
Abstract
Introduction
Stroke is a significant health problem and is considered one of the leading causes of mortality and permanent disability worldwide. Hypertension is a primary risk factor for stroke. Thus, hypertensive patients’ knowledge, attitudes, and practices (KAP) are essential in preventing stroke.
Objective
To examine hypertensive patients’ KAP towards stroke prevention among rural population in Saudi Arabia.
Methods
The study utilized a cross-sectional design. The data were collected using a convenience sampling technique from hypertensive patients in the northwestern rural areas of Riyadh Province. A self-administered questionnaire was adapted from the Stroke Recognition Questionnaire (SRQ) and utilized to assess KAP towards stroke prevention among rural hypertensive patients. The STrengthening of the Reporting of OBservational studies in Epidemiology (STROBE) checklist was used to report the study.
Results
A total of 196 hypertensive patients participated in the study. The total mean scores categorization into three quartiles showed that most respondents had poor levels of KAP towards stroke prevention. Weak positive correlations were found between KAP of patients. There were statistically significant differences between respondents’ attitudes and practices with their age, education, marital status, and occupational status.
Discussion
This study denoted poor levels of KAP towards stroke prevention among hypertensive patients living in rural areas. This study showed the importance of further considering rural population by which improving their health and quality of life. Extending health educational programs and behavior-changing strategies to rural areas is essential to increase hypertensive patients and general public awareness about their stroke prevention and other health-related concerns.
Introduction
Cardiovascular diseases are a group of disorders considered as the primary cause of death and the main contributor to disability worldwide (Roth et al., 2020). Heart and blood vessel disorders are the main components of cardiovascular disease, including coronary heart disease, cerebrovascular disease, stroke, and other conditions that negatively impact global and public health (Ofori-Asenso & Garcia, 2016). Stroke is a significant health problem that causes mortality and permanent disability worldwide (Chen et al., 2020). It is known that cerebrovascular accident (CVA) and a neurologic disorder are originating from the blockage or rupture of cerebral blood vessels with ischemic or hemorrhagic etiologies (AlHarfany et al., 2020; Ullah et al., 2020). Stroke or CVA leads to death and is the third leading cause of disability worldwide (Williams et al., 2020). Annually, there are 15 million reported stroke cases, with 5.8 million reported deaths globally (Al-Senani et al., 2020). The incidence of stroke is approximately 43.8 per 100,000 in Saudi Arabia (KSA), which indicates the general public's lack of knowledge and awareness (Bakraa et al., 2021). Moreover, CVA is a significant cause of death and disability, where it accounts for about 6.4% of the mortality rate in KSA (Mubaraki et al., 2021).
Review of Literature
Stroke survivors suffer from several types of motor and non-motor problems, which impedes contribution to daily activities and deteriorates the quality of the patient's lives if improper resolving these complications (Im et al., 2020). Also, the stroke burden results in a wide range of activity limitations that requires personalized rehabilitation from patients to overcome them (Gittins et al., 2021). Stroke arises from modifiable and non-modifiable risk factors where hypertension (HTN) is considered a significant modifiable risk factor and accounts for 70% of ischemic stroke worldwide (Ma et al., 2018; Wang et al., 2022). HTN means an elevation of blood pressure where systolic blood pressure increases over 140 mmHg and/or diastolic blood pressure (DBP) increases over 90 mmHg at rest (Kurl et al., 2021). Globally, HTN continues to be a major risk factor for cardiovascular disease and mortality (Reboldi et al., 2022). HTN is often called the silent killer because it is asymptomatic in many cases and symptoms are difficult to detect without special apparatus, causing around 9.4 million deaths worldwide (Kalehoff & Oparil, 2020; Sayyad et al., 2021).
The prevalence of HTN varies among developed and developing countries; however, its incidence remains high, affecting about 40% of the worldwide population (Lugo-Mata et al., 2017). In the United States, for example, nearly 47% of all adults and 76% of those who are over 65 years old have HTN (Centers for Disease Control and Prevention, 2021). Data from 30 studies revealed that HTN is the most prevalent risk factor for stroke and has been reported in about 64% of patients with stroke, leading to the high hospital mortality rates (Wajngarten & Sampaio Silva, 2019). A study reported that the crude prevalence rate is estimated at around 29.5%, with wide variability between countries (Abboud & Karam, 2021). The Middle East and North Africa showed that the pooled prevalence of pre-HTN and HTN was 30.6% and 26.2%, respectively, accompanied with low awareness, and poor HTN control (Balouchi et al., 2022). In Saudi Arabia, HTN is a significant public health issue and is now one of the main causes of death. According to a recent national survey, the HTN prevalence rate in Saudi Arabia is 31.4%, where 57.8% of them were unaware of their illness (Alshammari et al., 2021). Additionally, 25% of those who were aged between 15 and 64 years old have been reported to have HTN (Alshammari et al., 2021; Khafaji et al., 2021).
The lack of understanding, improper diagnosis, and inadequate management of HTN contributed to an increased risk of stroke in different countries (O’Donnell et al., 2016). Several studies have shown a lack of awareness among hypertensive patients towards risk factors, warning signs, and behaviors of acute stroke (Bhat et al., 2021). For example, a study conducted in northwest Ethiopia among hypertensive patients showed that nearly 72% of the respondents did not know any risk factors and warning signs of stroke (Abate et al., 2019). In general, most community-based studies reveal that the general public has a deficiency in knowledge about stroke, lifestyle risk factors, and warning signs (Khalil & Lahoud, 2020). A shortage of information and poor self-care practice increases the burden of HTN, they in fact are a crucial challenge in controlling HTN (Alshammari et al., 2021). A study conducted in the Eastern Province of the KSA revealed relatively high illiteracy about stroke and its risk factors. The study revealed that 58.5% were unaware of stroke risk factors such as diabetes, and 59.9% did not identify the warning signs of stroke, including facial asymmetry (Zafar et al., 2020). Population awareness is vital to confront the lack of information regarding stroke and its associated factors for early stroke prevention (Arisegi et al., 2018).
Furthermore, effective management of stroke depends mainly on the public's awareness of its warning signs, which could help in earlier detection and better response rates (Kalehoff & Oparil, 2020; Sayyad et al., 2021). As HTN is considered a main modifiable risk factor for stroke, there is still a lack of studies that examine hypertensive patients’ awareness of stroke. Although some studies about HTN across different KSA provinces generally vary in HTN prevalence between 5% and 30% (Abseh et al., 2020), no study has been found that focused on an underserved population such as those who are living in rural areas. Therefore, it is necessary to measure hypertensive patients’ knowledge, attitudes, and practices (KAP) towards stroke prevention among rural population and explore that factor that may contribute the KAP levels. Generally, rural population have less access to healthcare services, as well as they have lower socioeconomic status compared to their counterparts in other areas which may influence hypertensive patients KAP toward stroke prevention. Thus, this study aims to assess hypertensive patients’ KAP towards stroke prevention in rural areas of Riyadh Province in KSA. Furthermore, differences and correlations between KAP and demographic characteristics were examined. This study's findings may help policymakers implement awareness programs for primary and secondary stroke prevention in KSA.
Methods
Study Design
The study utilized a cross-sectional, descriptive, and community-based design to examine hypertensive patients’ KAP among rural population. The STrengthening of the Reporting of OBservational studies in Epidemiology (STROBE) checklist was used to report the study.
Sample and Setting
The sample included rural population who are living in the northwestern rural areas of Riyadh Province in KSA. Riyadh Province includes about a hundred scattered rural areas or as known villages. They are located near urban areas or between them, and the population are less than five thousand. In KSA, approximately 20% of the total population lives in rural areas, and 8.5% of Riyadh Province population lives in rural areas (General Authority for Statistics, 2021). These rural areas have lower levels of education, lower income, and less access to healthcare services. The inclusion criteria for this study included adults aged 18 or older, diagnosed with HTN, lived in rural areas, and able to read and respond to the questions. The exclusion criteria included those treated from HTN, lived in areas other than rural, or did not wish to participate in the study.
Data Collection
A convenience sampling method was used to recruit participants for this study. The researchers created a link and a quick response (QR) code to collect data from participants using online methods to avoid direct contact during the COVID-19 pandemic. The researchers collected data from eligible participants at healthcare centers and small shopping malls. The participants were invited and recruited to answer the questionnaire after identifying that they were diagnosed with HTN and met the other inclusion criteria. Eligible participants then opened the link (after texting them) or scanned the QR code and began answering the questions. Participants had to agree to participate in the study before proceeding to the study questions. Otherwise, if they did not agree to participate, the questionnaire would close and end at this point. The data collection phase took place between May and September 2021.
Measurement
The researchers designed and constructed a self-administered questionnaire utilizing an adapted version of the Stroke Recognition Questionnaire (SRQ) to assess stroke prevention KAP amongst hypertensive patients (Abate et al., 2019). The original SRQ was translated using the forward-backward translation method by five bilingual experts. The researchers modified the study instrument as per the experts’ recommendations. The researchers carried out a pilot test on 30 respondents using the final version of the questionnaire and made corrections accordingly for the feasibility and content applicability of the questionnaire. The Arabic language is the primary language in KSA; thus, the researchers used the Arabic version of the SRQ in the study.
The respondents of the pilot study were excluded from the main study. The researchers pretested the instrument's items for the reliability of internal consistency before the questionnaire was released. The Arabic version of the SRQ in this study had acceptable reliability with Cronbach's alpha coefficient of 0.85, 0.92, and 0.85, respectively, for KAP.
The Components of the Questionnaire
The questionnaire included 42 items divided into four parts. Part 1 included seven sociodemographic characteristic questions about gender, age, marital status, occupation, educational level, controlling blood pressure, and whether the respondents had previously heard about stroke. Part 2 comprised 22 questions that assessed the respondents’ knowledge about stroke, including the definition of stroke (items 1, 2), risk factors of stroke (items 3–9), signs and symptoms of stroke (items10–15), and complications of stroke (items 16–22). This part was based on a three-point Likert-type scale to measure the level of knowledge rating as correct response (2 points), neutral (1 point), and incorrect correct answer (0 points). Part 3 consisted of six items to measure the number of attitudes towards stroke prevention. Questions of this part were based on a 5-point Likert scale ranging from strongly agree (5 points), agree (4 points), undecided or neutral (3 points), disagree (2 points), and strongly disagree (1 point). Part 4 consisted of seven items that assessed the number of practices towards preventing stroke. Questions of this part were based on a five-point Likert-type scale ranging from never do (1 point), rarely do (2 points), undecided (3 points), often do (4 points), and always do (5 points). The total mean scores of all the respondents’ KAP were calculated. According to the scoring method, the researchers categorized the total mean scores into three quartiles based on a scale of 100% to identify the level of KAP and interpreted them as follows: good (>75%–100%), moderate (50%–75%) and poor (<50%) (AL-Rawajfah et al., 2021; Jalal et al., 2021; Karami et al., 2017; Mateo et al., 2021; Rajbhandari et al., 2018).
Ethical Consideration
The investigation conforms with the principles outlined in the Declaration of Helsinki. The respondents were made aware of the aims and purposes of the study, and their full right to accept or freely refuse to participate or withdraw at any time without any consequences. All responses were anonymous, kept strictly confidential, and used for research purposes only, and the results did not identify the respondents personally. A written consent was obtained from all participants before answering the questions.
Data Analysis
The Statistical Package for Social Sciences (SPSS) version 28 was utilized for the data analyses. The researchers used descriptive statistics to calculate the frequencies, percentages, means, and standard deviations. The researchers tested the normality of the data using the Kolmogorov–Smirnova test, which denoted a non-normal distribution. Thus, the researchers adopted non-parametric tests of the inferential statistics (Mann–Whitney U, and Kruskal–Wallis, Spearman correlation coefficient) to compare differences or correlations between the study's variables. The significance level was fixed at a p-value of <.05 in all results.
Results
Sample Description
A total of 196 respondents participated in the study. Most of the respondents were male 174 (88.8%), less than 35 years old 169 (86.2%), had a college degree or above 144 (73.5%), were unemployed 110 (56.1%) and heard about stroke 151 (77.0%). Over half of the respondents were not married 108 (55.1%), and controlled their blood pressure 109 (55.6%) (Table 1).
Demographic Characteristics of the Participants (N = 196).

Assessment of Knowledge Level Towards Stroke Prevention
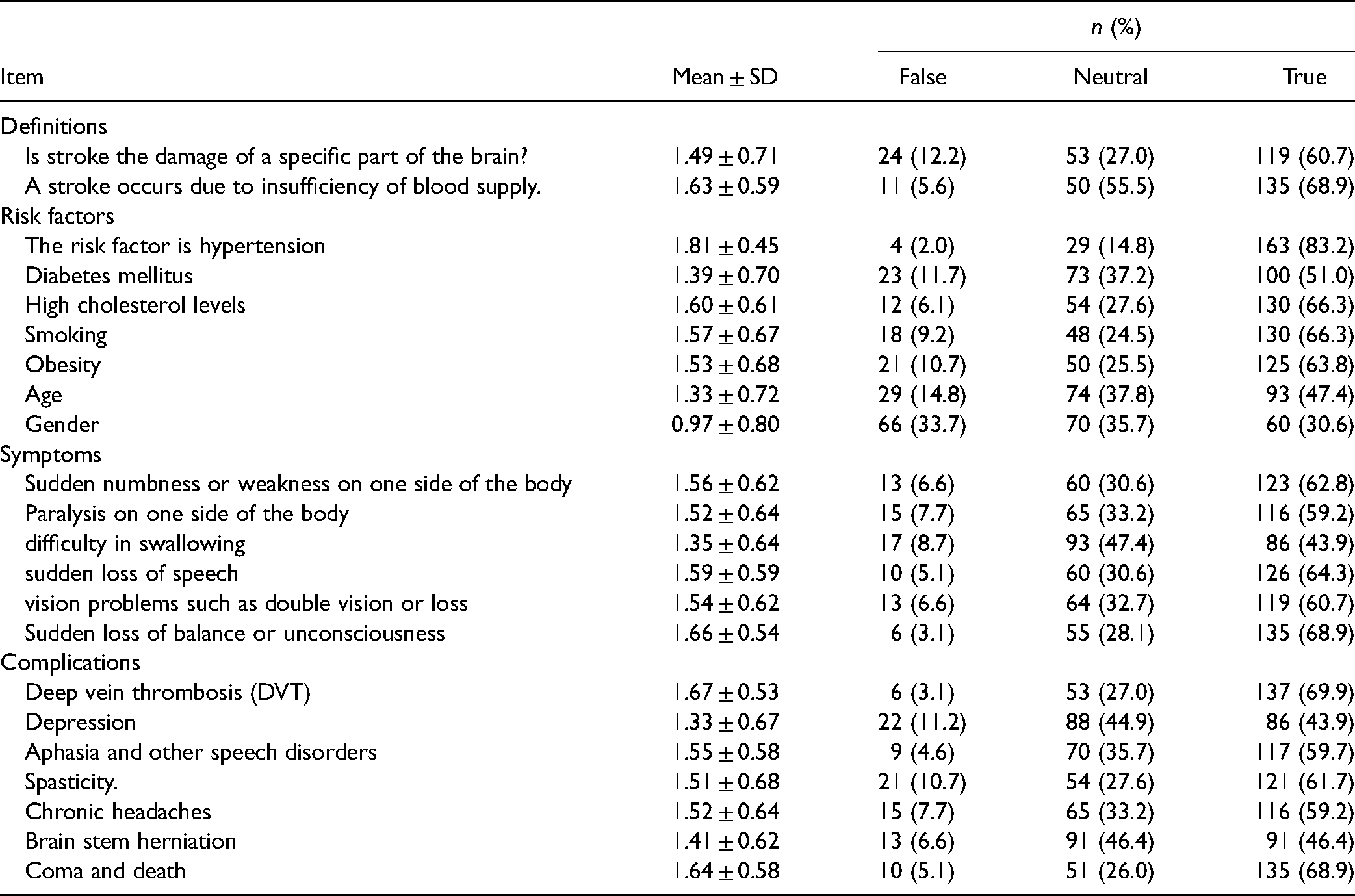
The results showed that respondents were mostly able to define stroke, 68.9% of the respondents correctly answered that stroke occurs due to insufficient blood supply, and 60.7% of them correctly answered that stroke is a damage of a specific part of the brain. Regarding the risk factors of stroke, 83.2% of the respondents correctly answered that HTN is a risk factor, followed by high cholesterol level and smoking with 66.3% correct answers. As symptoms of stroke, 68.9% of the respondents correctly answered that sudden loss of balance or unconsciousness is a stroke symptom, followed by sudden loss of speech 64.3% correct answers. Furthermore, 69.9% of the respondents correctly answered that stroke could be complicated to deep vein thrombosis, followed by coma and death with 68.9% correct answers (Table 2).
Knowledge Level Towards Stroke Prevention (N = 196).
Assessment of Attitude Level Towards Stroke Prevention
When combining those who agreed and strongly agreed, 53.1% agreed that stroke is preventable. Of the specific attitudes towards stroke prevention, the results showed that 60.2% of the respondents agreed that monitoring blood pressure regularly is a preventive attitude for stroke, followed by early diagnosis of stroke to prevent further complications with 59.2% (Table 3).
Attitude Level Towards Stroke Prevention (N = 196).

Assessment of Practice Level Towards Stroke Prevention
The findings for practices towards stroke prevention showed that most respondents (71.4%) would always respond by calling emergency or taking the stroke patient to the hospital immediately. Additionally, 39.3% of the respondents would always try to lose weight, and 34.7% follow a dietary regimen to prevent stroke (Table 4).
Practice Level Towards Stroke Prevention (N = 196).

Categorization of the Level of KAP Towards Stroke Prevention
To identify the level of KAP, the researchers categorized the overall mean scores into three groups of quartiles based on a scale of 100%: poor (<50%), moderate (50%–75%), and good (>75%–100%). The results of the scale category showed that most respondents had a poor level of knowledge (43.9%), attitudes (44.9%), and practices (47.4%) towards stroke prevention (Table 5).
Scale Categories for the Participants’ KAP Toward Stroke (N = 196).

Comparison of Mean Scores of KAP and Demographic Characteristics
The researchers utilized the Mann–Whitney U-test for two independent groups and the Kruskal–Wallis test for more than two groups to compare the mean scores of KAP towards stroke prevention and demographic characteristics. The results showed significant differences of practice mean score with respondents’ age groups. Respondents less than 35 years old showed a higher mean score for practices (M = 169 p = .001) than other age groups towards stroke prevention. The results also revealed significant differences of attitudes mean score with respondents’ educational level. Respondents with higher education (college/university degree or above) showed a higher mean score of attitudes towards stroke prevention (M = 105.44, p = .004) compared to those with low education (Table 6).
Comparisons of KAP Mean Scores and Demographic Characteristics (N = 196).

K-Mean = knowledge mean score; A-Mean = attitude mean score; P-Mean = practice mean score.
Mann–Whitney U and Kruskal–Wallis tests were used.
* p-values ≤ .05; ** p-values ≤ .001.
Moreover, there was a significant difference in the mean score of practices with the occupational status of respondents. Employed respondents had a significantly higher practice level towards stroke prevention (M = 117.56, p = .000) than those unemployed. Furthermore, there was a significant difference in the mean score of practices with marital status. Those who were married showed a higher practices level about stroke prevention (M = 111.35, p = .020) than unmarried ones. Finally, respondents who controlled their blood pressure had a significantly higher practice level (M = 114.42, p = .000) than those who did not control their blood pressure. The knowledge level did not significantly differ with all demographic variables (Table 6).
Correlation Between KAP
A Spearman's rho test was performed to examine the strength and direction of the correlation between the study domains of KAP. The results revealed a significant positive weak correlation between knowledge and attitude (r = .296, p = .000), and knowledge and practice (r = .248, p = .000). However, a significant negative weak correlation was observed between attitude and practice (r = −.249, p = .000) (Table 7).
Correlation Between KAP (N = 196).

Spearman's rho test was used.
* p ≤ .001.
Discussion
HTN contributes significantly to the stroke burden worldwide (Ma et al., 2018). Good awareness and knowledge of stroke risk factors are vital for early stroke prevention (Arisegi et al., 2018). Therefore, in this community-based study, we sought to investigate KAP towards stroke prevention amongst hypertensive patients in KSA. In the current study, most respondents were males, younger adults, not married, and employed, had a college degree or above, did not have a history of stroke, and almost half of them controlled their blood pressure. In general, HTN in KSA is at high risk in males and those at younger ages (Buang et al., 2019; Dar et al., 2019). And as HTN may sharply increase with age and other combinations of cardio-metabolic risk factors (Sarfo et al., 2021), more attention should be paid to all community members with specific consideration to those at higher risk. The level of awareness about HTN, for instance, is needed for all community members.
The current study revealed that most respondents had a poor level of knowledge about stroke prevention, risk factors, symptoms, and stroke complications. This result is consistent with an earlier study conducted in KSA, which showed that most hypertensive patients had poor knowledge about risk factors and warning signs of stroke (Mersal & Tork, 2020). Our study result is also similar to most previous international studies that indicated the level of knowledge and the basic understanding of risk factors and warning signs of stroke were inadequate among people with high blood pressure (Bhat et al., 2021; Houessou et al., 2021; Melak et al., 2021). For example, a study conducted in Indonesia found that the majority of patients with high blood pressure in the study were unaware of the risk of stroke (Setyopranoto et al., 2022). In contrast, our result is inconsistent with the studies conducted in Cameroon among the general public, which found high knowledge about stroke risk factors and warning symptoms (Nansseu et al., 2017). A possible explanation for our results is that most respondents may lack information due to insufficient awareness campaigns about stroke prevention and its risk factors, such as HTN. This would leave a significant education gap for residents of areas who may find difficulties accessing enough knowledge.
The current study demonstrated that most respondents had poor attitudes towards monitoring their blood pressure, early diagnosis, treating heart disease, and smoking cessation to prevent stroke. This result is inconsistent with some other international studies that showed most hypertensive participants had a neutral attitude toward stroke prevention approaches (Sinha et al., 2020). For example, this result is inconsistent with a study conducted in India that showed a relatively high attitude score of hypertensive people than the non-hypertensive people towards stroke prevention (Sreejesh et al., 2018). Our result could be contributed to the previous result where most participants had a poor level of knowledge, which may influence their behaviors and attitudes towards stroke prevention. If not corrected, lack of knowledge may impede proper respondent behaviors towards stroke prevention.
The present study also showed that most of the respondents had poor practices towards stroke prevention. They lack preventive measures such as trying to lose weight, exercising, adopting dietary regimens, regularly checking blood sugar levels and blood pressure, calling emergency healthcare services, or going to the hospital immediately. Generally, preventive practices for stroke have been reported to be mostly inadequate among hypertensive and diabetic patients (Melak et al., 2021). This result is consistent with another study conducted in a tertiary care hospital in Pakistan which indicated that stroke prevention practices were sub-optimal (Dar et al., 2019). One possible explanation for our result is the poor level of knowledge among respondents. This result may also be contributed to the lack of educational programs for individuals who live in rural areas.
This study examined the correlation between the study variables, namely KAP. The results showed a significant positive weak correlation between knowledge, attitudes towards stroke prevention. This correlation indicates that respondents who knew more about high blood pressure consequences had a better attitude towards stroke prevention. Accordingly, any increment in knowledge regarding stroke prevention among hypertensive patients will motivate them to change their attitude positively. The study also found a significant positive weak correlation between knowledge and practices. This finding means that good knowledge leads to better performance in some circumstances (Buang et al., 2019). Accordingly, someone who knew that HTN could cause stroke would perform a certain strategies for preventing stroke, including lifestyle modifications in regular physical exercise, avoiding tobacco use, regulating salt intake, and controlling major risk factors of HTN, diabetes, and heart diseases (Mulugeta et al., 2020). Therefore, the training program is vital to improve their practical behaviors towards stroke prevention. Knowledge is key for changing behaviors, so people must have sufficient and accurate information about stroke and its risk factors that would enhance both public preventive attitudes and practices. These results support the previous discussion about the possible effect of lack of knowledge on poor attitude and practices. Thus, a regular healthy educational program, specifically for underserved population, is crucial to increase understanding towards stroke prevention and enhance respondents’ preventative attitudes and practices.
This current study compared the mean rank scores of KAP towards stroke prevention with their demographic characteristics to determine any differences within the variables. There were significant differences between the mean scores of practices and the age of respondents. The respondents less than 35 years old showed a higher mean score of practices towards stroke prevention than the other age groups. This finding contrasts with a study conducted in India that showed most participants over 60 years old had good practices for stroke prevention (Sinha et al., 2020). Our result could be attributed to the high exposure to knowledge among younger people with the recent high growth of technology. Although some recourses nowadays are not valid and reliable, younger people are more open to searching and looking for information. Therefore, young people may become more adherent towards stroke prevention than elderly respondents.
In our study, respondents with a college degree or above showed a statistically significantly higher average score of attitudes towards stroke prevention than those with high school or below. And those who were employed exhibited a significantly higher practice towards stroke prevention than the other vocations. These results were expected as knowledge about stroke prevention increases with higher education and being employed (Arisegi et al., 2018). Thus, attitudes and practices would enhance with good knowledge, which has been found in our current study. A possible explanation for these results might be that employed and educated people are either exposed to more educational programs or can easily access required resources.
There was also a significant difference between the mean score of practices and marital status, where married individuals had a higher mean score of practices towards stroke prevention. This result is aligned with what has been reported by Melak et al. (2021); authors reported that lack of knowledge and preventive practices of stroke is associated with being unmarried. This may be related to the spousal social support between married couples that one gives to the other which could positively influence their health (Ryan et al., 2014), and stroke prevention is a health concern. Moreover, respondents who controlled their blood pressure had a significantly higher mean score for practices towards stroke prevention than those who did not control their blood pressure, indicating that those who maintain their blood pressure have good practical behaviors and adhere to preventive measures towards stroke prevention.
Finally, HTN is a significant risk factor for cardiovascular disease and stroke, where 70% of ischemic stroke is caused by high blood pressure. It contributes significantly to the stroke burden worldwide (Ma et al., 2018). HTN is a significant risk factor and contributes to the high burden of cardiovascular disease and stroke. Good awareness and knowledge of stroke risk factors are vital for early stroke prevention (Arisegi et al., 2018). Therefore, continuous health education is mandated for hypertensive patients to adopt preventive measures such as taking hypertensive medications and regularly checking blood pressure and sugar levels to prevent risk factors.
Limitations and Strengths
These results of the present study are not conclusive and have some limitations. First, the study recruited hypertensive patients from one part (northwestern) of the Riyadh Province. Second, a convenience sampling technique was used for data collection, leading to primarily male respondents. All these limitations could affect the generalizability of the study results to the entire population of KSA. A noteworthy strength of this study is that the focus was on people who live in rural areas. This would clarify the health status of those who live in those areas that may lack some services, including healthcare.
Implications for Practice
The study has important implication for nursing education and practice, and health policy. This study highlighted the level of awareness among rural population who are understudied. Thus, the study revealed important information about those population towards their health. Nurses play a significant role in providing holistic care to individuals, families, and the community. Specifically, Community/public health nurses role include educating public about their needs in order to monitor and improve their health. Therefore, knowing and understanding hypertensive patients’ levels of awareness towards stoke prevention would improve nurses’ preparedness and readiness to provide proper services, materials, and education to them.
Conclusions
This community-based study has highlighted the poor levels of KAP towards stroke prevention among hypertensive patients in rural areas of Riyadh Province in KSA. The findings suggest that policymakers should adopt effective health education interventions that could be useful for primary stroke prevention programs to help the community, especially high-risk groups with HTN, increase their awareness of the cardiovascular disease and stroke prevention in KSA. Further research regarding stroke prevention is still required to cover other areas of the KSA. Additionally, future research should focus on providing and implementing health education programs for hypertensive patients and the general public and measure their efficacy.
Footnotes
Acknowledgments
The authors extend their appreciation to the Deputyship for Research & Innovation, Ministry of Education in Saudi Arabia for funding this research work through the project number (IFP2021-029).
Author Contributions
Study design: FA, MA. Data collection: AM, MM, AAL. Data analysis: FA, MA. Study supervision: FA. Manuscript writing: FA, MA, AM, MM, AA. Critical revisions for important intellectual content: FA, AA.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
The researchers obtained ethical approval before conducting the study from Shaqra Universiyt, Saudi Arabia.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Deputyship for Research & Innovation, Ministry of Education in Saudi Arabia (grant number IFP2021-029).