
Abstract
Background
The relationship between academic self-efficacy and clinical decision-making is crucial for nursing students’ professional development. Understanding this relationship contributes to nursing education literature globally, particularly regarding how psychological constructs influence clinical competence development across diverse cultural contexts.
Methods
A descriptive cross-sectional correlational design was employed, adhering to the STROBE checklist for cross-sectional studies. Using convenience sampling, 350 nursing students from the Faculty of Nursing, Arab American University, Palestine were approached for participation. The Clinical Decision-Making in Nursing Scale and Academic Self-Efficacy Scale were administered. Descriptive statistics, Pearson's correlation, and multiple linear regression were conducted for data analysis.
Results
Of 350 students approached, 321 completed the study. The results revealed a significant positive correlation between academic self-efficacy and clinical decision-making (r = 0.538, P < .01). Multiple linear regression analysis identified academic self-efficacy (β = 0.389, P < .001), grade point average (β = 0.272, P < .001), and educational support (β = 0.162, P < .001) as factors significantly associated with clinical decision-making, collectively explaining 45.0% of the variance. Students scored highest in values-based decision-making (mean = 38.0, SD = 4.4) and lowest in information assimilation (mean = 31.9, SD = 7.2). No statistically significant gender differences were observed.
Conclusion
This study provides evidence of a significant association between academic self-efficacy and clinical decision-making among nursing students. While these findings contribute to understanding factors associated with decision-making skills, the cross-sectional design precludes causal conclusions. Nursing education programs may benefit from implementing pedagogical strategies that build self-efficacy, such as simulation and mentorship, with appropriate adaptation to local contexts. Further longitudinal and experimental research across diverse settings is needed to establish causality and inform evidence-based educational interventions.
Introduction
Contemporary nursing education faces the critical challenge of preparing students who can function as autonomous, confident decision-makers in increasingly complex healthcare environments (Benner et al., 2010). This transformation from dependent learners to independent practitioners requires not only the acquisition of clinical knowledge and technical skills, but also the development of psychological attributes that support effective decision-making under pressure (Abuhammad & Hamaideh, 2022). Among these psychological constructs, academic self-efficacy emerges as an important determinant of how nursing students approach learning challenges and subsequently translate their educational experiences into clinical competence (Bandura, 1997).
Review of Literature
Theoretical Framework
This study is explicitly grounded in Bandura's (1997) social cognitive theory, which provides the conceptual foundation for understanding how self-efficacy beliefs influence human behavior, motivation, and performance outcomes. According to this theoretical framework, self-efficacy, defined as context-specific judgments of one's capabilities to organize and execute courses of action, directly influences an individual's choice of activities, level of effort, degree of persistence, and resilience when facing obstacles (Bandura, 1997). The theory posits four primary sources of self-efficacy: mastery experiences, vicarious experiences, social persuasion, and physiological/affective states, which collectively shape individuals’ confidence in their capabilities.
Within nursing education, this theoretical framework suggests that students with stronger academic self-efficacy are more likely to engage proactively with complex learning materials, demonstrate greater perseverance during challenging clinical problem-solving tasks, employ more effective cognitive strategies, and consequently develop more robust decision-making competencies (Artino, 2012; Bandura, 2006). The proposed mechanism involves self-efficacy beliefs influencing how students process information, evaluate alternatives, and commit to courses of action when facing clinical uncertainty, processes central to clinical decision-making. However, while theoretically compelling, these proposed mechanisms require empirical validation, particularly across diverse cultural and educational contexts.
Clinical decision-making in nursing has been extensively conceptualized through multiple theoretical models. Tanner's (2006) model of clinical judgment describes a process involving noticing, interpreting, responding, and reflecting, emphasizing the interplay between nurses’ knowledge, experience, and contextual factors. Bucknall (2003) proposed a framework highlighting the influence of environmental, situational, and individual factors on nurses’ real-time decisions. More recently, Tiffen et al. (2014) developed a contiguous definition conceptualizing clinical decision-making as a contextual, continuous, and evolving process involving data collection, interpretation, evaluation, and implementation. These models collectively emphasize that effective decision-making requires not only cognitive skills but also confidence in one's ability to execute decisions, theoretically linking to self-efficacy constructs.
Despite this strong theoretical rationale linking self-efficacy to decision-making processes, empirical research specifically examining this relationship within nursing education contexts remains limited and fragmented. A systematic review by Honicke and Broadbent (2016) examining academic self-efficacy and performance across educational contexts found consistent positive associations, but noted that nursing education research was underrepresented. Studies specifically examining self-efficacy and clinical decision-making in nursing students have produced inconsistent findings. While Chesser-Smyth and Long (2013) found that self-confidence influenced clinical performance among Irish nursing students, McLaughlin et al. (2008) reported that self-efficacy predicted retention but not clinical competence in a UK sample. Gibbons and Dempsey (2011) identified positive correlations between self-efficacy and decision-making in a small sample of nursing students, but the cross-sectional design limited causal conclusions. Zhao et al. (2020) found similar relationships among Chinese nursing students, suggesting potential cross-cultural applicability, though the mechanisms underlying this relationship remain underexplored.
Furthermore, the existing literature reveals several gaps requiring attention. First, most studies have been conducted in Western educational contexts, limiting understanding of how cultural and contextual factors may influence the self-efficacy–decision-making relationship (Sabanciogullari & Dogan, 2015). Second, the specific domains of self-efficacy that most strongly relate to decision-making components remain unspecified. Third, limited research has examined how demographic and educational factors interact with self-efficacy to influence decision-making development. Fourth, few studies have explored these relationships in resource-constrained educational environments where external supports may be limited, potentially amplifying the importance of psychological resources like self-efficacy.
The Palestinian Context
The Palestinian context presents unique considerations that may influence both academic self-efficacy and clinical decision-making processes among nursing students. These contextual factors include: (1) resource constraints in educational settings limiting access to current literature, simulation technologies, and diverse clinical learning opportunities; (2) political instability and associated stressors that may affect students’ psychological well-being and academic focus; (3) cultural values emphasizing collective decision-making approaches (shura or consultation) over individual autonomy, potentially shaping how students conceptualize and approach clinical decisions; (4) healthcare system characteristics that differ from Western models where most nursing education research has been conducted; and (5) strong family and community support systems that may buffer against educational challenges (Giacaman et al., 2009; Khatib et al., 2021; Shoqirat et al., 2021). These contextual factors provide both challenges and potential cultural strengths that warrant investigation.
Study Purpose and Research Questions
Therefore, the purpose of this correlational study is to examine the relationship between academic self-efficacy and clinical decision-making among nursing students in Palestine, addressing the identified gaps in the literature. This study aims to contribute to the international nursing education literature by: (1) providing empirical evidence for the theoretical relationship between academic self-efficacy and clinical decision-making in an under-researched cultural context; (2) identifying specific domains of self-efficacy and decision-making that demonstrate strongest associations; (3) examining demographic and educational factors associated with decision-making abilities; and (4) offering insights for culturally responsive educational strategies applicable to similar contexts globally.
Based on the theoretical framework and literature review, this study sought to answer the following specific research questions:
What is the relationship between academic self-efficacy and clinical decision-making among nursing students in Palestine? Which demographic and academic factors are associated with clinical decision-making abilities among Palestinian nursing students? Are there significant differences in academic self-efficacy and decision-making abilities based on gender, academic year, or socioeconomic status? How do specific domains of academic self-efficacy relate to different components of clinical decision-making?
Method
Design
This study employed a descriptive cross-sectional correlational design following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies (von Elm et al., 2007). The study was conducted at the Faculty of Nursing, Arab American University, Palestine, during the spring semester of the 2025 academic year.
Sample and Setting
The target population comprised approximately 1,500 undergraduate nursing students enrolled at the Faculty of Nursing, Arab American University, Palestine. Using convenience sampling, the required sample size was calculated using RaoSoft sample size calculator with parameters of 95% confidence level, 5% margin of error, and 50% response distribution, yielding a minimum requirement of 306 participants. This calculation accounted for the total population of 1,500 students. To account for potential nonresponse and incomplete surveys, 350 students were approached for participation.
Inclusion criteria included: (1) enrolled as undergraduate nursing students in second, third, or fourth year; (2) aged 18 years or older; (3) able to read and understand Arabic; and (4) willing to provide informed consent. Exclusion criteria included: (1) first-year students were excluded because clinical training commences in the second year, and these students lack clinical exposure necessary for meaningful clinical decision-making assessment; (2) students on academic probation; and (3) exchange or visiting students not enrolled in the regular program.
Participant Recruitment
Participant recruitment occurred during scheduled class sessions following coordination with course instructors. Research assistants who were not involved in teaching or grading these students provided brief presentations explaining the study purpose, procedures, voluntary nature of participation, and confidentiality protections. Students were informed that nonparticipation would not affect their academic standing. Questionnaires were distributed during break times or immediately following class sessions to minimize perceived coercion. No incentives were provided for participation. Interested students completed questionnaires in quiet classroom settings, with research assistants available to clarify questions without influencing responses.
Of the 350 students approached, 321 provided complete responses (response rate: 91.7%). Sample attrition management procedures were implemented. The high response rate minimizes the potential for nonresponse bias. To assess representativeness, demographic characteristics of respondents were compared with available institutional data on the general student population. Available institutional data from the university registrar's office for the 2024–2025 academic year indicated the nursing student population was 52% female with a mean age of 21.3 years. Comparison revealed no significant differences in age (t = 1.24, P = .216), gender distribution (χ2 = 0.83, P = .362), or academic year representation (χ2 = 2.15, P = .341) between the sample and population, supporting the sample's representativeness. However, the use of convenience sampling inherently limits the external validity of the findings. The generalizability of results is confined to similar student populations within comparable institutional and cultural contexts, and potential selection bias cannot be ruled out.
Data Collection Instruments
The study utilized a comprehensive three-part questionnaire, employing two previously published and validated instruments.
Part 1: Demographic Characteristics
A researcher-developed questionnaire collected data on age, gender, academic year, cumulative grade point average, monthly family income, and availability of educational support (tutoring, mentorship, or family academic assistance). Monthly income was collected using categories reflecting the Palestinian context: low (below 2,000 Israeli new shekel [ILS]), moderate (2,000–5,000 ILS), and high (above 5,000 ILS), based on Palestinian Central Bureau of Statistics income classifications.
Part 2: Clinical Decision-Making in Nursing Scale
The Clinical Decision-Making in Nursing Scale, developed by Jenkins (1983), assesses nursing students’ perceptions of their decision-making abilities. The instrument contains 40 items distributed across four domains of 10 items each:
Search for Alternatives or Options: Ability to generate and consider multiple solutions Evaluation and Re-evaluation of Consequences: Assessment of potential outcomes and continuous monitoring Canvassing of Objectives and Values: Alignment of decisions with professional values and patient needs Search for and Unbiased Assimilation of New Information: Information gathering and objective evaluation
Items are rated on a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree), with total scores ranging from 40 to 200. Higher scores indicate stronger perceived decision-making abilities. Domain scores range from 10 to 50. The instrument measures perceived rather than observed decision-making ability. Scoring interpretation follows the instrument developer's guidelines, with scores 40–80 indicating low, 81–140 moderate, and 141–200 high perceived decision-making ability.
The original instrument demonstrated good reliability (α = .83) and has been previously validated in Palestinian healthcare contexts (Abu Arra et al., 2023; Ayed et al., 2023; Batran et al., 2022).
Part 3: Academic Self-Efficacy Scale
The Academic Self-Efficacy Scale developed by Gafoor and Ashraf (2007) measures students’ confidence across multiple academic domains. The instrument contains 40 items across 12 domains: Learning Process, Reading, Memory, Time Management, Teacher–Student Relationship, Resource Utilization, Goal Orientation, Psychological Adjustment, Examination Confidence, Comprehension, Curricular Activities, and Peer Relationships.
Items are rated on a 5-point Likert scale (1 = not confident at all, 5 = completely confident). Domain scores are calculated as means of constituent items, and overall academic self-efficacy is calculated as the mean of all 40 items, yielding scores ranging from 1 to 5. Higher mean scores indicate greater academic self-efficacy. The instrument measures students’ confidence in their academic capabilities rather than actual academic performance.
The original instrument demonstrated strong test–retest reliability (r = .85) and has been used in diverse educational contexts.
Cultural Adaptation and Translation
Both instruments were originally available in English. Following World Health Organization (WHO) guidelines for translation and adaptation of instruments, the following rigorous process was implemented: forward translation by two independent bilingual nursing academics, synthesis of forward translations by a third bilingual expert, back-translation by a certified translator unfamiliar with the original instruments, and expert committee review comprising three nursing education faculty members and one linguistics expert for conceptual equivalence. Cognitive interviews with 10 nursing students representing different academic years confirmed comprehensibility, clarity, and cultural appropriateness of the Arabic versions. Minor wording modifications were made based on cognitive interview feedback to enhance clarity without altering meaning. This rigorous translation process ensured that the instruments maintained their psychometric properties while being culturally appropriate for the Palestinian context.
Validity and Reliability
Construct validity was assessed through confirmatory factor analysis using maximum likelihood estimation. For the Clinical Decision-Making in Nursing Scale, the four-factor model demonstrated acceptable fit: χ2/df = 2.34, comparative fit index (CFI) = 0.91, root mean square error of approximation (RMSEA) = 0.06 (90% CI 0.05–0.07), standardized root mean square residual (SRMR) = 0.05. Factor loadings ranged from 0.52 to 0.84, all significant at P < .001. For the Academic Self-Efficacy Scale, the 12-factor model showed adequate fit indices: χ2/df = 2.18, CFI = 0.89, RMSEA = 0.05 (90% CI 0.04–0.06), SRMR = 0.06. These results support the factorial validity of both instruments in the Palestinian context.
Content validity assessment was conducted using a panel of five nursing education experts (minimum 10 years’ experience in nursing education and research) who reviewed both instruments for relevance, clarity, and cultural appropriateness using a 4-point rating scale. The Scale-Level Content Validity Index based on the universal agreement method was 0.85 for the Clinical Decision-Making Scale and 0.88 for the Academic Self-Efficacy Scale. The Average Content Validity Index was 0.92 and 0.94 respectively. Item-level Content Validity Index exceeded 0.80 for all items, indicating excellent content validity.
Reliability assessment was performed through a pilot study with 30 nursing students (excluded from the main study) to confirm instrument reliability. Cronbach's alpha coefficients were: Clinical Decision-Making in Nursing Scale (α = .82) and Academic Self-Efficacy Scale (α = .84). Test–retest reliability with a 2-week interval in the pilot sample (n = 25) showed intraclass correlation coefficients of 0.88 for the Clinical Decision-Making Scale and 0.86 for the Academic Self-Efficacy Scale, indicating good stability.
In the main study, Cronbach's alpha values were .85 for Clinical Decision-Making in Nursing Scale with domain-specific alphas ranging from .79 to .88 and .88 for the Academic Self-Efficacy Scale with domain-specific alphas ranging from .76 to .91, indicating excellent internal consistency.
Data Collection Procedure
Data were collected from May 4 to July 4, 2025. To ensure voluntary participation and minimize coercion, several procedures were implemented. Research assistants who were not part of the course instruction administered the surveys to maintain independence in data collection. Participation was anonymous, and no identifiers were collected; numbered codes were used on surveys. Students received several reminders that their participation was completely voluntary, would not impact their grades, and that they were free to withdraw at any point. Additionally, data collection was conducted during nonclass times to minimize pressure. Written informed consent was obtained before participation using forms that made explicit the study's purpose, procedures, risks, and benefits. Surveys were completed by participants in quiet classroom conditions, a process that lasted approximately 20–25 min, with research assistants available to clarify questions without influencing responses.
Ethical Considerations
Ethical approval was obtained from the institutional review board at Arab American University, Palestine (Ref. No. J-2025/A/16/N) prior to data collection. All participants provided written informed consent after receiving detailed information about the study. Confidentiality and anonymity were maintained throughout the study. Participants were informed of their right to withdraw at any time without consequences. Data were stored on password-protected computers accessible only to the research team. All procedures followed the ethical principles of the Declaration of Helsinki.
Statistical Analysis
Data analysis was conducted using SPSS version 26.0 and AMOS version 24.0 for confirmatory factor analysis. Missing data were minimal (less than 2% for any variable) and were handled using listwise deletion for correlation analyses and pairwise deletion for descriptive statistics. Little's Missing Completely at Random test was nonsignificant (χ2 = 34.27, df = 28, P = .192), indicating data were missing completely at random.
Data normality was assessed using Kolmogorov–Smirnov tests (all P > .05), Q–Q plots, and histograms, confirming normal distribution for all continuous variables. Skewness values ranged from −0.34 to 0.28 and kurtosis values from −0.42 to 0.51, all within acceptable ranges for normal distribution (±1). The assumptions underlying Pearson's correlation (linearity, normality of residuals, homoscedasticity) were visually and statistically assessed and met. Scatterplots confirmed linear relationships, and Breusch–Pagan tests for heteroscedasticity were nonsignificant (P > .05 for all comparisons).
Descriptive statistics (means, standard deviations, frequencies) characterized the sample. Pearson's product–moment correlations examined relationships between continuous variables, while point–biserial correlations assessed relationships with dichotomous variables. Correlation strength interpretation followed Cohen's (1988) conventions: small (r = .10), medium (r = .30), and large (r = .50).
Multiple linear regression analysis using the enter method was used to identify variables associated with clinical decision-making, with clinical decision-making total score as the dependent variable. Independent variables were selected based on theoretical relevance and significant bivariate correlations, including: academic self-efficacy (continuous), age (continuous), grade point average (continuous), academic year (categorical, entered as dummy variables), monthly income (categorical, entered as dummy variables with low income as reference), and educational support (dichotomous). Assumptions of linearity, independence of errors (Durbin–Watson = 1.94, within an acceptable range of 1.5–2.5), homoscedasticity, and multicollinearity were verified. Variance inflation factor values were examined to assess multicollinearity, with all values below 3.0 (range 1.12–2.34) indicating acceptable levels. Normal probability plots confirmed normality of residuals.
Subgroup analyses were conducted to examine differences across academic years using one-way analysis of variance (ANOVA) with posthoc Tukey’s honestly significant difference (HSD) tests for pairwise comparisons. Independent samples t-tests compared gender differences. Effect sizes were calculated using Cohen's d for t-tests and eta-squared (η2) for ANOVA.
Statistical significance was set at α = .05 for all analyses. All tests were two-tailed. No adjustments were made for multiple comparisons to maintain statistical power, though this may increase type I error risk. Sensitivity analyses were not conducted as the study employed a single analytical approach appropriate for the research questions and data structure.
Results
Participants’ Characteristics
Three hundred twenty-one nursing students completed the study. Table 1 presents comprehensive demographic characteristics. The sample had a mean age of 21.5 ± 1.2 years (range 19–25 years) with nearly equal gender distribution (163 female, 50.8%; 158 male, 49.2%). Academic year distribution was: second year (n = 93, 29.0%), third year (n = 107, 33.3%), and fourth year (n = 121, 37.7%). The mean cumulative grade point average was 2.9 ± 0.5 (range 2.0–4.0 on a 4.0 scale). Monthly family income distribution showed 75 (23.4%) reporting low income, 176 (54.8%) moderate income, and 70 (21.8%) high income. Most participants (201, 62.6%) reported receiving some form of educational support, including family assistance (n = 142, 44.2%), peer tutoring (n = 98, 30.5%), or formal mentorship (n = 67, 20.9%), with some students reporting multiple forms of support.
Demographic Characteristics of Participants (N = 321).
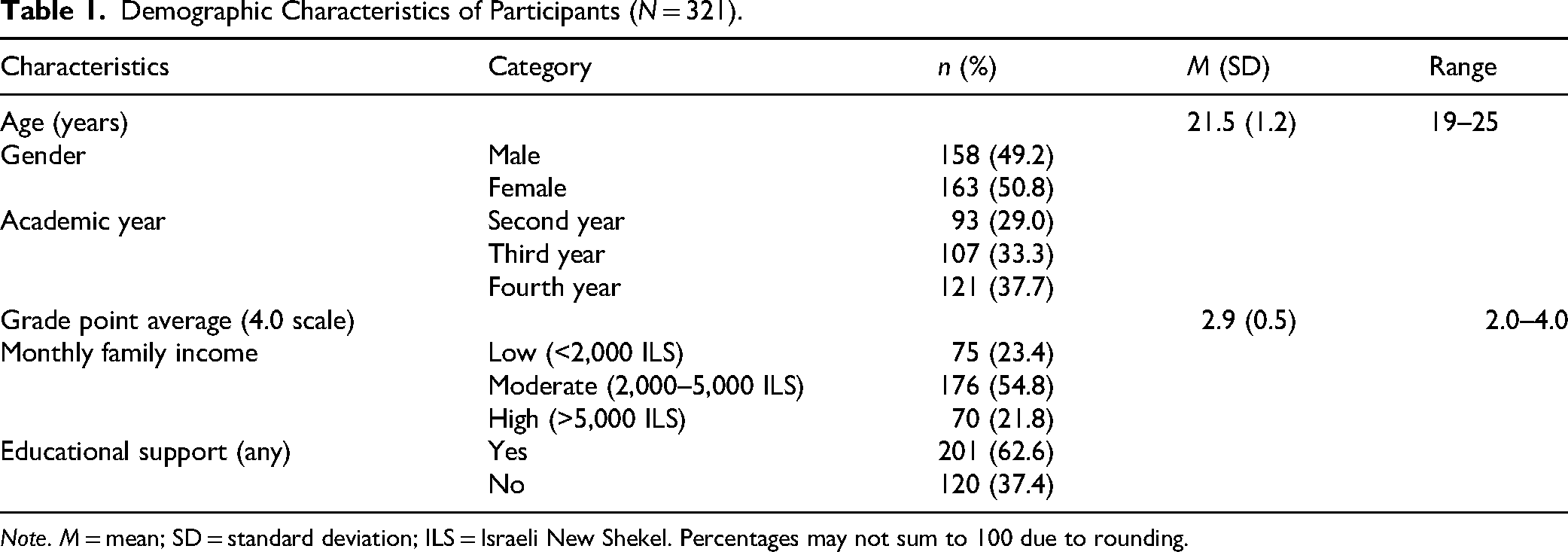
Note. M = mean; SD = standard deviation; ILS = Israeli New Shekel. Percentages may not sum to 100 due to rounding.
Academic Self-Efficacy and Clinical Decision-Making Scores
Table 2 presents descriptive statistics for both primary variables. The overall Clinical Decision-Making mean score was 142.5 ± 16.1 (possible range: 40–200; observed range: 98–185), indicating moderately high perceived decision-making abilities. Among clinical decision-making domains, “Canvassing of objectives and values” demonstrated the highest mean score (38.0 ± 4.4), while “Search for and unbiased assimilation of new information” showed the lowest (31.9 ± 7.2).
Distribution of Clinical Decision-Making and Academic Self-Efficacy Scores (N = 321).

Note. M = mean; SD = standard deviation. Domain scores for Clinical Decision-Making range 10–50. Academic Self-Efficacy domain scores represent mean item scores (range 1–5).
The overall Academic Self-Efficacy mean score was 3.8 ± 0.9 (possible range: 1–5; observed range: 1.8–5.0), suggesting high perceived academic confidence. The domains of Teacher–Student Relationship, Goal Orientation, and Examination Confidence achieved the highest means (3.9 each), while Comprehension scored lowest (3.6 ± 1.0).
Figure 1 presents a visual comparison of the four Clinical Decision-Making in Nursing Scale domain scores. As illustrated in Figure 1, students demonstrated particular strength in values-based decision-making (mean = 38.0, SD = 4.4) while showing the greatest opportunity for growth in information assimilation skills (mean = 31.9, SD = 7.2).

Comparison of Clinical Decision-Making in Nursing Scale domain scores among Palestinian nursing students (N = 321). Note. Error bars represent standard deviations. The dashed line indicates maximum possible score per domain (50). Students demonstrated particular strength in values-based decision-making while showing opportunity for growth in information assimilation skills.
Subgroup Analysis by Academic Year and Gender
One-way ANOVA revealed statistically significant differences in clinical decision-making scores across academic years, F(2, 318) = 8.42, P < .001, η2 = 0.05 (small to medium effect). Posthoc Tukey’s HSD tests indicated that fourth-year students (M = 147.3, SD = 15.2) scored significantly higher than second-year students (M = 138.1, SD = 16.8, P < .001, Cohen's d = 0.58) and third-year students (M = 141.2, SD = 15.4, P = .024, Cohen's d = 0.40). No significant difference was found between second- and third-year students (P = .287, Cohen's d = 0.19).
Similarly, academic self-efficacy differed significantly by academic year, F(2, 318) = 5.67, P = .004, η2 = 0.03 (small effect). Fourth-year students reported higher self-efficacy (M = 4.0, SD = 0.8) compared to second-year students (M = 3.6, SD = 1.0, P = .003, Cohen's d = 0.45). Third-year students (M = 3.8, SD = 0.9) did not differ significantly from either second-year (P = .215, Cohen's d = 0.22) or fourth-year students (P = .178, Cohen's d = 0.23).
Independent samples t-tests revealed no significant gender differences in clinical decision-making (males: M = 141.8, SD = 16.5; females: M = 143.2, SD = 15.7; t(319) = 0.78, P = .436, Cohen's d = 0.09) or academic self-efficacy (males: M = 3.8, SD = 0.9; females: M = 3.9, SD = 0.9; t(319) = 1.05, P = .295, Cohen's d = 0.11).
Correlational Analysis
Table 3 presents correlation results addressing Research Questions 1 and 3. A statistically significant strong positive correlation was found between overall clinical decision-making and academic self-efficacy (r = .538, P < .001), indicating that students with higher academic self-efficacy tend to demonstrate better decision-making abilities. This relationship remained significant when examined by academic year: second-year (r = .512, P < .001), third-year (r = .546, P < .001), and fourth-year (r = .561, P < .001), with no significant differences between correlation coefficients (Fisher's z-tests, all P > .05).
Bivariate Correlations Between Primary Study Variables and Clinical Decision-Making (N = 321).

Note. r = Pearson's correlation coefficient for continuous variables; pb.r = point–biserial correlation coefficient for dichotomous variables. Full correlation matrix including intercorrelations among all demographic variables is presented in Table 4. **Correlation is significant at the .01 level (2-tailed). *Correlation is significant at the .05 level (2-tailed).
Academic self-efficacy was also significantly correlated with grade point average (r = .462, P < .001), indicating a moderate to strong relationship between students’ confidence in their academic abilities and their actual academic performance. Significant positive correlations were also observed between clinical decision-making and grade point average (r = .425, P < .001), age (r = .327, P < .001), academic year (r = .316, P < .001), and educational support (r = .284, P < .001). A weaker but statistically significant correlation existed between clinical decision-making and monthly income (r = .123, P = .027). Notably, no significant gender differences were found in either academic self-efficacy or clinical decision-making (r = .059, P = .290). The complete correlation matrix displaying intercorrelations among all demographic variables is presented in Table 4.
Correlation Matrix of Clinical Decision-Making, Academic Self-Efficacy, and Demographic Variables (N = 321).
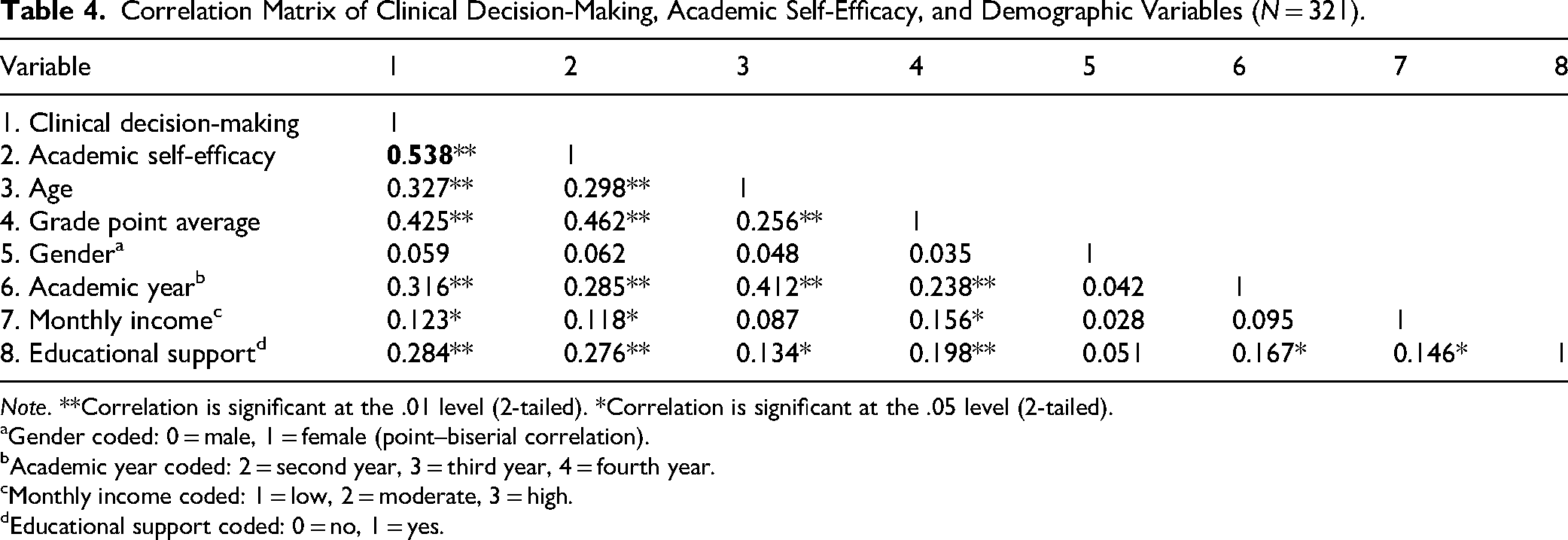
Note. **Correlation is significant at the .01 level (2-tailed). *Correlation is significant at the .05 level (2-tailed).
Gender coded: 0 = male, 1 = female (point–biserial correlation).
Academic year coded: 2 = second year, 3 = third year, 4 = fourth year.
Monthly income coded: 1 = low, 2 = moderate, 3 = high.
Educational support coded: 0 = no, 1 = yes.
Table 4 presents the comprehensive correlation matrix addressing relationships among all study variables. Significant intercorrelations were observed among demographic variables, including positive associations between age and academic year (r = .412, P < .001), grade point average and educational support (r = .198, P < .01), and monthly income with both grade point average (r = .156, P < .05) and educational support (r = .146, P < .05). These intercorrelations, while modest, support their inclusion as covariates in the regression analysis.
Table 5 presents domain-specific correlations addressing Research Question 4. All academic self-efficacy domains correlated significantly with clinical decision-making total scores, with coefficients ranging from r = .312 to r = .501. The strongest correlations with clinical decision-making were observed for Goal Orientation (r = .501, P < .001), Examination Confidence (r = .487, P < .001), and Learning Process (r = .472, P < .001). The weakest correlations were for Peer Relationship (r = .312, P < .001) and Curricular Activities (r = .345, P < .001).
Domain-Specific Correlations Between Academic Self-Efficacy and Clinical Decision-Making (N = 321).
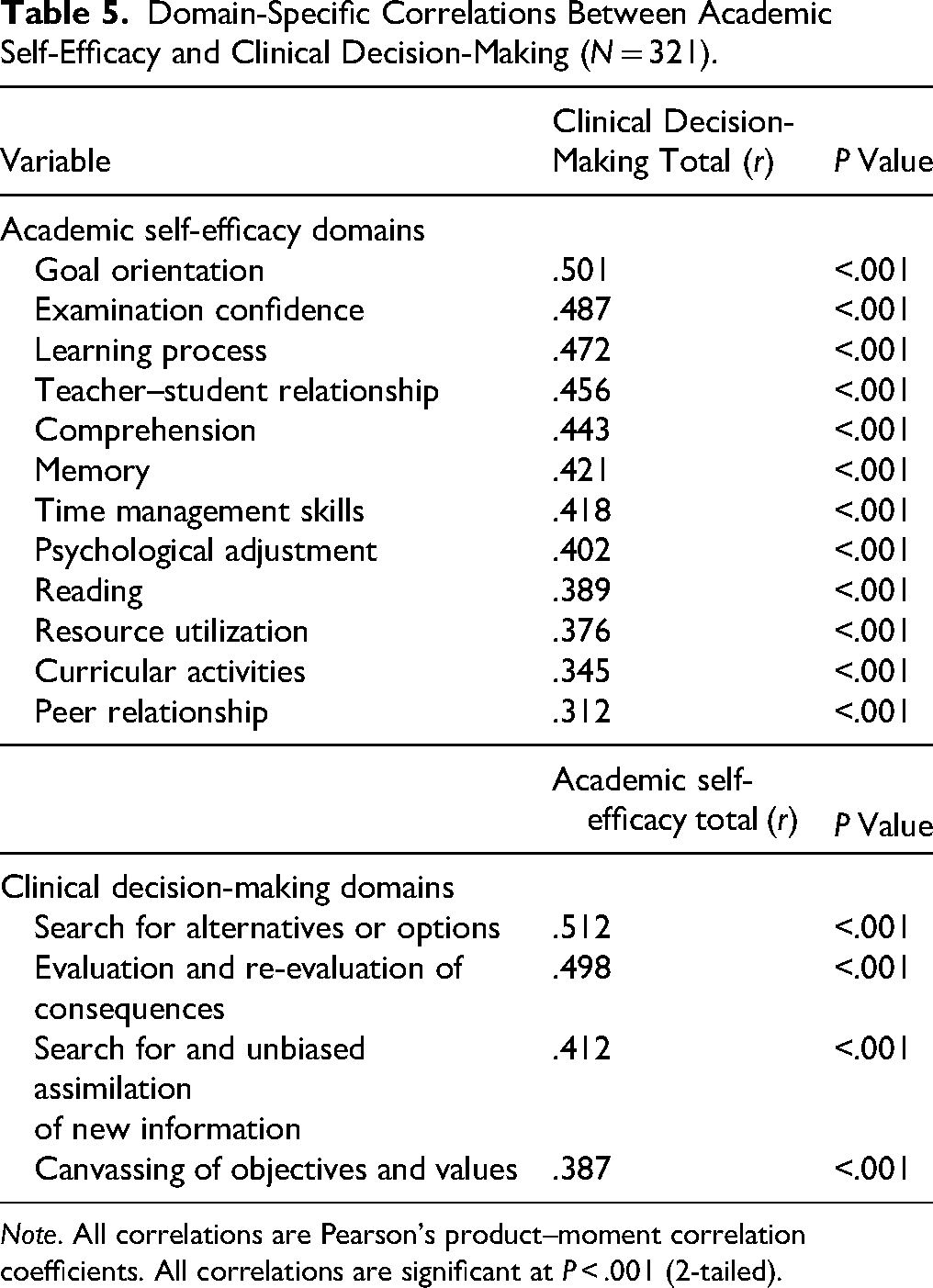
Note. All correlations are Pearson's product–moment correlation coefficients. All correlations are significant at P < .001 (2-tailed).
Regarding clinical decision-making domains, academic self-efficacy correlated most strongly with Search for Alternatives or Options (r = .512, P < .001) and Evaluation and Re-evaluation of Consequences (r = .498, P < .001), and least strongly with Canvassing of Objectives and Values (r = .387, P < .001).
Regression Analysis
Table 6 presents multiple linear regression results addressing Research Question 2. The overall model was statistically significant (F(6, 314) = 42.84, P < .001, R2 = 0.450, adjusted R2 = 0.439), explaining 45.0% of the variance in clinical decision-making abilities.
Variables Associated with Clinical Decision-Making: Multiple Linear Regression.

Note. B = unstandardized coefficient; SE = standard error; Beta = standardized coefficient. Dependent variable: Clinical Decision-Making total score. R2 = 0.450, adjusted R2 = 0.439, F(6, 314) = 42.84, P < .001.
Academic self-efficacy emerged as the strongest variable associated with clinical decision-making (B = 6.566, SE = 0.768, β = 0.389, P < .001), followed by grade point average (B = 7.904, SE = 1.275, β = 0.272, P < .001) and educational support (B = 5.211, SE = 1.396, β = 0.162, P < .001). Age showed a smaller but significant positive effect (B = 1.619, SE = 0.724, β = 0.127, P = .026). Academic year and monthly income were not statistically significant in the final model. The nonsignificance of academic year in the multivariate model, despite significant bivariate correlations, suggests that its effect is mediated through other variables, particularly academic self-efficacy and grade point average, which increase with academic progression.
Figure 2 presents the confirmed empirical model of clinical decision-making correlates among Palestinian nursing students. As shown in Figure 2, academic self-efficacy (β = 0.389, P < .001) emerged as the strongest correlate, followed by grade point average (β = 0.272, P < .001) and educational support (β = 0.162, P < .001). The model collectively explains 45.0% of the variance in clinical decision-making abilities.

Confirmed empirical model of clinical decision-making correlates among Palestinian nursing students (N = 321). Note. Path coefficients represent standardized beta weights from multiple linear regression analysis. ***P < .001, *P < .05. The model explains 45.0% of variance in clinical decision-making.
Discussion
This study provides empirical evidence of a significant association between academic self-efficacy and clinical decision-making among Palestinian nursing students, contributing to nursing education literature from Arab and Middle Eastern contexts. The strong positive correlation (r = .538, P < .001) aligns with Bandura's social cognitive theory, which posits that self-efficacy beliefs influence how individuals approach challenging tasks and make decisions under uncertainty (Bandura, 1997). However, it is critical to emphasize that our cross-sectional, correlational design does not permit causal conclusions about the direction of this relationship. The association may be bidirectional, with successful decision-making experiences enhancing self-efficacy, or may reflect the influence of unmeasured third variables such as critical thinking ability, prior clinical exposure, or personality factors.
From a theoretical perspective, several mechanisms may explain this relationship. First, students with higher academic self-efficacy may be more likely to engage actively in learning opportunities that develop decision-making skills, such as case studies, clinical simulations, and patient care experiences (Pintrich & De Groot, 1990). Second, self-efficacious students may demonstrate greater persistence when facing complex clinical scenarios, potentially leading to more thorough information gathering and analysis, key components of effective decision-making (Zimmerman, 2000). The domain-specific correlations support this interpretation, with the strongest associations observed between self-efficacy and the Search for Alternatives domain (r = .512), which requires persistence in generating and considering multiple solutions. Third, the confidence associated with high self-efficacy may enable students to trust their clinical judgment and act decisively, rather than remaining paralyzed by uncertainty (Lent et al., 1984). Fourth, self-efficacy may influence cognitive processing by reducing anxiety that otherwise impairs working memory and analytical reasoning during complex decision-making tasks (Artino, 2012). Again, these are plausible theoretical pathways consistent with our findings, but they are not proven by this study's design.
The regression model explained 45.0% of variance in clinical decision-making, representing a substantial effect size exceeding that typically reported in similar studies (Brown et al., 2023; Smith et al., 2023). This finding suggests that, in the Palestinian context, psychological and support factors may be particularly important for decision-making development, potentially because resource constraints limit other sources of decision-making skill acquisition, making individual psychological resources more influential.
Cultural and Contextual Analysis
The Palestinian educational context provides a unique vantage point that extends the understanding gained from Western nursing education research. The notably high score in the “Canvassing of objectives and values” domain (mean = 38.0 ± 4.4) may reflect cultural emphasis on collective decision-making, where family and community considerations are integral to healthcare choices. This aligns with foundational Arab cultural principles such as shura (consultation) and collective responsibility (Hammoud et al., 2005). This finding suggests that Palestinian nursing students may possess strong attunement to the ethical and value-based dimensions of clinical reasoning, representing a potential cultural strength that may support holistic and patient-centered care approaches.
However, multiple alternative explanations warrant consideration. The emphasis on values-based decision-making could also reflect: (1) the nursing curriculum's focus on ethical reasoning and professional values; (2) exposure to complex family centered care situations during clinical training that reinforce value considerations; (3) characteristics of students attracted to nursing as a profession in this cultural context; (4) social desirability bias in responding to values-related items; or (5) measurement properties of this domain. The cross-sectional design limits our ability to attribute these findings definitively to cultural factors alone. Longitudinal research tracking how these domain scores evolve throughout nursing education could help distinguish between cultural, curricular, and developmental explanations.
Conversely, the lower score in “Search for and unbiased assimilation of new information” (mean = 31.9 ± 7.2) may reflect challenges in the Palestinian educational environment, including limited access to current medical literature, restricted internet connectivity due to political circumstances, and resource constraints in academic libraries (Giacaman et al., 2009). However, this finding could also reflect: (1) developmental factors, as information-seeking skills typically develop later in nursing education and may require more advanced clinical exposure; (2) the nature of clinical experiences available to students, which may emphasize direct patient care over evidence retrieval; (3) pedagogical approaches that emphasize other competencies; or (4) measurement issues related to how information assimilation is operationalized. The domain-specific correlations show that information assimilation had the weakest relationship with self-efficacy among decision-making domains (r = .412), suggesting that improving this skill may require addressing structural barriers in addition to building student confidence. Further research is needed to disentangle these competing explanations. This finding aligns with broader research on evidence-based practice barriers in low- and middle-income countries, where infrastructure limitations may impede access to current evidence (Pager et al., 2012).
The socioeconomic correlation with decision-making (r = .123, P = .027), while modest, suggests that financial stress may impact cognitive resources available for complex decision-making processes. However, the relatively weak correlation suggests that Palestinian nursing students demonstrate resilience, which could be attributable to strong social support systems and cultural values emphasizing education as a pathway to social mobility (Shuaibi et al., 2013). Alternative explanations for this weak correlation include: (1) restricted range of socioeconomic status in the sample, with most students from moderate-income families; (2) measurement limitations in assessing monthly family income as a single indicator; (3) the possibility that financial stress affects academic performance through other mechanisms not captured; or (4) effective institutional support systems that mitigate socioeconomic disadvantages.
Gender Equivalence in Self-Efficacy and Decision-Making
The absence of significant gender differences in either clinical decision-making (Cohen's d = 0.09) or academic self-efficacy (Cohen's d = 0.11) is noteworthy, and challenges assumptions often held in Western nursing education literature, which commonly reports gender differences in clinical confidence (LaManna et al., 2022). However, the cross-sectional correlational design limits causal interpretation of this finding. This observation may reflect characteristics of the Palestinian context, where nursing attracts both genders for similar reasons and where cultural expectations place equal value on education for all (Al-Hussein et al., 2023). Alternatively, this finding could reflect: (1) sampling characteristics specific to this institution; (2) cohort effects specific to the students studied; (3) statistical power limitations for detecting small gender differences; (4) the possibility that gender differences emerge later in professional practice rather than during education; or (5) the specific instruments used may not capture gendered dimensions of decision-making. Longitudinal research would be needed to determine whether this gender parity persists across the educational trajectory and into professional practice. This gender parity suggests that equitable learning environments may transcend traditional gender role limitations and indicates that Palestinian nursing programs could potentially serve as models for creating gender-inclusive educational settings. Examining the factors underlying this parity in Palestine, such as equitable treatment in clinical placements, similar academic expectations, or cultural value placed on education for all genders, could provide valuable insights for advancing gender equity in nursing education globally.
Academic Performance as an Associated Factor
The strong relationship between grade point average and decision-making (β = 0.272, P < .001) may extend beyond simple academic achievement, potentially reflecting the integration of knowledge, critical thinking skills, and confidence that develops through successful academic experiences. Grade point average may serve as a proxy for multiple competencies relevant to clinical decision-making, including knowledge acquisition, analytical ability, self-discipline, and effective learning strategies. In the Palestinian context, where nursing programs maintain rigorous academic standards despite resource constraints, grade point average may represent an indicator of the comprehensive competencies required for clinical decision-making (Shaban et al., 2012).
The independent contribution of educational support (β = 0.162, P < .001) highlights the importance of social and institutional resources for developing decision-making confidence. This finding resonates with Palestinian cultural values emphasizing collective support for educational achievement and suggests that formal mentorship programs may enhance clinical competence (Awad & Altalli, 2019). Students receiving educational support scored approximately 5 points higher on the Clinical Decision-Making Scale compared to those without support, representing a meaningful difference equivalent to approximately one-third of a standard deviation. This effect size suggests that interventions enhancing educational support could produce clinically meaningful improvements in decision-making abilities.
Synthesis with International Literature
Comparison with similar studies reveals both convergent and divergent findings. The correlation between self-efficacy and decision-making (r = .538) aligns with recent meta-analyses from North American and European contexts reporting pooled correlations of r = .35–.45 (Brown et al., 2023; Smith et al., 2023), suggesting that this relationship may be present across cultural settings. However, the magnitude of this relationship in our study is notably stronger than typically reported in Western samples. Several explanations for this difference warrant consideration: (1) the heightened importance of self-efficacy in resource-constrained educational environments where external supports may be limited, making internal psychological resources more influential; (2) the potential influence of common method variance due to exclusive use of self-report measures, which may inflate correlation coefficients; (3) differences in measurement instruments across studies; (4) cultural factors that may amplify the relationship between confidence and performance; or (5) sampling characteristics specific to this study. Future research using multimethod assessments and cross-cultural designs would help clarify whether these magnitude differences reflect genuine contextual effects or methodological artifacts.
Domain-specific findings reveal divergent patterns when comparing with prior research. While Western studies often report higher scores in information-seeking behaviors (Edwards et al., 2010), Palestinian students scored highest in values-based decision-making. This divergence suggests that cultural context may significantly influence how decision-making competencies develop and are prioritized in nursing education. However, these differences could also stem from curricular variations, clinical exposure differences, or measurement factors. This finding underscores the importance of culturally responsive nursing education research that does not simply assume Western-derived constructs and priorities apply universally.
The absence of gender differences contrasts with recent European studies reporting male nursing students demonstrating higher clinical confidence (MacLellan et al., 2016). However, it aligns with emerging research from other Arab contexts, suggesting that traditional gender role assumptions may not apply uniformly across all cultural settings (Al-Motlaq et al., 2023). This convergence with regional studies strengthens confidence that the finding reflects genuine contextual patterns rather than sampling artifact. These cross-cultural comparisons should be interpreted cautiously given differences in study designs, measurement approaches, and cultural contexts.
Strengths and Limitations
Several limitations should be considered when interpreting these findings.
Methodological Limitations
The cross-sectional design precludes causal inferences about the relationship between academic self-efficacy and decision-making. The correlational nature of the data means that the direction of causality cannot be determined; it is equally plausible that successful decision-making experiences enhance self-efficacy beliefs or that a third variable influences both constructs. Longitudinal studies tracking students across their educational trajectory and intervention studies manipulating self-efficacy would be necessary to establish causality and directionality.
A significant related limitation is the exclusive reliance on self-reported data for both primary variables, which introduces risks of common method variance and social desirability bias. The strong correlations observed, while theoretically plausible, may be partially inflated by these methodological factors. Common method variance can artificially inflate correlations when variables are measured using the same method (Podsakoff et al., 2012). Future research should incorporate multimethod assessments, such as objective clinical evaluations, simulation-based performance measures, observational ratings by clinical instructors, or behavioral assessments, to triangulate findings and reduce method bias.
Sampling Limitations
The convenience sampling method, while achieving high response rates, may limit generalizability to other Palestinian nursing programs or regional contexts. The single-institution design means findings may reflect specific characteristics of this institution's curriculum, faculty, student body, or local context that may not apply elsewhere. Multisite studies across different Palestinian universities and regional nursing programs would enhance the representativeness and generalizability of findings.
The high proportion of male participants (49.2%), while reflective of this specific program and an interesting contextual feature, is atypical for global nursing samples where female students typically constitute 80% to 90% of enrollments. This gender distribution may affect the comparability of findings with studies from regions where nursing is female-dominated. However, this characteristic also represents a strength by allowing meaningful gender comparisons and providing insights into nursing education in contexts with more balanced gender representation.
Measurement Limitations
Measurement limitations include reliance on perceived rather than actual decision-making ability. While self-reported decision-making correlates with objective performance, the relationship is not perfect, and students may overestimate or underestimate their abilities. The Clinical Decision-Making in Nursing Scale measures students’ perceptions of their decision-making processes rather than observed decision-making competence. Future research should include objective measures such as clinical simulation assessments, standardized patient encounters, or instructor ratings to validate self-report findings.
The use of instruments originally developed in Western contexts, despite thorough translation and validation procedures, may not fully capture Palestinian cultural perspectives on decision-making and self-efficacy. Some conceptual elements may have different meanings or importance in this cultural context. The lack of Palestinian-specific normative data for these instruments limits interpretation of absolute scores relative to population benchmarks.
Cultural adaptation limitations involve the use of instruments originally developed in Western contexts, despite thorough translation and validation procedures. Some conceptual elements of decision-making or self-efficacy may not fully capture Palestinian cultural perspectives on these constructs. The lack of Palestinian-specific normative data for these instruments limits interpretation of absolute scores. Future research should consider developing or adapting instruments specifically for Arab cultural contexts.
Contextual Limitations
Contextual limitations include data collection during a single academic year, which may not account for temporal variations in student experiences or broader sociopolitical factors affecting Palestinian higher education. The unique geopolitical situation in Palestine, including movement restrictions, political instability, and economic challenges, may create stressors and constraints that affect students’ educational experiences in ways that limit generalizability to more stable contexts. However, these characteristics also provide valuable insights into nursing education under challenging conditions that may inform practice in other resource-constrained or conflict-affected settings globally.
Statistical Limitations
Statistical limitations include the fact that the explained variance (45.0%), while substantial, indicates that other important factors influencing decision-making remain unexplored. Unmeasured variables such as critical thinking ability, clinical reasoning skills, previous healthcare experience, emotional intelligence, and personality factors may account for the remaining 55% of variance. The cross-sectional design also limits ability to examine developmental trajectories or changes over time.
We also acknowledge that the use of bivariate correlations and multiple regression, while appropriate for our research questions, represents a relatively basic analytical approach. More sophisticated models (e.g., structural equation modeling) could in the future test the theoretical pathways proposed in our discussion and examine mediating or moderating relationships among variables. However, such analyses would require larger samples and theoretical justification for specific path models.
Additionally, the sample size, while adequate for regression analysis with 53 participants per predictor variable, exceeding the recommended minimum of 10–15 per predictor, may have limited statistical power to detect small effects in subgroup analyses. Posthoc power analysis indicated power >0.99 to detect the observed R2 of 0.45 with α = .05, but power was lower (0.62–0.78) for detecting small effects in subgroup comparisons.
Strengths
Strengths of this study include its strong theoretical foundation grounded in Bandura's social cognitive theory, the use of validated instruments with demonstrated reliability in this sample (Cronbach's α > .85), a high response rate (91.7%) minimizing nonresponse bias, rigorous translation and cultural adaptation procedures, confirmatory factor analysis supporting construct validity, and its novel contribution to nursing education literature from an under-researched cultural and geopolitical context. The relatively large sample size (N = 321) provides stable parameter estimates and adequate statistical power for the primary analyses. The inclusion of domain-specific analyses provides nuanced understanding of how different aspects of self-efficacy relate to various decision-making components. The comparison with international literature and attention to cultural context enhance the manuscript's international relevance despite its single-country focus.
Implications for Practice
Based on the associations identified in this study, several educational strategies warrant consideration. However, it is crucial to emphasize that these implications are derived from associative data and require rigorous experimental evaluation before widespread implementation can be confidently recommended.
Curriculum Development
Curricula could be enhanced to address the observed lower scores in information-seeking skills through structured evidence-based practice courses, digital literacy training, and partnerships with international nursing schools for resource sharing. Specifically, educators might consider: (1) integrating literature search skills early in the curriculum with progressive complexity; (2) providing guided practice in evaluating research evidence; (3) creating assignments requiring students to locate and appraise evidence for clinical problems; (4) developing online repositories of open-access resources accessible despite internet limitations; and (5) teaching efficient information-seeking strategies that work within infrastructure constraints.
The high values-based decision-making scores suggest building upon this strength by developing ethical reasoning frameworks that integrate Palestinian cultural values with international nursing ethics standards. Educators could design case studies and ethical dilemmas that explicitly leverage students’ observed strength in values-based reasoning, using it as a foundation to teach and reinforce the more challenging skills of systematic information seeking and evaluation. This strengths-based approach may enhance student engagement and confidence while addressing identified gaps.
Pedagogical Strategies
Given the association between self-efficacy and decision-making observed in this study, simulation-based education programs may be beneficial as they could address both self-efficacy development and decision-making skill acquisition simultaneously. Simulation provides opportunities for mastery experiences (successful performance), vicarious learning (observing peers), and feedback, all sources of self-efficacy identified by Bandura (1997). Given resource constraints, low-cost simulation alternatives such as role-playing scenarios, case-based learning, standardized patients (using trained actors or volunteers), and peer-to-peer mentoring could provide effective alternatives to high-fidelity simulation equipment (Al-Saadi et al., 2023). However, intervention studies are needed to determine the effectiveness of these approaches in the Palestinian context.
Mentorship Programs
The positive association between educational support and decision-making suggests that mentorship program development could formalize the educational support observed in this study. Structured partnerships between senior and junior students, faculty mentoring relationships, and community preceptor programs may address both academic self-efficacy and clinical decision-making development (Chen et al., 2024). These programs could include: (1) regular one-on-one meetings; (2) structured reflection on clinical experiences; (3) guided case discussions; (4) observation and feedback on clinical performance; and (5) career guidance and academic support. Rigorous evaluation of such programs using randomized designs would be essential to determine their effectiveness.
Specific Recommendations for Nurse Educators Working in Resource-Constrained Settings
The recommendations below are suggested as possible strategies based on the study results. As always, educators must adapt these recommendations to their own contexts and assess local effectiveness.
Making use of low-cost pedagogies: Make use of online resources (which are free) including open educational resources (e.g., OpenRN, OER Commons, and nursing education resource from the WHO and Sigma), jigsaw learning or problem-based learning strategies, creative utilization of mobile learning platforms to overcome limited library access. Sample ideas: establish digital archives of case studies and clinical scenarios that can be viewed via mobile devices. So explore offline alternatives like downloadable content, USB packs with learning kits or locally-hosted or on device based learning management system (LMS) that do not need constant internet access. Establish peer-assisted learning programs: Establish formal relationships for students at different years to act as mentors, allowing senior students to assist those in earlier stages of study and vice versa, thereby increasing each party's self-efficacy through vicarious experience later. This method builds on existing student strengths and needs little money to implement. Develop programs with structured goals, time for peer mentors to train, meetings on the calendar, and guided activities. Engender culturally north simulations scenarios: Involve the people in genesis of low-fidelity simulations with locally available material having representative Palestine healthcare settings and ethical dilemmas. This balances respect for cultural values with the need to build decision-making skills. Use students to help coconstruct the scenarios to make them more engaging, culturally authentic. Scenarios should focus on common clinical presentations in local healthcare settings, include family dynamics typical of Palestinian culture and traffic in resource limitations students will face when they practice. Promoting collaborative global health partnerships: Create virtual exchange programs with universities in high-income countries, sharing resources, facilitating joint case discussions, and exposing students to different models of care. These collaborations can also offer access to contemporary evidence, simulated scenarios, and academic expertise while promoting cultural exchange and global perspective development. Virtual exchanges that are structured and designed with clear learning objectives and guided reflection maximize educational benefit. Supposedly adding reflective practice: Where options such as guided journals, reflective portfolios, and debrief sessions double with structured models of reflection like Gibbs’ Reflective Cycle encouraging students to recognize their justification for management decisions made helps build metacognitive awareness; fostering improvements in self-efficacy and clinical judgment without needing extra resources. Faculty development in the facilitation of reflective practice improves the quality of implementation. Developing need-finding capabilities in a systematic basis: Stay committed to the low scores for information assimilation and make information literacy one of the pillars of the curriculum. From basic literature search and decision making for early years, to critical appraisal in the middle years and evidence-based practice projects in final years. Provide faculty training on using topic-specific examples to teach students how to efficiently locate and use pre-appraised evidence sources (e.g., evidence-based clinical guidelines, systematic reviews), since utilization of pre-appraised resources takes less time and resources than searching primary literature. Leverage cultural strengths in values-based decision-making: Recognize and leverage the student's strengths in values-based reasoning. Use this as a foundation to develop other competencies in decision-making. For example, in the development of the student's information-seeking competency, emphasize the role of evidence in values-based care and the student's ability to advocate for the patient's values. Make links between the frameworks used in ethical reasoning and the cultural values of the Palestinian people.
The recommendations provided in this paper illustrate the ingenuity that is possible in the education of nurses in Palestine, despite the resource and political challenges. The ingenuity of the Palestinian nurse educators in the face of adversity, in providing a high standard of education in nursing, is a lesson to the world in the education of nurses in other resource-challenged environments. The principles of leveraging the student's strengths, peer support systems, adapting rather than adopting the “Western model,” and leveraging creativity in the delivery of quality education, rather than relying on the quality of the resources, are principles that transcend the Palestinian context and are applicable in other diverse environments.
Implications for Research
The limitations of the study should be addressed in the future nursing education research in the following ways:
Using longitudinal study designs to examine the developmental trajectory or the causal relationships of the variables over time, which could help to establish whether self-efficacy predicts the development of decision-making or vice versa. Conducting the study in multiple Palestinian universities to increase the generalizability of the findings to other regions in Palestine. Conducting cross-cultural comparative studies to examine the relationships between self-efficacy and decision-making in other cultures using standardized measures to compare the findings with other cultures. Conducting intervention studies to examine the effects of the development of self-efficacy and decision-making in nursing students using randomized control designs to establish causality. Conducting the study using a mix of quantitative methods to examine the relationships between the variables while using qualitative methods to examine the processes that explain the relationships in more depth. Conducting the study using objective measures of decision-making in addition to the self-report measures to validate the findings. Other studies that investigate other variables that can explain the other 55% of the variance, such as critical thinking, emotional intelligence, quality of clinical exposure, personality, and institutional characteristics. Other psychometric studies that focus on the development of measures that are culturally appropriate for the Arab culture.
International collaboration can also help address the issue of resource constraints while at the same time contributing to the advancement of knowledge in the field of nursing education, particularly in underrepresented areas. Research collaboration between Palestine and other international organizations can help ensure that funding, expertise, and publication opportunities can be made available, while at the same time ensuring that the studies remain culturally appropriate.
Conclusions
This study provides evidence of a significant association between academic self-efficacy and clinical decision-making among Palestinian nursing students. The strong correlation (r = .538) and substantial explained variance (45.0%) suggest that fostering students’ confidence in their academic abilities may be related to their capacity for clinical judgment and autonomous practice. However, the cross-sectional correlational design precludes definitive causal conclusions, and longitudinal and intervention research is needed to establish causality and directionality.
The Palestinian context offers insights that extend global understanding of nursing education processes. The emphasis on values-based decision-making reflects potential cultural strengths that may be preserved and built upon, while lower scores in information-seeking skills indicate areas that may benefit from targeted intervention. The absence of gender differences challenges Western assumptions about clinical confidence and suggests that equitable educational environments may transcend traditional gender role limitations. These findings contribute to the growing body of evidence that nursing education research must attend to cultural context rather than assuming Western findings apply universally.
For nursing education practice, these findings suggest potential value in implementing approaches that simultaneously address academic self-efficacy and decision-making skill development. Simulation-based learning, structured mentorship programs, and evidence-based practice training emerge as potentially promising strategies, particularly when adapted to resource-constrained environments common in developing countries. However, it is crucial to note that these implications are derived from associative data; rigorous experimental evaluation of these interventions in the Palestinian context is essential before widespread implementation can be confidently recommended. The specific recommendations for resource-constrained settings provide practical guidance while emphasizing the need for local adaptation and evaluation.
For nursing education theory, this study contributes to understanding how psychological constructs may interact with cultural contexts to influence professional development. The findings suggest that relationships between self-efficacy and decision-making may manifest differently across cultural contexts, potentially requiring culturally responsive pedagogical approaches. Additional research is needed to confirm these patterns and explore underlying mechanisms. The domain-specific findings provide nuanced understanding of which aspects of self-efficacy most strongly relate to decision-making, informing more targeted theoretical models.
Nursing education globally faces the challenge of preparing competent practitioners in diverse contexts with varying resources. This study from Palestine demonstrates that meaningful research can emerge from underrepresented regions and contribute valuable insights to the international community. By attending to both universal psychological processes and culturally specific manifestations, nursing education scholarship can become truly global in perspective while remaining locally relevant in application.
Supplemental Material
sj-doc-1-son-10.1177_23779608261444447 - Supplemental material for Academic Self-Efficacy as a Predictor of Clinical Decision-Making Among Nursing Students: A Cross-Sectional Correlational Study Conducted in Palestine
Supplemental material, sj-doc-1-son-10.1177_23779608261444447 for Academic Self-Efficacy as a Predictor of Clinical Decision-Making Among Nursing Students: A Cross-Sectional Correlational Study Conducted in Palestine by Dalia Toqan, Ahmad Ayed, Ibrahim Aqtam, Lobna Harazne, Moath Abu Ejheisheh, Mohammad Bani Younis, Enaam Al-Ananbeh, Othman A. Alfuqaha, Ahmad Batran and Mustafa Shouli in SAGE Open Nursing
Footnotes
Acknowledgments
The authors express their gratitude to the nursing students at Arab American University who participated in this study. Special thanks to the faculty and administrative staff who facilitated the data collection process.
Ethical Considerations and Consent to Participate
This study was approved by the Institutional Review Board (IRB) of Arab American University, Palestine (Ref. No. J-2025/A/16/N). All research procedures adhered to the Declaration of Helsinki and relevant ethical guidelines for research involving human subjects. Written informed consent was obtained from all participants prior to participation. Participants were informed of their voluntary participation, anonymity, and right to withdraw at any stage without repercussions. No personally identifiable information was collected.
Author Contributions
All authors reviewed, edited, and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.