
Abstract
Introduction
Disaster education courses for nurses help in improving their disaster preparedness. However, in Jordan, few studies measured the effectiveness of the implementation of disaster management education course on nurses’ knowledge, skills, and disaster preparedness.
Study Objective
This study examines the effect of disaster management education course on nurses’ knowledge, skills, and preparedness for disaster management.
Methods
A quasi-experimental design was used among a convenience sample of 73 nurses from two hospitals. One-day disaster management education course workshop was conducted for eight hours. The Disaster Preparedness Evaluation Tool (DPET) was used to examine study variables. The nurse's knowledge, skills, and preparedness were measured at three points of time. Data were collected using a self-administered questionnaire over three months’ period (May 1-July 29, 2023).
Results
The results revealed a significant improvement in nurses’ knowledge, skills, and preparedness for disaster management immediately after, and after one month of the implementation education course. The results provide evidence about the effectiveness of implementing disaster management education course in enhancing nurses’ knowledge, skills, and preparedness for disaster management.
Conclusion
Policymakers need to implement education course to address nurses’ needs concerning disaster management preparedness and implement strategies to improve their knowledge and skills.
Introduction
Background
Disasters are unforeseeable catastrophic events that affect environmental, social, and economic factors worldwide. The United Nations Office for Disaster Risk Reduction (UNDRR) defines a disaster as “a serious disruption of the functioning of community or society at any scale due to hazardous events interacting with conditions of exposure, leading to one or more of the following: human, material, economic and environmental losses and impacts that exceed the ability of the affected community or society to cope using its resources” (UNDRR, 2020). According to the International Federation of Red Cross & Red Crescent Societies (IFRC), disasters are classified into Natural Disasters, Man-Made, and Technological Disasters (International Federation of Red Cross & Red Crescent Societies, 2014). Natural disasters are sudden, extreme physical phenomena caused by environmental factors. It is divided into five categories: biological, meteorological, climatological, hydrological, and geophysical disasters. Man-made and Technological disasters are extremely hazardous events caused by humans. It included environmental degradation, pollution, conflict, industrial accidents, transport accidents, and complex emergencies (International Federation of Red Cross & Red Crescent Societies, 2014).
During the last two decades, global disasters have killed 1,23 million persons; 4 billion were injured, displaced, and needed emergency assistance; and the global economic loss was estimated to be over $2.97 trillion (Human Cost of Disasters, 2020). According to recent evidence from the United Nations Office for Disaster Risk Reduction (2024), there has been a noticeable increase in the number of disasters worldwide, with certain regions showing greater vulnerability compared to previous decades. Rising sea levels, climate change, poverty, fast urbanization, war, and civil unrest are all disaster-contributing factors (Palmer, 2018).
The coronavirus pandemic best illustrates the disastrous consequences of catastrophes on humans worldwide. As of 1st January 2023, approximately 656 million have been infected, and more than 6.6 million have died due to the coronavirus pandemic (World Health Organization (WHO), 2023). Additionally, the coronavirus pandemic negatively affected the global economy, social and mental health, and the healthcare system. These consequences redefine the humanitarian emergency paradigm and force the global community to develop new strategies to deal with disasters and mitigate their effects (International Federation of Red Cross & Red Crescent Societies, 2023).
International initiatives have focused on organizing and integrating disaster prevention and preparedness efforts and effective disaster management solutions (Patel, 2019). Disaster management is a cyclical and continuous process that aims to reduce the potential losses from hazards, ensure timely assistance to affected populations, and enable rapid and effective recovery (UNDRR, 2019). It is defined as “the organization and management of resources and responsibilities for dealing with all humanitarian aspects of emergencies, in particular, preparedness, response, and recovery to lessen the impact of disasters” (Leaning & Guha-Sapir, 2013). Appropriate measures taken at all stages of the disaster management cycle result in better preparedness, improved warnings, reduced vulnerability, increased community resilience, and disaster prevention in the next subsequent interaction (Warfield, 2015). Effective disaster preparedness is considered essential for successful disaster management (Sangkala & Gerdtz, 2018). In this context, disaster training refers to structured educational and practical programs—including simulations, drills, workshops, and competency-based exercises—that aim to equip healthcare providers, particularly nurses, with the knowledge, skills, and attitudes necessary to respond effectively to emergencies. This definition emphasizes both theoretical learning and hands-on practice to ensure readiness in real-world disaster scenarios.
Hospitals are the first line of defense during disasters. Nurses comprise the largest percentage of the healthcare system (WHO, 2020a, 2020b). Nurses provide physical and psychological services at all stages of disasters (pre-disaster, impact disaster, post-disaster) (Firouzkouhi et al., 2021). Professional knowledge and skills are essential elements of effective nursing practice. Knowledgeable and skillful nurses are key to better dealing with disaster management (Bakhshi et al., 2020). Further, effective disaster preparedness is positively correlated with nurses’ knowledge and skills (Azizpour et al., 2022). However, nurses indicate a lack of adequate knowledge, skills, training, and abilities in disaster nursing (Al Harthi et al., 2020). Furthermore, nurses face several challenges regarding disaster management such as disaster nursing being a new specialty, the need for more investment in preparedness, limited formal education, lack of research skills, and issues related to nurses’ roles in disasters. Educators, researchers, and stakeholders need to collaborate to tackle these issues and improve disaster nursing (Al Harthi et al., 2020).
The WHO and the International Council of Nurses (ICN) first introduced the Framework of Disaster Nursing Competencies in 2009. This framework outlined disaster nursing competencies across three key levels—knowledge, skills, and attitude—organized into eight domains: Preparation and Planning, Communication, Incident Management Systems, Safety and Security, Assessment, Intervention, Recovery, and Law and Ethics. In 2022, the ICN and WHO updated this framework to reflect evolving global health challenges, lessons learned from recent disasters and pandemics, and advancements in nursing roles. The ICN-WHO Global Competency Framework for Disaster Nursing (2022) emphasizes nurses’ leadership, inter-professional collaboration, ethical practice, and integration of digital technologies in disaster management. Each competency continues to include knowledge, skills, attitudes, and learning objectives necessary for achieving proficiency in disaster nursing (ICN & WHO, 2022). The ICN highlights the importance of continuous education, training, and participation in drills to strengthen preparedness and resilience among nurses and communities (ICN & WHO, 2022).
Training is a process that provides conditions in which individuals gain knowledge, skills, or ability. Disaster education has a benefit for victims/survivors, healthcare providers, and health institutions. It helps to reduce the mortality and morbidity of victims, maintain the psychological status of victims/survivors, and also improve healthcare providers’ competencies, self-efficacy, and self-esteem (Chang et al., 2022). Nursing initiatives play a vital role in supporting the development, implementation, and evaluation of disaster preparedness and response training programs to enhance nurses’ readiness for emergency situations (Robert & Brown, 2004).
Literature Review
Globally, the number of disaster training and education programs increased gradually over the last twenty years. Most of them focused on disaster preparedness and response; and are significantly associated with the enhancement of nurses’ knowledge, skills, and preparedness (Rahman & Atalla, 2020). A variety of approaches and techniques are used in disaster education courses to enhance nurses’ knowledge, skills, awareness, and attitudes. These include simulation, which provides realistic, scenario-based experiences that allow nurses to practice decision-making in a controlled environment (Aliakbari et al., 2015); instructor-led training, where educators deliver structured lessons and demonstrations to guide participants through disaster response protocols (Gebbie & Qureshi, 2002); drills
In the Middle East, Jordan is particularly vulnerable to both natural and man-made disasters due to its geographic location and regional instability. Although it is considered relatively safe from large-scale natural hazards such as earthquakes and floods, Jordan frequently experiences flash floods, droughts, and occasional seismic activity. Moreover, its proximity to conflict zones has resulted in complex humanitarian emergencies, large-scale refugee influxes, and increased pressure on the healthcare system (UNHCR, 2024). The country's health sector—especially hospitals—often operates at maximum capacity, leaving limited room for emergency surges during disasters. Consequently, strengthening disaster management, especially within healthcare institutions, is a national priority. Nurses, as frontline responders, play a pivotal role in ensuring hospital readiness and community resilience in such circumstances. Therefore, enhancing nurses’ disaster preparedness through structured education and training is essential to improving the national disaster response capacity.
Recognizing this gap, the present study was conducted in Jordan and aimed to examine the effectiveness of a disaster management education course in enhancing nurses’ knowledge, skills, and preparedness for disaster response. While Al-qbelat et al. (2022) also investigated the impact of disaster education, their study was limited to emergency nurses and measured preparedness only immediately after the intervention. In contrast, the current study focused on a broader group of healthcare professionals and assessed preparedness at multiple time points (immediately and one month after the course), thereby providing evidence on both the immediate and sustained effects of disaster education. The findings of this study are expected to provide valuable insights for policymakers and nursing leaders to better address nurses’ needs regarding disaster preparedness and to develop targeted strategies that strengthen their competencies in disaster management.
Methods and Materials
Study Design
A one-group pretest-posttest quasi-experimental design was used in this study to examine the effect of disaster education course on nurses’ knowledge, skills, and preparedness for disaster management. This design was chosen because it allows the evaluation of changes within the same group before and after the intervention when random assignment or a control group is not feasible in a real-world hospital setting. Such an approach is appropriate in educational and clinical environments where all participants are expected to benefit from the training and withholding it from a control group would raise ethical or practical concerns.
Setting and Sample
The study was conducted in two hospitals located in Amman, the capital city of Jordan. The first hospital, the Jordan University Hospital (JUH), is a large tertiary university-affiliated teaching hospital that serves as the main training center for the University of Jordan's Faculty of Nursing and Faculty of Medicine. JUH provides both general and specialized medical services and functions as a referral hospital for patients from across the country. It is a semi-governmental institution affiliated with a public university. The second hospital, the Jerash Government Hospital (JGH), is a public, non-teaching hospital under the Ministry of Health. It provides secondary healthcare services to the general population and is one of the major governmental hospitals in the central region.
Together, JUH and JGH employ approximately 1,100 nurses among a total workforce of about 3,500 healthcare professionals
A convenience sampling method was used to recruit participants. This sampling approach was chosen because of logistical constraints, limited access to hospitals outside Amman, and the feasibility of conducting the intervention in two large institutions with well-established continuing education programs. While convenience sampling from only two hospitals may limit generalizability, these hospitals were selected because they represent both university-affiliated and governmental healthcare settings, allowing for diversity in nurse demographics, clinical experience, and exposure to disaster situations.
The sample size was determined according to Cohen's tables (Jacob Cohen, 1992). At least 64 nurses were needed to achieve sufficient power (.80) at a medium effect size and an alpha level of .05. Considering a 10% attrition rate, the total sample size was increased to 73 participants. Nurses were eligible to participate if they had at least six months of work experience. Any nurse who did not complete the entire disaster education course or questionnaire was excluded from the study.
Nurses were specifically chosen for this study because they constitute the largest workforce in the healthcare system and are at the frontline of patient care during disasters. They play a crucial role in preparedness, triage, and response during emergencies, making their training and competencies essential for effective disaster management and hospital readiness.
Instrument
Nursing knowledge, skills, and preparedness levels were measured using the Classical Arabic version of the Disaster Preparedness Evaluation Tool (D P E T) (Al Khalaileh et al., 2010), which is a direct translation and cultural adaptation of the original English DPET (Tichy et al., 2009). The Arabic tool includes 13 items assessing knowledge, 11 items assessing skills, and 12 items assessing preparedness. Responses are rated on a 6-point Likert scale (1 = strongly disagree to 6 = strongly agree), with higher scores indicating higher levels of knowledge, skills, and preparedness respectively. In addition, the tool contains demographic questions (see Table 1).
Demographic Characteristics of Participants (n = 73).
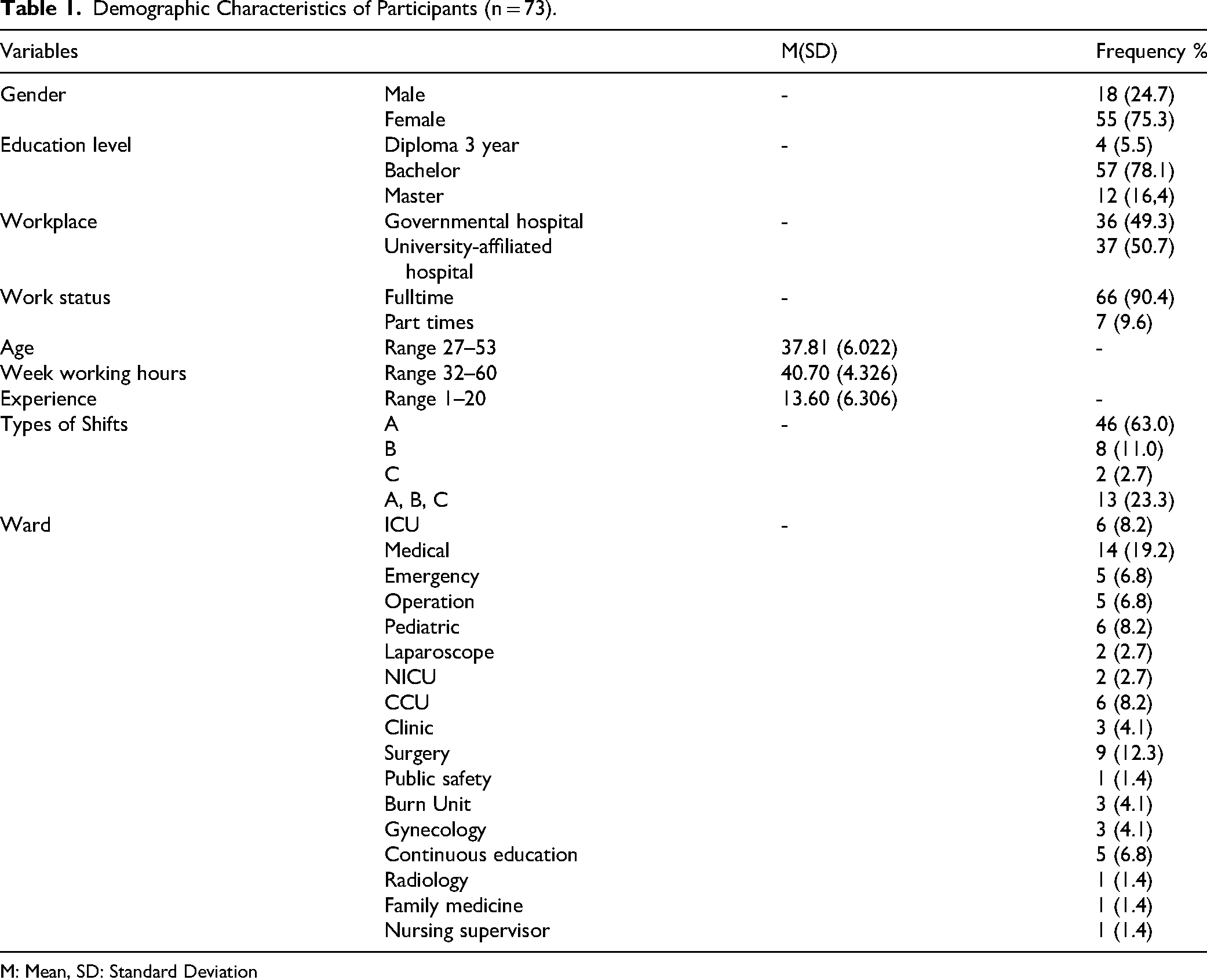
M: Mean, SD: Standard Deviation
The Arabic version of the instrument demonstrated high internal consistency, with a Cronbach's alpha of 0.90 (Al Khalaileh et al., 2010). In this study, the subscales exhibited the following alpha coefficients: knowledge (α = 0.921), skills (α = 0.910), and preparedness (α = 0.966). The overall alpha coefficient for the instrument was 0.93, indicating excellent reliability.
To further validate the construct structure of the instrument, exploratory factor analysis was conducted. The Kaiser–Meyer–Olkin (KMO) value was 0.873, indicating sampling adequacy, and Bartlett's test of sphericity was significant (p < 0.001). The total variance explained by the extracted factors was 68.4%, confirming the suitability of the data for factor analysis and supporting the internal structure of the instrument.
The Disaster Education Course
The disaster education course aimed to enhance nurses’ knowledge, skills, and preparedness for disaster management, as supported by existing literature (ICN, 2019a, 2019b; Rahman & Atalla, 2020; Robert & Brown, 2004).
The course included content on disaster definitions and types, core concepts (hazard, capacity, vulnerability, and crisis), disaster management, stages, family preparedness, nursing roles and competencies in disaster management, and hospital disaster scenarios. Educational methods included brainstorming, focus group discussions, PowerPoint presentations, and case scenarios. The course materials were reviewed by two experts in disaster management to ensure content validity.
Each education session consisted of three parts. Part 1 (120 min): Video and PowerPoint presentation of disaster definitions and types of disaster, family preparedness, chemical and biological disaster, and core concepts of disaster including hazard, capacity, vulnerability, and crisis. Part 2 (150 min): PowerPoint presentation and videos of the definition of disaster management stages of disaster management, and decontamination, and group discussion was used about the videos, disaster nursing, and disaster nursing domains, nursing roles, competencies in disaster management, and psychological first aid. Part 3 (90 min): Brainstorming, case scenarios, and focus group discussion of three scenarios related to disaster management in the hospital including: internal flooding, Bomb threat, and fire.
The training was delivered by the principal investigator, who is a registered nurse with specialized training in disaster management and two “Training of Trainers” certifications accredited by the Ministry of Health and the Jordan Nurses and Midwives Council. The trainer also has over five years of experience in hospital emergency preparedness education.
Before the intervention, participants were asked whether they had attended any previous disaster management training. Only 9.6% of the nurses reported any prior exposure to formal disaster education, and those sessions were general orientation lectures rather than structured courses. This low percentage suggests that the majority of participants were attending formal disaster training for the first time, minimizing bias due to prior training.
Data Collection
A self-administered questionnaire was used to assess participants’ baseline knowledge and skills. It required approximately 20 min to complete. The same instrument was administered immediately after the course and one month later to assess short-term and sustained effects.
Data collection occurred over three months (May 1-July 29, 2023). To reinforce learning, printed handouts summarizing the education course content were provided to each participant.
The disaster education course was integrated into the hospital's monthly education calendar for nursing staff. Sessions were held weekly, from 8:00 AM to 3:00 PM, with separate groups attending on different days to accommodate varying staff schedules. Participants were divided into eight groups, each requiring one week to complete. Four groups were from JUH, and four were from JGH. Each session comprised 7 to 13 participants.
Out of the 80 nurses initially invited to participate, 73 completed all phases of the study, resulting in a response rate of 91.25%. Seven nurses did not complete the post-test questionnaire due to schedule conflicts or workload pressures and were therefore excluded from the final analysis.
The researcher's qualifications, previous training, and standardized delivery procedures ensured consistency and credibility of data collection across both hospitals.
Ethical Consideration
After obtaining permission from the principal author of the original tool, to use the Arabic version of the DPET, the IRB approvals were obtained from the Jordan University of Science and Technology, Jordan Ministry of Health, and Jordan University Hospital (JUH).
Before beginning the training sessions, the researcher provided participants with detailed information about the study's purpose, methodology, schedule, and guidelines. This information was distributed through written materials and verbal explanations to ensure clarity and understanding. Participants were informed that their involvement was voluntary and that they had the right to withdraw at any time without any negative consequences. Subsequently, informed consent was obtained from each participant. Privacy and confidentiality were maintained.
Data Analysis
The Statistical Package of Social Science Software (SPSS) (version 25) was used for analysis. Descriptive statistics (Mean, Standard deviation, Frequency, and Percentage) were used to describe the demographic data. Repeated measure ANOVA was used to examine the effect of the disaster management education course on nurses’ knowledge, skills, and preparedness. The alpha level was set at 0.05 (Table 2).
Mean Differences of Knowledge, Skills, and Preparedness Pre-Test, Immediately After and After One Month of Implementation of the Training Program (n = 73).
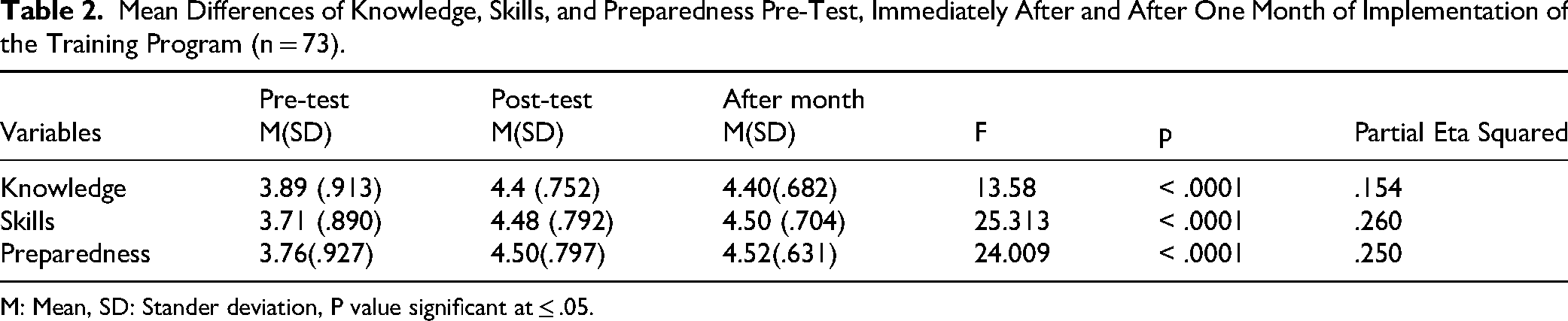
M: Mean, SD: Stander deviation, P value significant at ≤ .05.
Results
Sample Characteristics
Seventy-three participants completed the questionnaire at three points in time: before training, immediately after training, and one month after the implementation of the education course. The majority of them were females (n = 55; 75.3%). The mean age of participants was 37.81 ranging from 27 to 53 years. The participants’ mean experience in nursing was 13.60. Most of the participants worked full-time (n = 66; 90.4%) and had a four-year bachelor's degree (n = 57; 78,1%). Approximately half of them were working at the governmental hospital (49,3%); and a similar number of them worked at the university-affiliated hospital (n = 37; 50.7%). The mean of weekly working hours was 40.70 ranging from 32 to 60 h. The participants were from sixteen departments. Table 1 presents all sample characteristics.
The Effect of the Disaster Education Course on the Nurses’ Knowledge, Skills, and Preparedness for Disaster Management
The repeated measure ANOVA was used to examine the effect of the education course on Jordanian nurses’ knowledge, skills, and preparedness. The normality test was performed on the study variables. The study variables were normally distributed. The result showed a statistically significant difference in the means of nurses’ knowledge pre-test, immediately after, and after one month of attending the education course (F (2, 73) = 13.58, p < .001). Tukey post hoc indicated that there was a significant difference in the knowledge level between the pre-test and post-test (immediately after), and between the pretest and after one month of the implementation of education course. No statistically significant differences were found in nurses’ knowledge between immediately following and one month after the implementation of the education course. Table 3 presents data on the mean differences in knowledge, skills, and disaster preparedness from the pre-test, immediately following, and one-month post-implementation of the education course. Table 3 presents data about the results of the post hoc test (Tukey) for mean differences.
Post Hoc Differences in Nurses’ Knowledge, Skills, and Preparedness (n = 73).

Moreover, the result showed a statistically significant difference in the means of nurses’ skills pre-test, immediately after, and after one month of attending the education course (F (2, 73) = 25.313, p < .001). Tukey post hoc indicated that there was a significant difference in the skills’ level between the pre-test and post-test (immediately after), and between the pretest and after one month of the implementation of education course. However, no statistically significant differences were found in nurses’ skill levels between immediately after, and after one month of implementation of the education course.
Further, the results showed a statistically significant effect of an education course on nurses’ disaster preparedness immediately after and after one month of implementation education course (F (2, 73) = 24.009, p < .001). Tukey post hoc indicated that there was a significant difference in the disaster preparedness level between the pre-test and post-test (immediately after), and between the pretest and after one month of the implementation of education course. However, no statistically significant differences were found in nurses’ preparedness level between immediately after and after one month of implementation of the education course. The education course had a small effect size on nurses’ knowledge, skills, and preparedness. Partial Eta Squared scores were .15, .260. and .250 respectively, which indicates that the intervention explained approximately 15% of the variance in knowledge, 26% of the variance in skills, and 25% of the variance in preparedness. In practical terms, these values suggest that while the course had a statistically meaningful impact, its overall influence was moderate rather than large, highlighting the need for more comprehensive or repeated training to achieve stronger improvements
Discussion
This study aimed to evaluate the impact of a disaster management education course on nurses’ knowledge, skills, and preparedness. A total of 73 nurses participated, with assessments conducted at three time points: prior to the education course (pre-test), immediately following the education course, and one month after the education course.
The participants in the current study showed a significant improvement in their knowledge and practice after one month of attending the education course. Similarly, other international studies indicated that attending education courses improved nurses’ skills and practices (Jieun & Eunjoo, 2020). These results may be explained by the fact that disaster management remains an emerging and evolving concept within nursing practice, particularly in Jordan. In many healthcare settings, nurses have had limited access to structured disaster preparedness education, leading to gaps in competencies necessary for effective disaster response (Labrague et al., 2018). The disaster management education courses implemented in this study offered participants a structured opportunity to develop and strengthen their competencies in alignment with the International Council of Nurses (ICN) Disaster Nursing Competencies Framework (ICN, 2019a, 2019b). These competencies encompass critical domains such as preparedness, response, recovery, and mitigation, which are essential for effective disaster management (Usher et al., 2015). The structured, competency-based approach of the education courses likely contributed to the observed improvements in participants’ knowledge, practical skills, and overall disaster preparedness.
In this study, the majority of participants were female (75.3%), which reflects the gender distribution commonly reported in the nursing profession globally and in Jordan. According to the WHO (2020a, 2020b), women constitute approximately 70–80% of the nursing workforce. This predominance of female nurses may have influenced the study results in several ways. Literature suggests that female nurses often demonstrate strong commitment to caregiving roles, teamwork, and community response during emergencies, which can positively affect their engagement and performance in disaster management education (Al Thobaity & Williams, 2017). However, gender distribution was not expected to significantly bias the outcomes, as both male and female nurses underwent the same standardized training and evaluation processes.
Furthermore, the current study showed that participants who attended the education course significantly improved their disaster preparedness immediately following and one month following the education course, compared to their baseline preparedness level. This finding aligns with Al-qbelat et al. (2022), who reported a significant improvement in emergency nurses’ preparedness immediately after participating in a single 8-h disaster education course conducted over one week.
Moreover, Palestinian emergency nurses’ psychological preparedness regarding disasters and emergencies improved immediately after participating in a single 9-h psychological first-aid education course (Said, N. B. et al., 2020). Further, Nakhaei et al. (2019) reported a significant improvement in Iranian nurses’ preparedness for emergencies and disasters following a psychological first-aid workshop. The study assessed nurses’ preparedness immediately after the workshop and again one month later, finding sustained enhancements in their readiness to respond to such events. Moreover, Chang et al. (2022) found that self-assessed chemical disaster readiness ratings were higher for the intervention group one week following the intervention among emergency nurses in Taiwan.
The 8-h one-day disaster management education course in this study resulted in a moderate improvement in participants’ knowledge, skills, and preparedness for disaster management. This may be explained by the use of the traditional method in education, as Baetzner et al. (2022) reported that the use of technology-based approaches frequently yields education outcomes that are on par with or even better than those of traditional education. This is in contrast to the results of Pesiridis et al. (2015), who reported a significant effect of disaster preparedness and behavioral intention training program on nurses’ knowledge, preparedness, and behavioral intentions during disasters
Regarding the working experience of participants, the mean nursing experience in this study was 13.6 years, which may have contributed to the positive outcomes observed. Previous studies have demonstrated that nurses with greater clinical experience tend to possess higher baseline awareness and confidence in handling emergencies (Labrague et al., 2018). However, experience alone does not necessarily translate into disaster preparedness competence without structured training. The results of this study suggest that both experienced and less experienced nurses benefited from the education course, as the training provided standardized knowledge and skills that may not have been gained through routine clinical practice. This supports the notion that disaster management education serves as an equalizing tool that enhances preparedness across all experience levels.
Study Strengths and Limitations
This study has several notable strengths. First, the use of a quasi-experimental pretest–posttest design with repeated measurements at three time points allowed for the evaluation of both immediate and short-term sustained effects of the disaster education course, strengthening the internal validity of the findings. Second, the study was conducted in two large hospitals representing both a university-affiliated teaching hospital and a governmental non-teaching hospital, which enhanced the diversity of participants and increased the relevance of the findings across different healthcare settings. Third, a validated and highly reliable Arabic version of the DPET was used, with excellent internal consistency for all subscales, supporting the accuracy and robustness of the measured outcomes. In addition, the standardized delivery of the intervention by a qualified trainer ensured consistency in content and implementation across all participant groups.
Despite these strengths, the study measured nurses’ knowledge, skills, and preparedness immediately after the intervention and at follow-up, but did not assess long-term retention beyond the study period. The military health sector was excluded due to accessibility challenges, limiting the generalizability of findings to all healthcare settings. A convenience sampling method was used, which may affect the generalizability of the results. Data were collected using self-report questionnaires, which may introduce response bias. Additionally, the instrument used did not assess nurses’ attitudes toward disaster management, limiting the scope of preparedness evaluation.
Implications and Recommendations
For Practice
The results of this study indicate that implementing disaster management education course significantly enhances nurses’ knowledge, skills, and preparedness for disaster response, both immediately and over time. Given that disaster nursing is an emerging specialty in Jordan, nursing leaders should prioritize integrating regular disaster management education programs into nursing practice, raising awareness about disaster nursing, and developing and implementing disaster nursing competencies across all healthcare facilities.
For Research
Future research should include diverse healthcare sectors, such as military and private hospitals, employ qualitative methodologies to explore the challenges and needs of nurses in disaster preparedness, and adopt longitudinal designs to assess the long-term impact of disaster management education courses.
For Education
Educational institutions should integrate comprehensive disaster preparedness and response training into nursing curricula, provide ongoing training for nursing educators, and facilitate disaster drills and simulations to reinforce practical skills.
Conclusion
The results of this study indicate that implementing management education course significantly enhances nurses’ knowledge, skills, and preparedness for disaster response, both immediately and over time. The findings underscore the critical role of disaster-focused education in improving nurses’ knowledge, skills, and preparedness for disaster management. The greatest contribution of this study to disaster nursing lies in providing empirical evidence that short, structured educational programs can effectively strengthen nurses’ competencies, confidence, and readiness for emergency response. It also emphasizes the distinct nature of disaster nursing, which requires rapid decision-making, inter-professional collaboration, and adaptability under pressure, and demonstrates that targeted training can cultivate advanced competencies in leadership, critical thinking, and coordination essential for managing complex disaster situations. These outcomes advocate for the systematic integration of disaster management education courses to further enhance nurses’ knowledge, skills, and preparedness. Furthermore, the study highlights the necessity of implementing disaster management education across all educational levels and within healthcare institutions.
Footnotes
Acknowledgments
The authors acknowledge the study participants for their valuable participation.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the Jordan University of Science and Technology Ethical Review Committee before data collection. Participation was voluntary, requiring written informed consent for the survey. The participants’ rights were clearly outlined in the consent forms and reiterated verbally before their participation, including the option to withdraw at any time. All data were anonymized to ensure confidentiality.
Study Approval Number
The study approval number (ref. number: 10/3/2023).
Authors Contributions
RAA: Conceptualization; methodology; investigation; data curation; resources; funding acquisition; writing – original draft; writing – review and editing. RAA, YAS, HA, and MA: Methodology; investigation; formal analysis; project administration; supervision. RAA, YAS, HA, and MA: Conceptualization; methodology; software; validation; investigation; data curation; formal analysis; writing – original draft; writing – review and editing. All authors read and approved the final manuscript.
Funding
Jordan University of Science and Technology has funded the conduct of this research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The datasets used during the current study are available from the corresponding author upon reasonable request.