 41.8% (Tekelab et al., 2019). Regional studies support these findings: in Addis Ababa, timely ANC initiation was associated with maternal age, knowledge of ANC timing, and previous pregnancy experiences (Gelassa et al., 2023); in Oromia, women with planned pregnancies and higher education were more likely to initiate ANC timely (Fikrie et al., 2023).
Multiple factors have been identified as influencing timely ANC initiation. Socio-demographic determinants include maternal age, education, distance from health facilities, residence, marital status, exposure to mass media, maternal autonomy, occupation, paternal education, income, and family size (Abute Woiloro et al., 2025; Alem et al., 2022; Fagbamigbe et al., 2021; Gelassa et al., 2023). Obstetric and reproductive factors include parity, gravidity, pregnancy intention (planned vs. unplanned), previous pregnancy complications or outcomes, prior ANC experience, early recognition of pregnancy, paternal involvement, and knowledge of ANC (Gelassa et al., 2023; Geta & Yallew, 2017; Sarker et al., 2021; Tesfaye et al., 2017). Most previous studies defined timely ANC initiation using the FANC model and overlooked factors such as population status, reproductive health service use, and self-determination of pregnancy. This study therefore assesses the prevalence and determinants of timely ANC initiation among pregnant women in [study area], guided by the updated WHO eight-contact recommendation, by incorporating overlooked factors to fill existing knowledge gaps and provide evidence for targeted interventions.
Methods and Materials
Study Design, Period and Setting
An institution-based cross-sectional study was conducted from November 1, 2024, to February 1, 2025, in the antenatal care units of selected public health facilities in Debre Berhan City Administration, North Shewa Zone, Ethiopia. From the seven public health facilities in the area, two comprehensive specialized hospitals and two health centers were selected using a simple random (lottery) method. Debre Berhan is located approximately 120 kilometers northeast of Addis Ababa and serves as the administrative center of the North Shewa Zone. The city is situated at an elevation of about 2,840 meters above sea level, making it one of the highest towns of its size in Ethiopia. Historically, Debre Berhan holds significant importance, having served as one of the early capitals of Ethiopia and the former kingdom of Shewa. Currently, the city has a rapidly growing and diverse population, including an estimated 100,000 internally displaced persons (IDPs) residing in four established camps and within host communities, according to recent United Nations reports. This unique demographic composition creates complex and increased demand for maternal and reproductive health services. Maternal health services, including ANC, are provided in seven public health facilities in the city, comprising five health centers and two hospitals. Administratively, these facilities form the main public health service delivery points for maternal and child health care in the area. For this study, two comprehensive specialized hospitals and two health centers were selected from the available public health facilities and included as study sites.
Research Question
- What is the proportion of timely initiation of antenatal care among pregnant women attending public health facilities in Ethiopia, in 2025? - What socio-demographic, obstetric, and other factors determine timely initiation of antenatal care in this population?
Population
The source population for this study included all pregnant women receiving ANC at public health facilities. The study population comprised all pregnant women who attended ANC services at the selected public health facilities during the data collection period.
Eligibility Criteria
All pregnant women who attended ANC services at the selected public health facilities during the data collection period were included in the study. However, pregnant women were excluded those who were critically ill (such as being unconscious due to eclampsia or experiencing severe bleeding), unable to communicate (e.g., could not hear or speak), and their medical records were incomplete with no available caregiver or attendant who could reliably provide the necessary information. This exclusion criterion was applied to ensure the validity and completeness of the data collected.
Sample Size Determination and Sampling Techniques
The sample size for this study was calculated using both the primary and secondary objectives to ensure statistical robustness. For the primary objective assessing the prevalence of timely initiation of ANC the single population proportion formula was employed. The assumptions included a 95% confidence level (Z = 1.96), a 5% margin of error (d = 0.05), and an estimated prevalence (p) of timely ANC initiation of 46%, which was derived from a recent systematic review conducted in Ethiopia (Tesfaye et al., 2017). Applying these parameters yielded a final calculated sample size of 382 participants.

To address the secondary objective identifying factors associated with timely initiation of ANC a double population proportion formula was used, considering exposure to media as a key predictor variable. This calculation was performed using Epi Info version 7.2.6.0, assuming a power of 80%, 95% confidence interval, a 1:1 ratio of exposed to non-exposed, a proportion of timely ANC initiation among women exposed to media of 26.04%, and among those unexposed of 17.17%, as reported in a study from southern Ethiopia (Geta & Yallew, 2017). Resulted in a larger sample size of 790 participants. To account for potential non-response, a 10% adjustment was made, leading to a final required sample size of 869 participants. Since the sample size required for the secondary objective was larger and sufficiently addresses both objectives, the final sample size used in this study was 869 (Figure 1).
From the seven public health facilities in the city, two comprehensive specialized hospitals Debre Berhan Comprehensive Specialized Hospital (DBCSH) and Hakim Gizaw Teaching Hospital (HGTH) and two health centers Debre Berhan Health Center (HC1) and Ayer Tena Health Center (HC5) were selected using a simple random sampling technique (lottery method). To ensure representativeness across study sites, the final sample size of 869 participants was proportionally allocated based on the three-month ANC client load of each selected facility. Accordingly, HGTH served 780 ANC clients, DBCSH 650, DBHC 1,068, and ATHC 897 clients during the three-month period, giving a total of 3,395 ANC clients across the selected facilities. Based on proportional allocation, 200 participants were assigned to HGTH, 166 to DBCSH, 274 to DBHC, and 229 to ATHC. Within each facility, individual participants were selected using a systematic random sampling technique. The sampling interval (k) was calculated by dividing the total number of ANC clients by the allocated sample size for each facility, resulting in an approximate k-value of 4 across all sites. A random starting point between 1 and 4 was selected, after which every 4th eligible ANC attendee was included in the study until the required sample size for each facility was achieved (Figure 1). Schematic representation of the sampling procedure for the study on timely initiation of ANC and its determinants in public health facilities of Ethiopia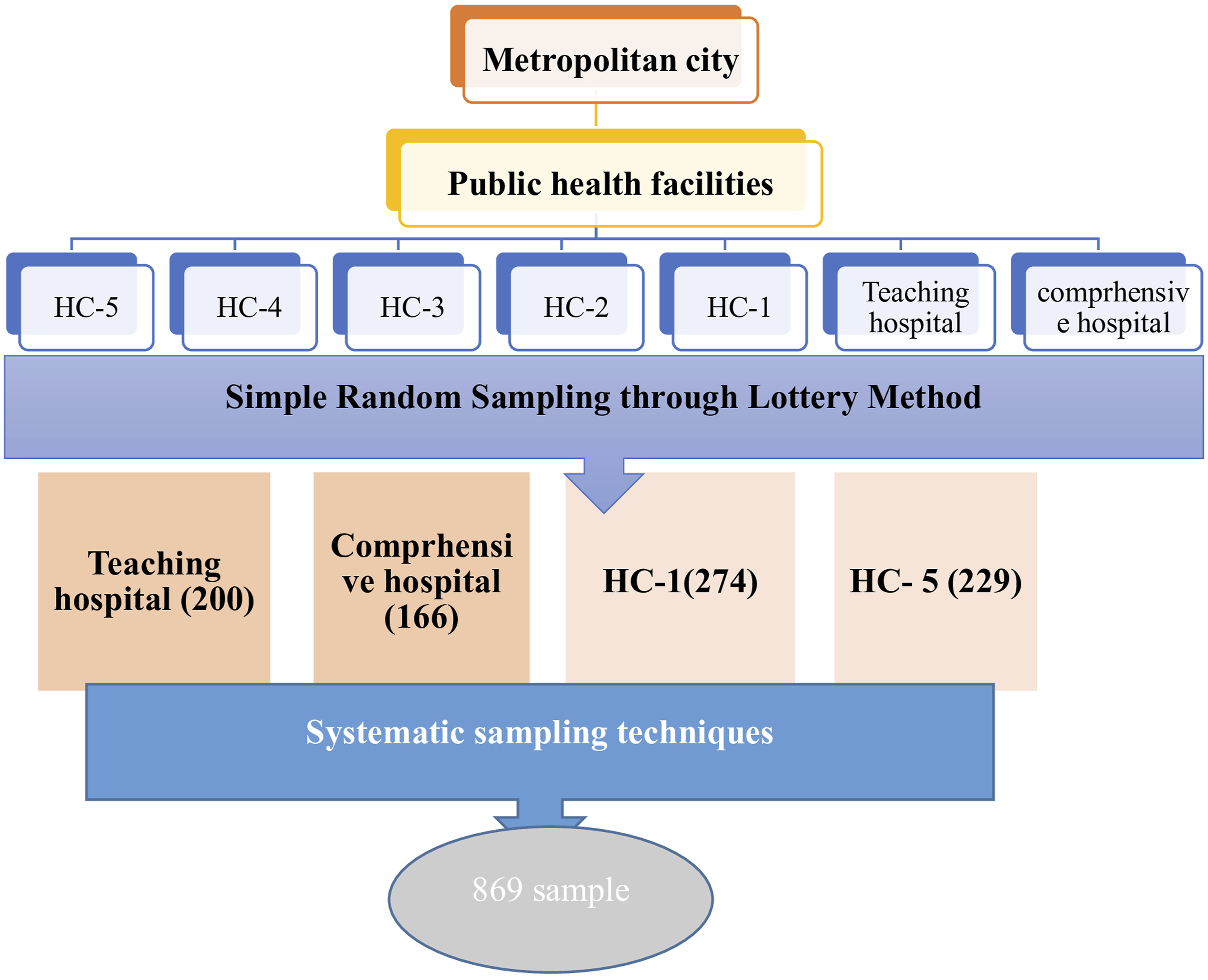
Study Variables
The dependent variable: Timely initiation of antenatal care.
Operational Definition/Measurement
Antenatal care: Is a maternal health service delivered by a team of healthcare professionals to pregnant women with the aim of promoting and preserving their wellbeing throughout pregnancy, childbirth, and the postpartum period, while also ensuring the birth and upbringing of a healthy child (Organization, 2024).
Timely initiation: Refers to a pregnant woman’s first contact with a skilled health provider within the first trimester of pregnancy (i.e., within the first 12 weeks of gestation) (WHO, 2016).
Gestational age (GA): Is defined as the age of the pregnancy in completed weeks. GA was primarily determined based on a reliable last normal menstrual period (LNMP). When both LNMP and early ultrasound were available, and there was no significant discrepancy between them, GA from LNMP was used. In cases where LNMP was unknown or unreliable, GA determined by early ultrasound was applied (ACOG, 2017).
A home-based pregnancy test: Is a self-administered diagnostic tool used by women to detect pregnancy at home by measuring the presence of human chorionic gonadotropin (hCG) hormone in urine (Organization, 2022).
Menstrual cycle irregularity: Refers to variations in the frequency, duration, or flow of menstrual periods that deviate from the normal menstrual pattern (Bennett & Brown, 2018).
Parental involvement in ANC: Refers to the active participation and support provided by the male partner (or parent) during a woman’s pregnancy and ANC visits (WHO, 2015).
Knowledgeable on ANC: Is measured using 20 questions, with scores ranging from 0 (all “No”) to 20 (all “Yes”). Participants who scored above the mean score of (14) were classified as knowledgeable, while those scoring at or below the mean were classified as not knowledgeable. (Kebede et al., 2022; Manukonda & Shanmugam, 2022).
Inter-pregnancy interval: Is the time between a live birth and the conception of the next pregnancy (Bartz, 2021; Organization, 2007).
Short inter-pregnancy interval: Is defined as less than two year between a live birth and the conception of the next pregnancy (Bartz, 2021; Organization, 2007).
Optimal inter-pregnancy interval: Is the time between a live birth and the conception of the next pregnancy, ranging from two to five years (1.5 to just under 5 years) (Bartz, 2021; Organization, 2007).
Preconception care: The provision of biomedical, behavioral and social health interventions to women and couples before conception occurs (WHO, 2013).
Utilization of preconception care: Is whether a woman received any one or more of the recommended preconception care interventions (such as counseling, screening, immunizations, or management of pre-existing conditions) before becoming pregnant (Atrash & Jack, 2020; Dean et al., 2014).
Paternal involvement: Is defined as joint participation in ANC services, including attending ANC visits with the partner, receiving information from healthcare providers, making shared decisions, and providing financial and physical support during pregnancy (Atiibugri, 2017). It was measured using a composite index of six equally weighted dichotomous items (Yes = 1, No = 0). The total score ranged from 0 to 6. Based on the cumulative score, male involvement was categorized as: Low involvement (categorized as “No”): score of ≤ 2 and High involvement (categorized as “Yes”): score of ≥ 3 (Muhabaw et al., 2024).
Data Collection Tool and Procedure
Data were collected using an interviewer-administered structured questionnaire deployed through Kobo Toolbox, enabling real-time entry and quality control. The tool, adapted from validated instruments and aligned with WHO ANC recommendations, covered sociodemographic, reproductive, and obstetric characteristics, service utilization, and knowledge of timely ANC initiation (Gessesse et al., 2024; Organization, 2016). To minimize recall bias, key clinical variables (e.g., gestational age at first ANC contact) were verified through medical records, including LNMP documentation and early ultrasound reports. Four trained midwives conducted face-to-face interviews, supervised by two master’s-level clinical midwives independent of the study sites. Supervisors ensured protocol adherence, data completeness, and resolution of inconsistencies, thereby enhancing validity and reliability.
Data Quality Assurance
Data quality was ensured through a multi-step strategy. A pretest on 5% of the sample at a non-study site assessed clarity and relevance of the tool, with feedback used to refine wording and structure. Data collectors and supervisors received a full day of training on study objectives, procedures, ethics, and Kobo Toolbox use, with emphasis on minimizing interviewer bias. During data collection, the principal investigator and two independent supervisors provided daily oversight through field visits, protocol monitoring, and real-time data checks. All entries were reviewed daily for completeness, consistency, and logical accuracy; discrepancies were promptly resolved through verification with records and data collectors.
Data Processing and Analysis
After thorough verification for accuracy and completeness, the collected data were imported into SPSS version 27 for detailed analysis. Initial data cleaning procedures, including cross-tabulation and descriptive statistics, were performed to ensure data quality by identifying and addressing missing values, inconsistencies, and potential outliers. Bivariable logistic regression analysis was conducted to explore potential factors associated with the timely initiation of ANC. Variables with a p-value of less than 0.25 in the bivariable analysis were subsequently included in a multivariable logistic regression model to control for confounding factors and to determine independent predictors of timely ANC initiation. Statistical significance was declared at a p-value of less than 0.05. The final findings were systematically presented using tables, charts, and descriptive text to provide a clear and comprehensive interpretation of the results.
Result
Socio Demographic Characteristic of the Sample Population
Socio-Demographic Characteristics of Study Participant at Public Health Facilities, 2025 (n = 857)

Obstetrics and Reproductive Related Characteristics of the Sample Population
Obstetrics and Reproductive Related History of Study Participant at Public Health Facilities, 2025 (n = 857)

Results of Research Question 1: Timely Initiation of Antenatal Care
Only 29.4% (95% CI: 26.4%–32.4%) of the 857 pregnant women attending ANC follow-up at public health facilities initiated their first visit timely (≤12 weeks gestation). Among the remainder, 19.3% began ANC between 12 and 16 weeks, while the majority (51.3%) initiated ANC after 16 weeks of gestation (Figure 2). Distribution of antenatal care initiation timing among pregnant women attending public health facilities (2025) (n = 857)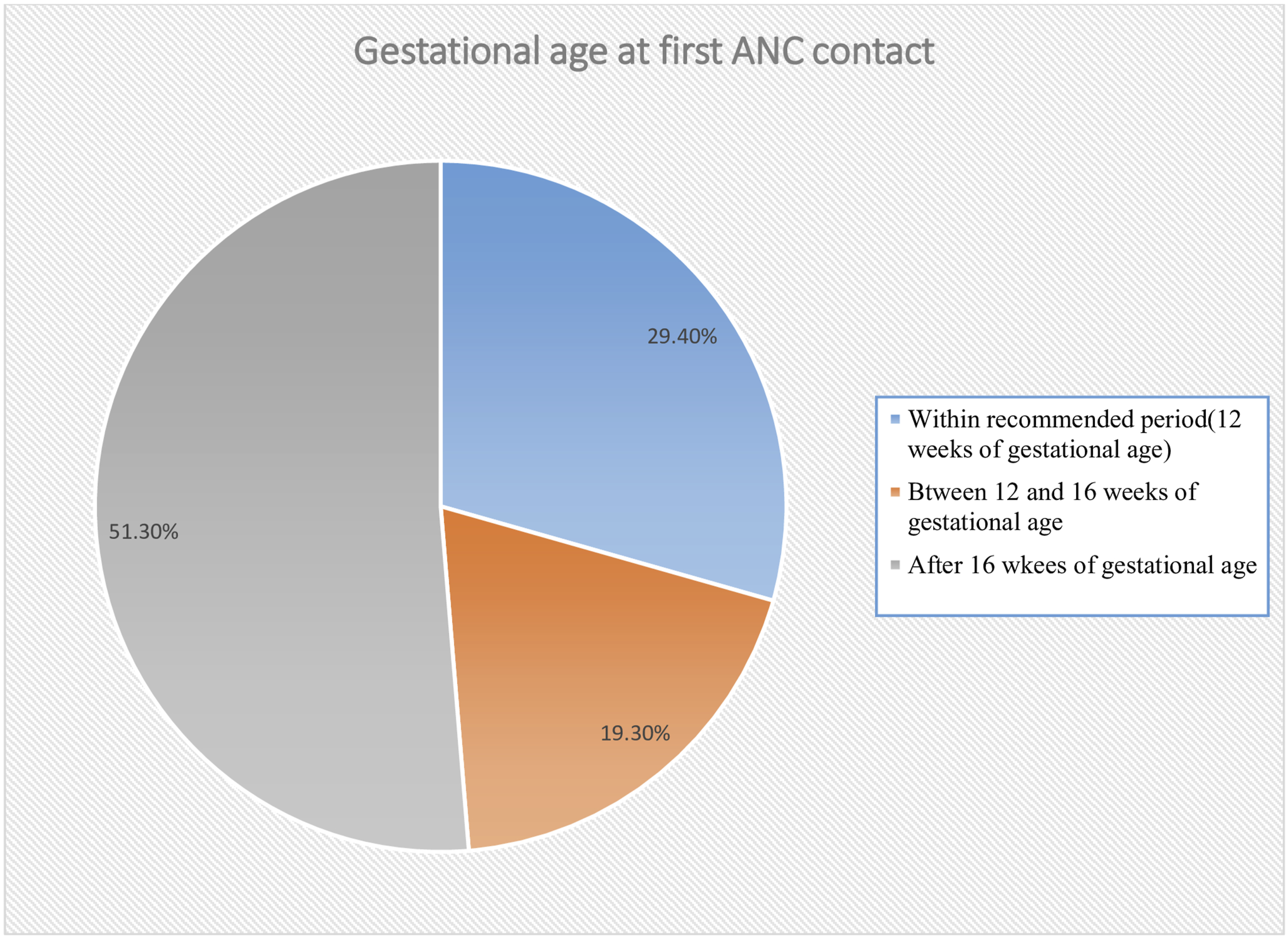
Results of Research Question 2: Factor Associated With Timely Initiation of Antenatal Care
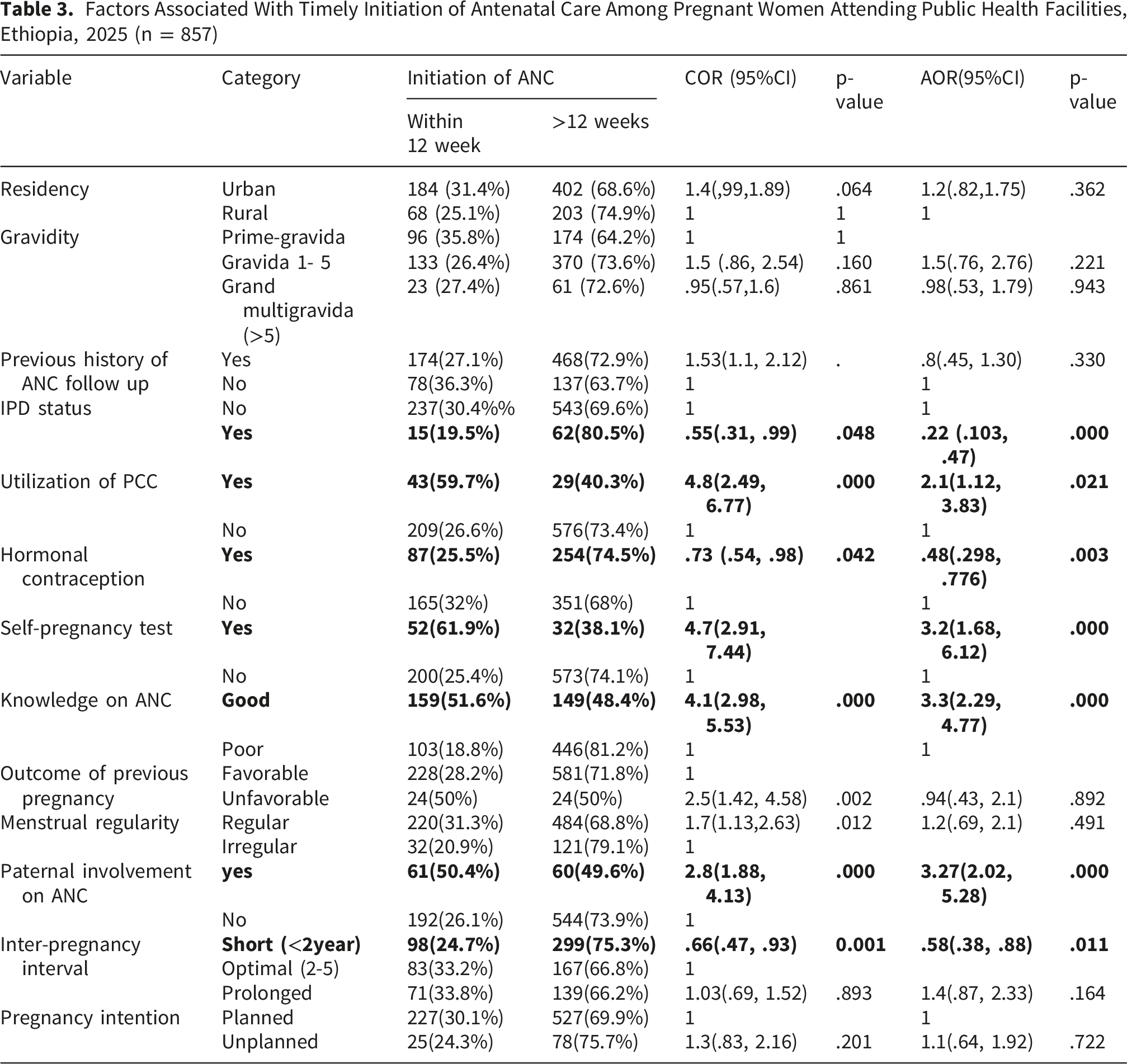
In the bivariable logistic regression analysis, thirteen variables were associated with timely initiation of ANC at a p-value< 0.25 and were considered potential confounders. These variables were included in the multivariable logistic regression model to adjust for their potential confounding effects. The variables included gravidity, residence, IDP status, PCC utilization, history of hormonal contraceptive use, self-pregnancy test use, menstrual cycle regularity, pregnancy intention, previous pregnancy outcomes, maternal knowledge, prior ANC experience, partner involvement, and inter-pregnancy interval.
Factors Associated With Timely Initiation of Antenatal Care Among Pregnant Women Attending Public Health Facilities, Ethiopia, 2025 (n = 857)
Discussion
This study assessed the timing of ANC initiation among pregnant women attending public health facilities. The proportion of women who initiated ANC timely was found to be 29.4% (95% CI: 26.4%–32.4%). This finding highlights a persistent public health concern, as more than two-thirds of pregnant women in the study area delay their first ANC visit beyond the optimal window for early detection and prevention of pregnancy-related complications. The result is consistent with several previous studies, suggesting a pattern of timely ANC initiation across various settings in Ethiopia and beyond. For example, a study based on the 2019 Ethiopian Demographic and Health Survey (EDHS) reported a national prevalence of timely ANC initiation at 26.8%, which closely aligns with our finding (Shiferaw et al., 2021).
Similarly, studies conducted in Ilu Ababor Zone (28.8%) (Tola et al., 2021), Mizan Aman town (30%) (Battu et al., 2023), Axum (27.5%) (Gebresilassie et al., 2019), reinforce the notion that timely ANC uptake remains suboptimal in diverse Ethiopian regions. Moreover, our finding is comparable to earlier national estimates from the 2016 EDHS, which showed that only 31% of women initiated ANC timely (31%) (Adulo & Hassen, 2023). Beyond Ethiopia, a similar trend is observed in other low-income settings. For instance, a study in Burundi, Nigeria also reported a timely ANC initiation rate of 27.5% and 26.7% respectively (Butoyi et al., 2023; Ndem et al., 2021). Underscoring that delayed ANC initiation is a common challenge across sub-Saharan Africa.
The proportion of women initiating their ANC timely in this study (29.4%) is notably lower than figures reported in several studies from other parts of Ethiopia and beyond. For instance, higher rates were observed in Hossana (34.3%) (Tessema et al., 2023), Bahir Dar (44.2%) (Tesfu et al., 2022), Addis Ababa (53%) (Girma et al., 2023), Wolaita Sodo (39%) (Hussen et al., 2016), Agaro town (41.9%) (Redi et al., 2022), systematic review on delayed ANC initiation in Ethiopia (36%) (Tesfaye et al., 2017), systematic review from demographic health survey data in Sub-Saharan Africa (38%) (Alem et al., 2022), Rwanda (51.7%) (Uwimana et al., 2023), Gambia (44%) (Nigatu & Birhan, 2023), south Africa (45%) (Muhwava et al., 2016), Afghanistan (55.8%) (Tawfiq et al., 2023), India (37%) (Tripathy & Mishra, 2023), Yemen (55.8%) (Tawfiq et al., 2023), London (72.8%) (McDonald et al., 2020), Nepal (70%) (Paudel et al., 2017), and USA (77.3%) (Osterman & Martin, 2018). The discrepancy between the findings of this study and those of previous studies can be explained by several contextual and methodological factors. Among studies conducted within Ethiopia including local studies and national systematic reviews the differences may stem from variations in study settings, regional disparities in access to maternal health services, and differences in participants’ socio-demographic profiles. This study includes; Unlike studies conducted in relatively stable urban or semi-urban settings, displaced women often experience disrupted access to health services, unfamiliarity with local health facilities, loss of social support networks, and competing survival priorities following displacement. These structural and social disruptions can substantially delay health-seeking behavior, including timely initiation of ANC (Abetie et al., 2025). Additionally, North Shewa is predominantly rural, with scattered settlements, limited transportation infrastructure, and variable availability of maternal health services. In contrast, studies reporting higher timely ANC initiation such as those from Addis Ababa, Bahir Dar, or Agaro town were conducted in urban settings where health facilities are more accessible, health information is more readily available, and women are more likely to have prior exposure to maternal health education. However, a key methodological difference that likely accounts for much of the observed variation is the definition of “timely initiation” of ANC. While earlier Ethiopian studies and reviews typically employed a 16-week gestational cutoff point in line with the FANC model, this study adopts the updated WHO recommendation, which defines timely initiation as the first ANC contact occurring within the first 12 weeks of gestation (Birungi, 2006; Organization, 2016). This stricter criterion likely contributed to the lower proportion of timely ANC initiation observed in the present study. When comparing findings with international studies, additional factors come into play. Countries such as the United States, South Africa, India, The Gambia, and Yemen generally report higher levels of timely ANC initiation. These differences are likely due to more favorable socio-economic conditions, stronger healthcare systems, and well-established maternal health policies in those countries. Furthermore, greater investments in health infrastructure, more widespread use of health information technologies, and robust community outreach programs contribute to improved timely ANC uptake (Anya et al., 2008; Ethiopian Public Health Institute, 2023; Myburgh et al., 2024). In Afghanistan and Rwanda, the referenced studies were population-based, using national demographic survey data that provide country-level representative estimates (Tawfiq et al., 2023; Uwimana et al., 2023). By contrast, our study focused on a single zonal city with a heterogeneous population, including IDPs, who may encounter additional barriers to timely ANC, such as limited mobility, low awareness, and socio-economic constraints. These local contextual factors likely explain the lower prevalence observed in our study compared to the national estimates from Afghanistan and Rwanda.
However, the proportion reported in our study is notably higher than that documented in previous studies conducted in rural Woreda of Sidama Zone, Southern Ethiopia (21.7%) (Geta & Yallew, 2017), Arba Minch in the Gamo Gofa Zone of Southern Ethiopia (17.4%) (Gebremeskel et al., 2015). As well as in other sub-Saharan African countries including Tanzania (24%) (Mgata & Maluka, 2019), South Sudan (14.1%) (Nasira Boi et al., 2022), Malawi (24.4%) (Palamuleni, 2024), Benin (24.6%) (Edgard-Marius et al., 2015), Bangladesh (11%) (Sarker et al., 2021), and South Africa (7.2%) (Beauclair et al., 2014). The discrepancies observed in the Sidama Zone study can be primarily attributed to its rural setting, where access to maternal health services and awareness about the importance of ANC remain limited. Rural women in such areas often face geographic, educational, and socio-cultural barriers that delay ANC initiation. In contrast, our study was conducted in a zonal city where health service infrastructure, access, and community health awareness are relative, which may explain the higher rate of timely ANC initiation (Belay et al., 2022; Kebede et al., 2022; Sekata, 2015). The differences between our findings and those from Arba Minch may be due in large part to the difference in the study periods. The Arba Minch study was conducted over a decade ago, during which time Ethiopia has implemented significant improvements in maternal health services, including expansion of health infrastructure, deployment of additional health professionals, and the strengthening of community-based health interventions such as the Health Extension Program. These advancements are likely to have had a positive impact on ANC uptake and timing (EMOH, 2010, 2023). As for the lower prevalence of timely ANC initiation in other Sub-Saharan African countries such as Tanzania, Malawi, Benin, and South Africa, these differences may be explained by a range of factors including variations in socio-demographic characteristics, health policy implementation, geographic access, and differences in health system performance. For instance, while South Africa has a relatively strong health infrastructure, disparities within urban informal settlements and rural areas may still hinder timely service utilization (Ebonwu et al., 2018; Phaswana-Mafuya et al., 2019). In contrast, Ethiopia’s targeted efforts at the community level, particularly in urban centers, may contribute to higher timely ANC uptake despite resource constraints (Medhanyie et al., 2012; Tiruneh et al., 2024). Particularly in Bangladesh and Gambia, the lower proportion of timely ANC initiation may be partly explained by the low prevalence of planned pregnancies, reported at 37.5% and 79.7%, respectively, compared to 88% in our study. Planned pregnancy is a well-established factor for timely utilization of maternal health services, as women and/or their partners are more likely to recognize the pregnancy promptly and initiate ANC on time, whereas unplanned pregnancies may delay care-seeking (Mekonnen et al., 2024; Tekelab et al., 2019). This difference likely contributes to the higher proportion of timely ANC initiation observed in our study. This study identified key determinants of timely ANC initiation, including being an IDP, prior use of PCC and hormonal contraceptives, use of self-pregnancy tests, good maternal knowledge on ANC, partner involvement, and short inter-pregnancy intervals. These factors suggest that health awareness, reproductive planning, male support, and targeted interventions among vulnerable groups play a critical role in promoting timely ANC uptake.
The finding of this study indicates that a significant proportion of pregnant women are still initiating ANC later than recommended, which is inconsistent with the WHO, 2016 ANC model that emphasizes initiating the first contact within the first 12 weeks of gestation to ensure comprehensive maternal and fetal health assessment (Organization, 2016). Moreover, the observed low level of timely initiation poses a challenge to achieving Sustainable Development Goal (SDG) 3.1, which aims to reduce the global maternal mortality ratio, and SDG 3.7, which seeks to ensure universal access to sexual and reproductive health-care services, including antenatal care. Strengthening timely ANC uptake is therefore essential for aligning local practices with these global maternal health targets (Organization, 2024).
This study found that internally displaced women had 78% lower odds of initiating ANC within the recommended time compared to non-displaced women. This finding is consistent with evidence from a study in Nigeria, which reported significantly lower ANC uptake among internally displaced women (Adebangbe & Mturi, 2021). The disparity may be attributed to multiple interconnected factors. IDPs often face limited access to maternal health services due to several challenges, including unfamiliarity with their new environment, lack of information and awareness, security concerns, and socio-cultural and psychosocial barriers (Chi et al., 2015; Okorafor et al., 2024; Sami et al., 2020). Moreover, health facilities serving displaced populations frequently suffer from critical limitations, such as staff shortages, restricted operating hours, and inadequate medical supplies, all of which further hinder timely ANC service utilization (Mohamed et al., 2021). These findings underscore the urgent need for targeted interventions to improve ANC access and timing among displaced women, addressing both systemic barriers and individual-level vulnerabilities. This highlights the need for interventions tailored specifically to the unique needs of IDPs, such as mobile outreach ANC services, community-based health education, enhanced referral networks, and integration of maternal health support within humanitarian assistance programs, as supported by existing literature on maternal health services for displaced populations. Although IDP status showed a strong association, the relatively small proportion of IDPs warrants cautious interpretation.
In this study, pregnant women who utilized PCC services for the current pregnancy were nearly twice as likely to initiate ANC within the recommended timeframe compared to those who did not. This finding aligns with evidence from a large-scale study in China, which demonstrated that women who accessed PCC were significantly more likely to initiate ANC timely and adhere to recommended maternal and child health services (Liu et al., 2006). This association can be attributed to the core function of PCC, which is to prepare reproductive-aged individuals both medically and behaviorally for a healthy pregnancy. PCC provides essential counseling, health screening, and risk assessment before conception, increasing women’s awareness of the importance of timely ANC initiation, institutional delivery, emergency preparedness and others. Moreover, women who receive PCC are more likely to be engaged with the healthcare system, understand their reproductive health needs, and follow recommended care pathways throughout pregnancy (Olson, 2020; Wilson, 2019). Therefore, PCC serves not only as a critical entry point to maternal health services but also as a catalyst for optimal and timely utilization of ANC and related interventions.
Pregnant women who used hormonal contraception prior to their current pregnancy were found to have 52% lower odds of initiating their first ANC visit timely. This association may be explained by the well-documented side effects of hormonal contraceptives, particularly their influence on menstrual cycle patterns. Hormonal contraceptive methods such as pills, injectable, implants, hormonal IUDs can often cause menstrual irregularities, including delayed, light, or absent periods. These changes can obscure the early signs of pregnancy, especially missed menses, which is commonly used by women to detect pregnancy. As a result, women may misattribute amenorrhea to contraceptive side effects rather than pregnancy, leading to a delay in pregnancy recognition and subsequently late initiation of ANC (Richter, 2023). This finding aligns with clinical observations and literature reporting that menstrual irregularities due to hormonal contraception can interfere with the timely detection of pregnancy and delay access to maternal health services (Nobles et al., 2022). Therefore, healthcare providers should counsel women using hormonal contraception about the possibility of irregular bleeding and the importance of early pregnancy testing if they suspect pregnancy, to promote timely ANC initiation. Providers should incorporate clear guidance on how contraceptive-related menstrual changes may mask early pregnancy signs and emphasize proactive pregnancy testing and prompt ANC initiation, particularly for women using methods known to cause cycle irregularities. Pregnant women with good knowledge of ANC, particularly the importance of timely initiation, are about three times more likely to begin their first visit timely. This aligns with studies from Southwest Ethiopia, Axum, Ambo, and multi-country analyses in sub-Saharan Africa, all showing a strong positive association between maternal knowledge and timely ANC uptake (Alem et al., 2022; Daniels-Donkor et al., 2024; Fetene et al., 2023; Redi et al., 2022). Informed women are more likely to seek care proactively, enabling timely monitoring of fetal development, management of complications, and receipt of essential health education, which reduces adverse pregnancy outcomes, including late complications and congenital anomalies (Mohamed et al.(2016); Tesfay et al., 2023). These findings emphasize the need for community and facility-level interventions to improve maternal knowledge on ANC timing and benefits.
Women receiving positive partner support were nearly three times more likely to initiate ANC timely compared to those without such support. This finding is consistent with studies from West Central Ethiopia, Hawassa, Mekele, Southern Ethiopia, and Gedeo Zone, which report a strong association between partner involvement and timely ANC initiation (Betru & Birhanu, 2024); Degefa et al., 2024; Gessesse et al., 2024; Haile & Brhan, 2014; Mamo et al., 2021). Partner support provides emotional and practical assistance, including shared decision-making, financial help, and accompaniment to health facilities, which reduces barriers and reinforces the importance of timely ANC (Abute Woiloro et al., 2025; Adisu et al., 2025; Betru & Birhanu, 2024). These findings highlight the need for health interventions promoting male engagement, such as couple-based education, community sensitization, and male-friendly antenatal services.
Women with short inter-pregnancy intervals are significantly less likely to initiate ANC timely. Although direct evidence is limited, literature shows that short birth spacing is associated with lower uptake of reproductive health services and adverse pregnancy outcomes (Brhane et al., 2019; Gurmu et al., 2022; Jena et al., 2021). Short intervals are often linked to unintended pregnancies, which can delay pregnancy recognition and timely engagement with maternal health services due to denial, stress, or lack of support (Ahrens et al., 2018; Haight et al., 2019). Additionally, closely spaced pregnancies may limit women’s physical, emotional, and social capacity to seek care, compounded by childcare responsibilities and financial constraints in low-resource settings like Ethiopia. These findings highlight the importance of integrated postpartum family planning services to promote optimal birth spacing and timely ANC uptake.
Implication for Practice
The findings highlight the need for policymakers to prioritize timely ANC within maternal health programs, implement targeted strategies for vulnerable populations such as internally displaced women, and expand access to preconception care, family planning, and other reproductive health services to strengthen the maternal continuum of care. Timely ANC initiation is likely to be cost-effective, as it facilitates early identification and management of pregnancy-related risks, prevents complications, and reduces the need for costly emergency obstetric interventions. Given that maternal and neonatal health services are exempted from fees in Ethiopia, the government may benefit from early recognition and management of complications that would otherwise require expensive care.
In line with our findings, we recommend specific, actionable interventions at the community and facility levels, including:
Community-based awareness programs to improve maternal knowledge of ANC, utilizing health extension workers, local women’s groups, and mass media campaigns to disseminate culturally appropriate information on timely ANC initiation and self-pregnancy testing. Evidence shows such programs significantly improve maternal health knowledge and service utilization. Male engagement initiatives to enhance paternal involvement in maternal care. Practical approaches include inviting partners to ANC counseling sessions, community dialogues targeting men, and inclusion of male-focused educational materials. Active male participation positively influences timely ANC attendance and overall maternal health outcomes. Promotion of home-based self-pregnancy testing to facilitate timely pregnancy recognition, particularly among women using hormonal contraception, which can mask early pregnancy signs.
Tailored interventions for IDPs, such as mobile ANC outreach services, temporary maternal health clinics in displacement camps, community health volunteers from within the IDP population, and strengthened referral networks. Evidence suggests that context-specific approaches for displaced populations improve access and utilization of maternal health services (Chi et al., 2015; Mohamed et al., 2021; Sami et al., 2020). By integrating these strategies, policymakers and health planners can enhance timely ANC initiation, particularly among vulnerable populations, improve maternal and neonatal outcomes, and optimize the use of available health resources. Midwives
Strength & Limitation of the Study
The strength of this study lies in its focus on timely initiation of ANC based on the newly recommended guidelines. It also addresses a mixed population, including urban, rural, and IDP women, and incorporates previously unstudied variables, enhancing the comprehensiveness of the findings. While this study provides important insights into timely ANC initiation, a few points should be considered. The cross-sectional design limits causal interpretations. Data were collected through participant interviews, which may introduce minor recall bias; however, collection at discharge in a calm environment with adequate time for responses was implemented to minimize this risk. This study was facility-based and conducted in a single zonal city, with a relatively lower proportion of rural participants. As a result, findings may not be fully generalizable to rural Ethiopian settings, where geographic, socioeconomic, and health system barriers differ. Future community-based and multi-regional studies are recommended. Furthermore, Although the study included 869 participants, the sample size was calculated for the secondary objective and not specifically for each predictor in the multivariable analysis. Some non-significant associations may reflect limited power for certain variables. Consequently, caution is needed when interpreting the results. Despite these considerations, the study’s strengths including timely data collection, high participation, inclusion of unstudied variables, and a well-characterized population support the reliability and relevance of the findings.
Conclusion
This study found that timely initiation of ANC remains low in the study area. Key factors associated with timely ANC initiation include internally displaced status, use of PCC, prior hormonal contraceptive use, self-pregnancy testing, maternal knowledge, partner support, and optimal birth spacing. To improve timely ANC uptake, we recommend strengthening PCC services, promoting self-pregnancy testing, enhancing community awareness, and encouraging male involvement. Targeted interventions addressing these determinants are essential for improving maternal and neonatal health outcomes.
Footnotes
Acknowledgements
We would like to express our sincere gratitude to Debre Berhan University, Asrat Woldeyes Health Science Campus for granting ethical clearance and supporting the successful implementation of this study. Our heartfelt appreciation also goes to the data collectors and supervisors for their commitment and diligence in gathering high-quality data in accordance with the study protocol. Most importantly, we extend our deepest thanks to all the study participants for their time, trust, and willingness to share valuable and reliable information.
Ethical Considerations
This study involving human participants was reviewed and approved by the Institutional Review Board (IRB) of Debre Berhan University, Asrat Woldeyes Health Science Campus (Ref. NO: IRB-396). All procedures performed in the study were in accordance with the ethical standards of the institutional and national research committees, and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Consent to Participate
Prior to data collection, written informed consent was obtained from all participants. The purpose of the study, the procedures involved, potential risks and benefits, and the voluntary nature of participation were clearly explained to each participant. Confidentiality and anonymity were assured throughout the research process.
Author Contributions
TNK played a significant role in the proposal development, data entry, and conceptualization. Each author contributed to the formal analysis and the initial draft writing. They equally participated in the preparation, editing, and approval of the paper for submission for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.