
Abstract
Introduction
Stroke affects patients’ physical, psychological, and social well-being, with many survivors suffering anxiety, depression, and a decline in quality of life (QOL). These problems remain underexplored among Middle Eastern populations.
Objectives
This study aimed to assess levels of stroke-related anxiety, depression, and QOL, as well as to determine their associated factors and predictors among Iraqi patients with stroke.
Methods
A cross-sectional descriptive correlational design was used, employing the Stroke-Specific Quality of Life (SS-QOL) scale and Hospital Anxiety and Depression Scale on 200 Iraqi stroke survivors.
Results
The sample consisted of middle-aged and older adults, with a mean age of 58.3 years and 42% of participants aged 65 or above; 52.5% were male. Clinically significant levels of anxiety and depression were reported, with a mean score of 12.2 (SD = 3.4) for anxiety, and 11.46 (SD = 3.45) for depression. Higher risk was observed in older, unmarried, unemployed patients and those in early or intermediate stages since stroke onset. Levels of QOL poorly declined poststroke and were below the theoretical mid-range levels of SS-QOL, with mean SS-QOL = 82.6 (SD = 30.2; range = 49–129). Predictor variables of poor QOL included advanced age (B = −0.647, p < .001), unmarried status (B = −5.85, p < .01), hypertension (B = −4.73, p < .05), early post-stroke stage vs chronic (B = −19.8, p < .001), intermediate vs chronic stage (B = −11.3, p < .001), and clinically significant levels of anxiety (B = −6.61, p < .01) and depression (B = −23.6, p < .001). Together, these predictors explained 87% of the variance in QOL (adjusted R2 = .874, F(18,181) = 77.5, p < .001). Severe depression emerged as the strongest predictor, accounting for 31% of variance (t(181) = −23.6, p < .001; sr2 = .310).
Conclusions
Iraqi stroke survivors experience severe levels of anxiety and depression, consistent with poor QOL, and are influenced by socio-demographic and clinical factors. Early assessment and targeted management of high-risk groups by healthcare providers should be considered with the objective of optimizing recovery and rehabilitation. Depression is of great clinical importance due to its significant impact on QOL.
Introduction
Stroke is a major health threat in the world and the second leading cause of death, responsible for about 11% of global deaths. It is also a significant contributor to long-term physical disability and the second most common cause of cognitive decline and dementia (World Health Organization [WHO], 2020). Advances in medical care have increased survival rates and lowered stroke-related mortality in high-income countries. In contrast, Low- and middle-income countries have experienced rising stroke-related deaths, and now carry the heaviest burden, accounting for over 85% of global stroke fatalities (GBD 2021 Forecasting Collaborators, 2024; WHO, 2020). Disability-adjusted life years, which include both years of life lost and years lived with disability, are nearly seven times higher in these regions compared with high-income countries. In many of these countries, reliable data on stroke risk factors are scarce, making prevention and management more challenging (Feigin, 2007; Feigin et al., 2022).
Review of Literature
The prevalence of stroke is higher in the Middle East (WHO, 2020). In Iraq, stroke is an increasing public health concern, with both incidence and disability rates rising each year. The Global Burden of Disease Stroke Collaborators reported an incidence of 196.2–218.3 per 100,000 people in 2019 (Feigin et al., 2022). Stroke is the second leading cause of deaths in Iraq with 53 deaths per 100,000 population (WHO, 2020). This increase is mainly due to common risk factors, such as hypertension, smoking, and diabetes (Abd, 2019; Feigin et al., 2022). Stroke care is still limited, with few centers able to offer advanced stroke treatment, such as mechanical thrombectomy. Consequently, many stroke survivors experience some delays in the treatment, complicating their outcomes and placing extra pressure on health services (AL-Fayyadh, 2017; Alshalchy et al., 2024). Geographic and logistical barriers and continued security issues are additional barriers to access stroke care within the 6-hour period for the already limited specialized care centers, reducing the opportunity for life-saving interventions. Consequently, mortality and long-term disability rates are high (Abd, 2019; Alshalchy et al., 2024; GBD 2019 Stroke Collaborators, 2021).
Various clinical symptoms are common in stroke survivors, such as paralysis, disturbed balance, motor defects, speech problems, vision problems, and bowel/bladder dysfunctions (Dąbrowska-Bender et al., 2017; Lo Buono et al., 2017). Moreover, stroke can be related to depression, anxiety, and changes in personality (Abuadas et al., 2023; Ayasrah et al., 2018, 2022, 2024). Some of the most prevalent psychological complications after stroke are poststroke depression and anxiety that adversely impact recovery, functional outcomes, and overall quality of life (QOL) (Abuadas et al., 2023; Ayasrah et al., 2018, 2022, 2024). These conditions are often most pronounced in the first few months after an initial stroke.
Women, younger patients, unemployed, smokers, patients with severe strokes, and those with comorbid depression are more likely to report poststroke anxiety (Abuadas et al., 2023; Ayasrah et al., 2018, 2022). In contrast, poststroke depression has been associated with lower education levels, chronic diseases, smoking, dependence in performing activities of daily living (ADLs), and speech impairment (Abuadas et al., 2023; Ayasrah et al., 2018, 2022). Such psychological impairments are often underestimated by healthcare providers who paid more attention to physical disabilities caused by stroke, although many patients have clinically significant levels that make the recovery process more complicated (Abuadas et al., 2023; Ayasrah et al., 2018, 2022, 2024). Early screening and timely referral to psychiatric care, especially for patients with severe symptoms, can enhance psychological well-being and recovery outcomes (AL-Fayyadh, 2019; Ayasrah et al., 2022).
Recent studies have focused on the enhancement of QOL, especially in chronic diseases, where it is viewed as a primary indicator of the effect of the disease on the overall well-being of the patients (Ayasrah et al., 2024; Lourenço et al., 2021). Improving QOL is among the primary goals of stroke rehabilitation, and it involves continuous monitoring of QOL indices and treatment outcomes in terms of physical, psychological, cognitive, and occupational functioning (Ojo Owolabi, 2011; Williams, Weinberger, Harris, Clark, et al., 1999). The measurement of QOL in such a population, however, is complicated by the high variability of stroke symptoms and their related psychological and social effects (Williams, Weinberger, Harris, and Biller, 1999). Although both generic and stroke-specific instruments are employed, stroke-specific measures of quality of life (SS-QOL) are typically desirable, as they are more likely to reflect the multidimensional challenges faced by stroke survivors (Jarosławski et al., 2020; Tsalta-Mladenov & Andonova, 2021; Williams, Weinberger, Harris, and Biller, 1999).
Poststroke, QOL is usually decreased, and this is related to many socio-demographic factors, including old age, female sex, being single, low gross monthly income (GMI), and undergoing the initial recovery stages after a stroke (Ayasrah et al., 2024; Chen et al., 2019; Tsalta-Mladenov & Andonova, 2021). The role of psychological impairments (mostly anxiety and depression) and a lack of family or social support are also important (Ahmed et al., 2020; Alshahrani, 2020; Ayasrah et al., 2024). Furthermore, accessibility and availability of healthcare services are also significantly different among the communities that directly influence the severity of stroke and its impact on QOL (AL-Fayyadh, 2017; Alshalchy et al., 2024; Chen et al., 2019). These factors are important to identify the high-risk groups and inform clinical decision-making (Alshalchy et al., 2024; Ayis et al., 2015).
In developing countries like Iraq, the healthcare system is limited by conflicts, political instability, and lack of resources. These obstacles lead to limited access to timely and sufficient care; thus, it is difficult to improve the QOL of stroke (Ahmed et al., 2020; Alshalchy et al., 2024). Moreover, culture and social issues also influence patients' perceptions of QOL after stroke (Ayasrah et al., 2024; Basheti et al., 2019; Omu & Reynolds, 2013). Nevertheless, there is still a significant research deficit concerning stroke-related anxiety, depression and QOL in the Middle East, particularly in Arabic cultural contexts such as Iraq. It is necessary to assess anxiety, depression, and QOL together since these issues are interrelated, and their interaction can be used to guide specific interventions to enhance post-stroke outcomes. To our knowledge, no studies have yet examined psychological impairments such as anxiety and depression, and QOL among patients with stroke in Iraq, leaving their experiences inadequately understood. This study, therefore, aims to: (1) Assess levels of stroke-related anxiety, depression and QOL; (2) Determine factors associated with stroke-related anxiety and depression and determine predictor variables of QOL, among Iraqi patients with stroke.
Materials and Methods
Design
This study used a cross-sectional correlational design. Patients with stroke were recruited from eight hospitals located in Baghdad, the capital governorate of Iraq, and Al-Mothanna governorate in the south. Participants were identified in medical wards, neurology outpatient clinics, and physiotherapy centers between November 2024 and April 2025.
Research Questions
This study addressed the following research question:
What are the levels of stroke-related anxiety among Iraqi patients with stroke? What are the levels of stroke-related depression among Iraqi patients with stroke? What factors are associated with stroke-related anxiety and depression among Iraqi patients with stroke? What are the levels of QOL among Iraqi patients with stroke? What are the predictors of QOL among Iraqi patients with stroke?
Sample
The head nurses and lead physiotherapists reviewed medical records to determine eligibility and referred potential participants. Individuals approached in patient rooms or waiting areas were given a detailed description of the study and offered informed consent if they were willing to participate. Data was collected directly from patients using a self-report tool, which could not be completed by proxy. Figure 1 shows a flow diagram of patient recruitment and inclusion criteria.

Flow diagram of patient recruitment, exclusion, and final sample size.
Inclusion/Exclusion Criteria
Eligibility criteria included: (1) having Iraqi nationality; (2) aged 18 years or older; (3) have had their first ischemic or hemorrhagic stroke within at least 1 month of the date of interview; (4) mild to moderate functional impairments determined by the rehabilitation healthcare providers; (5) ability to understand and speak Arabic; and (6) providing an informed consent (verbal with witness or written). Patients with moderate aphasia (dysphasia) were eligible to participate according to confirmations from their attending clinicians. Exclusion criteria included major cognitive or verbal impairments (e.g., dementia or severe aphasia) due to concerns about response accuracy and reliance on caregivers. Patients were also excluded if they had a history of drug abuse, depression, and/or anxiety disorders prior to the stroke event based on their medical records, dependency in performing ADLs, or comorbidities likely to adversely affect QOL, such as advanced cancer or chronic renal failure. Patients with a history of recurrent stroke were excluded to minimize the confounding effect of previous experience of stroke events. Patients with a transient ischemic attack were also excluded because of the transient nature of their symptoms that did not usually lead to permanent psychological and/or functional impairments, nor did they affect their QOL.
The sample size was calculated using G*Power 3.1.9.4 software. A multiple linear regression model with a fixed design was used, assuming a medium effect size of 0.15, a significance level (α) of 0.05, and 16 predictors based on previous research (Ayasrah et al., 2024). These parameters indicated that, to achieve adequate statistical power, a minimum sample of 143 participants was needed. A total of 200 patients with stroke were recruited to account for potential attrition and allow for group comparisons.
Ethical approval was obtained from the Institutional Review Board committees of the selected hospitals. To ensure confidentiality, each participant was assigned a unique identification code. After obtaining informed consent from the patients, two of the study researchers collected clinical data using medical records and conducted face-to-face structured interviews. The interviews with inpatients were conducted in their rooms while patients recruited from outpatient clinics and physiotherapy centers were interviewed in separate rooms set up for the purpose of conducting the study. The interviews were carried out in 15–30 min depending on the level of comfort for the patient.
Data was collected by a structured questionnaire with three sections. The first part included 21 items concerning socio-demographic characteristics (e.g., age and employment status) and medical information (e.g., previous illnesses, type of stroke and time since stroke onset). These variables were selected according to the findings from the previous studies (Ahmed et al., 2020; Alshahrani, 2020; Ayasrah et al., 2024; Chen et al., 2019; Tsalta-Mladenov & Andonova, 2021). The second section used the Hospital Anxiety and Depression Scale (HADS) to assess emotional health (including symptoms of anxiety and depression). Developed by Zigmond and Snaith in (1983), and intended for use in non-psychiatric hospital environments, the HADS includes 14 items, equally split into two subscales: anxiety (HAS) and depression (HDS). Each item is scored on a four-point Likert scale from 0 to 3 to yield subscale scores from 0 to 21. There are three categories: “Scores of 0–7 suggest normal levels, 8–10 suggest borderline abnormalities, and 11–21 suggest clinically significant levels of anxiety or depression, representing a probable case” (Zigmond & Snaith, 1983). The final section of the questionnaire was the validated Arabic version of the SS-QOL (Sallam et al., 2019).
The SS-QOL is a standardized self-report instrument developed by Williams, Weinberger, Harris, and Biller (1999) to assess health-related QOL in stroke patients. It specifically targets stroke-related impairments and includes 49 items grouped into 12 domains, presented in two parts. The first part focuses on physical and functional aspects, assessing the level of difficulty experienced in six domains: “self-care, vision, language, mobility, work/productivity, and upper-extremity function”. Responses are rated on a five-point Likert scale ranging from “couldn’t do it at all” to “no trouble at all”. The second part addresses emotional, cognitive, and social aspects through the remaining six domains: “thinking, personality, mood, energy, family roles, and social roles”. These items are rated on a five-point Guttman-type scale, from “strongly agree” to “strongly disagree” (Williams, Weinberger, Harris, and Biller, 1999).
Higher scores on both parts of the SS-QOL suggest better perceived QOL. Domain scores can be calculated by taking the average response to items in each domain. To obtain a total score of SS-QOL, it is necessary to average or sum all the scores of the items to obtain a possible score range of 49 to 245. The SS-QOL has been translated and validated in several languages and cultures. Its psychometric properties show satisfactory evidence of acceptable internal consistency (Cronbach's α ≥ 0.73) and good construct validity, where correlations range from 0.71 to 0.92. The scale is also positively related to general QOL scales, like WHOQOL-BREF and SF 36 (Odetunde et al., 2017; Williams, Weinberger, Harris, and Biller, 1999). Good to high internal consistency (Cronbach's a = 0.78–0.94) and moderate construct validity (r = 0.06–0.55) for the Arabic version are also evident (Sallam et al., 2019).
Statistical Analysis
Descriptive statistics were used to present sample characteristics and medical data. Frequencies and percentages were used to summarize categorical variables, while means, standard deviations (SD), and interquartile ranges (IQR) were used to report continuous variables. Group differences were evaluated by independent t-tests, one way analysis of variance or by chi-square tests, based on appropriate statistical assumptions. To determine correlation, Pearson's correlation was employed for continuous variables and biserial correlation (Pr) for dichotomous variables. Hierarchical regression was used to identify predictors of QOL level, which was measured using SS-QOL scores. Data was screened to ensure that statistical assumptions were met. The variance inflated factor (VIF) was calculated to assess the existence of multicollinearity. The range was (1.1–3.0), and therefore the threshold was acceptable. Categorical predictors having more than two categories were recoded to binary variables and one of these was chosen to be the reference. Data analysis was conducted using IBM Statistics software, version 21.
Result
Sample Characteristics
A total sample of 200 patients with stroke participated in the study. The mean age was 58.3 years (SD = 11.95), ranging from 30 to 84 years, with 42% aged 65 or older. Of the participants, 52.5% were male, and 65.5% were married. Most lived in urban areas (60%) and resided with their families (83%). More than half (57%) were unemployed. The mean family GMI was 529,163 Iraqi Dinar (approximately $400), and 54.5% reported their income as insufficient. Regarding education, 62.5% had not completed secondary school, having only elementary or preparatory education. Smoking was reported by 30%, and 35.5% had a history of surgery. The majority had comorbid conditions, including hypertension (79.5%) and diabetes mellitus (53%). Hemorrhagic stroke was identified in 59.5% of participants, and 50% were in the early stage following stroke onset. Table 1 presents the sample demographics and clinical data.
Characteristics of the Study Participants (N = 200).

Abbreviations: M (SD): Mean (Standard Deviation); BSc: Bachelor's degree;*: Undergraduate education level; ID: Iraqi Dinar; DM: Diabetes mellitus, HTN: Hypertension; HD: Heart diseases.
Levels and Associated Factors of Stroke-Related Anxiety and Depression
Participants reported elevated levels of anxiety and depression, indicating severe psychological impairments. For anxiety, the mean HAS score was 12.2 (SD = 3.4), classifying participants as probable cases. Depression scores were similarly high, with a mean HDS of 11.5 (SD = 3.5), also indicating probable cases. Age was significantly associated with both psychological impairments. Advanced age correlated moderately with higher anxiety scores (r = 0.378, p < 0.001) and depression scores (r = 0.477, p < 0.001). Older participants were more likely to be classified as severe cases of anxiety (Pr = 0.521, p < 0.001) and depression (Pr = 0.672, p < 0.001), suggesting that advanced age is a strong associated factor of psychological impairments.
Psychological impairments were also determined by marital status. Welch's analysis of variance (ANOVA) showed that there were significant differences between the marital groups with respect to the mean scores HAS and the mean scores HDS (F'(2, 21) = 6.2, p < 0.01; F'(2, 23) = 18.8, p < 0.001, respectively). Post-game Howell tests showed that the divorced/widowed group had higher level of anxiety compared to the married group (MD = 1.30, p = 0.016, 95% CI [0.20–2.40]); but there were no statistically significant differences between the singles group and the other two marital groups. In terms of depression, the post-game Howell tests showed that the singles group scored higher in depression compared to both the married group (MD = 5.92, p < .001, 95% CI [3.3–8.5]) and the divorced/widower group (MD = 5.17, p = .001, 95% CI [2.5–7.8]). There was no significant difference in depression scores between the married and divorced/widowed groups.
Stroke stage based on onsets was also associated with psychological impairments. For anxiety, Welch's ANOVA—used due to heterogeneity of variances (Levene's test, p < .05) —showed significant differences across stages (F′(2,110) = 14.3, p < .001). Post hoc Games–Howell tests indicated that early-stage patients had higher anxiety scores than late-stage patients (MD = 2.98, p < .001, 95% CI [1.65–4.30]), while no difference was found between early and intermediate-stages. Patients in intermediate-stages also had higher anxiety than late-stage patients (MD = 2.01, p < .01, 95% CI [0.64–3.39]). For depression, one-way ANOVA revealed significant differences in HDS scores across stages (F(2,197) = 18.89, p < .001). Post hoc Scheffé tests indicated that early-stage patients had higher depression scores than both intermediate (MD = 1.87, p < .01, 95% CI [0.41–3.32]) and late-stage patients (MD = 3.14, p < .001, 95% CI [1.85–4.43]), with no significant differences between intermediate and late groups. Other variables, such as gender and type of stroke, were not significant correlates. Table 2 presents crosstabulations of anxiety and depression classifications with selected demographic and clinical variables, along with correlation coefficients for variables that violated chi-square assumptions. These variables were selected based on previous literature.
Post-Stroke Anxiety and Depression Based on Demographics and Clinical Data.
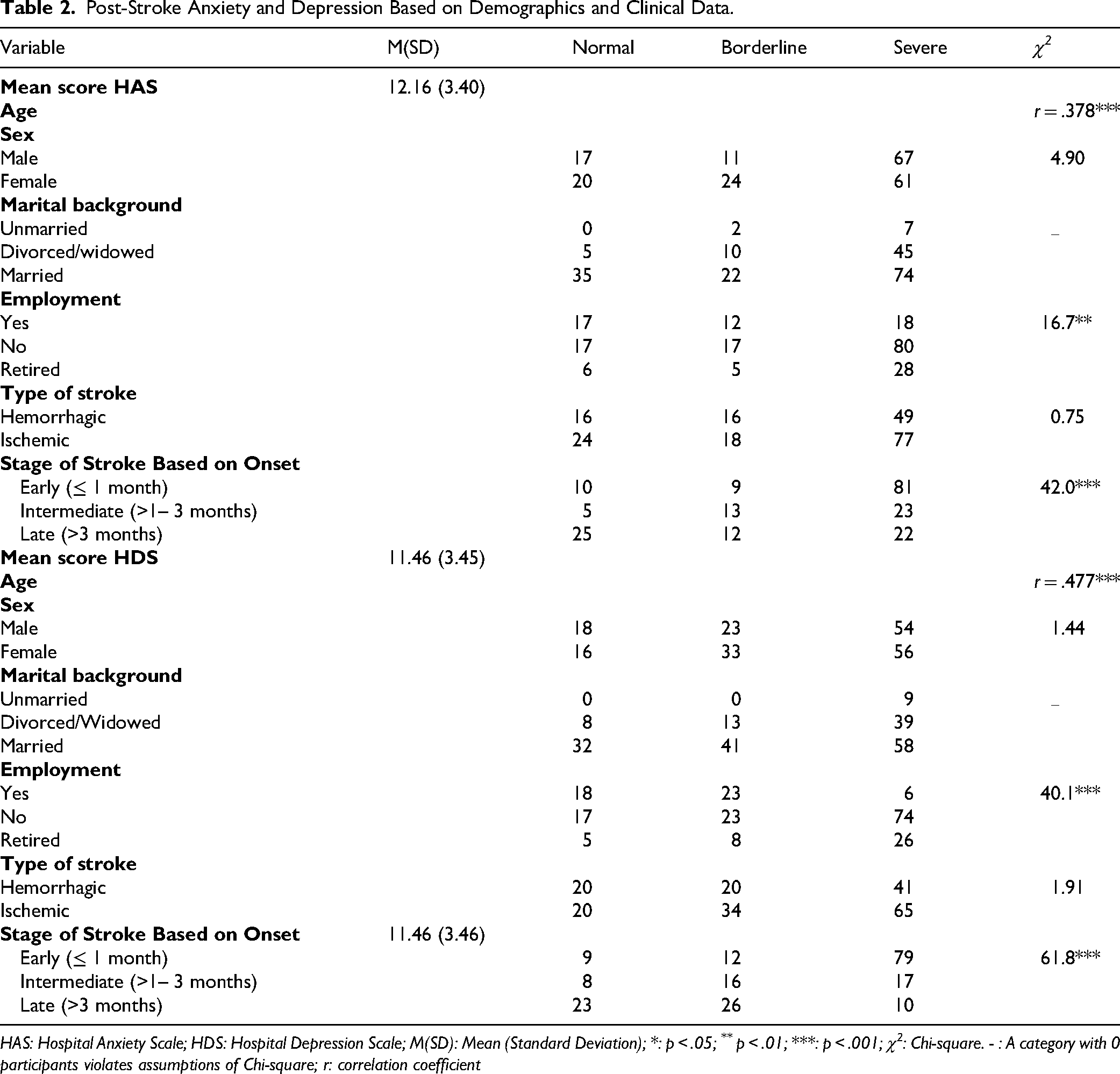
HAS: Hospital Anxiety Scale; HDS: Hospital Depression Scale; M(SD): Mean (Standard Deviation); *: p < .05; ** p < .01; ***: p < .001; χ2: Chi-square. - : A category with 0 participants violates assumptions of Chi-square; r: correlation coefficient
Levels and Predictors of Quality of Life
The total SS-QOL summary score, based on 49 items, indicated poor functioning, with a mean of 82.6 (SD = 30.2; range = 49–129, theoretical range from 49–245). No significant differences were detected in total SS-QOL scores based on sex (t(198) = –1.51, p = .133). However, stroke stage was significantly associated with QOL (F(2, 197) = 143.2, p < .001). Scheffé post hoc tests revealed that patients in the early stage of stroke had significantly lower SS-QOL scores than those in the intermediate stage (MD = –30.4, p < .001, 95% CI [–39.3 to −21.5]) and late stage (MD = –52.8, p < .001, 95% CI [–60.6 to −45.0]). Additionally, patients in the intermediate stage had significantly lower scores than those in the late stage (MD = –22.4, p < .001, 95% CI [–32.1 to −12.7]). Overall, patients in the early stage exhibited the poorest QOL. Age was significantly associated with QOL, with advanced age demonstrated a strong correlation with lower scores (r = –0.778, p < 0.001).
All 12 SS-QOL domains had observed mean scores below the theoretical mid-range, indicating that participants generally reported lower QOL across all areas. Among the domains, mobility and language had the highest mean scores —approximately 9.6 and 9.4, respectively—yet these values remain below the theoretical mid-range. In contrast, energy had the lowest mean score at 4.55, suggesting it is one of the most affected aspects for participants. Figure 2 illustrates the distribution of scores across the 12 domains, showing poor functioning in most areas.

Scores across the 12 SS-QOL domains.
A two-step hierarchical regression analysis was conducted to predict QOL levels based on demographic and clinical variables. In the first step, demographic variables identified from previous studies were entered. The rationale for this order was that non-stroke–related factors were considered first. The regression model including the 10 selected demographic variables was statistically significant, explaining approximately 64% of the variance in QOL scores (R = 0.814, R2 = 0.664, adjusted R2 = 0.644; F(10, 189) = 37.0, p < .001). The contributions of individual predictors were assessed using the t ratios for the regression coefficients. Among the 10 variables, age (t(189) = –12.5, p < .001) and employment status (t(189) = 3.7, p < .001) were significant predictors of QOL, whereas the remaining variables were not statistically significant. Both age and employment status were meaningfully associated with QOL. Older age was linked to lower QOL scores, as reflected by the negative slope. In contrast, being employed was associated with higher QOL levels. Among all predictors in the model, age was the strongest predictor, uniquely explaining 45% of the variance in QOL scores (sr2 = .453).
After controlling for socio-demographic variables, the addition of clinical characteristics increased the explained variance in QOL to 87% (adjusted R2 = 0.874, F(18, 181) = 77.5, p < .001). The change from Model I to Model II was significant (ΔR2 = 0.223, F(8, 10) = 44.0, p < .001). In Model II, age, marital background, place of residence, history of hypertension, stroke stage, and severe anxiety or depression reaching the probable case threshold were significant predictors of QOL. Stroke stage was included as two dummy variables—early and intermediate—with the late stage serving as the reference group. Positive coefficients for marital status and residence indicated that being married or living in an urban area predicted higher QOL. Negative coefficients for age (advanced age), hypertension, early or intermediate stroke, and severe anxiety or depression indicated lower QOL. Other predictors were not significant when controlling for the remaining variables. Overall, this set of predictors explained a large proportion of the variation in QOL, with severe depression emerging as the strongest predictor, accounting for approximately 31% of the variance (t(181) = –23.6, p < .001; sr2 = 0.310). Table 3 presents a summary of the regression results.
Multiple Hierarchical Regression of Quality of Life Levels on Demographics and Clinical Characteristics (N = 200).

Description of abbreviations: B: regression coefficient; Partial (sr2): the squared semipartial correlation coefficient (the distinctive proportion of the dependent variable (quality of life levels) explained by the certain independent variable. * p < .05; ** p ≤ .01; *** p ≤ .001.
Discussion
This study indicates that stroke has a significant influence on the socio-demographic and psychological health of patients in Iraq. A stroke-specific QOL measure was employed, which is consistent with previous studies indicating that these measures are more sensitive to the presence of multidimensional impairments experienced by the stroke survivor compared to generic measures, and can better inform rehabilitation and clinical decisions (Tsalta-Mladenov & Andonova, 2021; Williams, Weinberger, Harris, and Biller, 1999).
The sample consisted mainly of middle-aged and older adults, which is representative of the age groups that are usually affected by stroke. The age of the participants is also one of the established risk factors of stroke which might explain the increased percentage of older participants. The risk of stroke increases twice every decade after age 55, with the majority of incidents occurring among those aged 65 years and above. This age distribution could also have an impact on poststroke recovery and QOL, since in many cases older adults are prone to functional impairment. As the population grows, the number of strokes is likely to increase, posing major challenges to health care systems and policymakers (Yousufuddin & Young, 2019).
Socioeconomic difficulties were also observed, with the average family income being quite low (approximately 400$ per month) and over half of the participants finding their income to be inadequate. The level of education was also low with about two-thirds not finishing secondary school. Conversely, the social support level was relatively high, as approximately two-thirds of participants were married and about 80 percent of them resided with their families.
The psychological impairments were also noteworthy, as the majority of participants reported clinically significant levels of anxiety and depression. Both disorders were more severe during the early stage of stroke probably because of the psychological impact of the sudden loss of functions, uncertainty, and disruption of the lifestyle. Although these impairments are significant, healthcare providers often underestimate them and pay more attention to physical rehabilitation. However, stroke-related anxiety and depression are commonly known to worsen functional outcomes and restrict recovery, and this could be the reason why they are highly associated with poorer QOL in this study. We find that the results of this study are align with prior studies conducted in the Arabian contexts (Abuadas et al., 2023; Ayasrah et al., 2018, 2022, 2024), but the level of psychological impairments in the current study was even higher, which highlights the necessity of introducing mental health assistance into stroke management. Specifically, depression was the most significant predictor of low QOL, which supports its importance as an intervention priority.
The results show a significant decrease in the QOL for all domains of SS-QOL. Participants reported significant restrictions on physical and emotional well-being, social roles, and self-care activities. These results highlight the importance of continued rehabilitation and specific interventions that targeted physical and psychological impairments of stroke. The findings are consistent with research in Arabian contexts, including studies on Saudi Arabian stroke patients (Alshahrani, 2020; Ayasrah et al., 2024), and align with international evidence from Western and Asian populations, which also demonstrate substantial declines in QOL poststroke (Chen et al., 2019; Jarosławski et al., 2020; Lourenço et al., 2021).
The energy domain was the least averaged with fatigue and loss of vitality being two of the major challenges. The previous literature indicates that the symptoms of fatigue might be mixed with the symptoms of mood disorders, such as anxiety and depression in the patient who has a minor stroke, and fatigue is usually considered a symptom of mood disorders; yet, to prevent the overlap, fatigue and mood disorders must be assessed independently (Vitturi et al., 2021). This underscores the need to refer patients who are classified as having anxiety and/or depression, particularly those with severe levels, to a psychologist so that additional assessment and diagnosis can be made.
The levels of QOL reported by the study participants were even lower than previously reported, indicating the severity of poststroke impairments in this group. This can be relatively attributed to the lack of adequate stroke care services in Iraq, which greatly influences the severity of stroke and the outcomes of patients. Place of residence was found to be an important predictor of QOL with rural patients (who may have limited local services and access to specialized care) reporting lower levels of QOL than urban patients, which is in line with the previous studies (Jarosławski et al., 2020). It is, however, remarkable that patients living both in rural and urban areas exhibited overall lowered QOL compared with results from other areas reported in previous literature. There is also limited chance to receive advanced interventions such as mechanical thrombectomy that is available in very limited centers in Iraq. Thus, patients face the problem of delayed access to urgent treatment, which frequently exceeds the 6-hour therapeutic window, and leads to worse health outcomes (Alshalchy et al., 2024). Although progress has been made in stroke management all over the world, Iraq is still fighting with the absence of specialized stroke facilities, inadequate health infrastructure, and persistent security issues, all of which deny many patients timely and effective care.
Having a history of hypertension was identified in this study as a significant predictor of stroke burden, which further highlights its importance in determining the outcomes of stroke. Hypertension has also been reported as one of the key risk factors of stroke globally, which underpins its significance as a modifiable risk factor of stroke incidence and recovery, particularly the hemorrhagic ones. Ischemic stroke predominates in the world as compared to hemorrhagic stroke; however, the increased prevalence of hemorrhagic stroke in this study sample might be linked to regional differences in risk factor management, particularly hypertension which is also a prevalent risk factor of stroke in Iraq. Moreover, it might be attributed to the cross-sectional and hospital-based design of the current study, which is more likely to present more severe forms of strokes, including hemorrhagic ones. The results of the study indicate the extreme necessity of the specific prevention and management interventions in the Iraqi healthcare system (Abd, 2019; AL-Fayyadh, 2019).
The findings of this study showed no differences in stroke-related anxiety and depression or overall QOL according to sex. The result is consistent with Jarosławski et al. (2020), who found no correlation between sex and anxiety or QOL among patients with stroke in various contexts, and with Ayasrah et al. (2018), who found no significant differences in poststroke depression based on sex (Ayasrah et al., 2018; Jarosławski et al., 2020). Nevertheless, the findings of this study are contrary to those by Alshahrani (2020), Ayasrah et al. (2022), and Ayasrah et al. (2024), who have found that there are significant sex-based differences in anxiety and QOL among stroke patients. These studies show that female stroke survivors are at increased risk to experience higher level of anxiety and lower QOL (Alshahrani, 2020; Ayasrah et al., 2022, 2024).
In line with previous research, marital status was also an important related variable with anxiety and depression and a predictor of QOL, with married individuals reporting better overall outcomes (Alshahrani, 2020; Chen et al., 2019). It is noteworthy that all participants who were singles, coupled with over three-quarters of them, expressed clinically significant levels of depression and anxiety, sufficient to be classified as probable cases. These study findings confirm previous literature, which indicates that social support is an important part of recovery and rehabilitation poststroke, and it has a direct impact on psychological well-being and overall QOL (Alshahrani, 2020; Chen et al., 2019).
Older participants were more likely to report lower QOL and higher rates of stroke-related anxiety and depression, which is linked to the increased burden of comorbid conditions and reduced functioning with age (Ayasrah et al., 2024; Chen et al., 2019; Tsalta-Mladenov & Andonova, 2021). In contrast, employed status was associated with increased QOL and lower anxiety and depression, most likely due to the financial stability and social interaction that employment may provide. The most significant socio-demographic factor analyzed was age, and its influence on the outcome and recovery following stroke is remarkable. Furthermore, age-related alterations together with stroke-related impairments also restrain daily functioning and raise the risk of psychological distress, and this is also lowering QOL (Chen et al., 2019; National Institute of Neurological Disorders and Stroke [NINDS], 2025).
The findings of this study support other studies reporting the correlation between time since the onset of a stroke and stroke-related anxiety and depression and QOL, and that timely detection and management are important in maximizing the outcome and recovery of patients. Fifty percent of the participants were in the early stage of stroke, and a higher proportion of them had severe anxiety and depression and poor QOL, which may be attributed to their adaptation to the sudden loss of functional ability, uncertainty, and lifestyle changes induced by the stroke. In the present study, severe depression appeared as the most significant predictor of low QOL, which is in line with previous studies (Jarosławski et al., 2020). These psychological impairments may disturb rehabilitation, lower patient satisfaction, and raise healthcare expenses (Abuadas et al., 2023; Ahmed et al., 2020; Ayasrah et al., 2022; Chen et al., 2019; Lourenço et al., 2021). They can also have a negative impact on adherence to medication and long-term treatment, increasing the risk of stroke recurrence (Basheti et al., 2019, 2022, 2024). Since the early poststroke period is usually the best period to initiate rehabilitation services, psychological well-being interventions like early detection and referral to professional evaluation and treatment are necessary to enhance patients’ recovery and achieve the best possible QOL.
This study has not assessed other negative and positive factors that are identified in literature and affect psychological impairment and QOL in stroke survivors. Such negative aspects as financial pressures, expensive treatments, and geographical barriers could delay early diagnosis and timely management and contribute to poorer outcomes (Ayasrah et al., 2024; Chen et al., 2019). Timely stroke management in Iraq is usually not accessible because of the lack of stroke centers, insufficient healthcare infrastructure, and security concerns, leading to high mortality rates, long-term disability, augmented psychological impairments, and poor QOL (Abd, 2019; Alshalchy et al., 2024; GBD, 2019 Stroke Collaborators, 2021). The prior literature has identified strategies for enhancing stroke care. These involve pre-hospital interventions like community education to facilitate stroke awareness, pre-hospital triage procedures that may offer direct transfers to thrombectomy centers, and mobile stroke units, which are both location-specific and more relevant in urban areas with high population density. Simple stroke protocols (stroke codes), the location of stroke units and imaging rooms strategically, ambulance to imaging transport, and continuous education and training of stroke teams are some of the strategies applied within the hospital. They can be generally applied even in resource-restricted settings (Botelho et al., 2022). Alongside community education, these measures may be adopted in Iraq to deal with geographical and systemic barriers, minimize the delays in the treatment process, and enhance the outcomes of patients with acute stroke.
Positive factors include patient satisfaction, shorter hospital stays, support from healthcare providers, and strategies to improve gait, balance, and coordination (Jingwen et al., 2018; Schmid et al., 2013). Interventions such as physiotherapy, medication reviews, fall-prevention strategies, and early detection and management of stroke-related anxiety and depression have been demonstrated to improve functional outcomes, emotional well-being, satisfaction, and long-term QOL (Basheti et al., 2024; Jingwen et al., 2018; Schmid et al., 2013).
Strengths and Limitations
The exclusion of stroke patients with severe impairments in speech, language, or cognition; those patients with life-threatening conditions; those with previous strokes, or those with a history of drug abuse or psychological intervention due to anxiety/depression before stroke restricts the comprehension of the complete range of experiences of stroke survivors. The utilization of medical records to rule out patients who had a history of depression or anxiety before stroke may result in the inclusion of unidentified or unrecorded cases that were affected by the pre-stroke psychological situation. Additionally, the cross-sectional design used in this study may have an impact on the representativeness of long-term outcomes of stroke. The use of self-report instruments could also introduce socially desirable responses. However, the research involved patients representing a broad geographical area and from various hospitals, which strengthens its generalizability.
Despite these limitations, the results indicate a significant reduction of QOL in Iraqi stroke patients, as well as clinically significant psychological impairments and their predictors. In the future, longitudinal and intervention studies are needed to evaluate the experience of stroke patients across time and identify effective interventions to maximize their outcomes. Further research that includes fatigue along with anxiety and depression is also recommended to avoid overlapping.
Implications for Practice
There are various implications of this study in clinical practice. Clinicians and nurses caring for stroke patients should be aware that anxiety and depression are common and might reach clinically significant levels that disturb rehabilitation. The psychological status of patients, especially in the acute phase, should be assessed early enough to facilitate timely referral for proper diagnosis and subsequent treatment of patients at risk.
Following a stroke, the QOL of many survivors becomes evidently poor. Advanced age, single status, a history of hypertension, shorter time since the stroke, and clinically significant levels of anxiety and depression are all associated with declined QOL and potentially poor recovery. Elderly patients usually report higher levels of psychological impairments and a greater decline in QOL and thus require more support. Enhancing social support and managing modifiable risk factors, including high blood pressure, can be significant in terms of enhancing the recovery process and QOL.
Conclusion
Stroke is a growing health problem in Iraq associated with a high level of delay in providing timely and effective treatment due to many reasons, such as a lack of stroke care services, inadequate health care facilities, and the continued security problems. These problems were linked to high mortality rates, long-term disability, and poor health outcomes. In addition, patients with stroke in Iraq have severe levels of anxiety and depression, which are higher compared with those of Arabic and international literature. They also show poorer QOL than that reported elsewhere. The risk factors include older age, being single, the presence of hypertension, a recent stroke, and clinically significant levels of anxiety and depression. Prevention programs targeting hypertension as a modifiable risk factor along with reinforcement of social support and early detection and management of psychological impairments should be a priority. Also, the development of the healthcare system and the availability of specialized stroke care are needed to ensure that stroke survivors receive quality and timely care, and this can ultimately lead to improved QOL. Overall, these findings highlight the necessity for comprehensive stroke management strategies addressing not only medical and physical rehabilitation but also psychological care and socioeconomic support, especially considering Arabic culture, to enhance recovery and the overall outcome of the stroke survivors.
Footnotes
Acknowledgements
The research reported in this publication was supported by the Deanship of Scientific Research and Innovation at Al-Balqa Applied University in Jordan. The authors express their gratitude to Al-Balqa Applied University for its support.
ORCID iDs
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.