
Abstract
Introduction
Psychological first aid is an essential framework for delivering immediate emotional and psychological support to individuals affected by crises and traumatic events. Emergency nurses must possess adequate knowledge and preparedness to provide effective psychological first aid during emergencies.
Objective
This study aimed to assess the levels of knowledge and preparedness to provide Psychological First Aid (PFA) among emergency nurses working in hospitals across the West Bank, Palestine between February and April 2024.
Methods
A descriptive cross-sectional study was conducted between February and April 2024 among 164 emergency nurses working in 19 governmental and nongovernmental hospitals across nine cities in the West Bank, Palestine. Data were collected using an online structured questionnaire assessing nurses’ knowledge of and preparedness for psychological first aid. Statistical analyses were performed using descriptive and inferential statistics to describe study variables.
Results
Most nurses had moderate knowledge of psychological first aid (71.3%), 14.6% had low knowledge, and 14.0% had high knowledge. In terms of preparedness, 51.2% reported being prepared, 31.7% were unprepared, and 17.1% were uncertain. Preparedness was significantly influenced by sex, workplace setting, and professional roles (p < .05).
Conclusion
Despite moderate knowledge levels, over half of the emergency nurses reported adequate preparedness to deliver psychological first aid, suggesting a readiness to respond but with insufficient theoretical grounding. The findings highlight the urgent need to integrate psychological first aid modules into emergency nursing curricula, conduct periodic simulation-based training, and develop standardized institutional protocols to ensure consistent and evidence-based PFA delivery across Palestinian hospitals.
Keywords
Introduction
Recent humanitarian crises, natural disasters, and armed conflicts have drawn global attention to the urgent need for early psychosocial support among the affected populations (Loughry, 2024). Psychological First Aid (PFA) has been identified by the International Federation and Red Cross and Red Crescent Societies as the first and most essential psychosocial intervention to be delivered immediately following emergencies or traumatic events (International Federation and Red Cross, 2019). It is a humane, evidence-based approach designed to reduce acute distress, promote safety and calmness, and strengthen adaptive coping capacities in both the short and long term (Hermosilla et al., 2023).
The theoretical foundation of PFA relies on five core principles—safety, calmness, connectedness, self-efficacy, and hope—and it is delivered through structured actions, such as establishing contact, ensuring safety and comfort, stabilizing emotions, gathering information, offering practical assistance, and linking individuals with social and professional support (Wang et al., 2021). Importantly, PFA can be effectively provided not only by mental health professionals but also by trained nonspecialists including nurses, paramedics, and volunteers, making it a scalable and community-based intervention (Wang et al., 2021).
Growing empirical evidence demonstrates that PFA training enhances responders’ psychosocial competence and preparations, which collectively constitute their preparedness—the ability to confidently and effectively apply appropriate psychological support skills in crisis situations. A recent scoping review and randomized controlled trial reported that trained PFA providers exhibit reduced distress, better emotional regulation, and an improved ability to provide structured support during crises (Sijbrandij et al., 2020; Wang et al., 2021). In Palestine, trained nurses and first responders have reported increased confidence and calmness, improved safety awareness, and stronger social connectedness following PFA and general trauma training (Alwawi et al., 2019; Schafer et al., 2016). These findings indicate a pivotal role of PFA in the context of chronic instability and recurrent exposure to trauma.
Given the demanding nature of emergency nursing, characterized by exposure to war injuries, mass casualty events, and public health emergencies, PFA competence is critical to ensure both patient stabilization and caregiver psychological wellbeing (Barten et al., 2021). However, several studies have identified substantial gaps in PFA-related knowledge and preparedness among healthcare workers. For instance, Nair et al. (2023) found that nurses demonstrated poor to moderate knowledge of PFA, while approximately half reported moderate preparedness. Similar deficiencies have been noted across Asian and Middle Eastern contexts, suggesting a global need for structured educational programs (Said et al., 2022).
Over the past 5 years, an expanding body of evidence has assessed the level of knowledge and preparedness regarding PFA and emphasized the effectiveness of PFA education in improving nurses’ competence, communication, and resilience during crises. For example, a cross-sectional study of 580 Turkish nurses found low training uptake and moderate PFA preparedness (Kiliç Bayageldi & Kaloğlu Binici, 2024). A similar study of 536 Turkish nursing students reported high proportions without PFA training and only moderate readiness to apply PFA (Bayageldi & Binici, 2024). Chandler et al. (2023) highlighted that implementing PFA programs for healthcare workers enhances their perceived capability and reduces emotional exhaustion. Schoultz et al. (2022) found that PFA training among nursing home staff improved coping, empathy, and stress management, while Movahed et al. (2023) confirmed, through a systematic review, that structured courses strengthened both knowledge and self-efficacy. A randomized controlled trial by Madani et al. (2024) demonstrated that virtual PFA education significantly improves nurses’ communication and empathy in disaster contexts. Furthermore, global reviews have consistently shown that PFA interventions enhance psychosocial competence and expand access to early mental health support, especially in low-resource or conflict-affected regions (Adewunmi et al., 2025; Wang et al., 2021).
In Palestine, the situation is compounded by ongoing conflict, limited mental health resources, and frequent mass casualty incidents (Saad & Dergaa, 2023). Emergency nurses, often the first point of contact for psychologically traumatized individuals, are expected to deliver immediate emotional support despite the absence of standardized training or institutional PFA protocols (Al-Kalaldeh et al., 2020). This lack of structured guidance not only affects nurses’ confidence and response consistency, but may also influence patients’ satisfaction and the overall quality of care, as effective psychosocial support is closely linked to patient recovery, trust, and perceived safety (Amro et al., 2018). However, there is a lack of empirical data evaluating the current levels of knowledge and preparedness to provide PFA. Without such evidence, it is difficult to identify competency gaps or to design effective educational interventions tailored to local needs.
Review of Literature
Recent cross-sectional evidence suggests nurses’ PFA capability sits around a moderate level but rises with experience, role seniority, and training exposure. In Turkey, a study assessed the level of knowledge and preparedness regarding PFA and emphasized the effectiveness of PFA education in improving nurses’ competence, communication, and resilience during crises. For example, a cross-sectional study of 580 Turkish nurses found low training uptake and moderate PFA preparedness (Kiliç Bayageldi & Kaloğlu Binici, 2024). In addition, a nationwide survey of 580 nurses found moderate PFA application self-efficacy overall, with higher scores among those who had prior disaster education and drill participation, pointing out the value of structured practice opportunities (Bayageldi & Binici, 2024). Other study among nurses reported “above-medium” perceptions of disaster preparedness alongside stronger PFA self-efficacy in charge nurses versus staff nurses, and significantly better scores among nurses who had attended drills, highlighting the influence of senior responsibility and hands-on rehearsal (Çömez Ikican et al., 2025).
Extending to broader preparedness, an international survey of nurses with disaster field experience showed psychological readiness (a pre-requisite for competent PFA) was uneven and strongly associated with prior training and exposure, pointing to persistent preparedness gaps without formal programs (Said et al., 2022). Methodological work validating an Arabic PFA scale using a cross-sectional sample that included nurses further documented measurable variability in PFA knowledge, attitudes, and skills across professional groups, offering a reliable tool to track nurse competencies over time (Alshareef et al., 2025). Finally, a 2025 cross-sectional assessment of nurses’ psychological and operational readiness for mass-casualty events reinforced these patterns, linking preparedness indicators to training and experience and implying that embedding PFA content within disaster curricula may strengthen real-world response (Shubayr, 2025).
Therefore, this study aimed to assess the levels of knowledge and preparedness to provide PFA among emergency nurses working in hospitals across the West Bank, Palestine, and examine the association between demographic factors and both knowledge and preparedness levels. Addressing this gap will contribute to developing context-appropriate PFA training modules and integrating psychosocial care into emergency nursing curricula and disaster preparedness programs in Palestine.
Methods
Research Design
A descriptive cross-sectional design was employed to assess the levels of knowledge and preparedness to provide PFA among emergency nurses in West Bank, Palestine. This design was chosen because it allowed researchers to collect data at a single point in time, providing a snapshot of nurses’ current knowledge and preparedness regarding PFA. This design is particularly appropriate when the goal is to measure prevalence, identify patterns, and highlight potential gaps, without attempting to establish causality (Polit & Beck, 2020).
Setting and Population
This study was conducted among emergency nurses working in 19 governmental and nongovernmental hospitals distributed across nine major cities in the West Bank, Palestine (Jerusalem, Nablus, Hebron, Ramallah, Jenin, Tulkarm, Qalqilya, Bethlehem, and Tubas). These hospitals represent primary healthcare institutions that provide round-the-clock emergency and trauma services to a diverse patient population, encompassing both urban and rural catchment areas. The emergency departments of these hospitals vary in size and specialization, ranging from tertiary referral centers with high patient loads to district-level hospitals offering general emergency and acute care services.
The study population included all registered nurses currently employed in emergency departments, who were directly involved in patient care. The exclusion criteria included nurses who had previously received formal training in PFA or other structured mental health programs as well as those who declined to participate. Data were collected between February and April 2024 through an online structured questionnaire distributed via official hospital communication channels. This multicenter approach ensured the inclusion of nurses from various institutional contexts, enhancing the representativeness and generalizability of the study findings across the Palestinian healthcare system.
Sample Size and Method
Convenience sampling was employed to recruit participants. The required sample size was calculated using G*Power version 3.1 for an independent-sample t-test with a medium effect size (Cohen's d = 0.50), a two-tailed significance level of α = .05, and a statistical power of 0.95 (Kang, 2021). The minimum estimated sample size was 200 nurses. A total of 160 nurses completed the study, with an 82% response rate. Attrition was primarily due to clinical workload, rotating shifts, and scheduling constraints.
Instrument
A structured, self-administered questionnaire was adopted based on the Minnesota Department of Health (MDH) validated instruments and relevant literature to assess participants’ sociodemographic characteristics, knowledge, and preparedness regarding PFA (Minnesota Department of Health, 2022; Said et al., 2022). The questionnaire consisted of three sections. The first section collected sociodemographic data, including age, gender, marital status, educational level, workplace, job position, and years of work experience. The second section assessed knowledge using a 12-item scale developed by the MDH (2022), with dichotomous responses (“true” or “false”); correct answers were scored as 1 and incorrect as 0, with total scores ranging from 0 to 12. The cutoff points were as follows: low knowledge, 0–4; moderate knowledge, 5–8; and high knowledge, 9–12. The third section measured preparedness to provide PFA through10 items using a scale developed by Said et al., (2022) designed to assess readiness to apply PFA skills. Responses were rated on a five-point Likert scale ranging from 1 (very unprepared) to 5 (very prepared), with total sum scores ranging from 10 to 50, and classified into three levels: unprepared (10–23), uncertain (24–36), and prepared (37–50).
Pilot Study
Pilot research was conducted prior to the primary data collection of 21 participants from two hospitals who were excluded from the main study population. The main objective was to evaluate the reliability of the scales (knowledge: 0.89, preparedness: 0.95), clarify the questionnaire items, ascertain the average completion time, and verify the relevance and understanding of the tools within the local context. Minor linguistic adjustments were made to improve clarity and cultural relevance. The average completion time for the survey was approximately 15 min.
Data Collection
Data were gathered via a standardized self-administered online questionnaire developed using Google Forms. This strategy was selected to enable participation in a secure, accessible, and time-efficient manner, particularly given the volatile sociopolitical circumstances in the West Bank of Palestine.
The survey link was sent via professional WhatsApp and Facebook groups utilized by healthcare employees. The study team selected these platforms based on their past knowledge of usage within the target group and established professional communication networks. Invitation to participate among nurses employed in governmental and nongovernmental settings.
The Google Form was set up to permit only one answer per email account to prevent repeated submissions. A compulsory informed consent statement was incorporated into the initial survey page. Participants were informed of the study's objective, the voluntary aspect of their involvement, and the confidentiality of their responses. Advancing the questionnaire after reviewing the consent statement was considered evidence of their permission to participate. The finalized survey data were securely stored in encrypted files accessible to the lead investigators. The research staff oversaw the submission process to guarantee response quality, monitor completion rates, and address participant inquiries swiftly, as necessary.
Statistical Analysis
The collected data were analyzed using the Statistical Package for Social Sciences (SPSS) version 27. The data analysis was conducted using descriptive and inferential statistics. Regarding descriptive statistics, frequency, percentage, mean score, and standard deviation (SD) were used to describe the study variables. Regarding inferential statistics, independent t-tests and analysis of variance (ANOVA) for mean comparisons. The normality of data distribution was verified using the Shapiro–Wilk test, and homogeneity of variances was tested using Levene's test. Parametric tests were performed because the assumptions were met. Statistical significance was set at p < .05.
Ethical Consideration
Ethical approval for this study was obtained from the Institutional Review Board of MUC016/2025. Participants received detailed information regarding the study objectives, procedures, and right to withdraw at any time without penalty. Informed consent was obtained electronically before participation. Confidentiality and anonymity were maintained by excluding any identifying information and storing all responses in encrypted files accessible only to the investigators. This study adhered to the ethical principles of the Declaration of Helsinki.
Results
A total of 164 emergency nurses participated in this study. Most were aged 20 to 29 years (58.5%) and male (61.0%). Nearly equal proportions were single (47.0%) or married (47.0%). The majority held a bachelor's degree (70.7%) and worked in government hospitals (73.8%). Registered nurses formed the largest group (70.7%), and most participants had fewer than 7 years of professional experience (81.7%). As shown in Table 1.
Differences Between Demographic Variables in Terms of Both Knowledge and Preparedness to Provide PFA (n = 164).
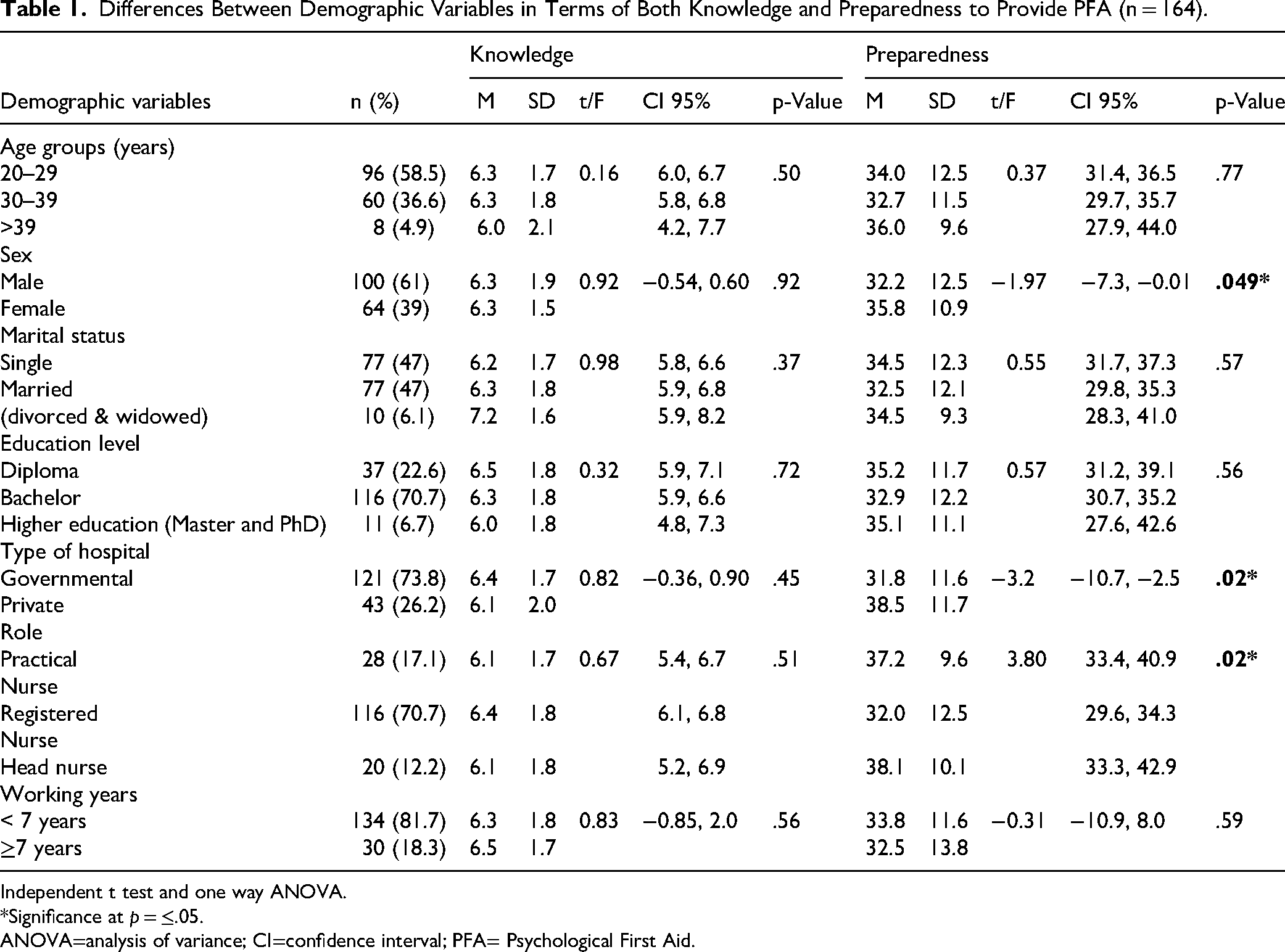
Independent t test and one way ANOVA.
*Significance at p = ≤.05.
ANOVA=analysis of variance; CI=confidence interval; PFA= Psychological First Aid.
Level of Knowledge
Overall, more than half of the nurses had moderate knowledge levels (71.3%), with (14.6%) showing low knowledge and only (14%) achieving high knowledge; the lowest correct response was for PFA (26.2%), while the highest was recognizing children's need for structured environments after trauma (60.4%). About half answered correctly on active listening (53.0%) and the timing of story sharing (62.2%), whereas fewer identified the importance of meeting basic needs, avoiding immediate psychotherapy, preparation and training, and stress-related symptoms (37%–42%); as seen in Table 2.
Frequency and Percentages for Each Knowledge Item Among Nurses (n = 164).
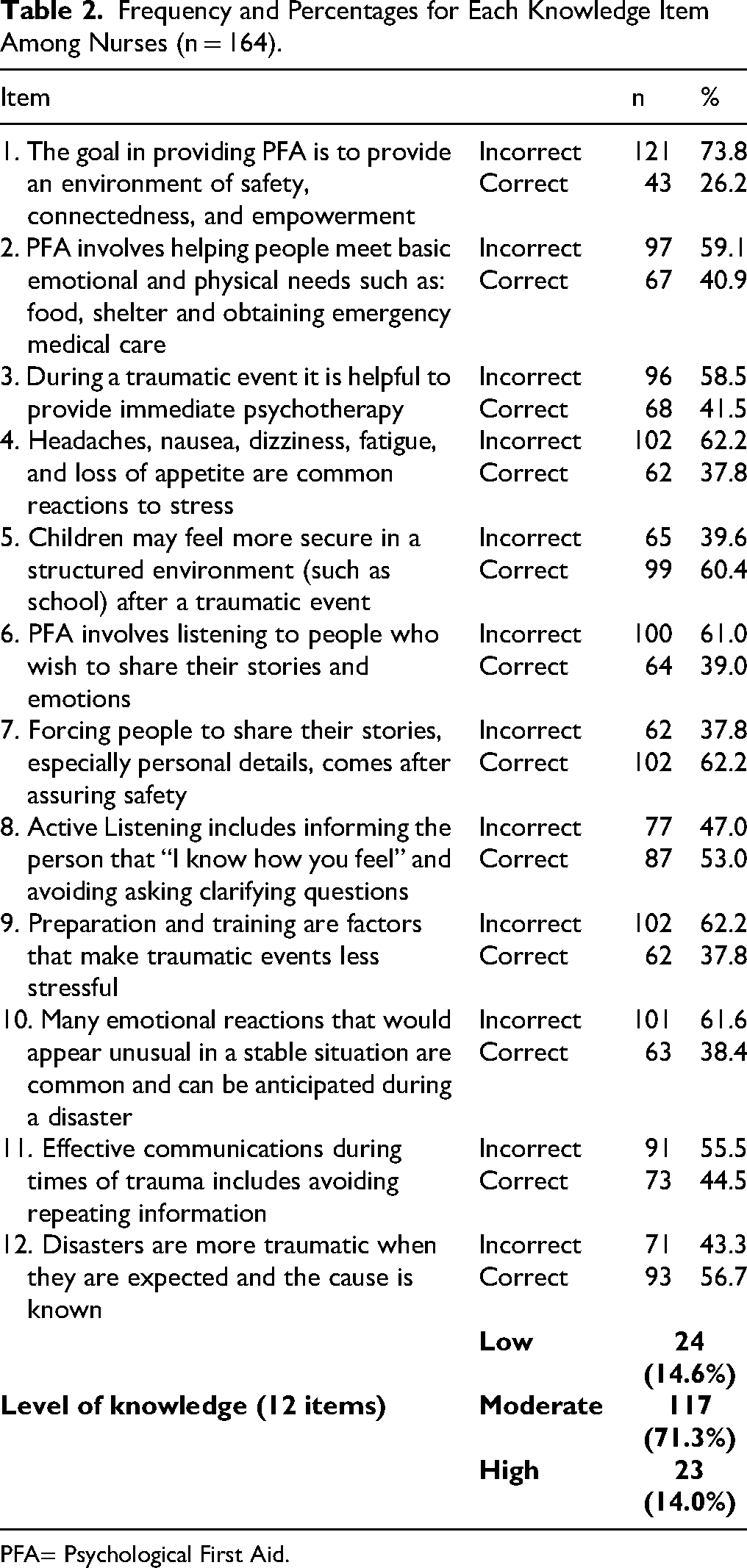
PFA= Psychological First Aid.
Level of Preparedness
Nurses showed a moderate level of preparedness in PFA (M = 3.36, SD = 1.37): 51.2% were prepared, 31.7% were unprepared, and 17.1% were uncertain. The highest scores were for active listening and communication (M = 3.55) and prioritizing basic needs (M = 3.45), whereas the lowest scores were for self-care (M = 3.21) and coping with stress (M = 3.31). These results highlight adequate communication skills, but limited resilience and self-care practices; as seen in Table 3.
Mean Score for Each Item Toward Preparedness to Provide PFA (n=164).

PFA= Psychological First Aid.
Differences Between Demographic Variables in Term of Knowledge and Preparedness Scores
The analysis showed no statistically significant differences in knowledge of PFA across demographic variables, including age, marital status, education level, hospital type, professional role, or years of experience. However, significant differences were observed in the preparedness levels. Female nurses demonstrated significantly higher preparedness than male nurses (p < .05) indicating greater readiness to provide PFA. In addition, nurses working in private hospitals reported higher preparedness than those working in governmental hospitals (p < .05). Professional role was also a determining factor, and a Tukey post hoc test indicated that head nurses and practical nurses exhibited greater preparedness than registered nurses (p < .05). These findings suggest that preparedness to deliver PFA is influenced more by sex, role, and institutional setting than age, education, or experience; as seen in Table 1.
Discussion
This study aimed to assess emergency nurses’ knowledge and preparedness to provide PFA in the West Bank and to identify gaps to guide future training and educational interventions.
Knowledge Toward PFA
The study revealed that emergency nurses demonstrated limited knowledge of PFA, consistent with findings from Turkey, Iran, and the Philippines, where nurses exhibited a low conceptual understanding of PFA principles and confusion between its scope and psychotherapy (Hassankhani et al., 2018; Kılıç & Şimşek, 2018; Labrague et al., 2018). Similar to global findings, participants in this study showed a stronger awareness of communication- and safety-related aspects than theoretical foundations, indicating a practical but incomplete understanding. This aligns with a recent study emphasizing that healthcare providers often prioritize immediate physical care, while overlooking psychosocial support as a structured process (Bright et al., 2024). However, a systematic review reported moderate to high knowledge levels following structured training programs (Schoultz et al., 2022). Palestinian nurses lacked similar educational opportunities. The gap observed here likely reflects the absence of institutionalized PFA curricula and continuous professional development. Evidence from recent trials demonstrates that targeted PFA programs, both in person and online, significantly improve knowledge and confidence (Madani et al., 2024). Therefore, the current results underline the need for the systematic integration of PFA content into emergency nursing education and national disaster preparedness frameworks.
Preparedness to Provide PFA
Nurses reported moderate preparedness levels, comparable to previous literature, where healthcare workers perceived themselves as moderately ready but uncertain about effectively psychological support techniques effectively (Al-Kalaldeh et al., 2020; Said et al., 2022; Zakaria & Chuemchit, 2017). Consistent with these studies, participants scored higher in communication and prioritizing basic needs—core PFA principles, but lower in self-care and stress management. These deficits mirror the international concern that healthcare workers receive minimal training in maintaining their psychological resilience during crises (Madani et al., 2024; Schoultz et al., 2022). The moderate preparedness found here suggests experiential familiarity rather than formal competence, highlighting the necessity for structured simulations and scenario-based exercises to translate theoretical knowledge into a confident practice.
Differences by Demographic and Professional Variables
The finding that female nurses exhibit higher preparedness aligns with previous evidence showing women's stronger interpersonal and empathetic engagement in psychosocial care (Huang et al., 2020). Similarly, nurses in private hospitals demonstrated greater readiness than those in governmental institutions, reflecting disparities in training resources and organizational support. Studies in Jordan and Palestine have also observed that well-resourced facilities provide more opportunities for continuous education, directly enhancing readiness for crisis responses (Alwawi et al., 2019; Said et al., 2022). The higher preparedness levels of head and practical nurses compared to registered nurses may relate to their leadership responsibilities and frequent frontline exposure during emergencies, findings consistent with regional disaster nursing research (Olorunfemi & Adesunloye, 2024). Collectively, these results highlight the influence of institutional environment and role expectations on nurses’ psychological readiness.
Strengths and Limitations
This study provides valuable insights into an underexplored area within Palestinian healthcare by examining emergency nurses’ knowledge and preparedness to deliver psychological first aid. Its multicenter design, involving 19 governmental and nongovernmental hospitals across nine cities, enhances the breadth and contextual relevance of the findings. However, the cross-sectional design limits causal inference, and the reliance on self-reported questionnaires may have introduced response bias, particularly in preparedness ratings where abilities could be overestimated. Additionally, the use of convenience sampling may restrict the generalizability of the findings to all emergency nurses in Palestine.
Nursing Implications
Integrating PFA concepts into undergraduate curricula and continuous professional development programs can bridge knowledge gaps and improve evidence-based practice. Regular simulation training and interprofessional drills should be implemented to enhance preparedness and confidence in crisis response. Moreover, nursing leadership should promote self-care and stress management strategies as integral components of professional readiness to ensure that nurses can sustain psychological resilience while caring for others. Developing institutional policies and national guidelines on PFA would also help standardize practice across healthcare settings, enabling nurses to provide consistent, safe, and compassionate support to individuals affected by trauma or disasters.
Conclusion
Emergency nurses in the West Bank demonstrated moderate preparedness but limited knowledge of psychological first aid, indicating a clear gap between perceived readiness and evidence-based competence. Although nurses showed relative strength in communication and in addressing immediate patient needs, deficiencies in theoretical understanding, self-care, and stress-management skills underscore the need for systematic professional development. These findings are consistent with international evidence and suggest that, in the absence of structured education and institutional support, nurses’ capacity to deliver consistent and effective psychosocial care remains fragmented. To address these gaps, psychological first aid principles should be formally integrated into undergraduate and postgraduate nursing curricula in Palestine, alongside continuous professional development initiatives. Hospitals are encouraged to implement regular, scenario-based training and simulation exercises to reinforce theoretical knowledge and enhance practical application in emergency contexts. In addition, healthcare institutions should embed self-care, stress-management strategies, and peer-support mechanisms within PFA training to promote nurses’ psychological resilience. Coordinated efforts between the Ministry of Health, the Nursing Council, and humanitarian organizations are also essential to develop standardized, context-appropriate PFA protocols that ensure consistent practice across healthcare settings. Finally, future research should examine the long-term effects of structured PFA training on nurses’ performance and patient outcomes to guide evidence-informed policy and curriculum development.
Footnotes
Acknowledgements
The authors sincerely thank all the participants in this study working governmental and nongovernmental settings in the West Bank, Palestine. Despite heavy workloads and challenging conditions due to ongoing conflict, their dedication made this research possible.
Ethics Approval and Consent to Participate
Ethical approval for the conduction of the study was obtained from the Ethical Committee of Modern University College Approval no. (muc016/2025). An informed consent was provided to all the participants prior to their enrollment in the research as well as participants were informed that they were voluntarily participating in the first page of the questionnaire. Confidentiality while gathering data was ensured. Additionally, participants were assured that all personal information would be protected, secured, and kept confidential. The research adhered to the ethical standards outlined in the Declaration of Helsinki regarding the rights, protection, and wellbeing of research participants.
Consent for Publication
This manuscript does not contain any individual person's data in any form (including individual details as name, images, or videos).
Author Contributions
NA conceptualized the study, performed data analysis and interpretation, wrote the initial draft, and contributed to revisions. SS and MS conceptualized the study, critically revised the entire manuscript for important intellectual content. AF, FI, FM, HR, AI, and HA were responsible for data collection and entry, follow the ethical approval, building the figure and contributed to the writing of the manuscript as well.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.