
Abstract
Objectives
To explore the experiences of patients, carers, nursing students, and health care workers of the BOOST 2.0 implementation trial in the subacute geriatric rehabilitation ward and understand the factors influencing uptake and sustainability.
Methods
This research is a qualitative study using a thematic analysis approach. Semistructured individual and focus group interviews were conducted with various stakeholders who were involved in the implementation trial. A total of 11 focus groups and 31 individual interviews were included in the present study, which were recorded, transcribed verbatim, and coded using reflexive thematic analysis. After themes were constructed using open coding, they were presented using the Consolidated Framework for Implementation Research. Participant validation was conducted with members of the research team who were not involved with coding to ensure accuracy of the research findings.
Results
Three key themes were developed: (1) perceptions about the BOOST 2.0 intervention, (2) perceptions of the implementation strategy of BOOST 2.0, (3) BOOST 2.0 within the inner (ward) and outer (hospital) setting
Conclusion
This study provides insights into how the alternative health workforce can deliver health interventions in hospitals. Further research is needed to explore the effectiveness of using a diverse clinical workforce to deliver interventions that can improve outcomes for patients.
Introduction
The proportion of older Australians as part of the total population is increasing and is set to reach about 23% by 2066 (Australian Institute of Health and Welfare, 2024). By the age of 55, nearly 50% of older Australians will have some form of disability. Older persons represent a large proportion of people needing rehabilitation services, with an average age of those requiring rehabilitation being 75 years (Australasian Rehabilitation Outcome Centre, 2024). Falls, fractures, and deconditioning from other major illnesses are the most common impairment categories requiring rehabilitation in older Australians. Mobility and self-care without needing another person is the most common goal for rehabilitation programs for older persons and works best when delivered by a multidisciplinary team (Cameron & Kurrle, 2002). Furthermore, the complexity and dependency of patients admitted for rehabilitation are increasing, resulting in a need for more resources (McKechnie et al., 2020).
Review of Literature
Increasing patient engagement and therapy intensity can improve functional outcomes in older individuals, including improved mobility, independence in activities of daily living, and less risk of institutionalization (Lenze et al., 2012). Specific components of rehabilitation programs that can facilitate improved outcomes include family participation, nurse-led task-specific training, collaborative goal setting, and transdisciplinary involvement (Tijsen et al., 2019). There is evidence that alternative workforces, such as allied health assistants and preregistration physiotherapy students, can be used to increase therapy intensity in the setting of low-trauma hip fracture surgery (Kimmel et al., 2016; March et al., 2024).
The older patients in rehabilitation have the greatest interaction with nurses compared to any other rehabilitation clinicians, more so during weekends than weekdays (McKillop et al., 2015). Nurses in geriatric rehabilitation settings often have the role of a coach to increase independence in functional activities and solve the problems that patients may encounter in their rehabilitation journey (Guitar et al., 2023). There is potential for nursing students to be involved in enhancing rehabilitation care as part of the interdisciplinary rehabilitation team. This can enrich the nursing student's knowledge of the role of other clinicians in providing holistic care, with the potential to improve their confidence in communicating with other disciplines and improving patient care (Ho et al., 2022). Student nurse involvement in activities around the rehabilitation ward is useful for the extended rehabilitation team as they can educate and work with the patients and implement participation in meaningful activities, bring their unique perspectives and innovation, in turn improving the quality of care provided to the older adults (Deli Poggi et al., 2021; Pay & Sørbye, 2018). Therefore, this embedded qualitative research study (Kidder & Fine, 1987), within an implementation trial (BOOST 2.0), testing the effect of using nursing students and allied health assistants to increase therapeutic exercise frequency in a subacute geriatric rehabilitation ward, was undertaken to explore the experiences of the patients, carers, clinicians, and health service managers and understand factors influencing implementation.
Methods
Setting and Study Participants
This prospective qualitative study was part of the BOOST 2.0 implementation evaluation—a 3-month high-frequency exercise program in a subacute rehabilitation ward for patients over 60. Most participants were admitted post-hip fracture, falls, or medical deconditioning. Patients with elective surgeries or weight-bearing restrictions were excluded. The hospital serves a culturally diverse population, and interpreters were used as needed. Staff from multiple disciplines were invited to participate, though social work was unavailable. Pre-implementation surveys identified service delivery gaps.
Intervention
BOOST 2.0 explored the feasibility of using nursing students to implement sit-to-stand functional exercise during weekdays, in addition to standard physiotherapy care during the week. The goal was to provide two additional nursing student-led sessions lasting 15 to 20 min during weekdays. A single additional weekend exercise session was provided by an Allied Health Assistant (AHA) in the context of no routine weekend therapy. Chair-based and bed-based exercises were provided to support patient choice and engagement in exercise if they declined standing exercises. Usual care physiotherapy was a combination of group and one-to-one strength and balance exercises, mobility, and stairs training. The exercise sheet is available as Supplemental Appendix A. The exercises were adapted from a previous implementation trial in the acute setting following hip fracture surgery (March et al., 2024).
Implementation Strategies
The implementation included nursing student orientation via a PowerPoint presentation and practical demonstration by a senior physiotherapist (PT). Laminated exercise sheets were placed at bedside, and staff were oriented through in-services. Participant details were shared in daily multidisciplinary handovers and on the ward communication board. Nursing students received limited supervision from senior and ward PTs during placement.
Data Collection
Two separate semistructured interview guides were developed for patients/carers and staff, informed by the Consolidated Framework for Implementation Research (CFIR; Damschroder et al., 2022). The interview guides are available in Supplemental Appendixes B and C. Patient/carer interviews were conducted by two local clinician researchers of medical and physiotherapy backgrounds with prior knowledge in qualitative research methods and identified as female. Both worked in the ward and were responsible for providing part of the clinical care to some of the participants interviewed. The interviews were conducted within a week of discharge from the hospital as a face-to-face or telephone interview. Patient participants could choose to have a carer participate as a proxy or to be interviewed together. The interviews ranged from 15 min to 30 min.
Semistructured interviews and focus groups were conducted to gather the staff and student experiences. Insights were also gathered through interviews with the healthcare managers and steering committee members regarding the implementation of the study. A diverse group of staff stakeholders—including nursing student facilitators, coordinators, ward staff, multidisciplinary teams, consumer representatives, and the implementation team—were invited to participate in the qualitative study. Nursing students were approached postplacement, while other staff were invited after implementation. Participants could choose between focus groups or interviews, conducted either face-to-face or via Microsoft Teams. The selection of focus group participants was based on availability on the allocated dates. Perspectives were captured from over half of the permanent nursing staff, more than half of the nursing students, and all allied health and junior medical staff during the implementation period.
The staff and student interviews were completed by four clinician researchers from medical and physiotherapy backgrounds and one consumer representative, all of whom identified as female. Eight focus groups were conducted for the nursing students, with three students in each group. Two focus groups were conducted for nursing staff, with two members in one and three members in the other. A focus group was conducted for PTs with two members. The duration of the interviews and focus groups varied between 20 min and 1 h.
Data Analysis
Four authors were involved in the data analysis, with two authors independently coding data from one group of participants (patients/carers and staff). Codes were compared within each participant group and discussed with the coders and the lead author. Codes were grouped and then constructed into themes for each group of participants. Themes from both groups were compared, discussed, and interpreted by the authors involved in coding and the local project steering committee (Ramanadhan et al., 2021). In view of the alignment of themes between both participant groups, themes generated from patient/carer and staff groups are presented together. To aid interpretation for the reader, themes are presented as they align with relevant CFIR domains, as there were many context-specific experiences explored that need conceptual scaffolding for a global audience. Microsoft Excel was used to manage and sort the data.
The four authors involved in data analysis bring a range of perspectives to this analysis. SR is a rehabilitation physician providing clinical care, MM is an Australian-trained senior PT and postdoctoral researcher external to the implementation site, and AD is currently a graduate PT and researcher involved in BOOST 2.0 implementation. During the study, AD was the AHA involved in providing weekend exercise therapy to participants as part of this study. AV is a junior doctor who was also trained as a Registered Nurse (RN) and provided clinical care on the ward after implementation.
The results were presented and discussed with the wider rehabilitation team for participant validation. The results were not validated with the nursing student cohort, as they no longer had postings in the facility, nor with the patient and carer cohort. The consumer representative who was part of the project steering committee and had a carer role in the past was able to comment on the patient and carer perspective. All eligible participants were approached for participation, with no restrictions or limitations based on data saturation. During implementation and postimplementation, the project steering committee held regular meetings to reflect on implementation strategies, data collection, and analysis. Minutes from these meetings, kept by the lead author, alongside reflective diaries from the coders involved in analysis, helped to bring reflexivity and provided an audit trail (Finlay, 2021).
Ethical Considerations
This study was reviewed and approved by the Local Health District Ethics committee (2023/ETH00809). Informed consent was obtained from staff, students, and clinicians to participate in individual interviews or focus groups.
Results
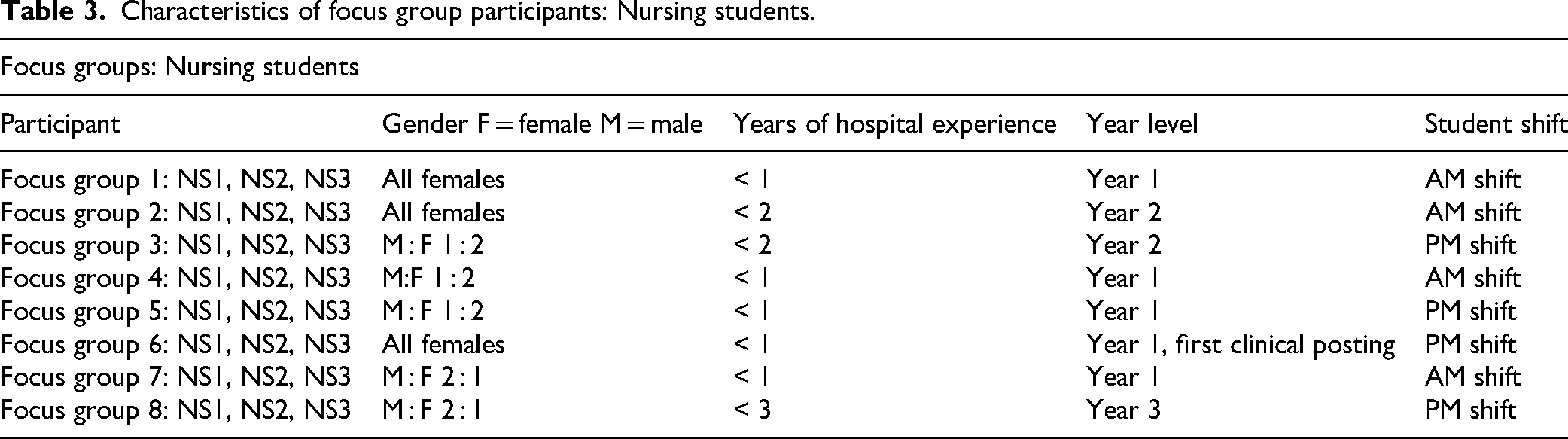
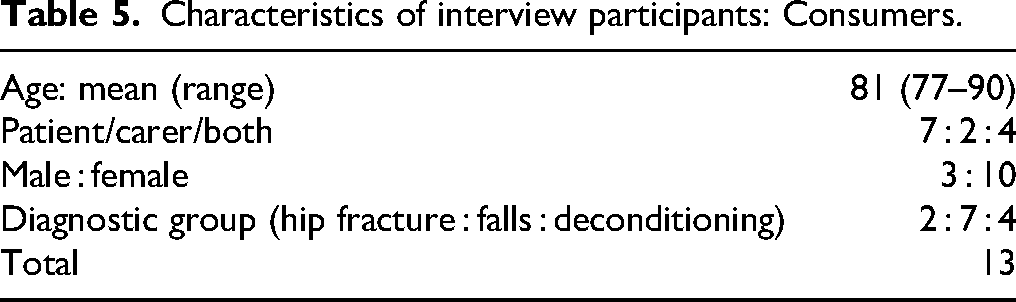
The characteristics of participants who completed the interviews are presented in Tables 1 to 5. The staff interviewed were mostly female, comprising individuals with a wide range of experience from newly graduated nurses to seasoned professionals with more than 20 years of experience. The nursing students were mainly from the first year of training, majority were female. The patient cohort was largely female than male, with falls being the most common diagnostic category. Eleven focus groups and 31 individual interviews were completed, and in total, 62 participants provided their insights.
Characteristics of interview participants: Nursing students.

Characteristics of interview participants: Staff.

Characteristics of focus group participants: Nursing students.
Focus group composition staff.

Characteristics of interview participants: Consumers.
Themes
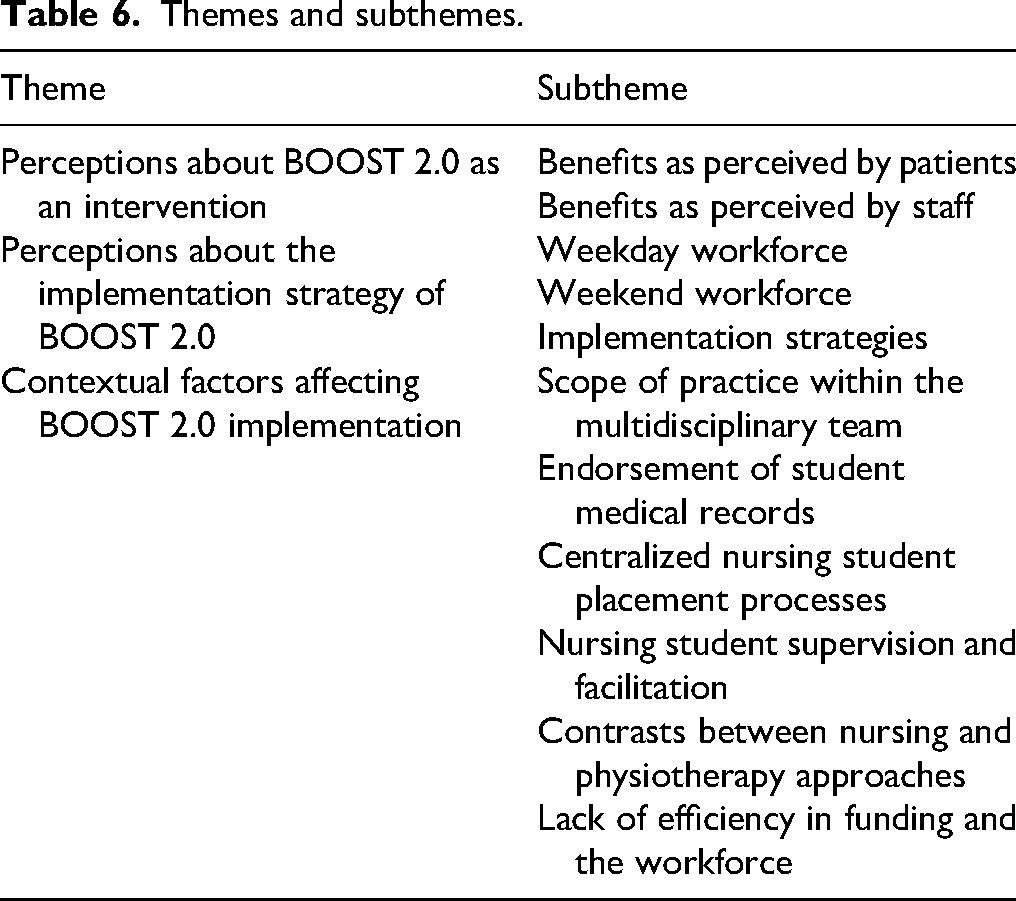
Three major themes were developed: (1) perceptions about BOOST 2.0 as an intervention, (2) perceptions about the implementation strategy of BOOST 2.0, and (3) contextual factors affecting BOOST 2.0 implementation. Table 6 gives a summary of the themes and subthemes.
Perceptions about BOOST 2.0 intervention
Themes and subthemes.
A wide range of staff stakeholders perceived BOOST 2.0 positively, with benefits for patients, nursing students, and the rehabilitation service. The intervention was perceived to address the sedentary behavior of inpatients. I think it's been really beneficial for the patients because they're lying in bed constantly, it's not ideal. (Nursing Student, Focus Group 1) Especially in the ward they are in bed a lot. Lying down sitting down and everything. Just doing and having that extra exercise time is a good thing. (Nursing Student, Focus Group 5) … you don't really need a background in this… if someone came in with like no knowledge, it would be pretty straightforward. (Nursing Student, Focus Group 5) …it was very useful to get the patients in the mindset that they are here for therapy. [Physiotherapist (PT)] I think transfers like, getting in and out of bed… it improved a lot quicker and I think that [they] were quite familiar with the what the exercises were for. They have more opportunities to practice that. [Occupational Therapist (OT)] … it saved time off their discharge because it meant they'll probably be more robust by Wednesday as opposed to being more robust by Friday. (Medical Registrar) When you're introducing programmes like this, you'll see patients [spend] less time in hospital and overall improvements. (Nursing Student, Focus Group 7)
BOOST 2.0 also provided unexpected benefits, such as increased opportunity for social interaction and engagement with meaningful activities. Patients highly valued these increased interactions with staff. It was something to do apart from just being in bed all the time. (Patient 6)
The nature and wide range of recovery trajectories during admission and after discharge from the hospital were highlighted by the patient and carer participants. Many patients found exercise to be challenging initially, but their mastery improved over time. Carers observed improvements in the mobility, confidence, and independence of their loved ones with ongoing exercise. Some patients reported that there was a day-to-day fluctuation in their ability to participate in exercise, and carers were unable to observe improvements over time. I think we've noticed now that she's at home, she'll get up and try to take a couple of steps to the bed… So obviously those leg exercises are helping her with mobility. (Carer 11) One day she could, and then the next day she couldn’t, sort of thing, so it helped a bit but – yeah… (Carer 10) But I am old now, I can’t do much. (Patient 9) I think for her age is quite challenging for her because she came there and the recovery was quite slow. (Carer 3) I think getting patients early in the acute phase and ensuring that they don't deteriorate for the basic functions [like] going to the bathroom, sitting out of bed, catching them very early is probably the biggest potential mitigating factor to preventing a rehab admission. (Medical Registrar) …it really depends on the criteria, because rehab… it kind of makes sense, but then in other wards they might still be trying to get better from their own illness that they're diagnosed with… [Registered Nurse (RN) 3] With the exercise, I'm hoping that's going to help the muscles and everything in my leg. That's the main reason I want to try and keep them up. (Patient 13) I'm terrified of falling. That's why I hardly like to do so many things… but I'm hoping I might be able to do a bit more than what I came in here to do to help myself to prevent this. (Patient 12)
Perceptions about the implementation strategy of BOOST
The implementation of BOOST involved recruiting two alternative workforces to deliver the exercise sessions: nursing students and allied health assistants. Reflections about the effectiveness of these workforces revealed several facilitators and barriers in their respective uptake and implementation of BOOST.
Weekday Workforce: Nursing Students
Most nursing students did not feel confident implementing BOOST 2.0. Nursing students identified patient-related risk factors such as frailty as a key barrier, noting the potential for adverse events, including falls. This led to questioning around exercise and the nursing scope of practice. This was noted particularly in first- and second-year nursing students. I wasn't confident enough to actually help them, like mobilise because I wasn't sure what I can and can't do with them. (Nursing Student, Focus Group 2) …like they [were] really like frail and we don’t feel confident. (Nursing Student, Focus Group 6) I just happen to know from like doing things outside of like physical activity in gym. I understand what each type of exercise is. (Nursing Student, Focus Group 1) … if we focus on the BOOST project a lot, then we can't do meds or other routines, so that delays everything. (Nursing Student, Focus Group 8) It's just when if nurses need us to do like a bed change or bed pan or something. Kind of need to go to that first. (Nursing Student, Focus Group 1) … maybe a focus on how we sell it to the RN's to incorporate it into their day and well into the students day with the RN support, but I think it might be a bigger culture, nursing culture thing as well. [Nurse Unit Manager (NUM)] … maybe the ward physio, but I know they all communicate in that, but maybe join some of the meetings. (NUM) … with the involvement of the student nurses especially, it makes work a bit lighter and easier and also we can attend to more immediate things like patients who are clinically unwell. (RN 4) I think it's also beneficial for us as well, like as students like we're new to the workforce, so it builds confidence in us in communicating to patients. (Nursing Student, Focus Group 7) … this is like insight into OTs and physios, like their speciality. (Nursing Student, Focus Group 3)
Weekend Workforce: Allied Health Assistants
I guess the advantage of using AHAs that were already on the books is they have that orientation and exposure… it's all activities they're familiar with. (PT Manager) …if [the] AHA is doing it… they know that it's [a] type of exercise. (OT) I thought it was a very useful way to maintain mobility in patients if they couldn't have weekend physiotherapy, which was often the case. (Medical Registrar) They were like they had nothing else to do, so they were looking forward to seeing someone, you know, come and do some sort of activity. [Allied Health Assistant (AHA) 1] I'm just using more prompting on how to perform the exercises correctly, like for sit to stands, making sure that they are placing their hands on the armrest and that their feet are positioned correctly before they do the stand. (AHA 2) I think sometimes the nursing students, when a patient declines, they're not as pushy. They wouldn't push patients, but they would leave it. (OT)
Implementation Strategies
To support implementation, printed exercise handouts customized for each patient were affixed to the patient's bedside. These were clear, easy to read, and demonstrated the exercise for those with cognitive impairment or cultural diversity. These handouts prompted patients, ward staff, and families regarding engagement in BOOST 2.0 exercise outside of business hours. With one of the patients, it was mostly visual communication, like Bed 9. He was sort of just mirroring my movements. (Nursing Student, Focus Group 8) Just having the sheets there to prompt them as well or prompting family was good. (AHA 1) It was just a lot more motivating having someone there rather than being told to do it on their own. (AHA 2)
BOOST within the inner setting (ward)
Reflection during data analysis initially considered the hospital ward as the inner setting, with the organization, health system, and professional factors as the outer setting. However, many of the themes generated had implications across both inner and outer settings, so they were grouped together across contexts.
Scope of Practice Within the Multidisciplinary Team
Relationship dynamics between healthcare workers on the ward played an important role in implementation outcomes. Reflections about other disciplines revealed a range of perspectives on the roles of different health professions in the rehabilitation context and the implementation of BOOST 2.0. Some nurses and nursing students considered the BOOST 2.0 intervention as solely within the scope of physiotherapy, as it was exercise-based. …being that it's exercises, they kind of align that with being physio and that's not their role to take that kind of thing… (NUM) Because we're not physios, are we doing the right thing like we have to learn to be nurses… Is this appropriate for us to do as students? (Nursing Student, Focus Group 8)
Endorsement of Student Medical Records
A common issue amongst nursing staff was who would be responsible for the endorsement of nursing student documentation for BOOST 2.0 interventions. Nurses expressed concerns about signing student notes without having observed them delivering the session, or a lack of understanding of the intervention, and believed it was more appropriate for the PT to endorse. However, the design of the electronic medical record systems limited endorsement of nursing student documentation by a non-nursing health professional. So we were worried, our question was, are we the one signing the notes up because we are [not] physios. (Senior RN 1)
Centralized Nursing Student Placement Processes
There is a complex, centralized system for determining nursing student placements at the facility. This includes over 30 educational institutions requesting placements for four levels of nursing qualifications. Decisions regarding placement offers and approvals are made by a centralized placement manager 6 months ahead of the placement based on a range of factors for multiple hospitals across a health district. The subacute ward context tended to have nursing students early in their degree on short placements (2 weeks), as students nearer graduation tended to be assigned to placements in critical care instead of rehabilitation. … if they have a three-year student on their very last placement, they probably not going to choose 1B [rehab ward] right? (Student Placement Manager) It differs from different education providers and the time spent is determined by the education providers as well. (Student Placement Manager)
Nursing Student Supervision and Facilitation
Nursing student supervision was fragmented, involving ward nurses, facility-based facilitators, and external assessors with no coordinated communication or scheduling. Students prioritized external facilitators as they assessed performance. The external facilitators were difficult to engage for BOOST 2.0. Ward staff felt disempowered in guiding student learning, especially when students declined participation in tasks. This ad-hoc approach to nursing student supervision limited the effectiveness of BOOST 2.0 implementation. It's just those times when facilitator will just pull them out from on the floor and I'm like it's just like where are my student gone? (RN 4) How little sort of control or influence the actual ward-based nurses have over that whole process and the learning of those student nurses. (PT Manager) … we don't have a lot of say or supervision power over them in the sense of the entire placement and ability to like encourage them to participate in general. (NUM)
Contrasts Between Nursing and Physiotherapy Approaches
Key nursing and physiotherapy stakeholders noted that differences in student placement structures affected implementation. In contrast to nursing student placements, PTs providing student supervision had the capacity to determine appropriate learning activities, assess and provide feedback to students, and the key student supervisor was determined at the beginning of their five-week placement. … engagement with the nursing students and their facilitators was not what we had originally expected… I think we went in there thinking that student placements ran quite similarly between disciplines. (PT Manager) … they observe the RN in all their duties and then they're supervised administering medication or doing personal cares or documenting… this is very different to the allied health where they might be supervised, assessed, given feedback, reported on and do that cycle again… (NUM) … that made it so, it feels like there's a lot of work that's put in but not a lot outcomes. (PT Team Leader) … it seems like it's a physio, potentially an OT activity more similar rather than nursing because nursing seems quite a big gap to bridge. (PT Team Leader)
Lack of Efficiencies in Funding and Workforce
Existing processes for recruitment and remuneration of staff using project-based funds were onerous and did not fit with funding timelines. A successful strategy was to increase the hours of existing staff, rather than employing new staff; however, this limited the hours available for BOOST 2.0. … [can be] extremely difficult and time consuming, and to set things up so they can actually be paid properly, particularly through project funds. (PT Manager)
BOOST 2.0 implementation was impacted by the lack of a funded senior PT and dedicated allied health assistants on the ward. This limited consistent leadership and continuity, affecting both routine care and project success, especially amid physiotherapy staff turnover. I think I would have needed a consistent person to drive it. (PT Team Leader) … if we could get more and allied health assistance and regularly just post it to Ward 1B it would help to provide more consistent therapy but obviously that requires change in budget. (Rehabilitation Consultant) … within the constraints of this Hospital, I don't know if [weekend physiotherapy] that's possible. (Medical Registrar)
Discussion
This study found that BOOST 2.0 was mostly positively received by its stakeholders. The intervention was perceived to bring several benefits to staff, patients, and the implementation setting, including skills development, increasing opportunities for therapy, and facilitating quicker discharges from the hospital. Despite this, not all implementation strategies were effective. AHAs helped to maximize consistency of therapy through weekend BOOST sessions and experienced greater ease with implementation. On the other hand, nursing students faced greater challenges with uptake and consistent implementation due to placement priorities and a lack of clinical experience and training, which affected their confidence. A lack of awareness of the intervention on the floor revealed shortcomings in the visibility and communication of BOOST 2.0 across the implementation period, which led to a lack of buy-in by nursing staff and facilitators. Finally, funding and recruitment constraints limited the scale of the intervention, while perceived roles of healthcare workers held by students and staff revealed barriers that impacted stakeholder readiness to endorse and implement BOOST 2.0.
The pre-implementation survey provides context for how the findings can be applied. The key stakeholders identified that more training, resources, and enhanced communication were important to improve the care provided. Only one in four of the staff who responded to the survey were aware of the guidelines for therapy provision in rehabilitation, and even fewer thought the current resources were able to provide the therapy necessary to meet those standards.
The results of this project add to the existing evidence regarding the acceptability and efficiency of extra weekend therapy in subacute care to improve function and hospital length of stay, regardless of workforce (Caruana et al., 2022; Ogawa et al., 2024; Sarkies et al., 2018; Snowdon et al., 2024). The implementation of weekend therapy in rehabilitation wards is inconsistent, despite clinical guidelines (Caruana et al., 2018; Queensland Clinical Senate, 2015). This project highlighted the impact of weekend and weekday clinical routines on the implementation of additional therapy. Patients and carers valued weekend therapy for both physical and social reasons, and weekend staff perceived implementation to be more efficient as there were no competing demands for patient time. Imperatives to develop “seven-day services” need to consider whether the current advantages of weekend clinical routines would be lost during implementation (Sommer et al., 2019).
The project highlighted the impact of nursing student supervision on the implementation of interventions by nursing students. The model in the current context used an ad hoc combination of ward nurses, facility-based facilitators, and external facilitators employed by a university. Although a range of supervision models have been described (Franklin, 2013), no single model has been established as superior, with different models conferring different benefits to students (Ekstedt et al., 2019). The key ingredients for a successful model include an explicit structure for student supervision, approachable staff who are open to students, collaboration between peers, supervisors, and facilitators, and a sense of belonging (Antonsen et al., 2023; Hellström-Hyson et al., 2012; McLeod et al., 2021; Sweet & Broadbent, 2017). The ad-hoc model used and the lack of communication between all staff involved in nursing student supervision adversely affected the implementation of the project. Future implementation needs to consider how the current models of student and staff supervision vary for each discipline and tailor strategies accordingly.
The results have highlighted the issue of functional exercise and discipline scope of practice. Many nursing students reflected that BOOST was not in their scope of practice and was a better fit for physiotherapy or occupational therapy colleagues, noting clinical risks they felt unable to mitigate, such as falls. However, these students did not reflect on how functional exercise replicated activities of daily living, which were within the nursing scope of practice. Reflecting on the scope of practice and delegating within this scope is a key outcome of the Australian Nursing Standards Assessment Tool (Ossenberg et al., 2020), and these views perhaps reflect those of emerging practitioners. In their most recent guidelines, the Association for Rehabilitation Nurses (USA) outlines “promotion of health and successful living” and “interprofessional team care” as two key domains of a rehabilitation nursing professional role (Vaughn et al., 2016). Both involve physical activity, so further reflection by nursing students and facilitators on the scope of practice of rehabilitation nurses may be a useful learning strategy for those involved, as well as a potential implementation strategy for future projects involving the implementation of physical activity using a nursing workforce.
Enhanced rehabilitation programs focusing on education, increased activity, and environmental changes that promote activity have been shown to improve long-term outcomes for hospital-acquired deconditioning (Smith et al., 2020). When the goals and value of additional therapy are better explained and understood, some of the concerns about individual role delineation could be less important (Perkins et al., 2007); an education process to increase understanding and acceptance of this programme may assist in changing the perspective of the staff, patients, and carers.
There was a wide range of confidence among nursing students in manual handling skills, despite this being identified by senior nursing stakeholders as a basic nursing skill appropriate for novice students. Previous work has explored solutions developed by PTs for nurses regarding safe manual handling in the context of patients with fall risk (Brusco et al., 2023; Kugler et al., 2023).
Although many patients and carers valued the BOOST intervention in achieving functional goals and hospital discharge, for some, there was no discernible benefit. This was often in the context of patients experiencing symptoms of severe frailty; however, there were no standardized approaches using frailty assessment or screening in this context. This aligns with existing evidence on the value of exercise in end-stage frailty (Kim & Rockwood, 2024), when the focus should be on physical activity to the level of individual patient tolerance, with a goal of providing comfort, rather than improvement in physical function. However, patients experiencing end-stage frailty, at or approaching the last 12 months of life, were not identified, and opportunities for shared decision-making regarding goals of care were not taken. Future research needs to consider how and when shared decision-making processes occur in the context of frailty, particularly in the inpatient rehabilitation context. This may include leveraging the skills provided by allied health professionals in assessment and communication, providing concrete examples of the impact of frailty on quality of life.
Strengths
A pragmatic, inclusive approach to consumer participation was adopted within the resources of the study, and a broad range of consumer perspectives was captured. Consumer perspectives were also represented on the study steering committee. A wide range of staff stakeholders across four disciplines were interviewed, making it likely that data saturation was achieved. The perspectives of more than half of the nursing students and approximately 80% of the staff working in the subacute ward during the implementation period were captured.
Limitations
The results of this study need to be considered in the context of some potential limitations. The patient and carer population catered by the service is culturally diverse, and this study had some scope to use interpreters. However, due to difficulties using phone interpreters in an elderly population, all the interviews with patients and carers except one were conducted with those who were fluent in English but spoke a language other than English at home. One patient interview was conducted with an Italian interpreter. Though maximum variation sampling was used to understand staff and student perspectives, a convenience sample was used for patient and carer interviews due to practical considerations. These may have limited the depth of reflection and reporting from patients and carers (Luborsky & Rubenstein, 1995). The individual transcripts were not returned to most of the participants due to time limitations and other practical implications due to rotating staff. However, the key findings from the interviews were summarized and presented to different staff members who participated in the interview and to the consumer group to receive feedback.
Implications to Practice
Preregistration nursing students can be a potential additional asset to engage patients in functional activities, but require more education on the role of nurses in a geriatric rehabilitation context. This requires changes to the clinical posting blocks to enable building confidence in communication and manual handling skills. System-level changes are required to improve models of supervision for nursing students in a rehabilitation context, as well as to change perceptions of their place in an interdisciplinary environment.
Conclusion
In conclusion, the intervention in Boost 2.0 was mostly positively received by its stakeholders and was perceived to bring several benefits to staff, patients, and the implementation setting, including skills development, increasing opportunities for therapy, and facilitating quicker discharges from the hospital. Despite this, not all implementation strategies were effective. Further investigation is needed to explore interventions that can be implemented to improve outcomes among older rehabilitation patients, given the opportunities to use a diverse clinical workforce, which includes student nurses.
Supplemental Material
sj-docx-1-son-10.1177_23779608261425203 - Supplemental material for BOOST 2.0: Feasibility of Using the Nursing Student Workforce to Increase Activity: A Qualitative Study
Supplemental material, sj-docx-1-son-10.1177_23779608261425203 for BOOST 2.0: Feasibility of Using the Nursing Student Workforce to Increase Activity: A Qualitative Study by Annabel Darmali, Seema Radhakrishnan, Christina Eagleton, Minh Pham, Sarah Faulds, Carmen Lazar, Anniella Vashti, Friedbert Kohler, Rebecca Ivers and Marie K. March in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608261425203 - Supplemental material for BOOST 2.0: Feasibility of Using the Nursing Student Workforce to Increase Activity: A Qualitative Study
Supplemental material, sj-docx-2-son-10.1177_23779608261425203 for BOOST 2.0: Feasibility of Using the Nursing Student Workforce to Increase Activity: A Qualitative Study by Annabel Darmali, Seema Radhakrishnan, Christina Eagleton, Minh Pham, Sarah Faulds, Carmen Lazar, Anniella Vashti, Friedbert Kohler, Rebecca Ivers and Marie K. March in SAGE Open Nursing
Supplemental Material
sj-docx-3-son-10.1177_23779608261425203 - Supplemental material for BOOST 2.0: Feasibility of Using the Nursing Student Workforce to Increase Activity: A Qualitative Study
Supplemental material, sj-docx-3-son-10.1177_23779608261425203 for BOOST 2.0: Feasibility of Using the Nursing Student Workforce to Increase Activity: A Qualitative Study by Annabel Darmali, Seema Radhakrishnan, Christina Eagleton, Minh Pham, Sarah Faulds, Carmen Lazar, Anniella Vashti, Friedbert Kohler, Rebecca Ivers and Marie K. March in SAGE Open Nursing
Footnotes
Acknowledgements
The authors would like to acknowledge the Physiotherapy Department, Fairfield Hospital, Prof Steve Frost, School of Nursing, University of Wollongong, School of Nursing, Western Sydney University, School of Nursing, Australian Catholic University, and School of Nursing, University of Technology, Sydney for this study.
Ethical Consideration
This study was reviewed and approved by the SWSLHD HREC (2023/ETH00809). Informed written consent was obtained from all participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Seed Grant in 2023 from the University of New South Wales Ageing Futures Institute.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The de-identified data will be made available if requested, pending approval from the South Western Sydney Local Health District.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.