
Abstract
Introduction
Hospitalization is a critical period for older adults. It can lead to functional and psychosocial decline, subsequently affecting their quality of life (Loyd et al., 2020; Mendes et al., 2023). These impacts may stem from factors intrinsic to the illness causing hospitalization and the aging process itself, as well as extrinsic factors related to hospital routines (Mendes et al., 2023).
Consequently, transitioning home after discharge is challenging for older adults. Re-adapting to daily life can be difficult due to the illness's effects and the need for ongoing recovery care (Sousa et al., 2023). This transition process can cause insecurity for both the older adult and their family, who often take on caregiving roles. This insecurity may stem from a lack of knowledge about clinical status, prognosis, and treatment options (Hestevik et al., 2019; Sousa et al., 2023). This was also evidenced in a qualitative study with Chinese older adults experiencing the transition process. Negative feelings, such as uncertainty, worry, depression, loneliness, and despair, were associated with knowledge gaps, persistent symptoms, negative experiences in previous transitions, and fear of coping with adverse events at home (Sun et al., 2023).
The purpose of care transition is to ensure continued, comprehensive, individualized, and safe care. Effective transitions aim to reduce unnecessary healthcare system use and complications. They also strive to improve user satisfaction and communication with the healthcare team (Fundação Oswaldo Cruz [FIOCRUZ], 2023). To achieve this, transitions should utilize strategies like health education. Such education prepares the older patient, family, and caregivers to manage home care post-discharge. This preparation aims to foster the older adult's independence and autonomy whenever possible (Tomazela et al., 2023).
According to the World Health Organization (WHO, 2016, p. 3), the concept of care transitions, as adopted in this study, encompasses: the various points where a patient moves to, or returns from, a particular physical location or makes contact with a health care professional for the purposes of receiving health care. This includes transitions between home, hospital, residential care settings and consultations with different health care providers in out-patient facilities.
Each transition has unique specifics depending on the origin and destination contexts, requiring coordination among professionals and services. Within the hospital setting, transitions can occur between teams in the same department, between different departments, between hospitals, and finally, to home care (discharge) (FIOCRUZ, 2023).
For the hospital-to-home transition specifically, discharge planning is crucial. This planning should involve the individual and their support network as central agents in creating the care transition plan. This plan should be developed through collaborative action by the multidisciplinary team (Aued et al., 2019). Nurses are recognized as key professionals in coordinating this process. Their focus on patient- and family-centered care, guidance, education, and promoting change makes them pivotal. Consequently, nurses often serve as the link between different levels of healthcare (Aued et al., 2019; Petrocini et al., 2022; Sousa et al., 2023).
The nurse's holistic view of individual and family needs is crucial for systematizing and formulating this plan. To achieve this, nurses utilize the nursing process (NP), the methodological tool that structures and documents their work. The NP consists of five stages: assessment, diagnosis, planning, implementation, and evaluation (ADPIE) (Pesut, 2006). This process aligns with current Brazilian legislation from the Federal Nursing Council (Conselho Federal de Enfermagem [COFEN], 2024).
Several factors influence the development and implementation of the NP. High nursing workloads can compromise discharge planning and patient/caregiver guidance. Flawed communication between different healthcare levels often hinders care coordination post-discharge. Treatment adherence is challenging, particularly for older adults with physical/cognitive limitations or lacking social support. Finally, social and economic barriers and low health literacy must also be considered, as they can impact the execution of discharge planning (Dolu et al., 2021).
Given these challenges, there is an urgent need for evidence to clarify and guide NP implementation for this population. Such evidence is vital due to the nurse's important role in planning and implementing interventions that support effective, needs-based care transitions for older adults. Preliminary research in the Joanna Briggs Institute (JBI) Evidence Synthesis, The Cochrane Database of Systematic Reviews, and Campbell Library databases has not identified publications focusing on this topic to date.
The objective of this research was to map and synthesize scientific evidence on the nursing process applied to older adults undergoing the care transition from hospital to home. To formulate the research question, the Population, Concept, and Context (PCC) strategy was adopted, where P = older adults; C = nursing process; C = hospital-to-home care transition. Therefore, the guiding question of this study was: What is the scientific evidence on the nursing process applied to older adults in the care transition from hospital to home?
Method
This study employs a scoping review methodology, guided by the recommendations outlined in the JBI Reviewer's Manual (Peters et al., 2020).
Protocol and Registration
The protocol and report for this research were developed following the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines (http://www.prisma-statement.org/Extensions/ScopingReviews). The final protocol was registered with the Open Science Framework (OSF) on April 13, 2023.
Eligibility Criteria
Eligible sources included original articles, case reports, case series, opinion/reflection articles, theses, and dissertations. These sources needed to address how the nursing process is developed for older adults during the hospital-to-home care transition. Sources were required to cite at least one stage of the NP. Additionally, included studies needed to be written in alphanumeric characters to facilitate translation. Exclusion criteria included review articles, letters to the editor, and sources not fully accessible. Sources were considered inaccessible if the full text could not be obtained via remote access (e.g., Federated Academic Community [CAFe] portal) or direct author requests (e.g., ResearchGate). No time limits were applied for publication dates. Duplicate records were considered only once.
Sources of Evidence
Searches were conducted in the following databases: National Library of Medicine (PubMed), EMBASE, Latin American and Caribbean Literature in Health Sciences (LILACS), Web of Science, SCOPUS, and Livivo. For gray literature, Google Scholar and the CAPES Theses and Dissertations Catalog were consulted.
Search Strategy
The search strategies were initially developed by the first author. They were subsequently reviewed by the research team, a librarian, and an expert in review methods. Strategies were discussed and refined through meetings. The specific search strategies and filters used in the databases are presented in Figure 1.
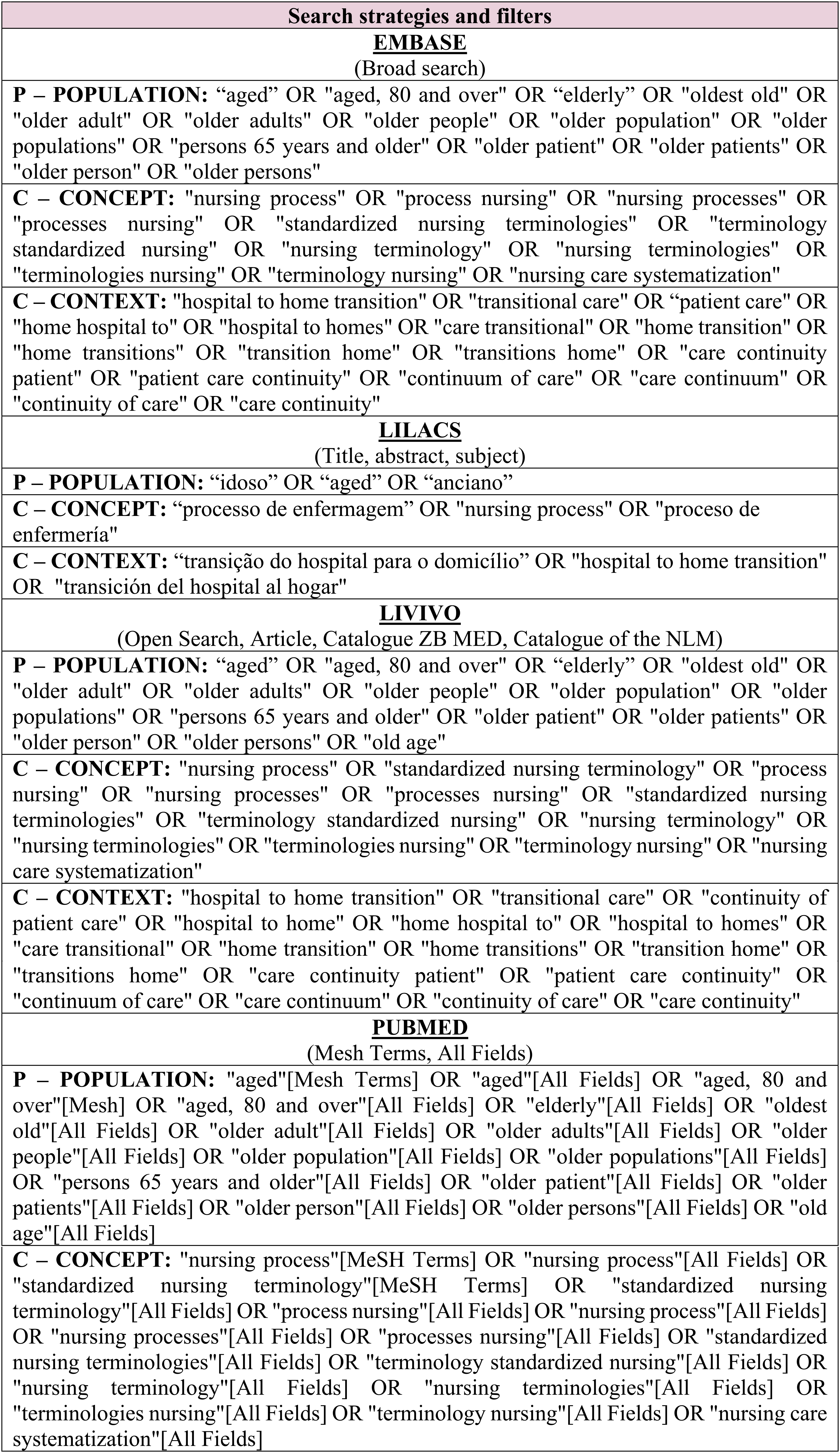
Search strategies and filters used in the databases.
The database searches were conducted on April 12, 2023, and the gray literature search on September 1, 2023. The searches were updated on March 6, 2025, except in the Livivo database due to a system error encountered during the search process.
Selection of Sources of Evidence
For source selection, references identified from database searches were first imported into EndNote (https://access.clarivate.com/login?app=endnote) to identify and remove duplicates. The remaining references were then imported into Rayyan (https://rayyan.qcri.org/welcome) for further automated analysis; duplicates were also manually reviewed and excluded at this stage. Titles and abstracts were independently reviewed by two researchers to identify sources that met the inclusion criteria and addressed the research question. Sources selected at this stage proceeded to full-text review and analysis.
Data Extraction Process
A Microsoft Excel® spreadsheet was created for data extraction, designed to capture variables relevant to this research. Reviewers were trained in the extraction process, and a pilot test was conducted to standardize information collection and refine the spreadsheet. The spreadsheet included several categories of items. These were: publication characterization (author, title, year, venue, country); research objectives; reasons for exclusion; methodological characteristics (study type, setting, population/sample/participants); evidence on NP/care transition (frameworks, explicit NP mention (yes/no), NP stages addressed, standardized language used, data collection instrument, diagnosis, planning, implementation, evaluation, other results/conclusions); and other data, such as study limitations. This extraction process was carried out independently by reviewers, with any discrepancies resolved through consensus meetings.
Data Analysis/Synthesis
Results were presented using figures and descriptive analysis, including frequency distributions (absolute numbers and percentages). The main results and conclusions from the included sources were analyzed and synthesized using a deductive approach, guided by theoretical references (Braun & Clarke, 2006). Thematic categories were pre-defined based on the Nursing Process definition and its stages (ADPIE acronym) (Pesut, 2006). Similar data across sources were grouped and numerically described. Nursing diagnoses were classified according to the latest NANDA International edition (NANDA-I, 2021). Nursing intervention prescriptions were classified using the Nursing Interventions Classification (NIC) (Butcher et al., 2020). Adjustments were made to align reported data with the updated nomenclature of these taxonomies. Finally, the nursing diagnoses identified in the sources were grouped according to the NANDA-I Taxonomy domains.
Results
The searches yielded 3,544 sources of evidence. Of these, 101 were excluded as duplicates. After reviewing titles and abstracts, 3,315 sources were excluded for not meeting the inclusion criteria, leaving 128 sources for full-text review. From this group, 117 were excluded because the full text was unretrievable (n = 13) or the source failed to meet all PCC criteria (n = 104). Ultimately, 11 sources of evidence were deemed eligible for inclusion (Figure 2).

Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) flowchart for sources of evidence selection.
Figure 3 provides a summary of the characteristics of the included sources, detailing author, title, year, country of publication, and standardized language used.

General characteristics of the eligible evidence sources for the scoping review, including author, title, publication year, country, and standardized language.
Among the 11 included sources (100%), nine were articles (81.8%) and two were dissertations (18.2%). The publication period spanned from 1993 to 2022. Notably, two sources (18.2%) were published in 2012, and three (27.3%) were published within the last five years (relative to the 2025 update search). Most sources originated from the United States (6, 54.5%), followed by Brazil (3, 27.3%) and England (2, 18.2%).
Regarding taxonomies, six studies (54.5%) mentioned using at least one taxonomy during a stage of the NP. The most frequently cited were as follows: NANDA-I (5, 45.4%), NIC (3, 27.3%), NOC (2, 18.2%), and the Omaha System (Problem Classification Scheme and Problem Rating Scale for Outcomes) (1, 9.1%) (Figure 2).
Notably, only two sources (18.2%) specified theoretical frameworks supporting the NP: the Self-Regulation Theory (Cossette et al., 2012) and Gottlieb's Strength-Based Care Theory (Manara, 2021).
Among the included sources, six (54.5%) reported using instruments during the initial assessment (data collection) stage. A total of 15 different instruments were cited across these sources. These instruments collected data on various aspects, including: demographic variables, caregiver preparation, functional dependencies, cognitive/physical/mental function, therapeutic/medication adherence, self-management, discharge needs, and learning (Karpiuk et al., 1997; Manara, 2021; Morrison et al., 2016; Rosted et al., 2012; Sampson & Doran, 1998; Shyu et al., 2008). Further details on these instruments are available in Figure 4.

Description of the data collection instruments used in the evaluation stage of the sources of evidence selected for the review, according to the respective references.
The diagnosis stage was mentioned in five (45.4%) of the 11 sources (Brito, 2022; Karpiuk et al., 1997; Lemos et al., 2020; Manara, 2021; Sheppard, 1993). Figure 5 presents the diagnoses identified in these sources, categorized according to NANDA-I (2021) domains.
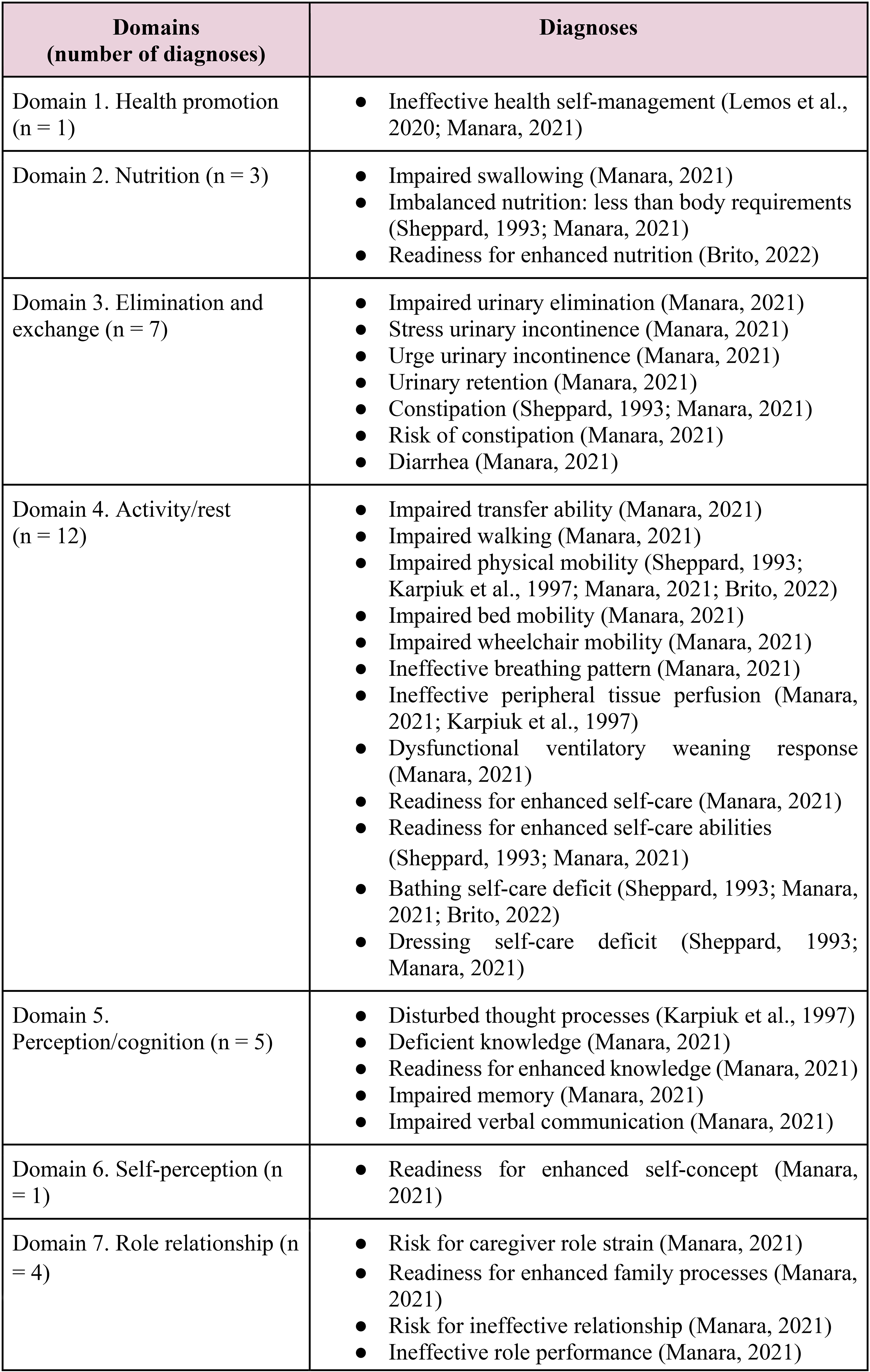
Description of nursing diagnoses, according to the NANDA-I domains, that were mentioned in each source of evidence.
A total of 54 distinct nursing diagnoses were identified across these five sources. Analysis by domain revealed that diagnoses related to Domain 11—Safety/protection (14; 26.0%), Domain 4—Activity/rest (12; 22.2%), and Domain 3—Elimination and exchange (7; 13.0%) were predominant (Figure 4). No diagnoses related to Domain 8—Sexuality, Domain 10—Life Principles, or Domain 13—Growth/development were identified.
Regarding the planning stage, only two sources (18.1%) mentioned using the NOC taxonomy to determine expected outcomes. One source listed outcomes such as Teaching: Disease Process, Teaching: Prescribed Medication, and Teaching: Prescribed Diet (Lemos et al., 2020). The other listed outcomes including Mobility, Knowledge: Pain Control, Self-care (Bathing, Eating), Knowledge: Infection Control, Fall Prevention Behavior, Vision Compensation Behavior, and Body Mechanics Performance (Brito, 2022).
For nursing interventions/prescriptions (planning stage), based on NIC, the most common interventions were as follows: Health Education (Brito, 2022; Cossette et al., 2012; Karpiuk et al., 1997; Lemos et al., 2020; Manara, 2021; McCauley et al., 2006; Morrison et al., 2016; Shyu et al., 2008); Referral to Health Resources (Brito, 2022; Cossette et al., 2012; McCauley et al., 2006; Rosted et al., 2012) or assisting families in identifying health services to improve patient health (Manara, 2021); Medication-related Teaching/Care (Brito, 2022; Karpiuk et al., 1997; Lemos et al., 2020; Manara, 2021; McCauley et al., 2006; Morrison et al., 2016); Diet-related Teaching/Care (Brito, 2022; Karpiuk et al., 1997; Lemos et al., 2020; Manara, 2021; McCauley et al., 2006); Skin Care (Brito, 2022; Karpiuk et al., 1997; Manara, 2021); Fall Prevention/Environmental Safety (Brito, 2022; Manara, 2021; McCauley et al., 2006); Hygiene/Bathing Care (Brito, 2022; Karpiuk et al., 1997; Manara, 2021).
Regarding the implementation stage, it is important to note that none of the sources of evidence provided insight into how this stage of the nursing process was carried out.
As for the evaluation stage (assessing progress), only four (36.3%) sources addressed it (Lemos et al., 2020; Manara, 2021; Rosted et al., 2012; Shyu et al., 2008). In one source (9.1%), the prior use of the NOC taxonomy during planning facilitated subsequent evaluation (Lemos et al., 2020). The remaining sources did not mention using standardized taxonomies for evaluation but reported using criteria to assess goal achievement and the need for plan modifications (Manara, 2021; Rosted et al., 2012; Shyu et al., 2008).
Discussion
Eleven sources of evidence published between 1993 and 2022 were included, mostly from the United States. The use of taxonomies was not universal, and only two sources mentioned adopting theoretical frameworks. During the initial assessment (data collection), 15 instruments were mentioned; their use enabled a comprehensive assessment of different aspects related to the older adult's needs and the caregiver's preparation for post-discharge care. Most listed diagnoses belonged to the domains of safety/protection, activity/rest, and elimination/exchange. During planning, interventions focused mainly on health education activities. None of the included sources described how the implementation stage occurred. Only four sources addressed how they conducted the evaluation stage (progress).
The NP was first cited by Lydia Hall in 1955 in the United States (Tannure & Pinheiro, 2011). Considering the NP generations, these sources (published 1990–2022) fall within the second to fifth generations. Over these decades, the NP has evolved significantly. This maturation involved standardizing nursing diagnoses, creating specific taxonomies, and structuring clinical thinking to link patient needs with expected outcomes. This period is now viewed as one of knowledge building. In this context, this research helps elucidate how the NP applied to older adults transitioning from hospital to home care has been outlined.
Standardized language systems contribute to knowledge development and clinical reasoning in nursing practice. They provide concepts and terminologies that improve the description of assessments, interventions, and outcomes related to care provided by nursing professionals. Using these systems is essential for creating an appropriate NP. It also improves nursing as a discipline and profession by grounding practices in scientific evidence (Lemos et al., 2020).
The NOC taxonomy outlines nursing outcomes. Professionals incorporating NOC into practice can measure changes in patient states after interventions and monitor progress toward expected outcomes. This means language systems not only guide care but also help standardize and improve care evaluation. However, this study found that not all sources mentioned using a standardized language system. This gap might stem from limited knowledge about these languages among some nursing professionals, potentially leading to reduced accuracy and inconsistent practice (Carvalho et al., 2013).
In addition to adopting taxonomies, using nursing theories is recommended to strengthen and support the NP. Encouraging nursing professionals to apply theories in practical, educational, and research settings is crucial for building solid knowledge (Nascimento et al., 2023).
Nursing theories enable a systemic view of phenomena relevant to the field. They can be useful for defining, explaining, and prescribing nursing actions, thereby supporting interventions during care practice (Bousso et al., 2014). Adopting nursing theories is essential for developing a scientifically based NP, as theories provide theoretical and practical support for nurses’ actions (Alves et al., 2021).
Adopting a nursing theory can guide what should be observed and which direction to follow when developing the NP. However, this study revealed a lack of theoretical frameworks in most sources. This absence may have influenced the types of diagnoses identified, potentially contributing to the lack of diagnoses in the sexuality and life principles domains and the prioritization of physiological/biological diagnoses. This suggests a focus on biological aspects over others.
Among the identified theories, Leventhal's Self-Regulation Theory proposes that individuals’ illness perceptions direct their health behaviors and risk factor management (Cossette et al., 2012). Gottlieb's Strength-Based Care Theory focuses on the person, identifying patient competencies, family resources, and community resources—emphasizing strengths rather than weaknesses (Gottlieb, 2012).
It should be noted that each theory has a specific focus. Therefore, understanding and applying nursing theories in practice is important. This application aims not only to directly improve patient care but also to disseminate knowledge generated and consolidated by nurses (Alves et al., 2021).
Ideally, a holistic assessment should be conducted to ensure care comprehensively meets the individual's needs (Facione et al., 2017). Assessing older adults’ physical and mental capabilities, dependence levels, post-discharge knowledge and preparation, and self-management abilities is crucial. This assessment should consider potential declines due to hospitalization, as previously discussed. Considering the older adult's social context and available social support is also vital, as these factors influence health (Guedes et al., 2017). This includes evaluating aspects like the caregiver's preparation for home care activities.
Regarding data collection, the study findings highlight the importance of a detailed assessment focused on the older adult's care transition. This helps identify related vulnerabilities and strengths. Therefore, using validated instruments that assess various aspects of the individual's biopsychosocial-spiritual sphere, along with their reference scales, supports a holistic assessment (Medeiros et al., 2021). Well-structured and focused data collection guides and facilitates subsequent NP stages.
It is known that hospitalization can cause functional and cognitive declines in older patients (Mendes et al., 2023). Therefore, understanding the most affected domains and predominant nursing diagnoses during the hospital-home transition is crucial. This knowledge helps direct nursing interventions toward actual or potential problems (risks). The results of this scoping review contribute to this understanding.
During the planning stage, nurses should develop a discharge plan. This plan instructs the patient, supporting an organized and clear care transition and aiming to minimize adverse events. Implementing targeted interventions, like those highlighted in this study, represents the nursing team's contribution to providing older patients with optimal conditions and preparation for discharge (Alves et al., 2019).
Regarding nursing interventions/prescriptions, educational activities predominated. Nurse-led education for older adults transitioning home should aim to prepare them to understand their health-disease process and treatment. It should also empower them, considering their abilities and limitations, to actively participate in self-care and complication prevention. Additionally, practical skills must be taught. This ensures the older adult or caregiver can provide effective, continuous home care after leaving the supportive hospital environment (Santos et al., 2022). These points generally align with the findings of the present study.
The evaluation (progress) stage is crucial for reviewing and adjusting the care plan. Adjustments are needed if goals, based on planned outcomes and deadlines, are not fully or partially achieved. This stage requires the nurse's critical thinking combined with knowledge of the patient's history. It's essential for observing potential interferences during the process. Based on the patient's current status and care provided, the nurse then determines necessary changes to the NP (American Nurses Association, 2021; COFEN, 2024). As evidenced in this study, using taxonomies like NOC during planning can aid in measuring results and determining if adjustments are needed.
Notably, none of the included sources addressed all NP stages for older adults in the hospital-to-home transition. Most focused only on diagnosis (n = 5, 45.5%) and/or intervention planning (n = 9, 81.8%). This focus prevented a comprehensive view of the entire NP for this specific population.
A limitation of this study is that some sources did not explicitly name the NP stages, which could have introduced selection bias during screening. To minimize this potential effect, the inclusion criteria required sources to specify terminology related to one or more NP stages in full.
Implications for Practice
These findings can assist clinical nurses in decision-making when developing the NP for older adults transitioning from hospital to home. Specifically, the findings help identify commonly used assessment instruments and frequently defined diagnoses and interventions. They also suggest methods for evaluating patient progress after nursing care implementation.
Further research is needed to advance nursing science regarding the NP for this population. Future studies should report and evaluate the NP, ensuring proper documentation of each phase. Crucially, these studies should incorporate theoretical bases and taxonomies to strengthen the scientific foundation of the profession. This is particularly important as the evidence identified in this review was limited in scope.
The mapping of the state of knowledge also supports constructing standardized nursing protocols in hospitals to improve care transitions for this population. Once protocols are systematized, evaluating the NP's contribution to care and management quality indicators is recommended. This evaluation represents an area where further research is needed, as it remains a gap in the scientific literature.
Conclusions
Eleven sources of evidence focusing on the NP application for older adults in the hospital-to-home care transition were analyzed. Regarding classification systems, only six sources mentioned using at least one; the NANDA-I taxonomy was the most cited. Only two sources emphasized using theoretical bases—specifically Leventhal's Self-Regulation Theory and Gottlieb's Strength-Based Care Theory—to support NP development.
During the initial assessment stage (data collection), six sources reported using various instruments. The diagnostic stage was referenced in five sources, identifying 54 distinct diagnoses; those related to the safety/protection, activity/rest, and elimination/exchange domains predominated. Concerning the planning stage, only two sources mentioned adopting the NOC taxonomy for determining expected outcomes. For intervention planning, NIC-based interventions related to health education were most common. A gap was identified concerning the implementation phase. Finally, in the evaluation stage (progress), only four sources addressed this aspect in their research.
Supplemental Material
sj-docx-1-son-10.1177_23779608251349951 - Supplemental material for Nursing Process Applied to Older Adults in Care Transition From Hospital to Home: A Scoping Review
Supplemental material, sj-docx-1-son-10.1177_23779608251349951 for Nursing Process Applied to Older Adults in Care Transition From Hospital to Home: A Scoping Review by Mayssa da Conceição Araújo, Gustavo Fernandes Lima, Rozemberg Falcão e Silva Alves, Nathan Garcia Rodrigues da Silva, Cristine Alves Costa de Jesus and Alisson Fernandes Bolina in SAGE Open Nursing
Footnotes
ORCID iDs
Author Contribution
Conceptualization: Mayssa da Conceição Araújo; Alisson Fernandes Bolina; Cristine Alves Costa de Jesus. Data Curation: Mayssa da Conceição Araújo. Formal Analysis: Mayssa da Conceição Araújo; Gustavo Fernandes Lima; Rozemberg Falcão e Silva Alves; Nathan Garcia Rodrigues da Silva; Cristine Alves Costa de Jesus; Alisson Fernandes Bolina. Funding Acquisition: Mayssa da Conceição Araújo; Gustavo Fernandes Lima; Alisson Fernandes Bolina. Investigation: Mayssa da Conceição Araújo; Gustavo Fernandes Lima; Rozemberg Falcão e Silva Alves; Nathan Garcia Rodrigues da Silva; Cristine Alves Costa de Jesus; Alisson Fernandes Bolina. Methodology: Mayssa da Conceição Araújo; Alisson Fernandes Bolina; Cristine Alves Costa de Jesus. Project Administration: Mayssa da Conceição Araújo; Alisson Fernandes Bolina. Resources: Mayssa da Conceição Araújo; Gustavo Fernandes Lima; Rozemberg Falcão e Silva Alves; Nathan Garcia Rodrigues da Silva; Cristine Alves Costa de Jesus; Alisson Fernandes Bolina. Software: Not applicable. Supervision: Mayssa da Conceição Araújo; Alisson Fernandes Bolina. Validation: Mayssa da Conceição Araújo; Alisson Fernandes Bolina; Cristine Alves Costa de Jesus. Visualization: Mayssa da Conceição Araújo; Gustavo Fernandes Lima; Rozemberg Falcão e Silva Alves. Writing—Original Draft: Mayssa da Conceição Araújo; Gustavo Fernandes Lima; Rozemberg Falcão e Silva Alves; Nathan Garcia Rodrigues da Silva; Cristine Alves Costa de Jesus; Alisson Fernandes Bolina. Writing—Review and Editing: Mayssa da Conceição Araújo; Gustavo Fernandes Lima; Rozemberg Falcão e Silva Alves; Cristine Alves Costa de Jesus; Alisson Fernandes Bolina.
Funding
This study was conducted with financial support from the Coordination for the Improvement of Higher Education Personnel (CAPES) and the Federal District Research Support Foundation (FAP-DF), Brazil.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Additional Information
The final protocol was registered with the Open Science Framework (OSF) on April 13, 2023 (https://osf.io/r56eh/).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.